
Abstract
Depending on the characteristics of the cancer and the specific treatment required, each type of cancer comes with a unique set of challenges in the psychological wellbeing of women. This research work mainly focuses on Ovarian cancer since the it is one of the 5
Introduction
Ovarian cancer is the fifth cause of cancer related deaths among women worldwide. The cancer in most women goes undiagnosed until late stages of the disease as the symptoms of the disease remain undetected until III and IV stage which leads to less chances of survival [1, 2].
The treatment usually requires repetitive cycles of chemotherapy and sometimes removal of reproductive organs also [3, 4]. This has a considerable impact on women’s psychological wellbeing. The initial diagnosis of ovarian cancer can contribute to the loss of confidence and cause fear of death [5, 6]. Some women with ovarian cancer also reported feeling isolated and alone due to lack of social support [7, 8, 9]. The impaired physical health associated with both treatment and disease have immense impact on psychological health including anxiety, depression, worrying about death etc. [10].
Recent studies have assessed the psychological impact by using screening tools. The screening in these studies provide insight the psychological impact. There are many tools in the literature used to analyse anxiety and depression among women with ovarian cancer.
The literature survey is broadly classified into two groups:
The tools such as DASS 21 [11], PHQ 9 [12], GAD 7 [13], HADS [14], HSCL-25 [15] are used to analyse the data and statistical tools are used for the prediction of psychological distress. Machine learning models like Logistic Regression [16, 17], Random Forest [18, 19], Naïve Bayes [20], SVM [21, 22, 23] and Neural Networks [24] are used for the prediction of psychological distress in women.
This research paper mainly aims to predict the psychological distress associated with both, having or being at risk of having ovarian cancer using commonly used Machine Learning algorithms and Fuzzy Inference Systems.
The organization of the paper is as follows:
Section 2 provides the detailed literature survey with gaps and problem statement. Section 3 describes the study protocol, data collection and the predictive framework. Section 4 provides the results and the comparative study. Section 5 explains the detailed discussion. Section 6 concludes the paper.
Research suggested that women with cancer are significantly more likely to have mental health issues than other women. The following describes the literature survey carried out to understand the impact of ovarian cancer on mental health.
As per the research work carried out by Bodurka et al. [25], 246 ovarian cancer patients were considered and depression and anxiety likelihood in them is analysed using CES-D and state anxiety subscale of Spielberger state trait anxiety inventory. This research proves that 21% of the patients who participated had depression and 29% had anxiety. The performance is measured using Zubrod score. Further Kornblith et al. [26] considered 151 ovarian cancer women for the study. Using Karnofsky performance status it is found that, out of 151 women, there are 33 women with global psychological distress, 17 with depression, 22 with anxiety and 17 with loss of behavioural emotional control. In the studies of Portenoy et al. [27], it is indicated that the mental health of the women with ovarian cancer is having greater association with physical symptoms and worsening of physical functioning. The performance status was evaluated using Zubrod score to analyse depression, anxiety, and quality of life. Marijke at al [28] considered 238 Dutch patients and 165 Norwegian patients. Using HADS tool, the authors analysed depression and anxiety and found that cancer patients in advanced stages report significantly higher levels of clinical depression symptoms than women in early stages. Similarly, Dena et al. [29] considered 145 ovarian cancer patients. Using the tools SAS, CSE-D, MUIS, SDS, SF-12, the authors performed mean and standard deviation and found that women with ovarian cancer have higher psychological needs than women without ovarian cancer. Erlick et al. [30] considered 157 ovarian cancer women and analysed the designed questionnaire. Spielberger state trait anxiety scale, CES-D scale using
The following gaps are found in literature survey:
The inherent fuzziness of the data has not been considered during the analysis of depression and anxiety. The correlation between anxiety and depression is not taken into consideration during analysis carried out in most of the research. The key factors responsible for depression and anxiety are not systematically studied. The mental health issues are not given due emphasis during the diagnosis, treatment, and the follow-up cycle.
In view the above limitations, the present research work focuses on developing a fuzzy-based intelligent healthcare application system with due attention to the psychological wellbeing of the patient during the treatment of ovarian cancer. In this study an Intelligent system is developed using multi criteria decision making using Fuzzy Sugeno and Mamdani Inference. The obtained results are compared with widely used computational methods and the analysis is presented. The output of the computational methods is also compared with the ground truth provided by the expert psychiatrists.
Study design
The research problem undertaken in this study is the development of a prediction model for mental health of women who are diagnosed with ovarian cancer. Women suffering from ovarian cancer and their caretakers who visited regularly for their treatment and follow ups with the oncology department of SDM Medical College & Hospital, Dharwad were inducted as participants in this study. Pregnant women, women suffering with other cancers were excluded from this study.
