
Abstract
OBJECTIVE:
To evaluate the efficacy and safety of percutaneous ultrasound-guided thermal ablation in the treatment of cervical metastatic lymph nodes (LNs) from papillary thyroid carcinoma (PTC).
MATERIALS AND METHODS:
A total of 77 patients with 79 LNs ablated by microwave ablation (MWA) or radiofrequency ablation (RFA) between September 2018 and October 2022 were enrolled in this study. After treatment, patients were followed up with measurement of diameters of LNs and serum thyroglobulin (s-Tg) at 1, 3, 6, and 12 months and annually thereafter. The paired t-test was used to compare the changes of s-Tg level, diameters of LNs before and after ablation.
RESULTS:
There were no serious complications related to ablation while one case of incomplete ablation in MWA was found during follow-up. The mean longest and shortest diameter of the ablated LNs reduced from 11.6 ± 4.3 mm to 5.0 ± 4.1 mm (p < 0.001), and from 6.1 ± 1.9 mm to 3.0 ± 2.5 mm (p < 0.001) at the last follow-up visit. Besides, the final volume reduction rate (VRR) was 61.8 ± 56.4% (range, –67.0 –100%). The complete disappearance rate was 46.8%, but there were 4 (5.1%) LNs becoming bigger than before. The average s-Tg level was 9.2 ± 26.6 ng/mL, a data significantly decreased to 3.7 ± 7.0 ng/mL at the last follow-up, but no statistical difference was shown.
CONCLUSION:
Thermal ablation is an effective and safe modality for the treatment of metastatic LNs from PTC.
Introduction
Papillary thyroid carcinoma (PTC), the commonest histological subtype of thyroid cancer, is comprising about 80–85% of all thyroid malignant tumors [1, 2]. Since the early 1980 s, the incidence of PTC has been notably increasing in many countries mainly because of the introduction of new diagnostic techniques, including ultrasonography (US) and fine-needle aspiration biopsy (FNAB) [3]. Despite the high morbidity, the mortality rate is extremely lower than many other malignancies. However, PTC still represents a clinical dilemma for surgeons on account of its high tendency of metastasis to cervical lymph nodes (LNs), and the ratio is reported even up to 20–90% [4]. After surgery there are still 15–30% of patients who will be detected with cervical lymph nodes metastases during follow-up [5, 6]. For this part of patients, repeated surgery is still recommended by guidelines for long-term survival, although the fibrosis and distortion of normal tissue planes secondary to postoperative scar formation have made this even more of a challenge [7]. Besides, a high rate of complications caused by reoperation, such as nerve injury, transient or permanent hypoparathyroidism, will inevitably increase patients’ fear and suffering [8]. Hence, a more non-invasive alternative to repeated surgery is urgently needed to relieve these difficult positions, and then benefit for both individual patients and the clinical practice as a whole.
In the recent few years, several minimally invasive techniques, especially US-guided percutaneous thermal ablations, including radiofrequency ablation (RFA) and microwave ablation (MWA) have achieved excellent results in the treatment of benign thyroid nodules, liver cancer, as well as renal tumor [9, 10]. As a consequence, these alternatives are gradually recognized by both patients and clinicians, and then obtaining widespread use. However, US-guided percutaneous thermal ablations, as an emerging technique to treat cervical metastatic LNs from PTC, still need further investigation of its safety and efficacy before completely replacing repeated surgery. To the best of our knowledge, relevant researches are limited, in which most of them are small sample studies [11–13]. So the aim of this study was to evaluate the efficacy and safety of thermal ablation for the treatment of cervical metastatic LNs from PTC.
Materials and methods
Patients
This retrospective study was approved by our hospital Institutional Review Board, and all patients signed an informed consent prior to ablation with knowledge of possible complications.
The inclusion criteria were as follows: (1) patients with total or subtotal thyroidectomy for PTC, and central neck dissection; (2) confirmed cervical LNs metastasis from PTC by US guided-FNAB; and (3) patients were ineligible or refused to undergo repeated neck explorations. And the exclusion criteria were: (1) pregnant women; (2) no appropriate puncture route for ablation; (3) patients with distant metastasis; (4) patients with severe respiratory or coagulation disorder; (5) allergic to the US contrast agent.
