
Abstract
Severe combined immunodeficiency (SCID) is a form of primary immunodeficiency disease (PID). It is characterized by a serious abnormality of the cellular and sometimes humoral system due to a deficiency in development of T cells, B cells and/or NK cells. The early diagnosis of SCID improves the prognosis. Typically, the initial consideration of SCID is made based on low lymphocyte counts. Notwithstanding, the heterogeneity of lymphocyte count presentation makes the diagnosis of SCID a significant challenge. The objective of this cross-sectional retrospective study was to analyze the lymphocyte subpopulation counts along with clinical manifestations within a Moroccan cohort diagnosed as SCID compared to children diagnosed with non-PID diseases. Thirty-five SCID confirmed patients were selected in the period between 2008 and 2018 and compared with non-PID patients. Results of peripheral blood T, B, and NK lymphocyte subpopulation counts were measured by flow cytometry for each SCID subtype. As expected, T cell count was less than 300 cells/
Keywords
Introduction
Severe combined immunodeficiency (SCID) is a genotypically and phenotypically heterogenous set of inherited primary immunodeficiencies (PID). SCID is considered a life-threatening pediatric emergency [16]. SCID kids are normal during childbirth and start suffering from severe infections in the first month of their life [6]. Transplantation of HLA-identical or T-cell-depleted haploidentical marrow from related donors is a life-saving treatment in patients with any type of SCID. SCID results in early death unless urgently treated by allogeneic hematopoietic stem cell transplantation, highlighting the critical importance of early diagnosis [7, 16]. Respiratory infections, failure to thrive, chronic diarrhea, persistent oral candidiasis, pneumonia, and sepsis are the most common presentation in SCID patients [6, 26].
SCID immunodeficiencies can be classified based on presence or absence of B and NK cells in the peripheral blood into T
We also describe the prevalence of SCID subtypes in Morocco and their clinical characteristics. The prevalence of SCID worldwide is estimated to be 1 in 40,000 to 75,000 live births [16]. Amongst Mediterranean populations, SCID represents 8.2% of PID in Tunisian Population [20], and 5.7% of PID in a Spanish study [18]. As indicated in the first report on the Moroccan registry, 8.74% of PID in the Moroccan population were diagnosed as SCID [4]. The distribution of various subtypes of SCID differs in different countries. In countries with consanguineous marriages, autosomal recessive SCID incidences can be higher [12, 29, 32, 33], although X-linked SCID is the most common worldwide form [33]. The percentage of SCID is significantly higher (21.1%) in the Iranian population [1]. It was also reported that, in Iran, the prevalence of undiagnosed PID was extremely high [3]. El Maataoui et al. reported that in Morocco, the most common subtype of SCID was T
Representative example of flow cytometry gating strategy and identification of specific lymphocyte subsets. Lymphocytes were selected based on their side-scatter and CD45 positive staining. Subsequently, T lymphocytes were identified as T cells (CD3
Subjects and samples
The study subjects were selected during a 10-year period from 2008 to 2018, from patients admitted to the Immuno-allergology and Respiratory Diseases unit of the Children’s Hospital of Rabat and referred to the Cellular Immunology Laboratory of the National Institute of Hygiene for determination of the lymphocyte subpopulations. Thirty-five patients were confirmed as SCID, while 622 young patients (
Immunophenotyping
Lymphocyte subpopulations were determined from peripheral whole blood by lyse, no-wash flow cytometry protocol [9]. Fluorochrome-labeled monoclonal antibodies were used to identify and estimate the percentage of CD4
Demographic data of patients with severe combined immunodeficiency and children with non-PID
Demographic data of patients with severe combined immunodeficiency and children with non-PID
Lymphocyte sub-population counts within the four SCID sub-types
Median, minimum (min) and maximum (max) values are represented as x1000 cells/
Data were analyzed in FlowJo software (BD Biosciences). Cells were initially gated for lymphocytes (CD45 versus FSC-A). CD3
Statistical analysis
Cell counts were expressed as medians (min-max). Statistical analysis was performed using SPSS 20.0. The non-parametric Kruskal-Wallis test was used to determine differences in predominance, biological and clinical features across the study subjects’ groups.
Ethics
Permissions were obtained from the datasets owner institutions for this retrospective study to use de-identified information from their databases.
