
Abstract
PURPOSE OF THE REVIEW:
Here we critically evaluate the literature on immunotherapy failure in inflammatory bowel disease patients. In particular anti-drug antibody production, and subsequently loss of response as the primary cause of immunotherapy failure in IBD patients. The benefits of shifting from the “standard” empirical dose escalation approach to therapeutic drug monitoring with anti-TNF
RECENT FINDINGS:
The American Gastroenterology Association and British Society of Gastroenterology both currently recommend the use of reactive therapeutic drug monitoring to guide treatment, following loss of response in inflammatory bowel disease patients with active disease. However, further research is required to prove the efficacy of a proactive therapeutic drug monitoring approach alone in remitted IBD patients.
SUMMARY:
A combination of personalised monitoring approach for anti-drug antibodies and therapeutic drug monitoring could provide beneficial treatment outcome for people with inflammatory bowel disease by predicting drug failure prior to clinical symptoms and allowing timely switching to an alternative drug.
Keywords
Illustrating inflammation in the gastrointestinal system and clinical features associated with (a) CD and (b) UC.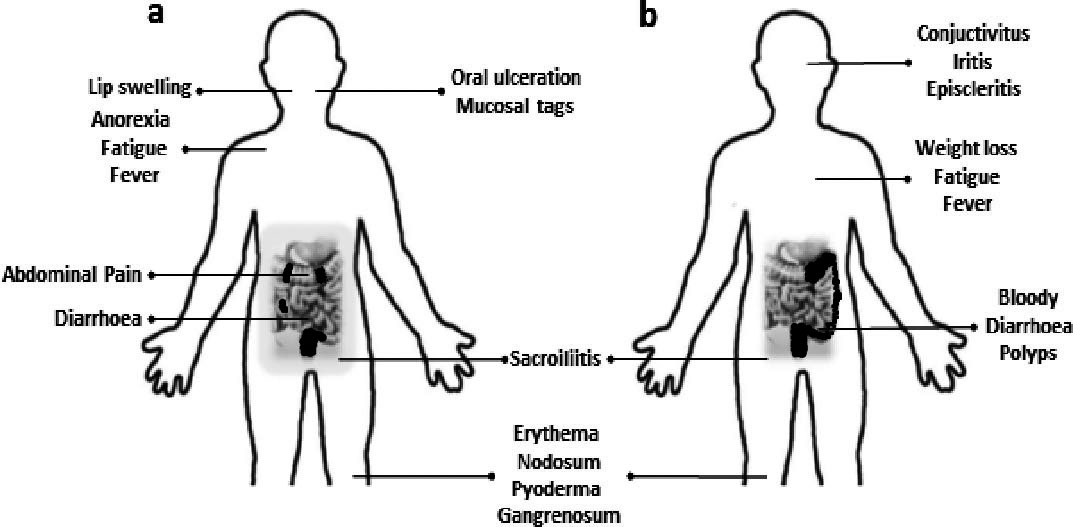
Inflammatory bowel diseases (IBD) are chronic, relapsing and remitting disorders of intestinal inflammation often with systemic manifestations. The term IBD encompasses a spectrum of disease, predominantly Crohn’s disease (CD) and ulcerative colitis (UC) and some crossover with intermediate conditions [1]. These are chronic, inflammatory conditions, primarily affecting the gastrointestinal system, with relapsing-remitting periods. Inflammatory bowel disease has a considerable impact on patient’s quality of life (QoL), the economy, and on the health care system [2]. Crohn’s disease can affect any part of the gastrointestinal tract, most frequently the terminal ileum and is associated with “skip-lesions”, transmural granulomatous inflammation and thickened involvement from the mouth to the anus, as seen in Fig. 1a. Ulcerative colitis can affect the whole large intestine, commonly the lower colon and rectum, as seen in Fig. 1b. Patients exhibit continuous diffuse, mucosal inflammation, possibly with the formation of pre-malignant pseudopolyps. The difference in location and degree of inflammation associated with CD and UC suggests why patients present with varying clinical features, as contrasted in Figs 1a and b.