There were 83 patients with 86 times of ablation performed in our department between September 2018 and October 2022. After removing patients lost to follow-up, a total of 77 patients with 79 times of RFAs or MWAs for cervical metastatic LNs from PTC were enrolled in this study. The flowchart detailing patient selection process is presented in Fig. 1.

Flowchart of subject selection.
During routine US follow-up after PTC surgical resection, US guided-FNAB was recommended to distinguish the essence of LNs once suspicious characteristics (e.g., hilar replacement, unclear margins, perinodal edema, node matting, calcifications and cystic changes) were revealed [14]. Meanwhile, the size (longest and shortest diameter), intralesional vascularity, location (right or left; II, III, IV, V or VI), and surroundings of all the suspicious LNs were carefully evaluated.
If metastatic LNs from PTC were cytologically confirmed by US guided-FNAB, and patients were ineligible or refused to receive repeated surgery, then ablation would be taken into consideration and some preoperative preparations must be done. First of foremost, no warfarin sodium or anti-platelet medications were taking for at least 2 weeks before ablation. Laboratory tests including blood coagulation, blood routine, thyroid hormone, as well as serum thyroglobulin (s-Tg), were measured within three days before ablation.
Equipment and procedures of ablation
Patients lay supine with their necks exposing fully, and an electrocardiograph (ECG) monitor was used to constantly monitor heart rate and blood pressure. After the nurse put a 18-gauge intravenous cannula into patients antecubital vein, the skin of ablation site from the chin to shoulders was well sterilized and then drape with sterile towels by the operator.
Step one: A pre-ablation contrast-enhanced ultrasound (CEUS). CEUS was performed using real-time US systems (model: LOGIQ E9, GE Healthcare, Pittsburgh, PA, USA), equipped with a linear probe (9L4, 4–9 MHz). SonoVue (Bracco, Bracco Imaging, Milan, Italy) was used as contrast agent in this examination and mixed with 5 mL 0.9% sterile saline. The selected plane for CEUS should be a medium-sized one including pathological LN and surrounding normal tissue for comparison. CEUS was conducted to observe the blood perfusion and enhancement mode of metastatic LNs by injecting 2.4 mL SonoVue suspension in a bolus fashion via a 18-gauge intravenous cannula, followed by a flush of 5 mL 0.9% sterile saline. After injection of contrast agent, continuous imaging was recorded immediately and lasted for 5 min. During this time, the operator must carefully observe the perfusion of metastatic LNs and vascularity within the ablation zone, thereby determining an appropriate puncture path.
Step two: MWA/RFA. A microwave ablation system (MTI-5A; Great Wall Medical Equipment Co. Ltd, NanJing, China) with a 16-gauge circulating water-cooled MWA probe (Microwave probe XR-A1610 W; Great Wall Medical Equipment Co. Ltd, NanJing, China), RFA devices consisting of a bipolar 470-kHz radiofrequency generator (CelonLab Power; Olympus-Celon, Teltow, Germany) or a commercially available internally cooled monopolar radiofrequency generator (StarMed, Goyang, South Korea), were selectively used in our department. The whole process of MWA/RFA was under monitoring of real-time US. Before ablation, the patient was given local infiltration anesthesia (5–10 mL 2% lidocaine) both at the puncture site and along the puncture path. Thereafter, a small skin incision was made at the puncture site. And then a 16-gauge ablation probe was percutaneously inserted into the targeted LN under real-time US guidance. For small LNs, mono-section ablation was almost enough, but for some big ones, the method of multipoint and multiplane moving-shot ablation was necessarily adopted to achieve complete ablation [15]. A power output of 30 W was used, and lasting for 5–10 s in each point depending on the tolerance of patients and the size of LNs. The ablation was stopped when the hyperechoic zone of microbubbles completely covered the initial targeted LN. Then waiting for the dissipation of microbubbles, CEUS was performed again to evaluate perfusion of the ablated area. The ablation was considered successfully finished if unenhanced areas on CEUS completely exceeded the ablated zone. If any enhanced area was seen within the initial targeted LN, a secondary ablation was immediately performed. And this counted as just one ablation.
