Association between tumor necrosis factor-alpha gene rs1800629 ( - 308G/A) and rs361525 ( - 238G > A) polymorphisms and prostate cancer risk in an Iranian cohort
Available accessResearch articleFirst published online February, 2020
Association between tumor necrosis factor-alpha gene rs1800629 ( - 308G/A) and rs361525 ( - 238G > A) polymorphisms and prostate cancer risk in an Iranian cohort
Prostate cancer (PCa) as the first men’s common cancer in the world and the third cancer in Iranian men is a heterogeneous disorder which sometimes several biopsies are needed for its diagnosis.
OBJECTIVES:
The aim of current study is finding new biomarkers in order to diagnose of PCa at the earliest possible stage. Hence, the relationship between rs1800629 and rs361525 polymorphisms of TNF- gene with PCa was investigated.
MATERIALS AND METHODS:
Blood DNA samples were collected from 100 patients with PCa, 110 with BPH, and 110 controls. Collected samples were examined using PCR-RFLP and Tetra-ARMS-PCR techniques to detect the desired polymorphisms.
RESULTS:
The frequency of rs1800629 genotypes in smokers was significantly different from non-smokers with PCa ( 0.001). Logistic regression analysis results showed that GA heterozygotes in comparison to GG homozygotes had higher risk of developing Benign Prostatic Hyperplasia (BPH) or prostate cancer. However, no significant correlation was considered between the risk of PCa and the TNF- gene polymorphisms (rs1800629 and rs361525).
CONCLUSIONS:
Although, the achieved results of this investigation demonstrated that the two examined genetic variants do not seem to be suitable markers for early diagnosis of prostate cancer in this pilot study; however increased risk for the disease is shown in GA heterozygotes and smokers which is indicative of some epigenetic factors influence on prostate cancer etiology.
The prostate is the largest accessory gland of the male reproductive system and the organ associated in Prostate cancer (PCa), Benign prostatic hyperplasia (BPH), and Prostatitis [1, 2]. The prostate cancer, is the second most common malignancies in men all over the world and the third common cancer among Iranian males [3]. It is a heterogeneous disorder as a normal age-related phenomenon [4] and rare amongst men younger than 40 years [5] which includes 7–9 percent of all cancers in Iran where most cases occur over 50 years of age [6]. Risk factors such as age, ethnicity/race, familial inheritance, and lifestyle may induce PCa growth in addition to genetic and epigenetic factors [7]. There are many clinical tests which have been used to diagnose the prostate cancer including the prostate-specific antigen (PSA) blood test [8], digital rectal exam (DRE) [9], magnetic resonance imaging (MRI) [10], sonography [11], and prostate biopsy (Gleason scoring) [12]. The above-mentioned clinical tests have their own disadvantages. For instance, information obtained from a single biopsy is not sufficient to diagnose and guide treatment decisions due to the heterogeneity of the prostate tissue [13]. So, the current study was carried out to determine new biomarkers for early diagnosis of PCa.
Genetic up to 42% and/or epigenetic alterations affect PCa through changing in the gene transcription and function in many malignancies [14]. Recent studies suggest that genetic polymorphisms in cytokines might be associated with increasing cytokine production and inflammation and eventually increasing prostate cancer risk [15].
Tumor necrosis factor alpha (TNF-), as a pro-inflammatory cytokine, which is secreted by various types of cells such as macrophages, T cells, and natural killer (NK) cells [16], plays significant roles in the pathogenesis of several diseases [17]. TNF- activates oncogenic transcription factors such as NF-kB and AP-1 [18] which accelerate cell proliferation, inflammation reaction, and anti-apoptotic activity. The prolonged inflammation in prostate tissue and escape from immune response may increase the fortuity of initiation and progression of cancer [19, 20, 21]. The TNF- protein induces the expression of adhesion molecules and invasion of metastatic tumor cells [22].
Moreover, TNF- gene is located in the class III region of the major histocompatibility complex (MHC III) on chromosome 6p21.3 [23] with 4 exons [24] and has significant roles in the regulation of differentiation, death, innate, and adaptive immune responses. Any impairment in the gene structure may associate with a variety of human diseases like infectious, cancer, autoimmune, etc. [25]. Several single nucleotide polymorphisms (SNPs) of the gene have been associated with susceptibility to several cancers including the breast, stomach, lung, and prostate cancers [26, 27, 28, 29]. rs1800629 is one of the most common polymorphisms with a G to A transition at 308 (TNF-308G/A) nucleotide upstream from the transcription initiation site in the promoter region, that can affect the TNF- levels [30]. The other common polymorphism which is located at 238 of the same promoter is rs361525 where a G to A substitution is happened (TNF--238G/A) and possibly affects the expression levels of TNF- [31]. Previous data have shown that these polymorphisms are considered as significant modifiers of transcription activation and are associated with increased release of TNF-. Therefore, it is assumed that TNF- polymorphism may be positively related to BPH and prostate cancer risk [32].
Hence, the current case-control study was done to investigate any association of TNF-a gene variants (rs361525 and rs1800629) with increasing the risk of the disease in a group of Iranian population.
Materials and methods
Subjects
In this study, blood samples include 100 PCa patients, 110 BPH, and 110 healthy individuals which were collected from the Pathology Department, Shohada-e Tajrish hospital. All participants provided a personal questionnaire including body mass index (BMI), PSA level, smoking consumption, family history of cancer, and detailed medical history. All participants had over 45 years old [33] and were matched by age.
Patients were selected based on the pathological findings including high PSA level and tissue biopsy with or without a family history of the disease. BPH group was selected according to the digital rectal examination (DRE), prostate volume (more than 30 ml), and urologist’s opinion (based on symptoms) without any history of malignancy and cancer. Patients with prostate volume less than 25 cm were not selected for BPH group. Healthy subjects were selected based on healthy prostate through clinical and paraclinical examinations such as DRE and PSA levels ( 4 ng/ml) and no personal or family history of PCa or BPH. The recipients of any hormone/chemotherapy, and/or radiotherapy were excluded from the study. All participants provided written informed consent.
