TNF- has been considered as the key regulator of inflammatory responses and is known to be participated in the pathogenesis of several diseases.
OBJECTIVE:
The aim of this study was to explore the relationship of (rs1800629) gene polymorphism associated to liver and pancreas disorders in sample of -thalassemia major adult Iraqi Patients.
MATERIAL AND METHOD:
Blood samples were obtained from 40 patients suffered from beta thalassemia with pancreas disorder, along with 40 patient suffered from thalassemia with liver disorder, and 40 patient suffered from thalassemia without pancreas or liver, from Ibn Al-Baladi Hospital, Baghdad, and 40 samples from age and gender-matched apparently healthy individuals as control group, all subjects with age more than 18 years. TNF308G/A (rs1800629) gene polymorphisms were assessed by Tetra- ARMS-PCR.
RESULTS:
The result of showed that heterogeneous GA and homogeneous AA genotypes were higher, while GG wild genotype was lower in beta thalassemia major patients with liver and pancreas disorders compared to control group.
CONCLUSION:
It can be concluded that the prevalence of TNF- 308 G/A SNP plus (A) allele could be associated with risk of liver and pancreas disorders in sample of beta thalassemia major adult.
-thalassemia is an inherited autosomal recessive blood disorder [1] considered most prevalent genetic disease worldwide [2]. Major type of thalassemia causes in severe anemia, which requires frequent and regular blood transfusions [3]. According to estimations, 3% of the global population possesses a phenotype associated with -thalassemia [4, 5]. The World Health Organization estimates that 68,000 people are born every year with -thalassemia and the incidence of symptomatic -thalassemia is thought to be 1 in 100,000 people in the general population [6]. The number of people with thalassemia in 2019 in Iraq is estimated to be over 22,000, according to the ministry of health, it consider a critical health problem in Iraq due to mainly the non-availability of equipment and drugs during different periods of turmoil and war and requires an efficient management strategy including public health education initiatives to promote early detection and treatment [7]. Even in nations where chelation is widely available, iron overload is still a serious issue for those with thalassemia major.
TNF is a potent inflammatory cytokine that increases cytokines and has a critical role in immune responses [8], in addition being a crucial multifunctional cytokine produced by a variety of immune cells, including macrophages [9]. The gene encoding TNF- is located in the class III region of the major histocompatibility complex on chromosome 6 between the HLA-B and HLADR genes [10].
Tumor Necrosis Factor- (TNF-) is an important inflammatory cytokine in the development of liver disease. This cytokine can cause hepatic injury, cirrhosis and eventually promote hepatocellular carcinoma [11, 12]. Moreover, TNF is believed to be one of the main pro-inflammatory cytokines involved in the destruction of pancreatic ß-cells [13]. Studies in vitro and in vivo have demonstrated that TNF ligand-inducing apoptosis-related repression of proliferation and differentiation erythrocyte progenitor cell. furthermore, there are significantly increases in the levels of TNF- which can prevent erythropoiesis in the bone marrow of thalassemia patients. In the promoter of the TNF gene, many (SNPs) were discovered. A number of disorders have been studied in association to the TNF308G/A SNPs. The prevalent allele G, is changed at location 308 with the rare allele A. The rare allele was related to elevated expression of TNF- despite its the accuracy of the mechanism are not clear [14]. These SNPs may result in structural changes in the regulatory sites of the gene, which may have an impact on TNF- production or function [15]. The biological effects of TNF- are numerous and complex, and they range from conferring disease resistance to causing pathological complications [16].
In fact, TNF- have contradictory function which may be caused by genetic polymorphism in the genes that regulate its synthesis and effects [17].
The aim of this study was to explore the relationship of (rs1800629) gene polymorphism associated to liver and pancreas disorders in sample of -thalassemia major adult Iraqi Patients.