Pathogenesis, aetiology, prevalence and epidemiology of IBD
Pathogenesis and aetiology of IBD remains unclear, although genetically predisposed individuals are at greater risk, likely due to dysbiosis of their gut microbiota and dysregulated immune system; other factors associated with developing IBD include pollution, diet, and lifestyle. Disease severity can be affected by the following clinical parameters: disease location, behaviour, age, serological markers, and lifestyle [3].
IBD is said to be the disease of the Western world, however its prevalence is increasing in newly industrialized countries. Globally, there was an 85.1% increase in IBD patients between 1990 and 2017, from 3.7 to 6.8 million. A trend was established where countries with a higher human development index (HDI) exhibited a higher prevalence than those with a lower HDI e.g., USA, UK, Australia, and Canada. Areas with previously low IBD prevalence experienced an increase in IBD patients e.g., south, and east Asia; an increase in their socioeconomic status likely caused lifestyle, diet, environmental and microbiota changes, thus increasing their risk. IBD can develop at any age, although 15-to-35-year-olds were more frequently diagnosed [4].
Management of IBD
The aim of treatment is to improve patient’s quality of life, avoid complications, surgery or hospitalisation and maintain remission; these conventional treatments and their indications based on the UK National Institute of Health and Care Excellence (NICE) British National Formulary (BNF) [5] and the online resource DrugBank [6] are summarised in Table 1. As IBD is an ongoing, fluctuating disease, investigations are carried out repeatedly to determine disease severity, extent, and guide treatment options [7].
*Olsalazine sodium can also inhibit thiopurine 5-methyltransferase; **Budesonide is also indicated for UC involving the rectum and recto-sigmoid disease