Primers sequences, PCR conditions, and fragment sizes for genotyping of the TNF- gene polymorphisms
95–5 min 95–30 sec 71.5–25 sec 38 cycles 72–20 sec 72–7 min
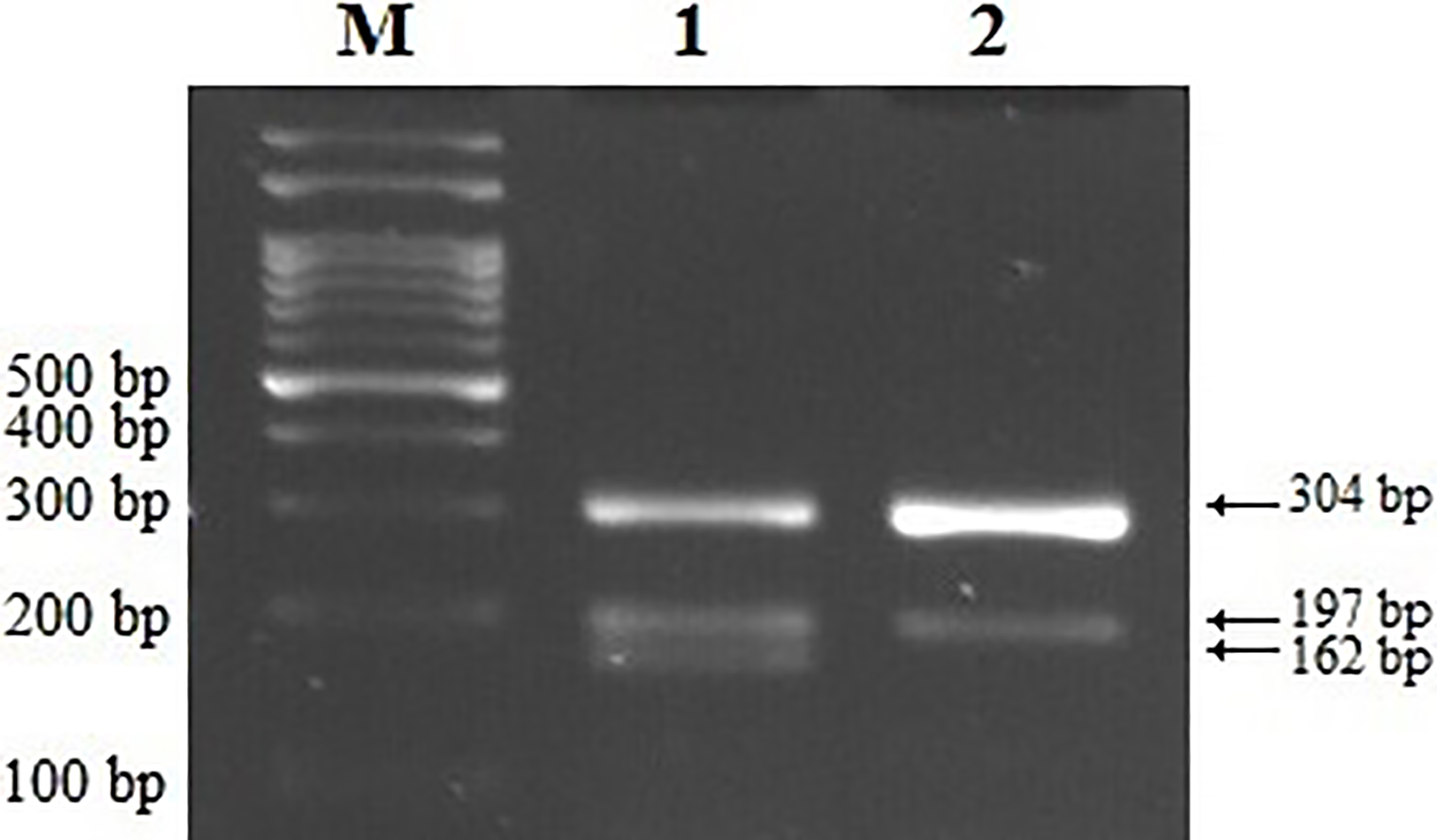
G allele: 304 197 bp A allele: 304 162 bp
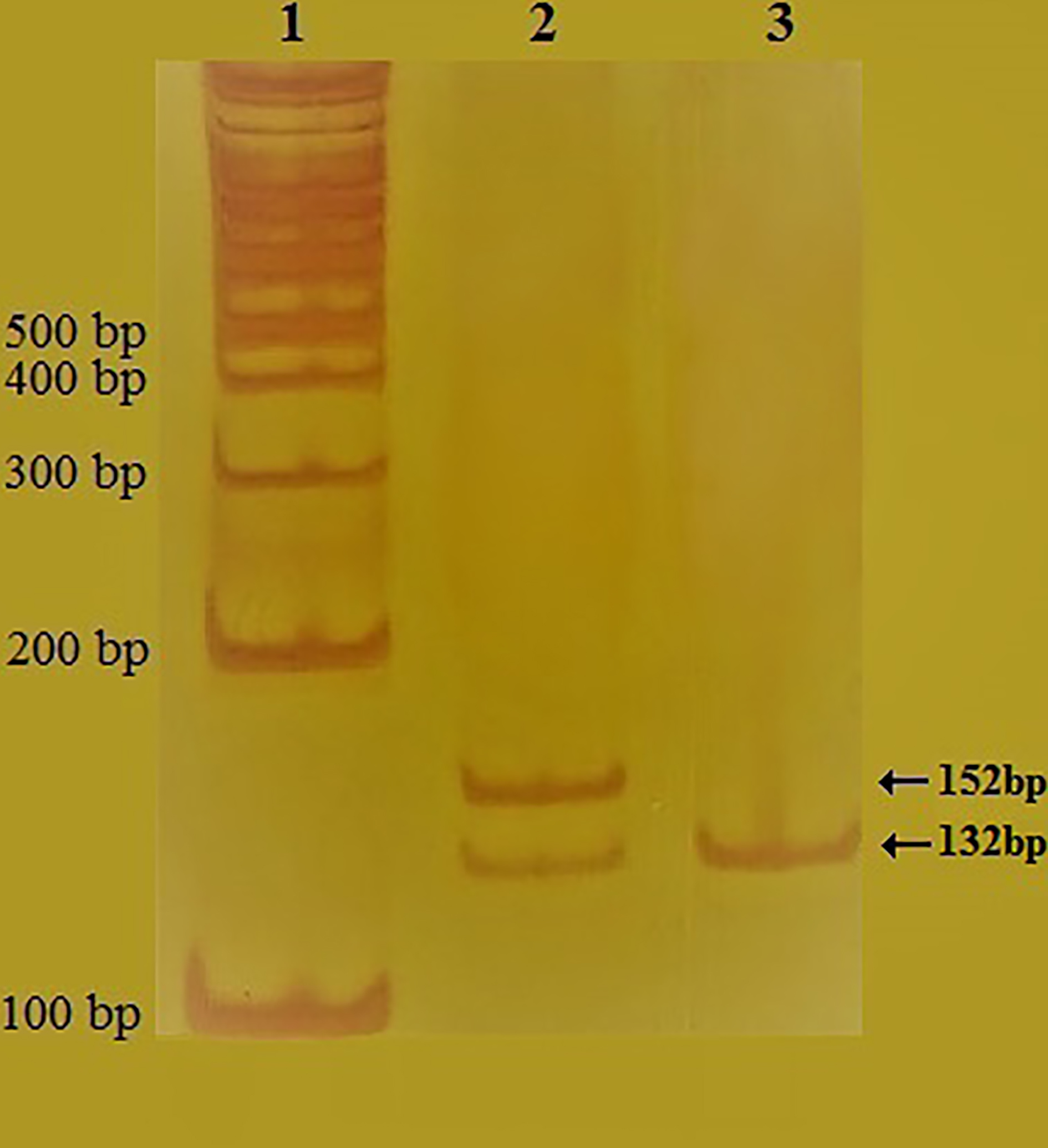
The electrophoresis analysis of TNF- promoter region amplified PCR product. A fragment of 152 bp indicates TNF- rs361525 on 2% agarose gel M: 50 bp DNA marker, S1 and S2: two examined samples.
Polyacrylamide gel electrophoresis analysis of rs361525 polymorphism genotypes of the TNF- gene on 12% polyacrylamide gel (PAGE) after PCR-RFLP amplification of the DNA samples and digestion by MspI restriction enzyme. Column 1: 100 bp DNA ladder, Column 2: GA heterozygote (152, 132 and 20 bp), Column 3: GG homozygote (132 and 20 bp). The 20 bp fragments are not visible due to the short length in both columns. However, the sequencing of the larger fragments confirmed the separation of the 20 bp genomic segment from it.
DNA extraction
Genomic DNA of peripheral blood samples was extracted using salting-out method. Nanodrop spectrophotometer and 1% agarose gel electrophoresis were used to measure the concentration, degree of purity, and protein contamination status of the DNA and evaluate its quality.
The sequencing result of TNF- rs361525 gene polymorphism PCR products. A: The homozygous GG genotype indicates the presence of the wild allele G. B: The heterozygous GA genotype contains two alleles A and G, respectively.
Genotyping of rs361525 polymorphism