Material and method
Blood samples were obtained from 40 patients suffered from TM with pancreas disorder as group A, along with 40 patient suffered from thalassemia with liver disorder as group B, and 40 patient suffered from thalassemia without pancreas or liver disorders as group C, from Ibn Al-Baladi Hospital, Baghdad, and 40 samples from age and gender-matched apparently healthy individuals as a negative control (Group D),the groups of patients include both male and female without hepatitis, all with age more than 18 years and checked the levels of ferritin, ALT and amylase for all groups to confirm liver and pancreas disorders. After obtaining the approval of the Ibn Al-Baladi Hospital and approval patients and under ethics committee on human research for a study conducted by the Institute of Genetic Engineering and Biotechnology for Post Graduate Studies, University of Baghdad (Reference number: 15/5/2022–1304), (1.5 ml) of venous blood was taken from all subjects, put in an anticoagulant tube contain (EDTA), mixed gently and kept in the (20C). Genomic DNA from frozen blood samples was extracted by using DNA extraction kit (Geneaid/Taiwan) according to Sambrook and Russell [18]. Purity and concentration of the DNA were measured by using Nanodrop spectrophotometer (Thermo Scientific/UK). Detection of TNF gene polymorphism G/A (rs1800629) by use T-ARMS-PCR. The primers for TNF were provided by (Bioneer/Korea) depending on NCBI-Gene Bank data base as illustrated in Table 1. The Program ARMS PCR of TNF- at position 308 G/A given in Table 2. The gel electrophoresis had been performed to determine the quality of the genomic DNA extraction and to visualize the PCR products size after finishing the ARMS PCR experiments.