Biologics are highly complex proteins derived from biological sources, commonly prescribed to patients with moderate to severe IBD, where conventional treatments in listed in Table 1 proved inadequate; these biologics and their indications are highlighted in Table 2 [8, 9]. In the case of treatment option for IBD all the biologics are monoclonal antibodies, targeting different molecules as shown in Table 2 and have differing mechanisms of action, as illustrated in Fig. 2 [10].
The pathogenesis of IBD and therapeutic cytokine/integrin targeting by biologic disease modifying agents. Created using Biorender.com.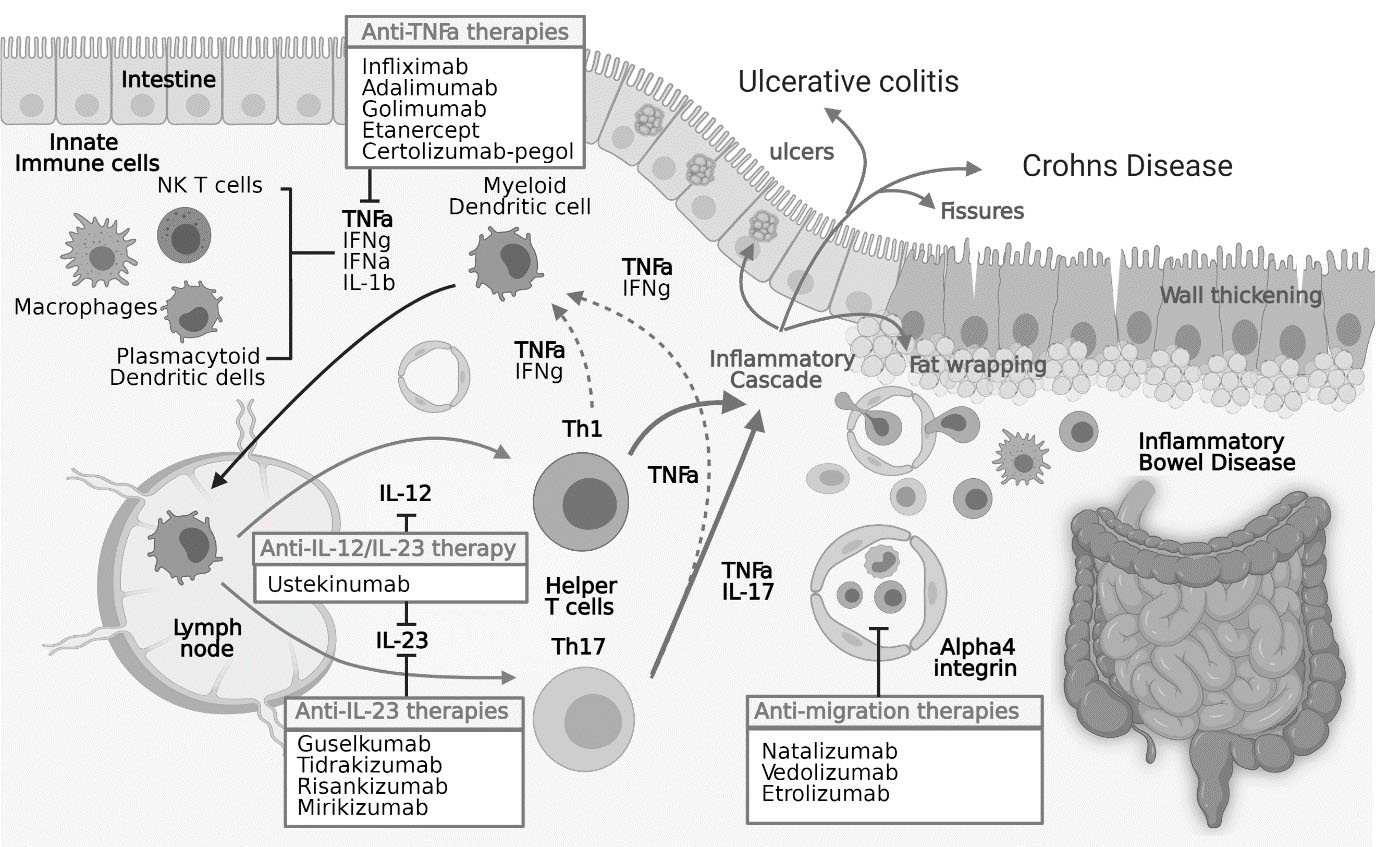
Biologics have proved to be effective in reducing disease complications, when used early after diagnosis, thereby decreasing the need for hospitalisation or surgery. Studies have shown anti-TNF agents are effective during induction and maintenance therapy, fistulizing CD and mucosal healing in CD patients, as shown in Tables 3 and 4. Adalimumab, Certolizumab, Vedolizumab and Ustekinumab were efficacious in treating CD patients unresponsive to other biologic therapies. After 4 weeks of treatment with 5 mg/kg intravenous infliximab, Targen et al. reported 81% of CD patients experienced positive outcomes compared to the placebo group (17%) [11]. With CD steroid-refractory patients, Lemann et al. reported 64% of patients achieved clinical remission, compared to placebo (34%) following 12 weeks of treatment with infliximab [12]).
Evidence collated from biologics trials for CD patients [8]
Evidence collated from biologics trials for CD patients [8]
Evidence collated from biologics trials for UCD patients [8]
Here we explores issues arising with immunotherapy in inflammatory bowel disease (IBD), particularly the occurance and persistance of anti-drug antibodies (ADAs) and subsequent loss of response (LOR). The literature is reviewed to determine the impact these factors have on IBD patients undergoing biological therapy and whether a personalised monitoring approaches can improve treatment outcomes for people with IBD. Despite improvement in clinical outcomes with immunotherapy in IBD patients, the need for conventional treatment and surgical intervention persists as a third of IBD patients are unresponsive to anti-TNF therapy and the majority lose response with time.