Step three: Postoperative observation. After ablation, all patients were carefully observed for approximately 2–3 h, and some possible complications (bleeding, hematoma, skin burns, hoarseness, etc.) were evaluated.
Post-ablation follow-up
Post-ablation follow-up examinations consisting of US and laboratory tests (i.e., s-Tg, thyroid hormone, blood coagulation, blood routine), were administrated at 1, 3, 6, and 12 months after treatment and annually thereafter. Additionally, CEUS was recommended at the first month of follow-up. US guided-FNAB, positron emission tomography (PET) and other accessory examinations were necessarily performed if there were suspicious distant metastases during follow-up. All examination data were recorded in detail at each follow-up.
Statistical analysis
Data of patients was presented using mean±standard deviation (SD) and ranges for quantitative characteristics, and absolute frequencies for qualitative characteristics. The paired t-test was used to compare the changes of s-Tg level, the longest and shortest diameters of LNs before and after ablation. Besides, volume reduction rate (VRR) was used to evaluate the ablation efficacy, an index calculated as follows: VRR = [(initial volume – final volume)×100% ] / initial volume. All statistical analyses were performed by using SPSS software, version 23.0 (IBM, Armonk, NY). Statistical significance was set at p < 0.05.
Results
Clinical characteristics of patients
The clinical characteristics of the study population are presented in Table 1. Among a total of 77 patients with mean age of 45.0 ± 14.1 years (range, 14–77 years), there were 17 males and 60 females, and two of them received 2 times of MWAs in our department. Of the 77 patients included in the study, five underwent 2 times of surgical resections, and 24 (29.3%) received total thyroidectomy combined with central neck dissection. After surgery, 28 patients did not receive postoperative Iodine 131 (I131) therapy, and the rest received one or two times I131 treatments. The mean time interval from surgical resection to MWA/RFA was 28.8 ± 30.4 months (range, 2–124 months).
Clinical characteristics of the study population
Clinical characteristics of the study population
Abbreviations: M/F, male/female; Y, year; SD, standard deviation; L, left; R, right; B, bilateral; No., number; M, month.
In 77 patients, a total of 246 LNs, 94 (38.2%) in the right neck and 152 (61.8%) in the left neck, were ablated in 79 times of ablations. The relevant information of the ablated LNs is listed in Table 2. There were 17 (6.9%), 50 (20.3%), 58 (23.6%), 28 (11.4%), and 93 (37.8%) LNs located in level II, III, IV, V and VI, respectively. It was observed that these LNs were mainly situated in level III, IV and VI. The mean ablation time was 102.6 ± 45.3 s (range, 27–196 s). Figure 2 shows a representative case of ablation.
Parameters of cervical metastatic LNs before and after ablation
Parameters of cervical metastatic LNs before and after ablation
Abbreviations: CEUS, contrast enhanced ultrasound; s, second; s-Tg, serum thyroglobulin; VRR, volume reduction rate. p1 - 3 value: last follow-up vs. pre-ablation in longest diameter, shortest diameter and s-Tg level, respectively.