The tetra-ARMS-PCR primers for TNF- at position 308 G/A gene polymorphism with their sequences and amplicon size
Primer
Sequence (5’–3’)
Product size
TNF308 (G)
GGCAATAGGTTTTGAGGGGCGTGG
251bp
TNF308 (A)
ACCCTGGAGGCTGAACCCCGGCCT
202bp
TNF308 (OT-F)
GCCCCTCCCAGTTCTAGTTCTATC
400bp
TNF308 (OT-R)
AAGCGGTAGTGGGCCCTGCACCTTC
ARMS PCR program of TNF- at position 308 G/A
PCR steps
Temp.
Time
Repeat
Initial denaturation
95C
5 min.
1
Denaturation
95C
30 sec.
35 cycle
Annealing
66C
30 sec.
Extension
72C
1 min.
Final extension
72C
5 min
1
Hold
4C
Forever
–
The results of this study were analyzed by using SPSS [19]. Chi-square test was used to find the differences among numbers of groups and genotypes, also to find the Odds ratio (ORs) with a 95% confidence interval (CI).
Results
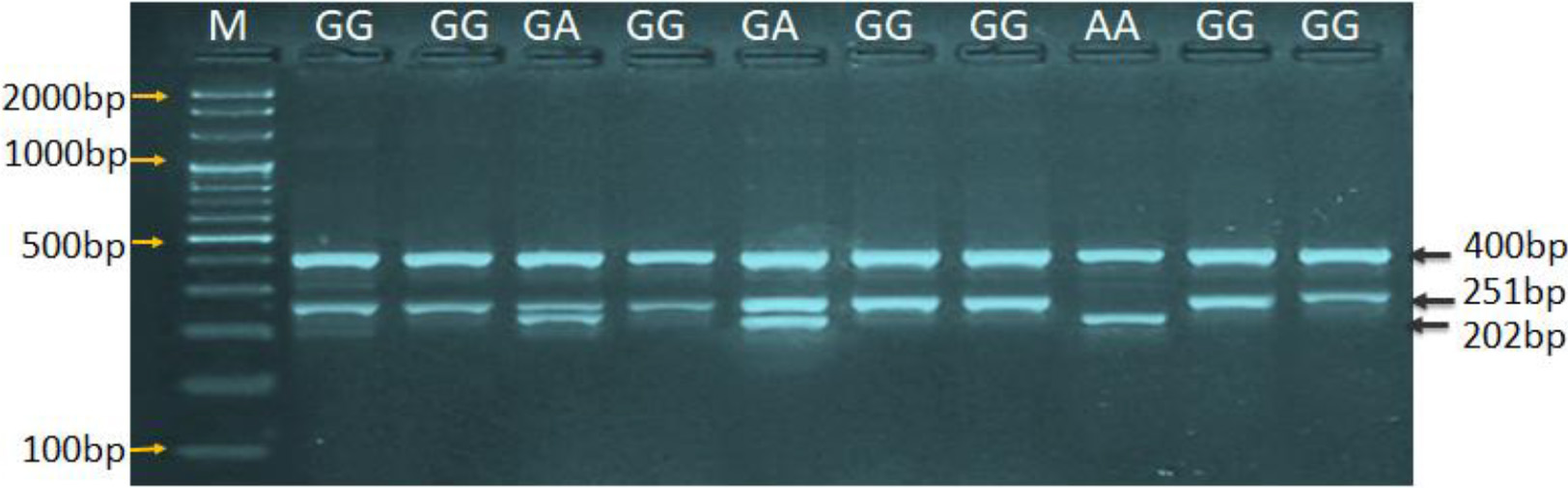
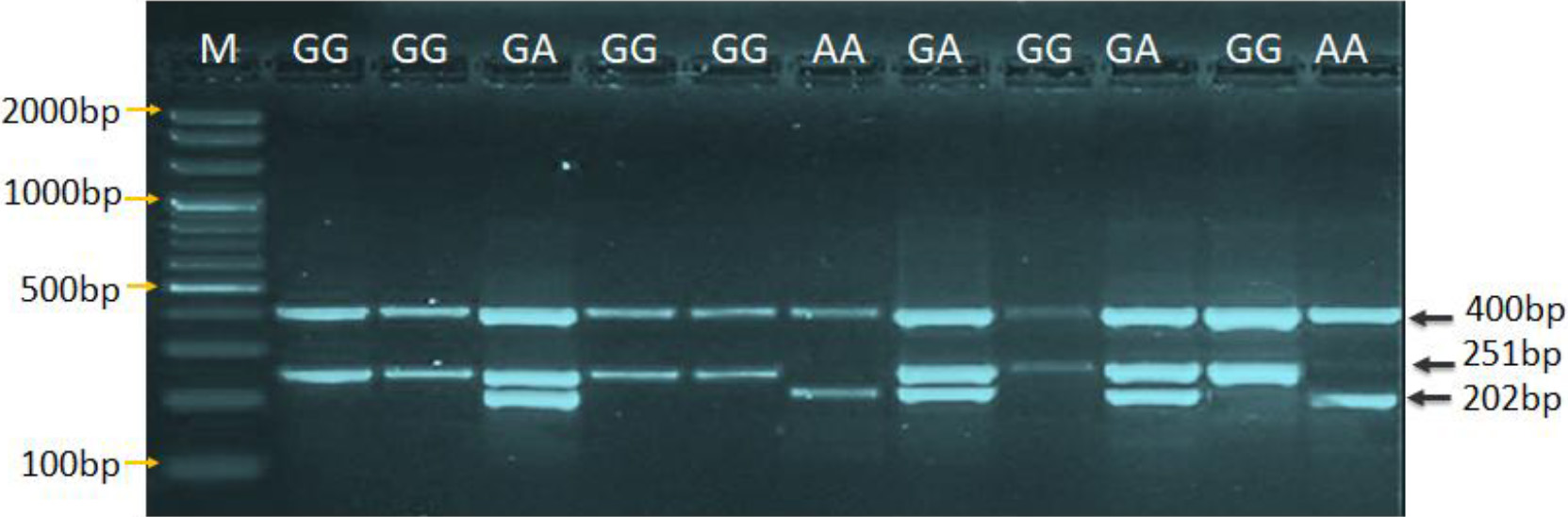
The result of distribution of TNF308 (rs1800629) polymorphism and allele frequency in thalassemia with pancreas disorders patients as group (A) and control as group(D) revealed that the wild genotype GG was 10 (25%), heterogeneous genotype GA was 16 (40%) with odds ratio (2.86), and homogeneous genotype AA was 14 (35%) with odds ratio (1.1), while G allele frequency was 36 (45) with Odd Ratio (OR) (0.288) and A allele frequency was 44 (55) with OR (2.76) in patents of (A) group with highly significant differences ( 0.01). In group (D) the wild genotype GG was 30 (75%), heterogeneous genotype GA was 7 (17.5%), homogeneous genotype AA was 3 (7.5%), G allele frequency was 67 (83.75%) and A allele frequency was 13 (16.25%), as shown in Table 3 and Figs 1, 2.