TNF- gene promoter 238G/A (rs361525) polymorphism was detected by PCR-RFLP according to Özhan et al. [34]. Primer sequences and PCR conditions for this SNP are listed in Table 1. PCR reactions were performed using 1 l (100 ng) of genomic DNA, 0.5 l (10 pMol) of each primer (Bioneer, South Korea), 8 l of Taq DNA Polymerase 2x Master Mix RED (Ampliqon, Denmark), and 8 l of ddHO. Moreover, PCR amplification was accomplished by thermal cycler PCR (SimpliAmp Thermal Cycler, ABI, USA). In the next step, PCR products were analyzed by 2% of agarose gel electrophoresis containing 4 l of gel stain (SMOBIO, Taiwan) and was examined on gel documentation apparatus (UVIdoc HD5, UVItec Cambridge, UK). The PCR products of 152 bp fragments were considered alongside a 50 bp of DNA Ladder (SMOBIO, Taiwan), as shown in Fig. 1. Afterwards, the PCR products were digested by MspI restriction enzyme (Fermentas, Hunover, MD, USA) at 37C for 16 h and then separated by polyacrylamide gel electrophoresis (PAGE, 12%), beside a 100 bp marker (SMOBIO, Taiwan), and then was stained with silver nitrate and visualized under a UV Transilluminator (VILBER lourmat). According to the Fig. 2, three genotypes were identified after the digestion which are including two 152 bp fragments (attributed to the AA genotype), two fragments of 132 bp/20 bp (the GG genotype), and three different fragments of 152/132/20 bp bands (the GA genotype). Finally, some of the PCR products of each genotype were randomly sequenced to confirm PCR-RFLP results (Genomin Company, Iran), as shown in Fig. 3.
Electrophoresis view of Tetra-ARMS-PCR generated fragments. Different TNF-308G A gene polymorphism genotypes of undergoing examination subjects are observed in columns 1 and 2. From left to right: M: DNA marker; 1: Heterozygous GA genotype (304,197 and 162 bp); 2: Homozygous GG genotype (304 and 197 bp).