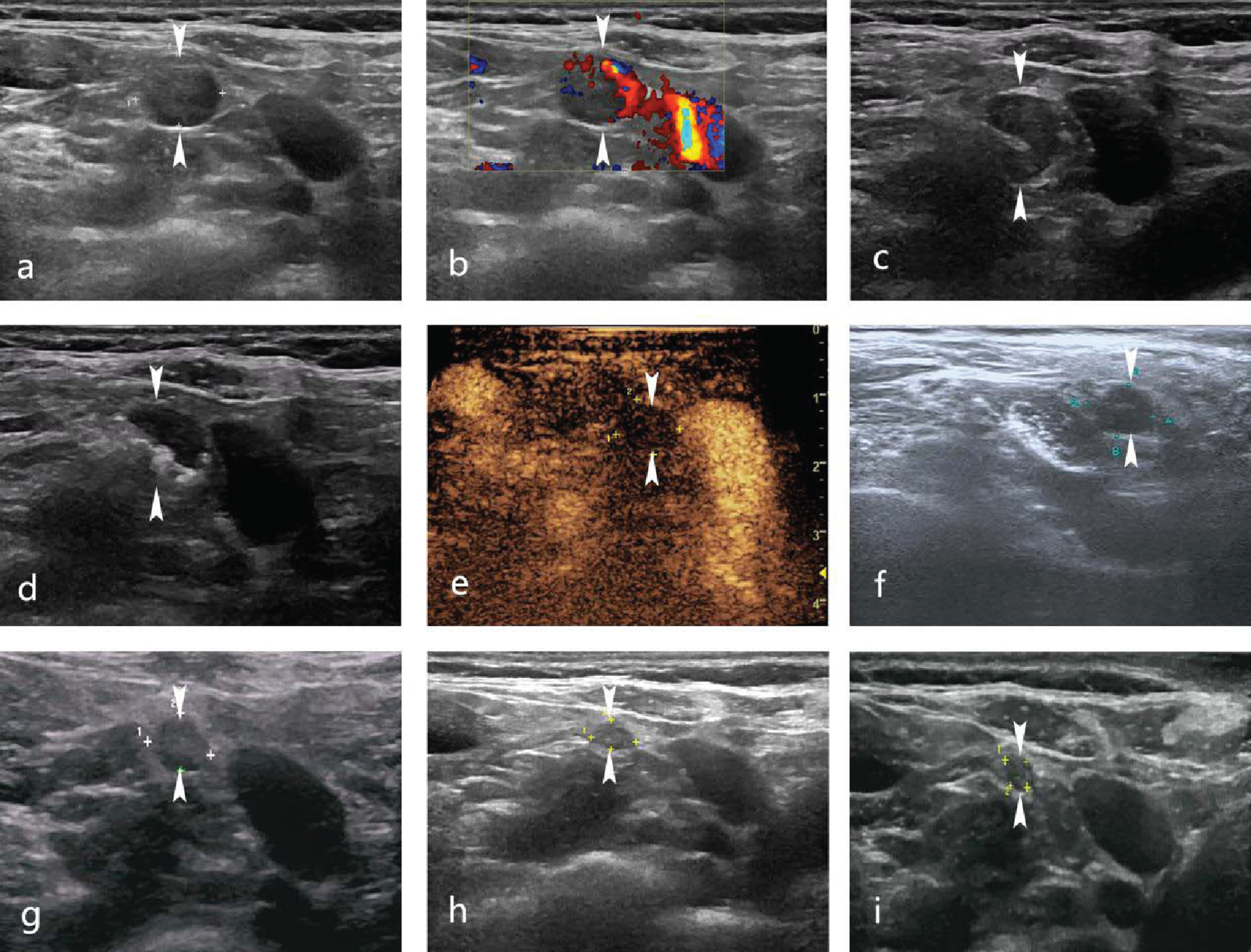
A 35-year-old woman received MWA of metastatic LNs from PTC 2 months after total thyroidectomy. Before MWA, B-mode US showed hypoechoic LN (size 10.2×8.6×8.7 mm) with cystic changes (a, arrow). On color Doppler US, intensely colored patterns were depicted (b, arrow). Then US guided-FNAB was performed to confirm LN metastasis from PTC (c, arrow). A 16-gauge MWA probe was percutaneously inserted into the targeted LN under real-time US guidance and started ablation (d, arrow). After MWA, the CEUS showed no enhancement in LN (e, arrow).1-month post-ablation, size 9.6×7.3×5.6 mm (f, arrow). 3-month post-ablation, size 6.9×5.2×5.3 mm (g, arrow). 6-month post-ablation, size 5.3×3.4×3.7 mm (h, arrow). 1-year post-ablation, size 3.5×2.6×2.4 mm (i, arrow).