Incidence of ADAs in IBD patients receiving different biologics
Incidence of ADAs in IBD patients receiving different biologics
Biologics are very expensive, restricting their use worldwide. Debates are ongoing on whether their benefits are cost-effective compared to conventional therapies; therefore, developing guidelines based on high-quality evidence, for indications of biologics in IBD patients is crucial.
Adverse effects of biologics include increased susceptibility to infections due to immunosuppression (e.g., latent TB), malignancies associated with prolonged treatment and injection site reactions. Following subcutaneous adalimumab injections, 24–38% of patients experienced injection site reactions. A trial looking at the incidence of patients developing cancers following infliximab therapy compared to the control population, found a statistically insignificant increased relative risk (1.1) [13]. Despite the large sample size (over 6000 patients), the study was relatively small for such rare adverse effects and for results to be statistically significant.
With monoclonal antibody therapy, there is potential for immunogenicity, initiating an immune response that produces ADAs; an issue observed even with fully humanized monoclonal antibodies like adalimumab [14]. Immunogenicity is a crucial factor to consider during treatment planning as the ADAs produced can reduce clinical response rates to the respective agent and increase the risk of infusion related reaction [15]. In clinical studies, immunogenicity of biotherapeutics is assessed by detecting antibodies produced against a specific agent and characterising them as neutralizing, non-neutralising, transient or persistent antibodies [16]. Research supporting ADA production and their incidence for biologics used in treating IBD based on peer reviewed article [17] and FDA approved labels [18, 19, 20, 21, 22, 23] are summarised in Table 5.
The studies in Table 5 all observed a higher incidence of ADAs in patients receiving immunotherapy alone than those receiving immunosuppressant drugs alongside immunotherapy i.e., azathioprine and methotrexate. However, the studies do not distinguish the type of ADAs produced. This is significant as neutralising ADAs have been shown to directly reduce the biologic’s therapeutic activity, whereas non-neutralising antibodies indirectly affect agent’s efficacy by increasing the rate of drug clearance. Additionally, there is no information provided to indicate whether the level of ADAs measured were free or total ADAs; this may signify why ADA levels were significantly lower in some studies compared to others following immunotherapy.