Demographic and clinical characteristics of the studied groups
Control ( 110)
BPH ( 110)
PCa (100)
value
Characteristics
Age
66.28 8.43
67.43 8.6
67.78 8.17
0.396
PSA (ng/ml)
1.67 0.87
5.81 4.05
20.75 29.19
0.001
BMI
24.12 4.14
25.07 3.45
25.07 3.67
0.104
Smoking status
Non smokers
71 (64.5%)
61 (55.5%)
56 (56%)
0.312
Current or former smokers
39 (35.5%)
49 (44.5%)
44 (44%)
Prostate volume
Not available
62.69 23.48
50.01 24.24
0.001
Gleason score
6
NA
NA
50 (50%)
6
NA
NA
50 (50%)
Significant values are shown in bold. Mean SD, Not applicable.
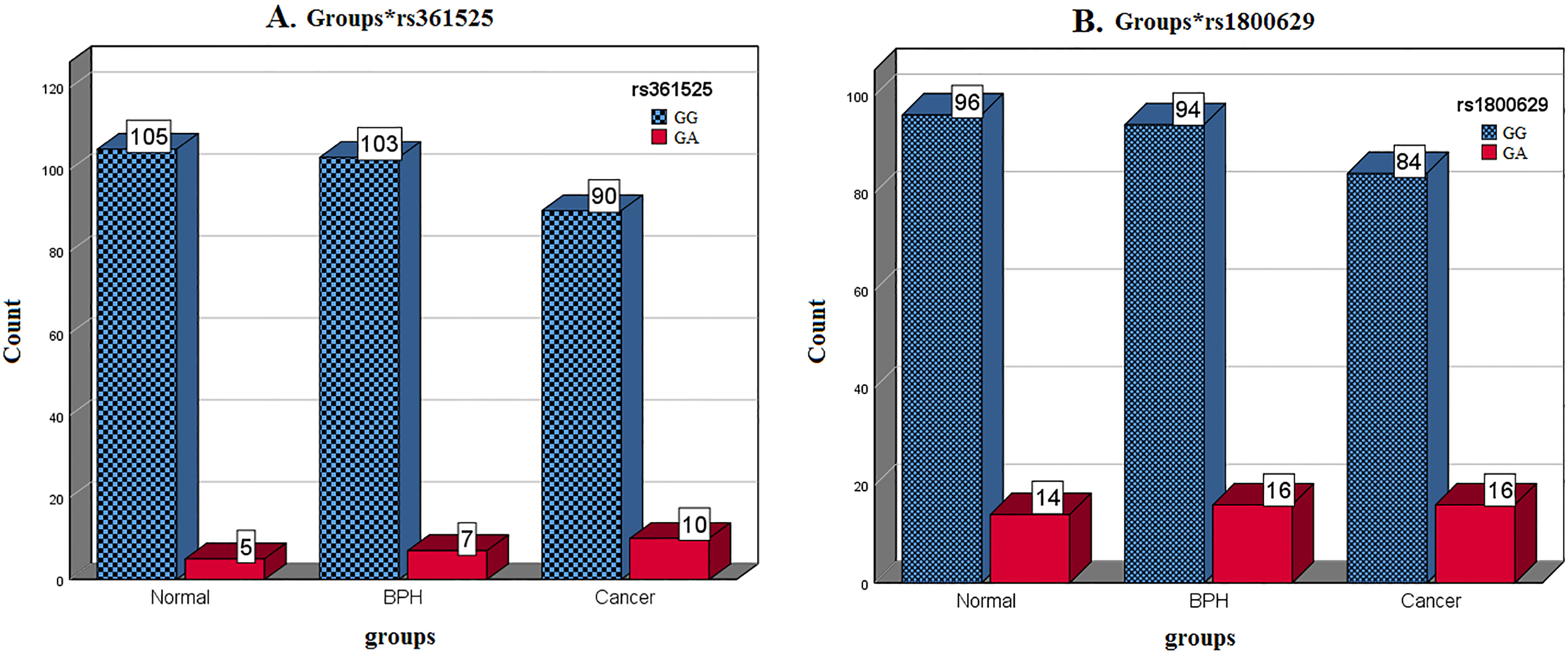
The frequency of genotypes in the understudy groups for the TNF- polymorphisms. A: rs361525 and B: rs1800629.
Genotyping of rs1800629 polymorphism
TNF- gene promoter 308G/A (rs1800629) polymorphism was investigated using Tetra-ARMS-PCR according to Solhjoo et al. [35]. The sequences of used primers and PCR conditions for this SNP are presented in Table 1. PCR reactions were prepared using 2 l (100 ng) of genomic DNA, 0.2 l of forward outer primer, 0.2 l of revers outer primer, 0.7 l of forward inner primer, 0.7 l of reverse inner primer (10 pMol each primer) (Bioneer, South Korea), 10 l of taq DNA Polymerase 2x Master Mix RED, and 10 l of ddHO. PCR was carried out using FlexCycler (Analytic Jena, Germany). The PCR products were analyzed by 2% agarose gel containing 4 l Gel stain and 100 bp of DNA marker and were detected by a UV transilluminator. The PCR products including 304/162 bp fragments (homozygote AA genotype), those with bands of 304/197/162 bp (GA heterozygote genotype), and samples with 304/197 bp bands (homozygote GG genotype) were shown in Fig. 4.
Statistical analysis
We used Chi-square test () to compare the frequency of genotypes and alleles in three studied groups to investigate the association between the two polymorphisms genotypes to analyze the demographic data and the Hardy-Weinberg equilibrium. -values less than 0.05 were considered as statistically significant. Multivariable logistic regression test was used to compute the odd ratio (OR) with 95% confidence interval (CI). All analyses were performed using SPSS v.25 software.