Considering the integrity of follow-up data, the LN with the largest diameter in each ablation was selected, so a total of 79 LNs was enrolled and then analyzed in this study. Before ablation, the mean longest diameter of the initial LNs was 11.6 ± 4.3 mm (range, 3–27 mm), and the data reduced to 5.0 ± 4.1 mm (range, 0–12 mm) at the final follow-up. Besides, at the last follow-up the average shortest diameter decreased from 6.1 ± 1.9 mm (range, 3–10 mm) to 3.0 ± 2.5 mm (range, 0–8 mm). And the VRR was 61.8 ± 56.4% (range, –67.0 –100%) at the final follow-up visit. Significant differences were shown in the longest and shortest diameter before and after MWA/RFA at the final follow-up (p < 0.001). During follow-up, 72 (91.1%) patients underwent CEUS and no enhanced area was seen within the ablated zone in 71 patients (Fig. 3). Finally, 37 (46.8%) ablated LNs completely disappeared, 4 (5.1%) LNs became bigger than before, and the rest 38 (48.1%) LNs remained as small scar-like lesions. The mean follow-up time of cervical LNs US was 9.1 ± 7.8 months (range, 1–26 months).
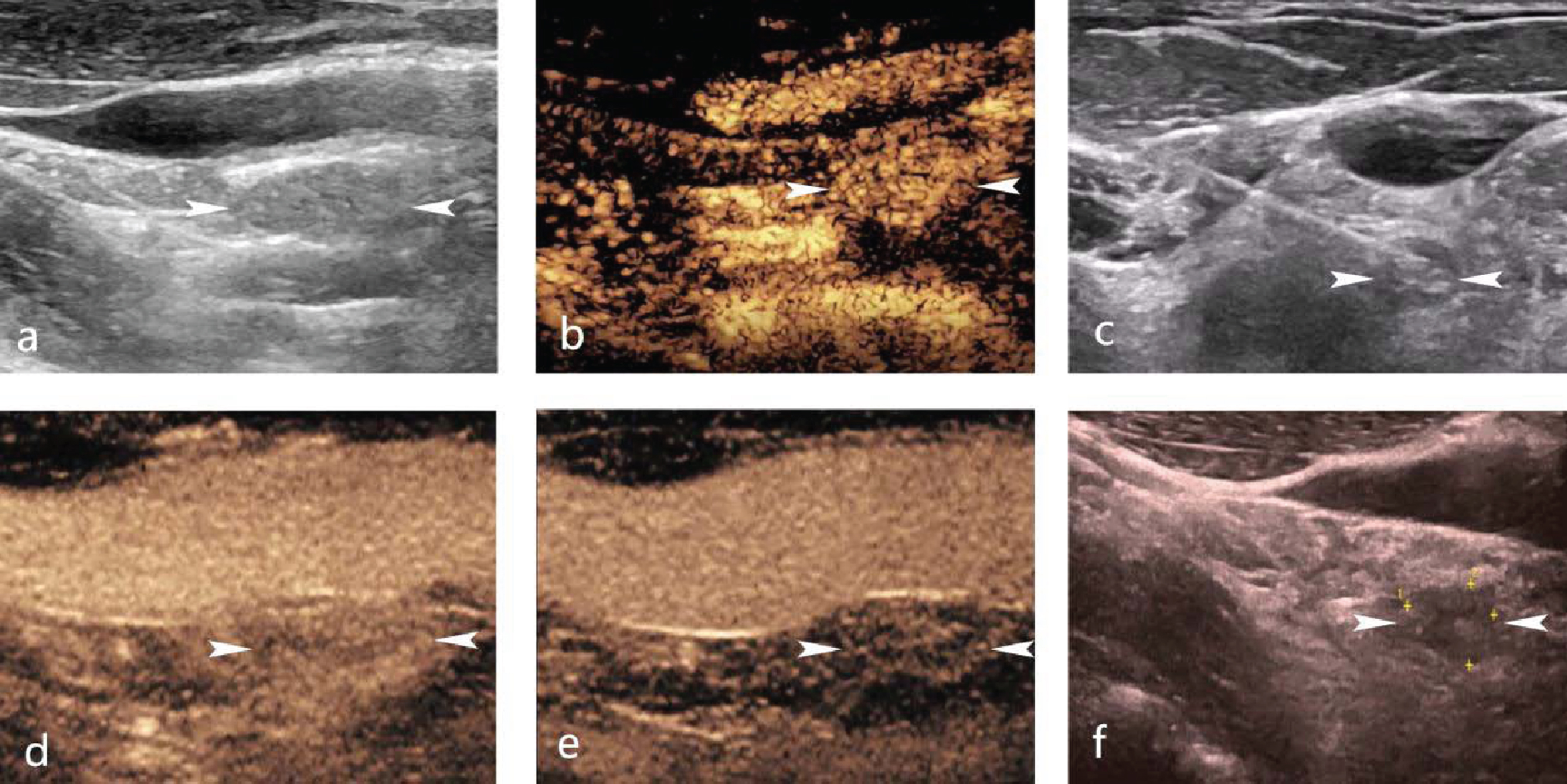
A 41-year-old man received MWA of metastatic LNs from PTC 10 years after total thyroidectomy. Pre-ablation, size 12.8×5.4×8.7 mm (a, arrow), high-enhancement in the early stage (b, arrow). Ablation under real-time US guidance (c, arrow). 1-month post-ablation, size 8.7×5.3×6.0 mm, high-enhancement in the early stage (d, arrow), low-enhancement in the late stage (e, arrow). 7-month post-ablation, size 8.6×5.1×5.2 mm (f, arrow).
In our study population, 74 (93.7%) patients underwent s-Tg examination before treatment and at the last follow-up. For those patients, the level of s-Tg reduced from 9.2 ± 26.6 ng/mL (range, 0.04–144.9 ng/mL) to 3.7 ± 7.0 ng/mL (range, 0.04–33.56 ng/mL). Although a marked reduction was shown, there was no statistical difference in s-Tg level before and after ablation. Besides, the mean follow-up time of s-Tg examination was 10.0 ± 8.1 months (range, 1–24 months).
Safety
