
Abstract
The number of biologic drugs available for the treatment of psoriasis continue to expand. However, being biological proteins and thus potentially immunogenic, there is evidence that anti-drug-antibodies develop against the various therapeutic proteins currently being utilised. Although chimeric antibodies that contain elements of the parental rodent monoclonal antibodies are immunogenic, anti-drug antibodies occur even if the biologic is a fully human protein and these can impact on clinical efficacy and safety. However, there is a wide variation in the reported level of anti-drug-antibodies for the same and different treatments that is highlighting issues with various assays used in anti-drug antibody detection. Here we review the available data on the occurrence of anti-drug antibodies in people with psoriasis treated with biologic agents.
Introduction
Psoriasis is a chronic inflammatory skin condition affecting 125 million people globally [1]. However, its impacts are not limited to the skin, since it is associated with many comorbidities, such as cardiovascular and inflammatory bowel diseases, mental disorders and psoriatic arthritis [2]. While the pathogenesis is complex, the immune system is thought to play a crucial role in disease development [3]. Greater understanding of pathogenesis has facilitated the development of monoclonal antibodies (mAbs) specifically targeting and inhibiting key molecules implicated in the pro-inflammatory pathways, broadening treatment options for those with moderate to severe psoriasis. Although this class of drugs has significantly improved treatment outcomes for patients, their immunogenic potential is of concern, with anti-drug antibodies (ADAs) being produced against them, which impacts on efficacy and patient benefits [3].
There are several types of psoriasis, the most common being plaque psoriasis, which accounts for 80–90% of all cases [3]. This subtype presents as well-defined, raised, red plaques on the skin, which are covered in silvery-white scale, which typically appear on the lower back, knees, scalp and elbows. Thus, those suffering may have a significantly lowered quality of life (QoL) [3]. Despite the involvement of genetic and environmental factors, it is primarily the immune system that dominates in the pathogenesis of psoriasis, with the IL-23/Th17 pathway at the centre of disease progression [4], which can be modulated by a number of therapeutic antibodies as illustrated in Fig. 1.
The pathogenesis of psoriasis and therapeutic cytokine targeting by biological disease modifying agents.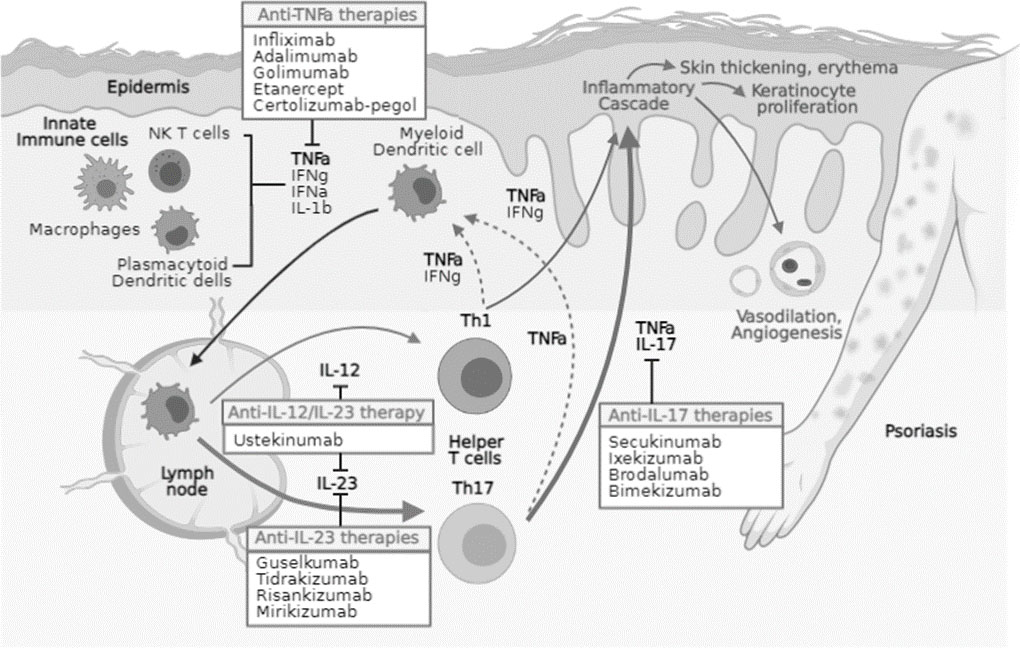
Innate immune cells including: natural killer (NK) T cells, macrophages, plasmacytoid dendritic cells and keratinocytes, activate myeloid dendritic cells. The latter act as antigen presenting cells and secrete IL-12 and IL-23, which facilitates T cell differentiation into Th1 and Th17 cells respectively. On activation, Th17 cells produce tumour necrosis factor
Given the chronic nature of psoriasis, the main goal of treatment is to achieve and maintain remission, through controlling the inflammatory process and reducing plaque formation. The choice of treatment depends on the severity of psoriasis and its impact on the quality of life (QoL) [5]. Topical therapies, the primary treatment for mild psoriasis, are available in a variety of formulations, including creams, lotions and ointments. The type used depends on patient preference and area needing coverage. Phototherapy, conventional (non-biologic) systemic therapies and apremilast are reserved for more moderate to severe cases [6]. There are a plethora of drugs used in psoriasis treatment (Table 1).