Genotypes distribution and allele frequency of TNF308 (rs1800629) gene in (A) and (D) groups
Genotype G/A
Group (A)
Group (D)
Chi-square
-value
Odds ratio
Lower 95% IC
Upper 95% IC
Wild: GG
10 (%25)
30 (75%)
3.88
0.033
Reference
Mutant heterogeneous: GA
16 (40%)
7 (17.5%)
4.08
0.043
2.86
1.01
8.07
Mutant homogeneous: AA
14 (35%)
3 (7.5%)
3.95
0.029
1.1
–
–
Total
40 (100%)
40 (100%)
Allele
Frequency
G
36 (45%)
67 (83.75%)
3.879
0.038
0.288
0.574
2.891
A
44 (55%)
13 (16.25%)
4.779
0.008
2.76
0.006
0.027
Total
80
80
( 0.01) ( 0.05); CI: Confidence interval; OR: Odd ratio; Group (A): thalassemia with pancreas disorder patients; Group (D): control.
Agarose gel electrophoresis showing T-ARMS-PCR product analysis for TNF- 308 G/A gene polymorphisms in group (A). Where M: marker (2000–100bp). The (GG) wild type homozygote genotype showing two bands at400bp and 251bp position. The (AA) mutant type homozygote showing two bands at 400bp and 202bp positions, whereas the (GA) heterozygote showing three bands at 400bp, 251bp and 202bp positions.
Agarose gel electrophoresis showing T-ARMS-PCR product analysis for TNF- 308 G/A gene polymorphism in group (D). Where M: marker (2000–100bp). The (GG) showing two bands at 400bp and 251bp positions. The (AA) mutant type homozygote showing two bands only at 400bp and 202bp positions, whereas the (GA) heterozygote showing three bands at 400bp, 251bp and 202bp positions.
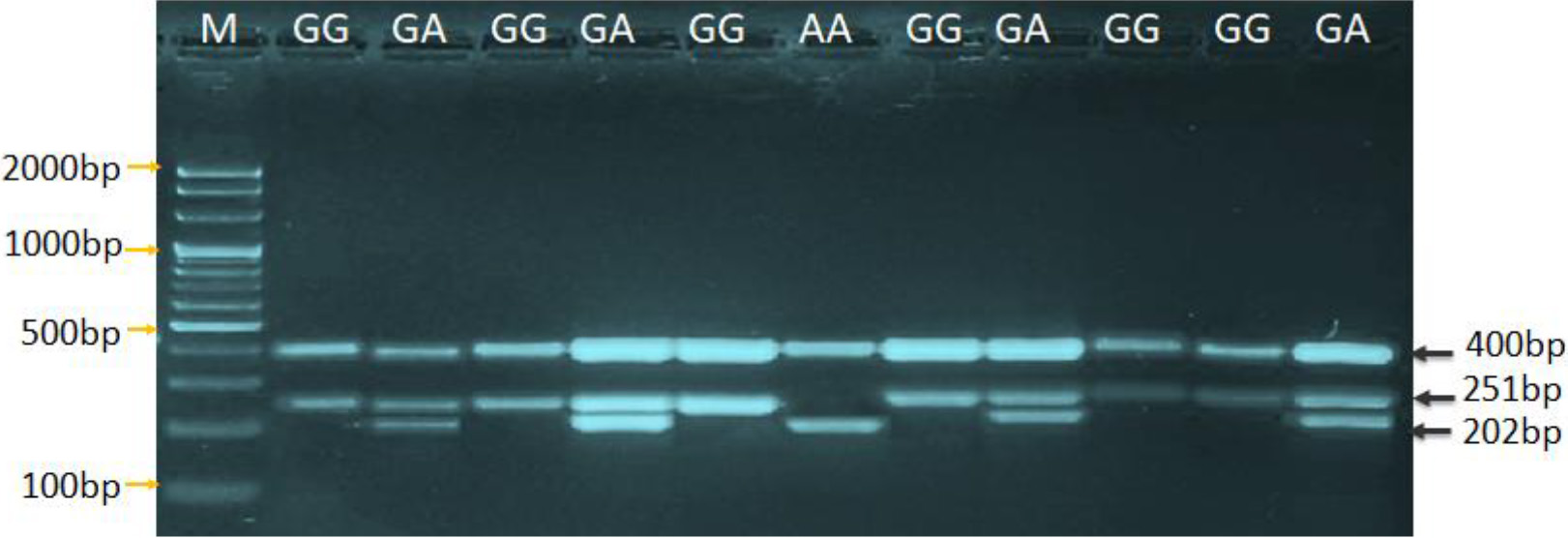
The results of distribution of TNF308 (rs1800629) polymorphism and allele frequency in thalassemia with liver disorders as group (B) and control as group (D) appeared that the wild genotype GG was 6(15%), heterogeneous genotype GA was 14 (35%) with OR (2.57), and homogeneous genotype AA was 20 (50%) with OR (0.012) while G allele frequency was 26 (32.5%) with OR (0.189) and A allele frequency was 54 (67.5%) with OR (3.76) in group(B) with high significant differences ( 0.01) as shown in Fig. 3. while the wild genotype GG was 30 (75%), heterogeneous genotype GA was 7 (17.5%), homogeneous genotype AA was 3 (7.5%), G allele frequency was 67 (83.75%) and A allele frequency was 13 (16.25%) in group (D) as given in Table 4.
Genotype distribution and alleles frequency of (rs1800629) gene in (B) and (D) group
Genotypes G/A
Group (B)
Group (D)
Chi-square