The study procedure is explained to the participants. The informed consent of the participants is taken. The ethical approval is obtained from the competent authority of the institution where this study is undertaken. A questionnaire is developed based on PHQ 9 and GDA 7 tools for analysing depression and anxiety with cancer. Table 1 provides the summary of the questionnaire. The study is supervised and validated by the expert panel comprising of a psychiatrist, oncologist, and a gynaecologist.
Data sampling
Women visiting SDM Dharwad who are suffering from early symptoms to advanced stage of ovarian cancer were interviewed by the psychiatrist and responses to the questionnaire were documented. In this process, 590 participants were interviewed, and data was recorded. This data was stored digitally and was used for further computational processing and analysed.
Questionnaire analysis
Table 1 provides a brief description of the questions asked to the participants. At total of 9 questions on depression and 7 questions on anxiety were used for the analysis of mental health of women suffering from ovarian cancer.
Brief description the questions asked to the participants
Brief description the questions asked to the participants
Figure 1 gives the summary of the entire dataset. From the figure, it is observed that 51.9% of the women have depression levels in the range of ‘moderately severe’ to ‘severe’. 80.8% of women have anxiety from ‘moderate’ to ‘severe’. From this it is obvious that ovarian cancer causes, severe anxiety and depression symptoms during the stages of treatment and diagnosis. It is especially high in women who are attending the screening program. During interview process it is noted that the depression and anxiety is mainly due to the surgical menopause, social/socio economic status, family commitments and palliative care.
Depression and anxiety levels in women with ovarian cancer.
From the list of questions, few questions were analysed in detail and the analysis is presented below. From Fig. 2, it is observed that out of 590 women, 366 women expressed moderate to severe anxiety. The following are the reasons expressed for nervousness during the interview. The disease can lead to removal of reproductive organs which in turn can cause natural feeling of losing womanhood and hormonal imbalance in the body. This can reduce the quality of life of the female which can recursively cause the development of psychological depression. Thinking constantly that something will happen to them makes them always feel fear and anxiety. The key point expressed is the family history of losing someone due to cancer.
Analysis of “nervous, anxious, or on edge”.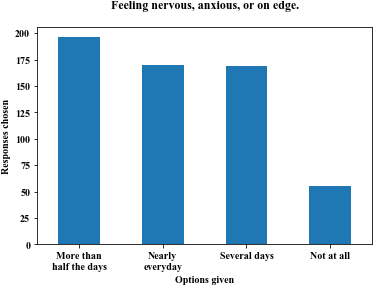
Analysis of “hurting or better off dead”.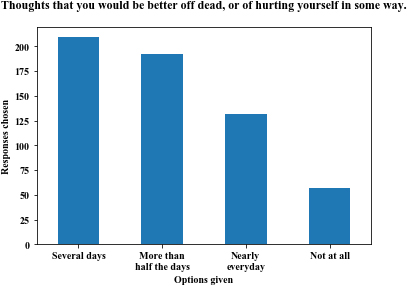
From Fig. 3, it can be observed that out of 590 women with cancer, 132 women feel like hurting themselves or have suicidal tendency every day and 209 women have this feeling for several days. During the interview it is observed that the suicidal feeling/thoughts occurs during the first 3 months after being diagnosed with cancer or in the advanced stage of cancer when women are afraid of years of treatment if the cancer reoccurs. Many women compare themselves with others and feel bad for their condition. Few women expressed the fear of recurrence as “What if I get it again, what am I going to do?”. The younger women with ovarian cancer who participated in the study expressed the feeling of hurting themselves more than the older women.