There were no serious complications or side effects related to the percutaneous ablation such as bleeding, skin burns or allergic reactions occurred intraoperatively and postoperatively. The ablation procedures were well tolerated in all patients.
Discussion
Minimally invasive surgery, as a new trend in clinical practice, has the advantages of early postoperative recovery, minimal wound extension for cosmetic effect, and few postoperative complications [16]. In addition, several emerging techniques, such as laser ablation (LA), RFA and MWA have pushed the development of minimally invasive surgery. With these techniques, it is theoretically feasible to take minimally invasive surgery one step further in terms of reducing recovery time, pain, and scarring in patients. Although nowadays these emerging techniques have been widely used in the treatment of benign and malignant tumors, complete assessments of their safety and efficacy are still limited [9, 17]. Therefore, in this present study, we shared our experience and further evaluate the efficacy and safety.
In clinical practice, repeated surgery aimed at cervical metastatic LNs is very difficult to perform especially for patients who had already underwent two or more times of neck surgical resections, due to sever fibrosis and distortion of normal tissue planes secondary to postoperative scar formation [7]. Besides, I131 is an another therapy for metastasis LNs from PTC [18]. However, the radioisotope is expensive and involves radiation, which limits its widespread use, especially in basic hospitals. And there are also some lesions that do not absorb iodine [19]. In response to this problem, ablation has been recommended as an alternative by the guidelines of ATA [7]. Some researches have reported that, MWA/RFA, as novel ablation techniques, can achieve larger and faster ablation by using higher temperature compared with LA [20, 21]. Therefore, MWA/RFA, as a less invasive and practical therapeutic strategy, was the best choice, mainly because of less postoperative affection and good efficacy.