-value
Odds ratio
Lower 95% IC
Upper 95% IC
Wild: GG
6 (15%)
30 (75%)
6.95
0.008
Reference
Mutant heterogeneous: GA
14 (35%)
7 (17.5%)
3.85
0.041
2.57
0.91
7.29
Mutant homogeneous: AA
20 (50%)
3 (7.5%)
4.4
0.022
0.012
0.005
0.026
Total
40 (%)
40 (%)
Allele
Frequency
G
26 (32.5%)
67 (83.75%)
6.173
0.006
0.189
0.525
2.693
A
54 (67.5%)
13 (16.25%)
6.779
0.008
3.76
0.006
0.027
Total
80
80
( 0.01) ( 0.05); CI: Confidence interval; OR: Odd ratio; Group (B): thalassemia with liver disorder patients; Group (D): control.
Agarose gel electrophoresis showing T-ARMS-PCR product analysis for TNF- 308 G/A gene polymorphism in group (B). Where M: marker (2000–100bp). The (GG) showing two bands at 400bp and 251bp positions. The (AA) mutant type homozygote showing two bands at 400bp and 202bp positions, whereas the (GA) heterozygote showing three bands at 400bp, 251bp and 202bp positions.
The findings of distribution of TNF308 (rs1800629) polymorphism and allele frequency in thalassemia without pancreas or liver disorders as group (C) and control as group (D) appeared that the wild genotype GG was 6 (15%), heterogeneous genotype GA was 18 (45%) with OR (1.51), and homogeneous genotype AA was 16 (40%)with OR (1.49), while G allele frequency was 30 (37.5%) with OR (0.496) and A allele frequency was 50 (62.5%) with OR (3.015) in group (C) with high significant differences ( 0.01) as shown in Fig. 4. while the wild genotype GG was 30 (75%), heterogeneous genotype GA was 7 (17.5%), homogeneous genotype AA was 3(7.5%), G allele frequency was 67 (83.75%) and A allele frequency was 13 (16.25%) in group (D) as illustrated in Table 5.
Genotypes distribution and allele frequency of TNF308 (rs1800629) gene in (C) and (D) groups
Genotypes G/A
Group (C)
Group (D)
Chi-square )
-value
Odds ratio
Lower 95% IC
Upper 95% IC
Wild: GG
6 (15%)
30 (75%)
6.96
0.005
Reference
Mutant heterogeneous: GA
18 (45%)
7 (17.5%)
5.96
0.015
1.51
1.25
9.84
Mutant homogeneous: AA
16 (40%)
3 (7.5%)
5.12
0.0146
1.49
0.767
0.215
Total
40 (100%)
40 (100%)
Allele
Frequency
G
30 (37.5%)
67 (83.75%)
3.86
0.031
0.496
0.677
0.305
A
50 (62.5%)
13 (16.25%)
0.012
0.003
3.015
0.007
0.030
Total
80
80
( 0.01) 0.05); CI: Confidence interval; OR: Odd ratio; Group (C): thalassemia without pancreas or liver disorders patients; Group (D): control.