ADA incidence in Table 5 varied between biologics due differing degrees of immunogenicity but comparing results across trials can be misleading due to immunoassay heterogeneity; their specificity and sensitivity differs. For example, a trial testing for anti-infliximab antibodies in UC paediatric patient found that with EIA and ECLIA, 7% and 52% of patients had anti-infliximab antibodies respectively. The significant difference in ADA incidence was due to the ECLIA method having a 60-fold higher sensitivity to the antibodies compared to EIA. Therefore, ECLIA-positive patients had detectable infliximab trough concentrations, which were generally undetectable using the EIA method as disclosed in the Remicade
The British Society of Gastroenterology guidelines for anti-TNF therapeutic drug monitoring in IBD patients [7].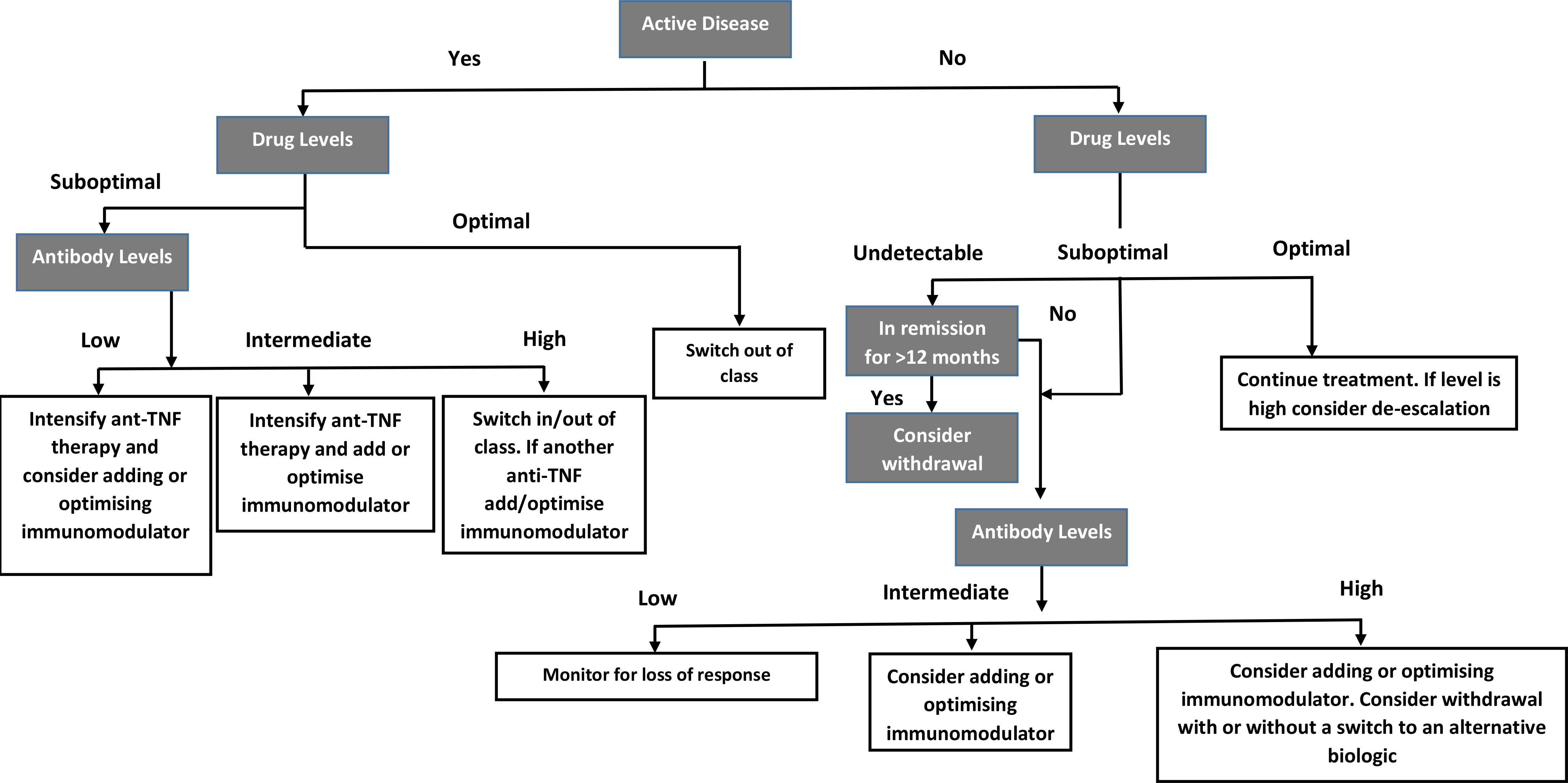
ADA formation following immunotherapy of IBD patients can impact patient safety, treatment efficacy and pharmacokinetics. A systematic review found an increased potential of adverse effects e.g., infusion-related reactions, in ADA-positive patients compared to ADA-negative patients following infliximab treatment. Additionally, ADA-positive patients had lower serum levels of the drug and fewer patients reached remission when compared to ADA-negative patients. The presence of ADAs is associated with reduced treatment efficacy, LOR following immunotherapy, and higher rates of secondary treatment failure. Efficacy was assessed using Mayo response, Crohn’s disease activity index (CDAI) response/remission and endoscopic improvement [24]. Note that CDAI has limitations as reproducibility is limited, ratings given are subjective (e.g., for abdominal pain), and there is possibility for interobserver variability. With standard dosing escalation, biological therapies do not provide long-term persistence due to ADA development and suboptimal drug levels. With most anti-TNF agents, a third of patients do not initially respond, for those that do over a half experience loss of response after the first year of treatment and 10–15% lose response for every subsequent year. The current treatment guidelines have proved effective in managing most patients; however, some continue to experience frequent relapse, LOR, serious complications, and require surgical interventions. Switching biologics can take time, during which the patient’s quality of life can significantly deteriorate; patients can take 8 weeks to notice an improvement in symptoms following induction phase of treatment. Dosing based on “one size fits all” approach is not ideal due to variations in disease course, outcomes, and phenotype. The broad range of responses demonstrated by individuals undergoing immunotherapy highlighting the complex, heterogeneous nature of IBD and necessity for personalised treatment [25].