Association between the genotypes of polymorphisms with demographic information
rs1800629 (%)
-value
rs361525 (%)
-value
GG
GA
GG
GA
Normal
Age
70
67
(83.8)
13
(16.3)
0.070
75
(93.8)
5
(6.3)
0.161
70
29
(96.7)
1
(3.3)
30
(100)
0
(0)
BPH
Age
70
60
(84.5)
11
(15.5)
0.704
67
(94.4)
4
(5.6)
0.672
70
34
(87.2)
5
(12.8)
36
(92.3)
3
(7.7)
Cancer
Age
70
53
(81.5)
12
(18.5)
0.360
61
(93.8)
4
(6.2)
0.081
70
31
(88.6)
4
(11.4)
29
(82.9)
6
(17.1)
Normal
PSA
4
96
(87.3)
14
(12.7)
–
105
(95.5)
5
(4.5)
–
BPH
PSA
4
37
(82.2)
8
(17.8)
0.632
44
(97.8)
1
(2.2)
0.199
4–10
45
(86.5)
7
(13.5)
48
(92.3)
4
(7.7)
10
12
(92.3)
1
(7.7)
11
(84.6)
2
(15.4)
Cancer
PSA
4
6
(75.0)
2
(25.0)
0.304
7
(87.5)
1
(12.5)
0.577
4–10
32
(91.4)
3
(8.6)
33
(94.3)
2
(5.7)
10
46
(80.7)
11
(19.3)
50
(87.7)
7
(12.3)
Normal
Smoke
Yes
35
(897)
4
(10.3)
0.564
37
(94.9)
2
(5.1)
0.828
No
61
(859)
10
(14.1)
68
(95.8)
3
(4.2)
BPH
Smoke
Yes
42
(857)
7
(14.3)
0.945
45
(91.8)
4
(8.2)
0.488
No
52
(852)
9
(14.8)
58
(95.1)
3
(4.9)
Cancer
Smoke
Yes
31
(705)
13
(29.5)
0.001
37
(84.1)
7
(15.9)
0.081
No
53
(946)
3
(5.4)
53
(94.6)
3
(5.4)
BPH
Volume
30
5
(71.4)
2
(28.6)
0.512
7
(100)
0
(0)
0767
31–70
62
(87.3)
9
(12.7)
66
(93.0)
5
(70)
70
27
(84.4)
5
(15.6)
30
(93.8)
2
(63)
Cancer
Volume
30
20
(83.3)
4
(16.7)
0.501
23
(95.8)
1
(42)
0387
31–70
49
(81.7)
11
(18.3)
52
(86.7)
8
(133)
70
15
(93.8)
1
(6.3)
15
(93.8)
1
(63)
Significant values are shown in bold.
Multivariable logistic regression in comparing BPH and PCa patients relative to the healthy group
Variable
BPH
PCa
-value
OR (95% CI)
-value
OR (95% CI)
rs1800629 (GA vs. GG)
0.47
1.47 (0.5–4.29)
0.39
2.30 (0.33–15.88)
rs361525 (GA vs. GG)
0.94
1.06 (0.16–6.72)
0.19
4.30 (0.48–38.37)
Age
0.64
0.99 (0.94–1.03)
0.28
1.03 (0.96–1.11)
BMI
0.03
1.10 (1.0–1.21)
0.08
1.13 (0.98–1.31)
PSA
0.001
2.74 (2.03–3.69)
0.001
3.19 (2.17–4.68)
Smoke (Yes vs. No)
0.49
1.30 (0.61–2.76)
0.74
0.81 (0.24–2.74)
Significant values are shown in bold.
Results
Characteristics of subjects
The demographic and clinical characteristics of the studied subjects are summarized in Table 2. The mean age of control, PCa, and BPH group was 66.28, 67.43, and 67.78 years ( 0.396), respectively. The mean of total serum PSA level was significantly higher in PCa (20.75 ng/ml) and BPH (5.81 ng/ml) than in healthy individuals (1.67 ng/ml) ( 0.001). Furthermore, there was no significant difference for the BMI index ( 0.104) and smoking status ( 0.312) but the prostate volume was significantly higher in the BPH patients among three under study groups ( 0.001).
Frequency analysis
The comparison between genotype frequencies of rs361525 and rs1800629 polymorphisms are presented in Fig. 5. Based on the Fig. 5, there was no significant difference in the distribution of genotypes among the three groups for each SNP. Besides, none of the samples had AA genotype of the polymorphisms. In addition, since none of the SNPs were in the equilibrium, we were not able to do a haplotype study.
Association between the SNPs genotypes and demographic information
Based on the Table 3, there is no correlation between age, PSA level, prostate volume, and rs1800629/ rs361525 genotypes in the studied groups ( 0.05).
While the relative frequency of each rs1800629 genotype was not significantly different between smokers and non-smokers of the BPH and healthy groups ( 0.05), this value was significantly different in all studied smokers and non-smokers ( 0.001).
Multivariable logistic regression
To match the variables, all quantitative and qualitative changeable and the studied polymorphisms evaluated by the multivariable logistic regression modeling. A comparison between the odds ratio (OR) for all individuals is indicated in Table 4.
The higher BMI showed to be statistically related to 10% increased chance of having BPH [ 0.03; OR 1.10; 95% CI (1.0–1.21)]. In addition, increased PSA was related to up to 2.74 times statistically higher chance of having BPH [ 0.001; OR 2.74; 95% CI (2.03–3.69)] and the 3.9 times increased risk of cancer [ 0.001; OR 3.19; 95% CI (2.17–4.68)].
Discussion
Prostate cancer is a multifactorial disease in which genetics and environmental factors are involved [36]. The etiology of PCa is unclear [37] but some polymorphisms of anti-inflammatory and pro-inflammatory cytokine genes regulatory regions affect the gene function [25]. PCa has tumor heterogeneity nature and numerous genes are revealed in its etiology. Therefore, looking for genomic variations as new potential biomarkers in the blood could enable us to detect the risk of disease before gene expressional changes in the early stage of the disease in a specific population.