Current psoriasis treatments: Treatments, their indicated disease severity, mechanism of action and side-effect profile
Current psoriasis treatments: Treatments, their indicated disease severity, mechanism of action and side-effect profile
Research advances in understanding psoriasis pathophysiology has allowed for the introduction of biologics, a class of drugs highly effective in treating moderate to severe psoriasis. Biologics are mAbs, fusion proteins or antibody fragments, which specifically target the pro-inflammatory cytokines involved in psoriasis (Fig. 1), aiming to reduce the side effects typically seen from using the aforementioned drug (Table 1) therapies [7].
Anti-TNF-
Anti-psoriatic biological therapeutic agents
Anti-psoriatic biological therapeutic agents
Despite Mirikizumab meeting the primary and all key secondary endpoints versus placebo at Week 16 and all key secondary endpoints versus Cosentyx
Since biologics are proteins, they may give rise to ADAs and thus are considered to be potentially immunogenic. These ADAs can be classified as either binding antibodies (BAbs) or neutralising antibodies (NAbs). The latter reduces drug functionality through binding to the active site of the drug, consequently inactivating it. BAbs attach to non-active site regions, forming an immune-complex with the biologic which promotes its clearance [10]. Hence, the presence of these ADAs can reduce drug efficacy, diminishing the therapeutic effects seen in people with psoriasis. There is growing evidence that a variety of factors are involved in ADA formation. These can be generally classified into drug-related, patient-related and treatment-related factors. Within drug-related factors, the molecular structure of biologics is thought to be a key determinant of immunogenicity [11]. Murine antibodies were the first therapeutics used in oncology treatment but demonstrated high immunogenicity since they were rodent-derived [12, 13]. This led to the development of mAbs composed of human constant regions and murine variable regions, termed chimeric antibodies, such as infliximab. Although this reduced immunogenicity, ADAs were still predicted to occur [14]. Hence, humanisation [15] was implemented, where the variable regions were humanised to contain only the complementarity determining regions of the original rodent antibody in humanized antibodies such as Campath-1H. However, even humanised antibodies are in some individuals immunogenic and give rise to ADA formation [16] and reduce the efficacy of treatment [17]. Despite theoretically possessing a reduced immunogenic potential, even fully human mAbs produce ADAs, which are of anti-idiotypic in nature [18]. Patient characteristics may further influence the production of ADAs. Genetic factors may influence how the immune system responds to biologics, creating variability amongst patients. Similarly, patients may respond differently to biologics depending on their age. Those suffering from chronic infections may have an enhanced immune response, increasing their likelihood of developing ADAs in comparison to those with impaired immune function. Additionally, prior exposure to similar proteins may pre-sensitise and induce immune responses in patients, producing immunological memory which may hinder the therapeutic benefits of subsequent biologics [19].
The treatment protocol can also contribute to ADA formation. It has been suggested that biologics are less immunogenic if a higher dose is given continuously over an extended period of time, in comparison to a lower dose delivered intermittently for a shorter period. Administration routes can also affect ADA formation, with intravenous administration deemed less immunogenic than subcutaneous and intramuscular routes [19]. Furthermore, it has been noted that concomitant use of immunosuppressants can aid in reducing ADA development, with studies showing a lower incidence of ADAs in psoriasis patients receiving concomitant methotrexate [11]. Therefore, it can be appreciated that numerous factors are involved in ADA formation.