Analysis of “trouble falling asleep and feeling something awful might happen”.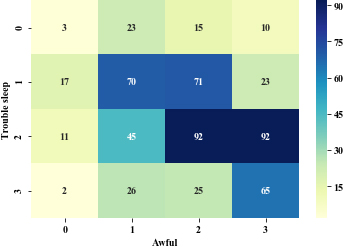
Analysis of “feeling down, depressed and feeling like they have let down their family”.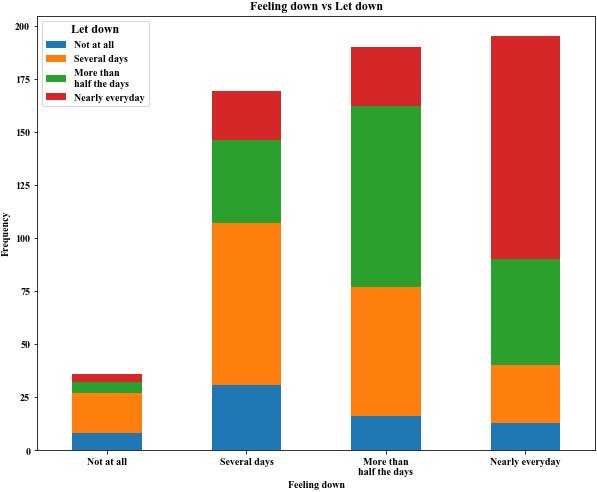
The heat map shown in Fig. 4 is the analysis of two parameters, “Trouble falling or staying asleep or sleeping too much” and “Feeling afraid as if something awful might happen” in women with ovarian cancer, as a grid of coloured squares. In the figure, the colours indicates the values of the variable in the corresponding cell range and it is observed that those who have ‘severe’ fear of something awful might happen also have ‘moderate severe’ trouble falling asleep and those who have ‘moderate severe’ fear of something awful might happen also have ‘moderate severe’ trouble in sleeping. Hence, both of them are closely interconnected. The high values in the diagonal indicate that most people have answered both questions similarly. The least number of values in squares 0-3 and 3-0 also compounds that fact. While only 3 people have stated that they have neither of the two problems i.e., 0-0, many people, 65, have said that they have both the problems nearly every day. 92 people have trouble sleeping more than half the days and feel like something awful might happen nearly every day.
In the analysis from Fig. 1, the women have high anxiety and depression. During the interview process, it is observed that those who have severe depression and anxiety have sleep disturbance. Those who gave higher scores to ‘Feeling nervous, anxious, or on edge’ also selected higher scored option for ‘Feeling afraid as if something awful might happen’. Hence, severe depression and anxiety results in severe sleep disturbance and feeling as if something awful might happen. Few women expressed the urination frequency and pelvic pain which adds to trouble in falling asleep. The details of Fig. 5 are given in Table 2. Very few people have answered “nearly every day” to just one of the questions posed. High values in the diagonal indicate that many people have answered both the questions similarly. Only 8 people have said that they feel neither of the things mentioned whereas the highest number of people, 105, have stated that they feel like they have let themselves or their family down and they also feel down, depressed, or hopeless nearly every day.
Crosstab of the people who feel both that they have let family down and feel down themselves
System architecture.
A woman who has participated in the study is considered as a subject in this research. Women suffering from early stage of ovarian cancer to advanced stage cancer were included in the study. Each woman was interviewed individually on PHQ9 and GAD7 tools by the psychiatrist to analyse the levels of depression and anxiety. The labels for each woman were given based on the final score they acquired by answering the questions. The data was saved in csv file format. Each row indicates the responses given by individual women and the column indicates the questions. Totally 16 questions were asked. For the machine learning purposes, the linguistic responses were converted into numbers which was carried out in the pre-processing stage. The processed dataset was fed into the following classification algorithms – KNN, SVM, Random Forest and ANN. It was split into 70% for training and 30% for testing. The performance of the model was measured in terms of accuracy. In the real world, answers for the questions will be linguistic in nature. The same responses given by the women participants were given to the rule based fuzzy inference system. In this research, the models used are Mamdani and Sugeno. A detailed system architecture is shown in the Fig. 6.
Mamdani-sugeno fuzzy inference systems
Two of the widely used fuzzy inference methods are Sugeno and Mamdani inference engines. In Mamdani fuzzy inference system, for fuzzification singleton with min-max inference process is used. The output is calculated using centre of gravity defuzzification method. Also, Sugeno inference engine is implemented by using singleton method for fuzzification using min max and order 0 inference process. The crisp output is evaluated using weighted average. It is depicted in Table 3.
Different methods for fuzzy inference system
Different methods for fuzzy inference system
As the data is imprecise in nature and there is inherent partial belongingness to a given class, fuzzy theoretic classification methods such as Mamdani and Sugeno inference systems are well suited for modelling the discrete input and output of the questionnaire involving depression and anxiety related questions. The questionnaire designed according to the criteria of PHQ 9 and GAD 7, which is depicted in Table 1, is used to acquire the data from various women participants with ethically approved protocol. Each question has to be answered as one of the four predefined possibilities viz, not at all sure, several days, over half the days, nearly every day. The PHQ 9 and GAD 7 criteria defines 5 (none, mild, moderate, moderately severe, severe) and 4 (Minimal anxiety, mid anxiety, moderate anxiety, severe anxiety) possible severity levels respectively. The aim of this research is to derive the mapping transformation between the depression/anxiety scores to the severity levels. This is achieved using suitably designed linguistic rule base by the expert psychiatrist. Table 4 provides sample fuzzy rules in the rule base for the severity score assessment corresponding to depression. Similarly, the fuzzy rules are designed for anxiety in Table 5.