TNF- as a key mediator of inflammation has an important role in PCa development [38]. By considering the potency of TNF- promoter rs1800629 and rs361525 SNPs and their gene expression effect, the SNPs were counted as possible functional variants and as new biomarkers for early detection of susceptibility to prostate cancer.
A meta-analysis results regret to count on TNF--238G/A polymorphism as a risk factor for prostate cancer, while accepts that TNF-308G/A may have a considerable role in the disease risk [15]. Many studies have also shown that the latest variant is associated with TNF- expression level elevation [39]. Lopez and his colleagues studied the effect of the variant on prostate cancer susceptibility and found that the A allele of TNF-A-308 showed 60% increased risk of PCa in Spain [40]. However, Jang and colleagues had previously reported that the TNF-A-238 polymorphism can play a protective role against cancers [41]. Moreover, many studies have been focused on the association between TNF-A-238 and various types of cancers [42]. Bandil and colleagues showed that either TNF--238G A or a haplotype of GA-AA were associated with the development of PCa and BPH. They also found a higher risk for smokers of TNF- SNP haplotypes [25].
The prostate cancer is an age-dependent phe- nomenon which increases with age [43]. Some researches indicate no difference in the distribution of genotype between younger and older control groups, while others have reported an age-related difference of the polymorphisms of specific genes [40]. In the present study, the mean age of the healthy group, BPH and prostate cancer patients did not show any significant difference which confirms that the age alone cannot be a cause of the prostate disease and its malignancies.
Kesarwani and colleagues showed that the PSA concentration was significantly different in the healthy group and PCa patients [44]. Other study showed that the PSA level was higher than normal (4 ng/ml) in cancer patients compared to patients with BPH [25]. Our study also showed that the PSA level increases 2.47 and 3.9 times in BPH and prostate cancer groups in comparison to the controls. Therefore, PSA while not enough but is still an important factor in determining the benign and malignant status from a healthy condition.
On the other hand, while our study showed a 10% gain between increasing BMI and the risk of the disease, some articles have reported a lack of correlation between the increase of BMI and prostate cancer [45]. Therefore, it seems that BMI parameters should be more considered regarding prostate diseases, especially in the context of the cancer.
Tobacco and alcohol consumption may play critical roles in the etiology of many cancers including PCa [46, 47].
Some studies have been reported that smoking and alcohol drinking suppresses TNF- production which adversely affect the immune response in inflammatory and infectious diseases and contributes to the incidence of cancers [48, 49, 50]. There are other sources that do not report any significant association between TNF-a 308G/A polymorphism and PCa risk in smokers compared to non-smokers [42]. In the current study, it was shown that the GA genotype of rs1800629 polymorphism has a higher significant incidence in smoker PCa patients than the non-smokers ( 0.001). So, it can be concluded that smoking in interaction with the GA genotype can increase the risk of prostate cancer.
In the actual study, the percentages of rs1800629 GA genotype in the three groups of healthy, BPH, and cancer were 12.7%, 14.5%, 16%, and 14.4% in total (46 out of 320 individuals), respectively. Moreover, the frequencies of rs361525 GA genotype were 4.5%, 6.4%, 10%, and in total 6.9% (22 out of 320 individuals), respectively. Analysis of the polymorphisms in the studied groups showed that although the frequencies of GG and GA genotypes had no significant differences, their relative frequencies were significantly different and GA showed a possible dominant model which could be a methylation-related site where the methylation level increases [51]. We had no AA genotype in this pilot study which indicates low frequency of A allele in the studied population. Investigation on a larger population may indicate the exact frequency of A allele of the studied TNF- polymorphisms in the future and will overcome the understanding of the SNPs mechanism of actions in the etiology of the prostate cancer.
Conclusions
Our study indicates that there is no significant association between TNF- gene (rs361525 or rs1800629) variant with the risk of BPH and PCa. However, we realized that GA genotype of the examined polymorphisms in comparison to the GG genotype increases the risk of BPH and PCa while the other variables do not show significant differences between the understudy groups ( 0.05) but, still, a potential association is considered between them (OR 1) which could be more interpreted for their possible PCa risk factor role. Hence, studies with a larger number of samples should be done to reveal the existence of the probable associations.
Footnotes
Acknowledgments
Special thanks to Dr. Seyed Ali Ziai the research deputy of the faculty of medicine at Shahid Beheshti University of Medical Sciences for authorizing the project performance at the Central Laboratory. Our sincere thanks to Dr. Seyed Mostafa Hosseipour mashkani from UTS University, Australia, for reviewing the article and submitting his suggestions, and appreciate to those who generously presented their blood samples to allow us to exam the research goals. This study was funded by Shahid Beheshti university of Medical Sciences (Grant number: 15139).
Conflict of interest
Farkhondeh Pouresmaeili has received research grants from Shahid Beheshti university of Medical Sciences. The rest authors have no conflict of interest.
References
1.
BhavsarA. and VermaS., Anatomic imaging of the prostate, BioMed Research International2014 (2014).
2.
AaronL.FrancoO.E. and HaywardS.W., Review of prostate anatomy and embryology and the etiology of Benign Prostatic Hyperplasia, Urologic Clinics43 (2016), 279–288.
3.
HabibiM.MirfakhraieR.KhaniM.RakhshanA.AzargashbE. and PouresmaeiliF., Genetic variations in UGT2B28, UGT2B17, UGT2B15 genes and the risk of prostate cancer: a case-control study, Gene634 (2017), 47–52.
4.
TaheriM.PouresmaeiliF.OmraniM.D.HabibiM.SarrafzadehS.NorooziR.RakhshanA.SayadA. and Ghafouri-FardS., Association of ANRIL gene polymorphisms with prostate cancer and Benign Prostatic Hyperplasia in an Iranian population, Biomarkers in Medicine11 (2017), 413–422.
5.
PernarC.H.EbotE.M.WilsonK.M. and MucciL.A., The epidemiology of prostate cancer, Cold Spring Harbor Perspectives in Medicine8 (2018), a030361.