Agarose gel electrophoresis showing T-ARMS-PCR product analysis for TNF- 308 G/A gene polymorphism in group (C). M: marker (2000–100bp). The (GG) showing two bands at 400bp and 251bp positions. The (AA) mutant type homozygote showing two bands at 400bp and 202bp positions, whereas the (GA) heterozygote showing three bands at 400bp, 251bp and 202bp positions.
Discussion
One of the most common complications associated with thalassemia is iron overload resulting from regular blood transfusions and the excess of iron can damage liver and endocrine system [20].
Since red blood cells are degraded in the reticulo-endothelial system iron overload will affect the hepatic macrophages (called Kupffer cells).Thereafter, intramacrophagic iron will be released progressively into the blood stream, in order to reach the bone marrow and lead to the production of new red blood cells. During this releasing process, plasma transferrin – the normal iron transport protein in the blood, whose normal saturation by iron is less than 45% – increases rapidly, reaching often 100%. This will lead to the appearance of plasma non-transferrin bound iron (NTBI) [21], an iron species which has the property to be very rapidly taken up by parenchymal cells (the hepatocytes for the liver), therefore accounting primarily for hepatic iron overload, the liver being, for circulating iron, both the first line target and the main storage organ, thus liver cells are damaged. Pancreatic iron overload is common in thalassemia major patients and pancreatic iron loading in thalassemia major patients begins in early childhood, as well as many studies have documented endocrine pancreas dysfunction in patients with thalassemia. It is frequently observed that the pancreas’ endocrine activity is impaired, which may result in severe diabetes mellitus [22, 23].
Single nucleotide alteration from guanine (G) to adenine (A) at location 308 is the most of popular in generally populations. This transformation has been shown affect the expression of TNF-. Unfortunately, there was no previous studies dealing with TNF308 (rs1800629) polymorphism in thalassemia patients, except study of Mohammed [24] which was agreed with present study when it examined the connection between TNF gene polymorphism with -thalassemia patients and found that the genotype AA and allele A were related to risk with -thalassemia susceptibility, and the mutant genotype AA had an O.R. value of 1.83, as well as the A allele had an O.R. value of 1.3. However, there were many studies that delved into the importance of this gene variation, such as study of Zhuang et al. [25] found that under three genetic comparison models, the TNF308 G/A polymorphism was substantially correlated with a reduced incidence of psoriasis and the study by Kim et al. [26] referred to there was no association between the risk of Nephrotic Syndrome and the TNF308 polymorphism. Also a study close to this study, which was conducted by Cavalcante et al. [27] who studied the connection between sickle cell anemia and frequent genotype of patients with TNF-alpha-308 G A polymorphism was GG 20; 80%), and GA ( 5; 20%). None of the patients with AA ( 0; 0%), and this similar to our results for frequency TNF308 (rs1800629) polymorphism. With regard to pancreatic disorders, there are many studies that have focused on this topic, such as study of Zhang et al. [28] in the Chinese population with acute pancreatitis, discovered no correlation between acute pancreatitis and TNF308. But, they suggest that TNF308 A allele is related to a higher risk of severe sepsis complicating of Acute Pancreatitis. And researchers by Sargen et al. [29] and Powell et al. [30] when studied of TNF308 genotyped in acute pancreatitis patients in UK population and found that TNF308 played role in severity and susceptibility to acute pancreatitis.
Conclusion
In a sample of adults patient with beta thalassemia major, the prevalence of the TNF- 308 G/A SNP plus (A) allele may be linked to an increased risk of liver and pancreatic diseases.