Measuring ADA
There are numerous assays available to detect ADAs, though their varying sensitivity and specificity adds to the complexity of measuring ADA levels. Standard assays include conventional radio-immunoassays and enzyme-linked immunosorbent assays (ELISA). However, a major challenge with these formats is drug interference. This occurs when ADAs become bound to the drug, which is present in excess, in an immune-complex, so remain undetected by the assay. Thus, standard assays can only measure free ADA, leading to an underestimation of immunogenicity and false negative results. This raises questions about their sensitivity [11, 20]. However, there are ‘drug tolerant’ assays, examples of which are affinity capture elution assays [21], acid-dissociation radio immunoassay [22], and pH-shift anti-idiotype antigen-binding tests [23], which can help to overcome these challenges. These assays include an acidification step which causes the dissociation of immune complexes, freeing bound ADAs and allowing for their detection [23]. Hence, these assays are more sensitive, which can result in fewer false negative results when used. More recently a sensitive assay has been developed as a generic platform for ADA testing using recombinant reporter which incorporates a dual tandem nanoluciferase between the drug VH and VL domains (GloBody™). The ADA-GloBody complexes are captured on immobilised Protein G and the retained nanoluciferase activity determined [24]. The amount of light generated being proportional to the amount of ADA in the sample. This assay can be performed with and without an acidification step to provide total and free ADA measures.
Anti-drug antibody incidence against biologics currently available to treat psoriasis
Anti-drug antibody incidence against biologics currently available to treat psoriasis
The issue of immunogenicity is recognised across all disease/conditions where biologic therapies are used [25]. There is increasing evidence regarding the immunogenicity of biologics used in the treatment of psoriasis as shown in Table 3.
Anti-TNF-
drugs
Differing levels of ADAs have been seen amongst the biologics within this subclass. A randomised controlled trial, involving 835 patients suffering from psoriasis, found anti-infliximab antibodies in 35.8–41.5% of patients on 5 mg/kg of infliximab, with higher levels (46.2–51.5%) seen in those on 3 mg/kg. It was also found that those with ADAs were less likely to maintain treatment response. With regards to safety, those deemed ADA positive were more likely to experience infusion reactions, though these were generally mild reactions. This could suggest that the presence of ADAs reduces the clinical efficacy of infliximab [26]. Conversely, a prospective study detected a significantly lower ADA incidence against infliximab, at 5.4%. However, there are limitations to this study. The short follow up period of 22 weeks may have not been long enough for ADA development to be observed [27].
An earlier randomised controlled trial found anti-adalimumab antibodies in 8.8% of 825 patients treated with the biologic over a 52-week period. This study also concluded that some patients who were ADA positive experienced reduce efficacy, though the effect was minimal. Nonetheless, ADAs were not linked to adverse effects seen in patients [29]. A significantly higher ADA incidence was found in a recent 51-week randomised, double-blinded phase III trial. At 17 weeks, ADAs were seen in 34.1% of patients, increasing to 45.1% at week 51. Of the latter, 85% were NAbs [28]. However, this difference in prevalence could be due to the use of more sensitive assays in the recent study, since there was no reporting on the testing modality used in the earlier study.
Although the newest of the group, certolizumab-pegol displays moderate immunogenicity. A study found the ADA prevalence at week 12 to be 5% and 4% in patients taking 200 mg and 400 mg of the drug respectively, increasing to 18% and 25% at week 24 [31]. The lowest incidence of ADAs within this group was seen in a study involving etanercept. This randomised controlled trial, comparing etanercept to its biosimilar, found just 1.9% of psoriasis patients developed anti-etanercept antibodies, all of which were BAbs, at week 12 of treatment. By week 52, there were no reported ADAs in patients [1]. This result is in line with a previous study, where 1.5% of 606 patients tested positive for BAbs, following serum analysis after 12 weeks. The presence of anti-etanercept antibodies had no adverse impact on clinical efficacy [30].
Anti-IL-12/23 drugs
Ustekinumab is the only biologic which falls under this category of targeting IL-12 and IL-23 through the shared p40 subunit and generally shows a lower immunogenicity compared to most anti-TNF-
Anti-IL-23 drugs
Despite the biologics within this group being humanised or fully human, they still display immunogenicity. In multiple phase III trials, involving a total of 1079 patients being treated with 150 mg of risankizumab over 52 weeks, the ADA incidence was 24%, with 14% of these being NAbs. Likewise, the presence of these ADAs did not impact the safety and clinical efficacy of risankizumab. However, there was no specification on the type of assay used to detect ADAs, a weakness in this study [37].