Personalised medicine (PM) involves tailoring treatment based on the individual’s underlying disease biology, environment and needs. With IBD, PM may be utilised in diagnostics, stratification, prognostication, and treatment response; this involves grouping patients based on likelihood of side-effects and response to therapy.
Risks associated with current therapies include exposing patients with indolent disease to avoidable side effects by over treating them with top-down therapy approaches or undertreating individuals who later develop complications with step-up therapy methods. To avoid disease sequelae, management approaches are shifting from “reactive” to “proactive”, where doses are tailored to maintain therapeutic effects, while minimising side-effects. Precision medicine plays a role in predicting response, guiding treatment, informed and shared decision-making [26].
Therapeutic drug monitoring (TDM) is an important part of precision medicine. The TDM involves assessing drug trough and ADA levels at a certain treatment phase to assess drug metabolism, compliance, and immunogenicity, to guide treatment in patients with active IBD. The aims of TDM are to adjust drug doses to prevent (proactive TDM) and overcome (reactive TDM) LOR.
In current clinical practice, TDM is utilised to guide treatment following empirical dose escalation, as illustrated in Fig. 3. The British Society of Gastroenterology’s 2019 guidelines recommend switching to a biologic with a different mechanism of action, when high ADA levels are detected alongside undetectable or sub-therapeutic drug-levels.
Alternately, patients with active disease may be switched to another anti-TNF, preferably alongside concomitant immunomodulators to reduce the risk of future ADA development. However, in individuals with low or intermediate antibody titres and sub-optimal drug level, the dose or frequency of the drug must be intensified [7]. However, “optimal” drug levels for biologics are not defined as this depends on the clinical context and assay used. The American Gastroenterology Association (AGA) recommend checking trough levels within 24-hours of the next dose and using the same assay for ADAs and trough levels, as assays for ADA titres are inconsistent [27]. The international organisation for the study of IBD (IOIBD) proposed several parameters indicating remission and used this to suggest targets for IBD patients to reach. For CD, targets proposed for clinical remission include resolving abdominal pain, altered bowel habits, and mucosal healing. With UC, targets proposed for clinical remission include resolving altered bowel habits, rectal bleeding, and mucosal healing.
Reactive therapeutic drug monitoring
Pharmacokinetic measurements are employed to manage IBD patients in induction and maintenance phases. Monitoring drug trough levels and ADAs routinely prolongs biologic use by ensuring drug levels are optimal, avoiding production of ADAs and subsequently future LOR. In patients experiencing LOR to a specific biologic, ADAs and drug levels are utilised to determine whether to adjust dosing intervals, switch class of biologics or switch anti-TNF agents. Maser and colleagues confirmed significant correlation between anti-TNF levels and clinical response; clinical remission rates were higher in CD patients with detectable infliximab levels (82%) than those with undetectable levels (6%) [28]. Seow and colleague observed similar results along with endoscopic improvement in patients with detectable infliximab levels [29]. Note factors that can accelerate drug clearance include high body weight, low albumin level and inflammation, alongside high CRP concentrations and specific markers. Target trough levels may also differ according to disease severity, behaviour and phenotype, and gender.
Therapeutic drug monitoring can even be used to predict clinical outcomes; Cornillie and colleagues found that a minimum of 60% CRP reduction with at least 0.5
Following empirical dose intensification, two meta-analyses found LOR in 18.2% and 37% for patients treated with adalimumab and infliximab respectively, with a calculated annual risk of LOR of 24.4% and 13% respectively [32, 33]. In these cases, reactive TDM can be utilised to manage patients with LOR. Measuring ADAs and trough levels is paramount to deciding the next step in treatment, whether this is switching to a different class of biologics, or dose intensification alongside a concomitant immunomodulator.