6.
Sadeghi-GandomaniH.YousefiM.RahimiS.YousefiS.Karimi-RozvehA.HosseiniS.MahabadiA.AbarquiH.BorujeniN. and SalehiniyaH., The incidence, risk factors, and knowledge about the prostate cancer through worldwide and Iran, World Cancer Research Journal4 (2017), 1–8.
7.
KaranD.ThrasherJ. and LubaroffD., Prostate cancer: genes, environment, immunity and the use of immunotherapy, Prostate Cancer and Prostatic Diseases11 (2008), 230.
8.
WolfA.HoffmanR.VolkR. and PensonD., Prostate-specific antigen screening for prostate cancer: yes, no, or maybe? The Medical Roundtable General Medicine Edition (2019).
GopinathN., Tumor detection in prostate organ using canny edge detection technique, International Journal of Pure and Applied Mathematics118 (2018), 211–217.
11.
MansouriF., The role of the clinical and molecular assays in prostate cancer detection, Asian Journal of Pharmaceutical and Clinical Research10 (2017), 11–15.
12.
ChenN. and ZhouQ., The evolving Gleason grading system, Chinese Journal of Cancer Research28 (2016), 58.
13.
TosoianJ.J. and AntonarakisE.S., Molecular heterogeneity of localized prostate cancer: more different than alike, Translational Cancer Research6 (2017), S47.
14.
KgatleM.M.KallaA.A.IslamM.M.SathekgeM. and MooradR., Prostate cancer: epigenetic alterations, risk factors, and therapy, Prostate Cancer2016 (2016).
15.
MaL.ZhaoJ.LiT.HeY.WangJ.XieL.QinX. and LiS., Association between tumor necrosis factor-alpha gene polymorphisms and prostate cancer risk: a meta-analysis, Diagnostic Pathology9 (2014), 74.
16.
SchillaciO.ScimecaM.TrivignoD.ChiaravallotiA.FacchettiS.AnemonaL.BonfiglioR.SanteusanioG.TancrediV. and BonannoE., Prostate cancer and inflammation: a new molecular imaging challenge in the era of personalized medicine, Nuclear Medicine and Biology (2019).
17.
El-TahanR.R.GhoneimA.M. and El-MashadN., TNF-α gene polymorphisms and expression, Springerplus5 (2016), 1508.
18.
AggarwalB.B.GuptaS.C. and KimJ.H., Historical perspectives on tumor necrosis factor and its superfamily: 25 years later, a golden journey, Blood119 (2012), 651–665.
19.
BandilK.SinghalP.SharmaU.HussainS.BasuS.ParashariA.SinghV.SehgalA.ShivamA. and AhujaP., Impacts of TNF-LTA SNPs/haplotypes and lifestyle factors on oral carcinoma in an indian population, Molecular Diagnosis & Therapy20 (2016), 469–480.
20.
KohaarI.TiwariP.KumarR.NasareV.ThakurN.DasB.C. and BharadwajM., Association of single nucleotide polymorphisms (SNPs) in TNF-LTA locus with breast cancer risk in Indian population, Breast Cancer Research and Treatment114 (2009), 347.
21.
KorobeinikovaE.MyrzaliyevaD.UgenskieneR.RaulinaityteD.GedminaiteJ.SmigelskasK. and JuozaityteE., The prognostic value of IL10 and TNF alpha functional polymorphisms in premenopausal early-stage breast cancer patients, BMC Genetics16 (2015), 70.
22.
KirkpatrickA.BidwellJ.Van den BruleA.MeijerC.PawadeJ. and GlewS., TNFα polymorphism frequencies in HPV-associated cervical dysplasia, Gynecologic Oncology92 (2004), 675–679.
23.
MotawiT.K.El-MaraghyS.A.SharafS.A. and SaidS.E., Association of CARD10 rs6000782 and TNF rs1799724 variants with paediatric-onset autoimmune hepatitis, Journal of Advanced Research15 (2019), 103–110.
24.
HeidariZ.MoudiB.SaghebH.M. and MoudiM., Association of TNF-α gene polymorphisms with production of protein and susceptibility to chronic hepatitis B infection in the south east Iranian population, Hepatitis Monthly16 (2016).
25.
BandilK.SinghalP.DograA.RawalS.K.DovalD.VarshneyA.K. and BharadwajM., Association of SNPs/haplotypes in promoter of TNF A and IL-10 gene together with life style factors in prostate cancer progression in Indian population, Inflammation Research66 (2017), 1085–1097.
26.
StephensK.E.LevineJ.D.AouizeratB.E.PaulS.M.AbramsG.ConleyY.P. and MiaskowskiC., Associations between genetic and epigenetic variations in cytokine genes and mild persistent breast pain in women following breast cancer surgery, Cytokine99 (2017), 203–213.
27.
ZhangX.WangJ.ShaoH. and ZhuW., Function of tumor necrosis factor alpha before and after mutation in gastric cancer, Saudi Journal of Biological Sciences24 (2017), 1920–1924.
28.
EatonK.D.RomineP.E.GoodmanG.E.ThornquistM.D.BarnettM.J. and PetersdorfE.W., Inflammatory gene polymorphisms in lung cancer susceptibility, Journal of Thoracic Oncology13 (2018), 649–659.
29.
WinchesterD.A.TillC.GoodmanP.J.TangenC.M.SantellaR.M.Johnson-PaisT.L.LeachR.J.XuJ.ZhengS.L. and ThompsonI.M., Association between variants in genes involved in the immune response and prostate cancer risk in men randomized to the finasteride arm in the prostate cancer prevention trial, The Prostate77 (2017), 908–919.
30.
DuG.-H.WangJ.-K.RichardsJ.R. and WangJ.-J., Genetic polymorphisms in tumor necrosis factor alpha and interleukin-10 are associated with an increased risk of cervical cancer, International Immunopharmacology66 (2019), 154–161.