Obviously, the results of this present study indicated that MWA/RFA was an effective modality for the treatment of metastatic LNs from PTC. Some similar results have been reported in other studies. For example, Guang et al. reported that, after RFA, 33 (61.1%) metastatic LNs completely disappeared and 21 (38.9%) remained as small scar-like lesions at the last follow-up visit with a mean follow-up of 21 ± 4 months (range, 12–24 months) [22]. Besides, in the study conducted by Zhou et al., the average largest diameter of 21 ablated LNs by MWA was reduced from 10.1 ± 4.7 mm (range, 3.1–20.0 mm) to 0.9 ± 1.6 mm (range, 0–4.1 mm; p < 0.05) with a mean follow-up time of 8.4 ± 4.1 months (range, 3–18 months) [23]. Teng et al. reported VRR of 95.45±8.60% (range, 59.83–100%), 99.34±2.85% (range, 86.10–100%) and 100% in 6, 12, and 18 months after MWA [13].
However, during follow-up, we found a case of incomplete ablation and could not confirm what was the exact cause of this case, such as the operator’s negligence or improper operation, post-ablation inflammatory reaction, calcification in the initial LN, or tumor recurrence [24]. Although no significant progress was observed, close follow-up observation was needed. It also made sense that CEUS has an important prognostic value because CEUS can better reflect blood perfusion of the ablated area [25–27]. Therefore, it is necessary to perform CEUS immediately after ablation and during follow-up. Besides, 4 (5.1%) LNs became bigger than before. Among them, CEUS were performed in the two LNs about one month after ablation and no enhancement were showed. Considering no significant progress or signs of recurrence were observed, extended area might be caused by unabsorbed ablation zone or inflammatory edema except for small measuring error [20].
In addition, compared with the extent of reduction in size, it seemed that MWA/RFA did not perform well in decreasing the level of s-Tg. S-Tg, as one of the most valuable biomarkers in thyroid diseases treatment and prognosis, also indicates the efficacy of metastatic LNs ablation after total thyroidectomy for PTC [28]. In the study conducted by Cao et al., which enrolled 14 patients with 38 cervical metastatic LNs treated by MWA, s-Tg level at the last follow-up (median 1.25 ng/mL) was significantly lower than the pre-ablation level (median 8.35 ng/mL) [29]. Significant decrease in s-Tg level after ablation usually indicates complete inactivation of the metastatic LNs [30]. But for patients who had only subtotal thyroidectomy, few s-Tg can be produced by the residual thyroid tissue and it may lead to the decrease of s-Tg prognostic value in the subsequent LNs ablation. That might be one of the main reasons why there was no statistical difference in s-Tg level before and after ablation in this study. Even so, it was necessary to monitor s-Tg level regularly before and after ablation, for the purpose of achieving better evaluation of the post-ablation efficacy.
The present study also had the following limitations. Firstly, verification bias might have occurred because the diagnosis of US guided-FNAB was limited to 1–3 suspected LNs. But quite a few patients were ablated three more LNs. Secondly, we did not provide comparison with repeated surgical resections or other less invasive alternatives. Therefore, a future prospective study involving different treatment techniques needs to be performed. Thirdly, the sample size in this present study was small and the follow-up period was relatively short for this slowly progressing disease. Accordingly, it was needed to follow-up these patients continuously and then evaluate the long-term outcomes.
Conclusion
Thermal ablation was an effective and safe modality for the treatment of metastatic LNs from PTC, and provided an alternative therapeutic strategy especially for patients who had previous surgical resections.
Footnotes
Acknowledgments
We sincerely thank all the patients who have participated in this study. We thank each of the authors for their efforts in research design, data collection and text writing. The authors gratefully acknowledge the precious guidance provided by Prof. Huixiong Xu at every stage of this paper.
Conflict of interest
No conflict of interest exits in the submission of this manuscript, and manuscript is approved by all authors for publication.
Funding
This research was financially supported by National Natural Science Foundation of China (Grants No. 82202154), Science and Technology Commission of Shanghai Municipality (Grants No. 19DZ2251100) and Shanghai Municipal Health Commission (Grants No. 2019LJ21 and SHSLCZDZK 03502).