Regarding the cost of utilising a reactive TDM-based approach, a multicentre, randomised control trial proved TDM-guided dosing to be more cost-effective in CD patients with LOR to infliximab compared to routine dose intensification; using trough levels and anti-infliximab antibody measurements to guide dosing reduced cost by 34% than escalating infliximab doses every 4 weeks by 5 mg/kg [34]. Similarly, an observational multicentre study concluded that applying the principles of TDM to manage IBD patients experiencing LOR following infliximab therapy was more cost-effective compared to the “standard” approach of managing LOR. Cost was reduced by 15% as more patients switched anti-TNF therapy and less dose intensification was required with TDM approach compared to empirical dose escalation [35].
The 2017 AGA guidelines recommend reactive TDM to guide anti-TNF therapy in patients with active IBD, to determine whether switching drug classes or optimizing dose is appropriate following LOR. Reactive TDM proved to be effective in guiding anti-TNF therapy, however there is insufficient data to support routine TDM with newly approved biologics, such as vedolizumab and ustekinumab [27].
Proactive therapeutic drug monitoring
Proactive TDM involves assessing ADA and trough levels for patients in clinical remission to modify the dose and frequency accordingly, to maintain therapeutic drug levels and prolong treatment with that biologic.
Proactive TDM provides the possibility of pre-emptive dose optimization to avoid future LOR. In TAILORIX, a randomised controlled trial comparing management of IBD patients through TDM-based dosing versus clinical symptom-based dosing of infliximab treatment, 47% and 40% of patients respectively sustained remission from week 22 to 54. The study concluded no difference in endoscopic and clinical outcomes after one year between dose intensification guided by proactive TDM and by clinical symptoms alone [36]. However, this conclusion must be carefully considered as limitations in the methodology makes comparison of the groups very difficult and therefore, isolating the effects of proactive TDM problematic; dose intensification was based on biological and clinical monitoring combined with TDM rather than TDM alone, meaning that dose intensification was allowed regardless of infliximab trough levels. Despite the study being unable to demonstrate the superiority of proactive TDM over the “standard” approach, the results revealed that pre-emptive TDM reduced the risk of LOR and flare-ups compared to clinically-based dosing.
Similarly, TAXIT, a large prospective trial, found that proactive TDM-based dosing was also not superior to clinically-based dosing, to achieve remission at 1 year following the optimisation phase; 69% and 66% of patients achieved remission, respectively. However, a significantly lower number of patients relapsed with proactive TDM-based dosing (7%) compared to clinically-based dosing (17%). Additionally, 15% of CD patients attained remission via proactive dose optimisation; this study showed that proactive TDM-guided dosing improves outcomes in CD patients with low drug levels. This study also demonstrates the economic benefits of proactive TDM-guided dosing as there was a significant 28% reduction in drug costs [37]. The TAXIT trial missed its primary endpoint due to design flaws; during the initial phase, TDM was utilised to optimize dosing in all patients. The follow-up period was up to 1 year, this may have been too short for proactive TDM to demonstrate its benefits considering the annual rate of loss of response for infliximab (10–20%). Additionally, the trial included patients who were not biologic-naïve and previously undergone biologic treatments for differing periods. Conversely, a multicentre retrospective study analysing IBD patients receiving infliximab therapy through proactive versus reactive monitoring of drug levels, observed superior clinical outcomes with proactive TDM. This includes greater drug levels, reduced IBD-related hospitalisation, and surgery, as well as lower therapy discontinuation rates, reduced risk of severe infusion reactions and ADA development [38]. Multi-centre, prospective studies with similar outcomes are needed.