Moreover, a recent study, investigating the development of ADAs against tildrakizumab, found patients treated with 100 mg had an incidence of 6.5%, increasing to 8.2% in those taking 200 mg. The incidence of NAbs was 2.5% and 3.2% for each dose, respectively. Additionally, the presence of NAbs, in those who were ADA positive, was associated with increased clearance of tildrakizumab and a reduction in clinical response by 10–15% [35]. Conversely, an earlier study showed 18% of patients produced ADAs against tildrakizumab following treatment. Despite this, the clinical response in ADA-positive patients was no different those who were negative for ADAs, contradicting the findings of the aforementioned study. However, the small sample size was a drawback to this study and may have influenced the outcomes [36].
In recent randomised controlled trials, assessing the incidence of ADAs against guselkumab and their impact, it was reported that 8.5% of patients were ADA positive following 100 weeks of drug exposure. Of those positive, 0.5% had NAbs. As with risankizumab, the presence of ADAs had no influence on the clinical efficacy of guselkumab. Furthermore, the use of a sensitive drug assay, alongside the large population (1829 patients) involved in this study, provides strength to the reported outcomes [38]. The results from these trials are consistent with a prior randomised controlled trial, which analysed patient serum samples, using a highly sensitive drug tolerant assay, to find an ADA incidence of 9% [34].
Anti-IL-17 drugs
Generally, IL-17 inhibitors demonstrate low immunogenicity when used in the management of moderate to severe psoriasis. A study, assessing the ADA prevalence against ixekizumab over a 60-week period, found that 17.4% of patients produced ADAs, of which 3.5% were neutralising. Furthermore, only patients with high-titre ADAs (2.4%) experienced a decrease in ixekizumab serum concentrations and a reduced clinical response. This finding suggests the impact of ADAs against ixekizumab may be related to ADA titre. Nonetheless, other factors which may influence ADA development, such as disease status and patient characteristics, were not explicitly investigated in this study, posing as a limitation [43].
In phase III trials for brodalumab, anti-brodalumab antibodies were detected in 1.8–2.3% of patients following a 52-week period of being treated with the drug. Additionally, no NAbs were detected in patients and there was no association with loss of efficacy as a result of ADAs [41]. A similar result was seen in clinical trials which assessed immunogenicity in a total of 4461 patients. Here, 2.5% of patients who were pre-treatment negative developed ADAs, and as with the previous study, all were BAbs. The presence of these ADAs had a small effect on clinical efficacy, with a majority of patients maintaining response through the 52 weeks of treatment. Analysis of the impact of ADAs on safety revealed no hypersensitivity reactions occurred from ADAs, with only a small percentage (1.8%) experiencing injection site reactions [42].
Furthermore, a study, investigating the development of ADAs against secukinumab across six phase III studies, reported that only 0.4% of patients developed ADAs, of which 33% were NAbs. There was a small impact on clinical efficacy, with a few patients experiencing loss of efficacy due to the presence of ADAs. Similarly, there were no apparent adverse effects related to ADAs, suggesting their presence has minimal impact on safety. It was suggested the low ADA incidence may be due to fully human antibodies, such as secukinumab, having a lower immunogenic potential [39].
A more recent study reported similar results to the aforementioned study. It was found that the incidence of ADAs, which was evaluated over 5 years, was
Conclusion
The development of biologics has been a significant advance in the management of psoriasis, with patients seeing improvements following their usage. However, it is evident there are still concerns with their use, a major one of which is their immunogenic potential. There appear to be discrepancies in the measuring of free ADAs and those bound in immune complexes (Table 3). This had led to different values relating to immunogenicity being published in the literature. Ideally, it would be useful to determine the total amount of ADAs and free ADAs in psoriasis patients being treated with these biologics. Thus, assays which can determine these two extreme values should be developed, to improve the accuracy and consistency of ADA reporting.
Footnotes
Acknowledgments
AE and ASK are recipients of an award from the National Institute of Health Research, “Rapid, Sensitive Detection of Resistance to Therapeutic Antibodies” Product Development NIHR201645.
Conflict of interest
VP, DB have nothing relevant to declare. AE is CEO of Camstech Ltd an early stage company developing novel biochemical sensing technologies. ASK has filed patents related to technology used for ADA assays.