Results
Characteristics of the study groups
Collected demographic information from different SCID groups and non-SCID control group is presented in Table 1. The sex ratio in our SCID group (M/F) was lower compared to non-SCID children (1.19 versus 1.69, respectively;
Laboratory findings
Results of lymphocyte phenotyping are summarized in Table 2. As was expected, in our study lymphopenia (
Lymphocyte subpopulation counts within SCID subgroups. Distribution of independent data for T cells (a), B cells (b) and NK cells (c) counts in the four SCID subgroups are graphically represented with the cut-offs as well as the median in non-PID patients (indicated by dotted lines). Gray area represents the range where values measured within SCID and non-PID patients overlap.
The remaining 11 SCID patients had extremely low number of T cells (5 cells/
Comparison of incidence (%) of SCID subtypes in Morocco and other countries
Notes:
Clinical manifestations in non-PID and SCID patients. Graphical representation of frequency of different clinical manifestations associated with SCID in SCID and non-PID patient groups. Mann-Whitney test, n.s. 
The distribution of the clinical manifestations within the study patient groups is represented in Fig. 3. In general, respiratory infections, failure to thrive and diarrhea were observed to be the most frequently present clinical manifestation within the SCID group, while the non-PID group most commonly presented with respiratory infections and diarrhea. Meningitis was observed more frequently in SCID patients in comparison with non-PIDs. Urinary tract infections, oral thrush, CMV infection and disseminated BCG infection after vaccination was only observed in the SCID group and not in non-PID group. By contrast, sepsis was more prevalent in non-PID group.
Distribution of clinical manifestations within four subgroups of SCID patients. Graphical representation of frequency of different clinical manifestations associated with SCID in the four subgroups of SCID patients.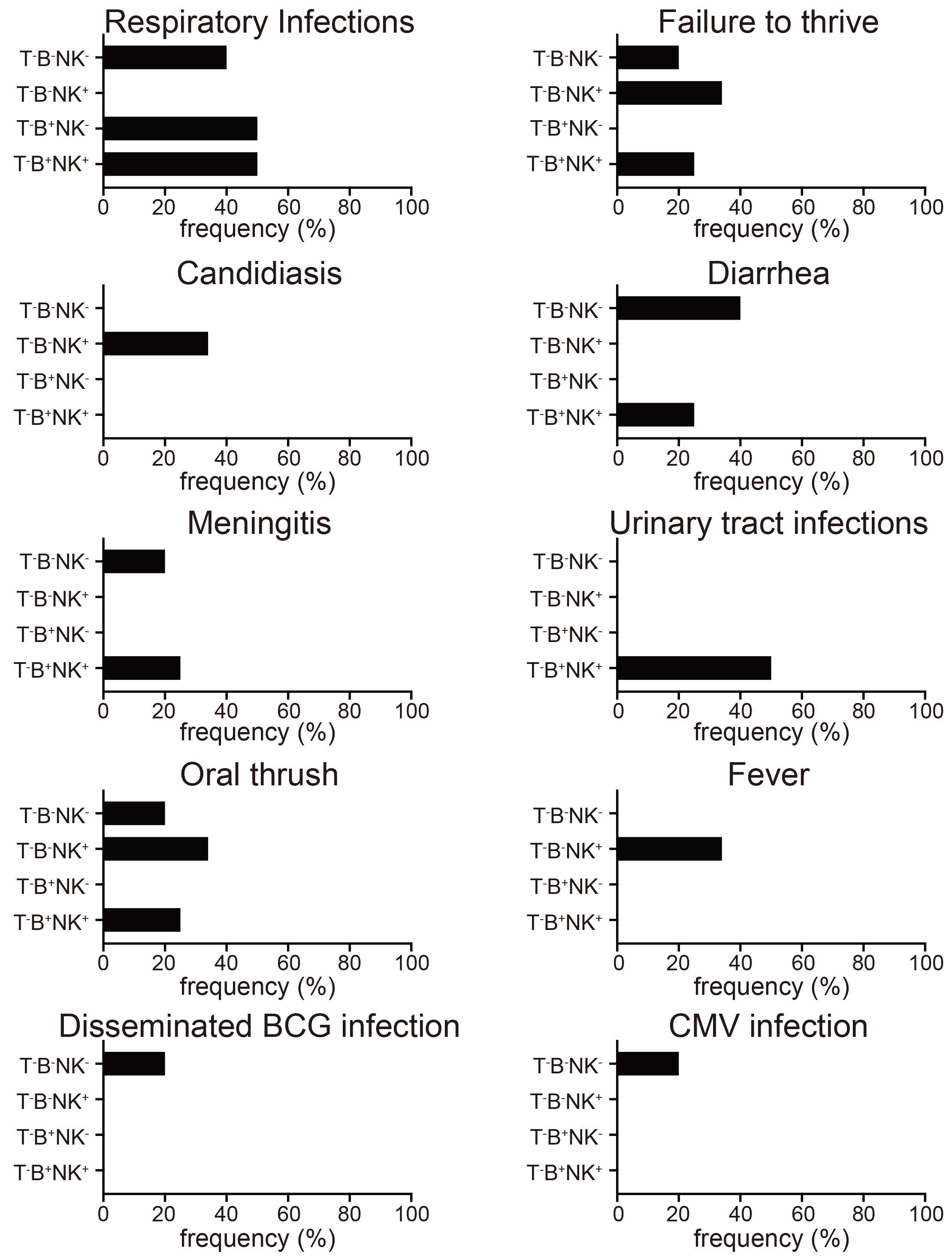
Distribution of clinical manifestations within the four subgroups of SCID patients is represented in the Fig. 4. Respiratory infections were observed across all the SCID groups, except T
Comparison of presentation (%) of clinical features of SCID in Morocco and other countries
NR, not reported. Notes:
The most intriguing finding in our study is that some SCID patients have unexpectedly high lymphocyte and T cell numbers. Diagnostic criteria of SCID mentions that T cell count should be lower than the cut off of 300 cells/
Consanguineous marriages in populations increase the prevalence of autosomal recessive SCID [12, 29, 32, 33]. In our study, positive consanguinity was found in 34% and information was not available for 14% of patients. Albeit significantly less than the 80% identified in an Iranian study [37], consanguinity in our cohort is still relatively high. The most common SCID subtype observed in our studies was T