Authors’ contributions
H. A. L. played a significant role in the conceptualization of the study, interpretation and analysis of data, software implementation, validation, formal analysis, investigation, resources, data curation, preparation of the manuscript, and writing-review and editing. B. J. M. also made substantial contributions to the research, including interpretation and analysis of data, validation, writing-review and editing, and supervision of the study. The authors confirm that all authors have read and agreed to the published version of the manuscript, and their combined efforts have resulted in the completion of this work.
Availability of data and materials
The authors acknowledge that the data supporting the findings of this study are available and can be obtained from the Institute of Genetic Engineering and Biotechnology for Post Graduate Studies, University of Baghdad in Iraq. Researchers or individuals interested in accessing the data may submit requests to the corresponding author, who will provide further guidance and facilitate the process.
Ethical considerations
Ethical approval or informed consent for a study conducted by the Institute of Genetic Engineering and Biotechnology for Post Graduate Studies, University of Baghdad (Reference number: 15/5/2022–1304).
Footnotes
Acknowledgments
The authors would like to express their sincere appreciation to the Institute of Genetic Engineering and Biotechnology for Post Graduate Studies team for their invaluable assistance throughout the course of this study. Their expertise and support have played a significant role in the successful completion of this research.
Conflict of interest
The authors affirm that they have no competing interests.
References
1.
KhalafM.A.Al-SaadiB.Q. and EwaidS.H., Evaluation of AHSP Gene Expression and Its Serum Level in Iraqiβ-thalassemia Major Patient, Iraqi journal of biotechnology21(2) (2022).
2.
Al-AliS. and Al-MusawiR., The relevance of rs 34598529 SNP of HBB gene amongβ-thalassemic patients dependent on blood transfusions in Thi-Qar governate, Iraqi Journal of Biotechnology21(2) (2022), 668–676.
3.
MajeedM.S., Evaluation of some Biochemical and Endocrine Profiles in transfusiondependent Iraqi major β-thalassemia patients, Iraqi Journal of Science58(2A) (2022),639–645.
4.
KliegmanR.M.StantonB.M. and GemeJ.S., Nelson textbook of pediatrics, 2(20) (2015).
5.
OrigaR., β-Thalassemia, Genetics in Medicine19(6) (2017), 609–19.
6.
Al-HameedawiA.K. and Al-ShawiA.A., Identification of novel mutations in β-thalassemia patients in Maysan Governorate, Iraq, Molecular Biology Reports50(4) (2023), 3053–62.
7.
MajeedM.S., Evaluation of some Biochemical and Endocrine Profiles in transfusiondependent Iraqi majorβ-thalassemia patients, Iraqi Journal of Science201, 639–6345.
8.
MohammedB.J., Association between TNF-alpha level and TNF-alpha gene polymorphisms in liver cirrhosis of Iraqi patients, Bioscience Research15(2) (2018, 1342–9.
9.
HusseinA.M. and AliH.Z., Detection of TNF Alpha Level as Biomarker in Different Stages of Cutaneous Leishmaniasis Infection, Iraqi Journal of Science (2022), 3313–3321.
10.
KazemiE.JamialahmadiK.AvanA.MirhafezS.R.MohitiJ.PirhoushiaranM.HosseiniN.MohammadiA.FernsG.A.PasdarA. and Ghayour-MobarhanM., Association of tumor necrosis factoα-308 G/A gene polymorphism with coronary artery diseases: An evidenc-based study, J clinical laboratory analysis32(1) (2018), e22153.
11.
MathewS.Abdel-HafizH.RazaA.FatimaK.QadriI., Host nucleotide polymorphism in hepatitis B virus-associated hepatocellular carcinoma, World journal of hepatology8(10) (2016), 485.
12.
MaL.ChenS.MaoX.LuY.ZhangX.LaoX.QinX. and LiS., The association between TNFR gene polymorphisms and the risk of Hepatitis B Virus-Related Liver Diseases in Chinese population, Scientific Reports8(1) (2018), 9240.
13.
MerolaJ.F.EspinozaL.R. and FleischmannR., Distinguishing rheumatoid arthritis from psoriatic arthritis, RMD open4(2) (2018), e000656.
14.