Very few prospective studies are available comparing reactive and proactive TDM in IBD patients, with the primary end point of maintain clinical remission. PAILOT, a recent multicentre, randomised controlled trial concluded superior outcomes for paediatric CD patients with proactive TDM than reactive TDM, as 82% and 48% respectively sustained remission from 8 to 72 weeks of adalimumab therapy [39]. Unlike the TAXIT trial, patients included in this study were all biologic-naïve. This trial’s methodology was also superior to that of the TAILORIX trial, as dose intensification was based only on plasmatic trough concentrations, allowing this trial to successfully reach its primary end point.
The PAILOT trial is currently the only large, multicentre, prospective study available comparing reactive and proactive TDM in IBD patients; therefore, a study identical to this is crucial to determine whether a similar outcome can be achieved with adult IBD patients.
Proactive TDM may be the solution to monitoring clinically remitted patients with active endoscopic disease, as well as dose de-escalation for IBD patients in endoscopic and clinical remission with supratherapeutic drug levels. Paul and colleagues carried out a prospective study with 20 CD patients in endoscopic and clinical remission with supratherapeutic infliximab levels. They found that with progressive dose de-escalation until 3–7
The AGA is yet to recommend routine proactive TDM in dormant IBD patients undergoing anti-TNF
Utilising a proactive TDM approach in clinically remitted patients to maintain “therapeutic” drug levels is not yet recommended however, it is crucial as low drug trough levels are associated with ADA development, and subsequently LOR. Reactive TDM-guided dosing may not be appropriate in recapturing response at this point and proactive TDM may therefore be the only solution to prolonging treatment with the same biologic. This is crucial as research demonstrates that the greatest therapeutic effects are achieved with the first biologic treatment the patient receives, and response to second line biologics is reduced in patients who have previously undergone treatment with anti-TNF agents. This again highlights the need for large, multicentre, randomised controlled trials to compare the value of reactive and proactive TDM in helping IBD patients to remain in remission and avoid LOR with first line biologics; these studies would provide the opportunity to further evaluate the effectiveness of proactive TDM and justify its application where the use of reactive TDM is not feasible.
Conclusion
In conclusion, immunotherapy has proven to be very effective in treating a large proportion of IBD patients with moderate to severe disease that responded inadequately to conventional treatments. However, biological therapies still pose limitations with long-term use, due to immunogenicity, ADA development and subsequent LOR. A personalised monitoring approach, specifically TDM has already proven to be cost-effective, and successful in allowing a greater proportion of patients to maintain clinical and endoscopic remission, compared to empirical dose escalation with anti-TNF therapy. Based on the research available, reactive TDM is currently recommended by the AGA when guiding treatment, following the LOR with anti-TNF therapy in IBD patients with active diseases. However, there is an insufficient amount of data available to support routine TDM with vedolizumab and ustekinumab; data on when to best measure drug trough levels and how to interpret the results for patients treated with these approved biologics is scarce.
As for proactive TDM, existing research does show promise regarding its use in anti-TNF dose de-escalation for patients in remission, as well as demonstrating its benefits in managing remitted patients compared to empirical dose escalation and reactive TDM. However, very few prospective studies are currently available and further data is required regarding the ideal frequency of proactive TDM and target drug levels for clinically remitted patients before this proactive approach can be recommended. To date, the PAILOT trial is the only multicentre, prospective study available comparing the use of proactive and reactive TDM for paediatric CD patients. This highlights the need for similar large, randomised control trials comparing proactive and reactive TDM in adult IBD patients, to determine whether the outcomes of this study can be replicated in the adult population.
Footnotes
Acknowledgments
AE and ASK are recipients of an award from the National Institute of Health Research, “Rapid, Sensitive Detection of Resistance to Therapeutic Antibodies” Product Development NIHR201645.
Conflict of interest
MB, DB have nothing relevant to declare. AE is CEO of Camstech Ltd an early stage company developing novel biochemical sensing technologies. ASK has filed patents related to technology used for ADA assays.