The percentage of patients in our study with a positive history of immunodeficiency in the family was 68.5%. This number is near to the 50% observed in an Iranian study [1]. In our study, the patients with SCID familial history were diagnosed earlier in comparison to the other SCID patients. A similar result was found in the study by Stephan et al. [31]. This is probably because families with history of SCID are more aware of this disease state through previous experiences. The majority of SCID infants in Morocco are diagnosed in a specialized pediatric medical center, often in a different city, after the family travels extensive distances to seek medical intervention. The understanding of SCID is generally poor without a family history and the symptoms are confused with repeated bouts of common infections. Albeit the diagnosis was earlier than SCID patients with no family history, it still took 75 days from time of birth. Brown et al. recently reported that detection of SCID at birth because of positive family history can improve outcome by over 90% [5]. Universal newborn screening could radically transform the outcome of SCID in Morocco, but in its absence, at the least Moroccan patients with positive family history should be tested at birth. Family history-based recommendation for testing at birth is likely to greatly increase the outcome in the interim, while we await universal newborn screening.
The clinical findings in the Moroccan cohort were mostly similar with other studies. For example, respiratory infection was the most frequent symptom across all the SCID groups, except in the T
Conclusion
Family history, consanguinity of patient’s parents, clinical profile and an abnormality in lymphocytes subpopulation counts should be considered together for the diagnosis of SCID in Morocco. Physicians must take into consideration the above mentioned signs even when the criteria of T lymphopenia less than 300 cells/
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Authors contributions
FS was responsible for the conception and design of the study. AEA, SEF, HT, KS and HB performed the acquisition and analysis of biological data. AEA and NEH were in charge of the collection of clinical features. NEH analyzed the clinical data. EAE, FS, NEH, and YB wrote and revised the manuscript. All authors read and approved the final manuscript.
Footnotes
Acknowledgments
The authors thank the personnel of the Immunology, Allergic and Respiratory Diseases Unit, Children’s Hospital of Rabat for their participation in the recruitment of study subjects and sample collections. We also thank Lindsey D. Hughes for help in preparation of this manuscript, including critical reading. We thank Carla V. Rothlin and Sourav Ghosh for helpful discussions and critical reading of the manuscript.
Conflict of interest
The authors declare that there is no conflict of interest regarding the publication of this paper.