JangD.I.LeeA.H.ShinH.Y.SongH.R.ParkJ.H.KangT.B.LeeS.R. and YangS.H., The role of tumor necrosis factor alpha (TNF-α) in autoimmune disease and current TNF-α inhibitors in therapeutics, International journal of molecular sciences22(5) (2021), 2719.
15.
LaddhaN.C.DwivediM. and BegumR., Increased Tumor Necrosis Factor (TNF) alpha and its promoter polymorphisms correlate with disease progression and higher susceptibility towards vitiligo, PloS one7(12) (2012), e52298.
16.
AbdulhameedS.A. and MohammedB.J., The Relationship of Gene Expression between TNF and TNF-Like Cytokine 1A Genes in Sample of Multiple Sclerosis Iraqi Patients, Iraqi Journal of Biotechnology21(2) (2022), 88–95.
17.
ElahiM.M.AsotraK.MatataB.M. and MastanaS.S., Tumor necrosis factor alpha- 308 gene locus promoter polymorphism: an analysis of association with health and disease, Biochimica et Biophysica Acta (BBA)-Molecular Basis of Disease1792(3) (2009), 163–72.
18.
SambrookJ. and RussellD.W., Molecular Cloning: Ch. 15. Expression of cloned genes in Escherichia coli, Cold Spring Harbor Laboratory Press (2001).
19.
Spss. Statistical package of social science. version 22, application guide: copy right by spss inc. USA. (2013).
20.
GreerJ.P.ArberD.A.GladerB.E.ListA.F.MeansR.M. and RodgersG.M., Wintrobe’s clinical hematology, Lippincott Williams & Wilkins, (2018).
21.
BrissotP.RopertM.Le LanC. and LoréalO., Non-transferrin bound iron: a key role in iron overload and iron toxicity, Biochimica et Biophysica Acta (BBA)-General Subjects1820(3) (2012), 403–10.
22.
De SanctisV.SolimanA.T.ElsedfyH.PepeA.KattamisC.El KholyM. and YassinM., fffhematology9(4) (2016), 401–8.
23.
CarioH.HollR.W.DebatinK.M. and KohneE., Insulin sensitivity and β-cell secretion in thalassaemia major with secondary haemochromatosis: assessment by oral glucose tolerance test, European journal of pediatrics162 (2003), 139–46.
24.
MohammedB.J., TNF-alpha gene polymorphism and its relation to vitamin D, calcium, alkaline phosphatase and ferritin status in Iraqi beta thalassemia patients, Biomedicine42(5) (2022), 906–11.
25.
ZhuangL.MaW.CaiD.ZhongH. and SunQ., Associations between tumor necrosis factorα polymorphisms and risk of psoriasis: a meta-analysis, PLoS One8(12) (2013), e68827.
26.
KimS.D.ParkJ.M.KimI.S.ChoiK.D.LeeB.C.LeeS.H.HongS.J.JinS.Y.LeeH.J.HongM.S. and ChungJ.H., Association of IL-1β, IL-1ra, and TNF-α gene polymorphisms in childhood nephrotic syndrome, Pediatric Nephrology (2004), 295–9.
27.
CavalcanteJ.E.MachadoR.P.LaurentinoM.R.dos SantosT.E.BandeiraI.C.Maia FilhoP.A.FigueiredoM.F.MartinsA.M. and LemesR.P., Clinical events and their relation to the tumor necrosis factor-alpha and interleukin-10 genotypes in Sickle-Cell-Anemia patients, Hematology/Oncology and Stem Cell Therapy9(1) (2016), 14–9.
28.
ZhangD.LiJ.JiangZ.W.YuB. and TangX., Association of two polymorphisms of tumor necrosis factor gene with acute severe pancreatitis, J Surgical Research112(2) (2003), 138–43.
29.
SargenK.DemaineA.G. and KingsnorthA.N., Cytokine gene polymorphisms in acute pancreatitis, JOP J the Pancreas1(2) (2000), 24–35.
30.
PowellJ.J.FearonK.C.SiriwardenaA.K. and RossJ.A., Evidence against a role for polymorphisms at tumor necrosis factor, interleukin-1 and interleukin – 1 receptor antagonist gene loci in the regulation of disease severity in acute pancreatitis, Surgery129(5) (2001), 633–40.