31.
WeiB.F.FengZ.WeiW. and ChenX., Associations of TNF-α-238A/G and IL-10-1082G/A genetic polymorphisms with the risk of NONFH in the Chinese population, Journal of Cellular Biochemistry118 (2017), 4872–4880.
32.
DabhiB. and MistryK.N., In silico analysis of single nucleotide polymorphism (SNP) in human TNF-α gene, Meta Gene2 (2014), 586–595.
33.
SadjadiA.NooraieM.GhorbaniA.AlimohammadianM.ZahediM.-J.Darvish-MoghadamS.FakheriH.BabaiM.SemnaniS. and Mansour-GhanaeiF., The incidence of prostate cancer in Iran: results of a population-based cancer registry, Archives of Iranian Medicine10 (2007), 481–485.
34.
ÖzhanG.YanarH.T.ErtekinC. and AlpertungaB., Polymorphisms in tumour necrosis factor alpha (TNF) gene in patients with acute pancreatitis, Mediators of Inflammation2010 (2010).
35.
SolhjooS.Mahmoudzadeh SaghebH.HeidariZ.HashemiM. and Rigi LadezM., Association between TNF-α (-308G > A) gene polymorphism and chronic periodontitis, Zahedan Journal of Research in Medical Sciences16 (2014), 10–14.
36.
MalikS.S.BatoolR.MasoodN. and YasminA., Risk factors for prostate cancer: a multifactorial case-control study, Current Problems in Cancer42 (2018), 337–343.
37.
KimY.H.ByunY.J.KimW.T.JeongP.YanC.KangH.W.KimY.J.LeeS.C.MoonS.K.ChoiY.H.YunS.J. and KimW.J., CDC6 mRNA expression is associated with the aggressiveness of prostate cancer, J Korean Med Sci33 (2018), e303.
38.
LiangG.WangQ.JiangY.WumanerA. and WangQ., Lack of association between TNFα rs1800629 polymorphism and prostate cancer risk: a meta-analysis, Int J Clin Exp Med9 (2016), 9373–9380.
39.
XingB.LiX.K.ZhangS.F.LuQ.B.DuJ.ZhangP.H.YangZ.D.CuiN.GuoC.T.CaoW.C.ZhangX.A. and LiuW., Polymorphisms and haplotypes in the promoter of the TNF-alpha gene are associated with disease severity of severe fever with thrombocytopenia syndrome in Chinese Han population, PLoS Negl Trop Dis12 (2018), e0006547.
40.
Sáenz-LópezP.CarreteroR.CózarJ.M.RomeroJ.M.CantonJ.VilchezJ.R.TalladaM.GarridoF. and Ruiz-CabelloF., Genetic polymorphisms of RANTES, IL1-A, MCP-1 and TNF-A genes in patients with prostate cancer, BMC Cancer8 (2008), 382.
41.
JangW.H.YangY.I.YeaS.S.LeeY.J.ChunJ.H.KimH.I.KimM.S. and PaikK.H., The -238 tumor necrosis factor-alpha promoter polymorphism is associated with decreased susceptibility to cancers, Cancer Lett166 (2001), 41–46.
42.
BerhaneN.SobtiR.C.MelesseS.MahdiS.A. and KassuA., Significance of tumor necrosis factor α-308 (G/A) gene polymorphism in the development of prostate cancer, Molecular Biology Reports39 (2012), 11125–11130.
43.
ZabaletaJ.LinH.-Y.SierraR.A.HallM.C.ClarkP.E.SartorO.A.HuJ.J. and OchoaA.C., Interactions of cytokine gene polymorphisms in prostate cancer risk, Carcinogenesis29 (2008), 573–578.
44.
KesarwaniP.MandhaniA. and MittalR.D., Polymorphisms in tumor necrosis factor-A gene and prostate cancer risk in North Indian cohort, The Journal of Urology182 (2009), 2938–2943.
45.
DanforthK.N.RodriguezC.HayesR.B.SakodaL.C.HuangW.Y.YuK.CalleE.E.JacobsE.J.ChenB.E. and AndrioleG.L., TNF polymorphisms and prostate cancer risk, The Prostate68 (2008), 400–407.
46.
PachecoS.PachecoF.ZapataG.GarciaJ.PrevialeC.CuraH. and CraigW., Food habits, lifestyle factors, and risk of prostate cancer in Central Argentina: a case control study involving self-motivated health behavior modifications after diagnosis, Nutrients8 (2016), 419.
47.
JoshiM.VermaY.GautamA.ParmarG.LakkadB. and KumarS., Cytogenetic alterations in buccal mucosa cells of chewers of areca nut and tobacco, Archives of Oral Biology56 (2011), 63–67.
48.
MianM.F.LauzonN.M.StämpfliM.R.MossmanK.L. and AshkarA.A., Impairment of human NK cell cytotoxic activity and cytokine release by cigarette smoke, Journal of Leukocyte Biology83 (2008), 774–784.
49.
LambertC.McCueJ.PortasM.OuyangY.LiJ.RosanoT.G.LazisA. and FreedB.M., Acrolein in cigarette smoke inhibits T-cell responses, Journal of Allergy and Clinical Immunology116 (2005), 916–922.
50.
HaddyN.SassC.MaumusS.MarieB.DroeschS.SiestG.LambertD. and VisvikisS., Biological variations, genetic polymorphisms and familial resemblance of TNF-α and IL-6 concentrations: STANISLAS cohort, European Journal of Human Genetics13 (2005), 109.
51.
ZhuX.LiR.KangG.KangQ.RaoW.YangM.CaoB.ZhangM.SunY.WangY.ChenX.YuY. and YuQ., CACNA1C polymorphism (rs2283291) is associated with schizophrenia in Chinese males: a case-control study, Disease Markers2019 (2019), 7.