Scoring system used for depression
Scoring system used for depression
Scoring system used for anxiety
Fuzzy rules to detect depression and anxiety
Fuzzy rules to detect depression and anxiety
Figure 7 depicts the Gaussian membership function and its support. There are 5 membership functions viz, none, mild, moderate, moderate severe and severe corresponding to depression and 4 membership function viz, minimal, mild, moderate and severe corresponding to anxiety.
Membership function of output variable for depression prediction and anxiety prediction.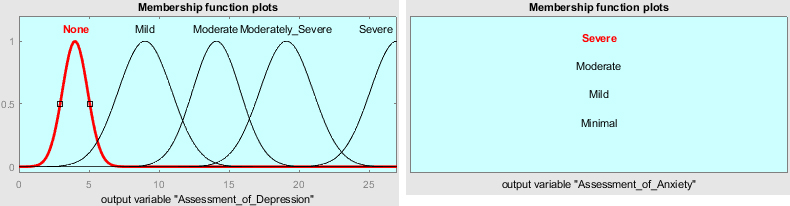
Mamdani-type Fuzzy Inference System was tested on data of 177 patients. It predicted that 171 of them are certainly suffering from depression and 174 women are certainly suffering from anxiety. However, according to the calculations made, 177 patients are suffering from depression and anxiety. The accuracy for depression is found to be 94.3% and for anxiety is 96.7%. Hence, as per the results, Mamdani-type FIS has an error rate of 5.7% which is almost 10 patients and 3.3% or about 5 patients for depression and anxiety respectively.
Based on the analysis, Sugeno-type Fuzzy Inference System is also applied on the 177-patient dataset. According to the Sugeno-type FIS, 173 patients are suffering from depression and 176 from anxiety. However, calculations show 177 patients suffering from depression and anxiety. 96.2% is the accuracy obtained for depression and 98.83% for anxiety. Therefore, upon comparison, Sugeno-type FIS delivers better results for mental health diagnosis. Diagnoses error rates are 3.8% or about 6 patients for depression and 1.17% error for anxiety or about 2 patients for anxiety.
Computational models like linear SVM, KNN, Random Forest and ANN are also applied to the same data. Evaluation metrics show that Linear SVM has predicted that 169 patients are positively suffering from depression and 171 from anxiety out of the 177 patients who are suffering from both depression and anxiety. Linear SVM gives an accuracy of 91.52% for depression and 93.78% for anxiety. Thus, based on the results obtained, linear SVM seems to be a better algorithm for mental health diagnosis. 8% or about 8 patients for depression and 6% error for anxiety or about 6 patients for anxiety are the diagnoses error rates. The performance of the computational models is shown in the Fig. 8.
ANN or Artificial Neural Network is a Deep Learning algorithm. ANNs use weights and bias to decide the predicted output while going through several layers. These layers are usually three types, namely – Input Layer, Hidden Layer and Output Layer. While the input is fed into the Input layer, after computation, the final result is obtained from the Output Layer. A simple ANN algorithm has been used to classify the patients to predict whether they have depression and/or anxiety or not. The accuracy for the current dataset is 72.7% for depression and 79.8% for anxiety. kNN has given the accuracy of 81.35 and 86.44 for depression and anxiety respectively. On the similar lines Random Forest has given accuracy of 76.27 and 92.07 for depression and anxiety respectively as shown in Table 7.
% accuracy for different classification models
% accuracy for different classification models
Performance of the classification models.
In this study an Intelligent system to diagnose mental health and well-being of women who are already undergoing treatment or diagnosis for ovarian cancer is evaluated. The fuzzy inference using Mamdani and Sugeno models is implemented, and its performance is compared with conventional machine learning models. The developed system provides highest accuracy of 96.2% and 98.83% for depression and anxiety respectively using Sugeno Fuzzy inference system. The developed methodology has the following merits:
Women can evaluate the mental health and emotional wellbeing at their own comfort without interfering with their privacy. The developed methodology/techniques can be used for mass screening of women of reproductive age for diagnosing and providing expert advice to the women at a reasonable low cost. The techniques can be used for early detection of mental health issues of women suffering from ovarian cancer. The present fuzzy methodology provides a higher performance in comparison with conventional machine learning methods. Hence the mental health issues can be accurately diagnosed using this methodology.
The present methodology can be further developed to provide promising solution to masses in emergencies, can support global humanity. An appropriate protocol can be designed based on the algorithmic and computer solution to provide a quick solution yet efficient diagnosis of mental health issues among women suffering from ovarian cancer.
Ovarian cancer is a type of cancer with high mortality rate due to late diagnosis. In most of the cases, due to the physical trauma, the mental health issues also aggravate. The present study investigates an algorithmic and computerized solution to diagnose mental health issues. The fuzzy Mamdani and Sugeno inference systems provide an improved performance in diagnosing mental health issues in comparison with conventional machine learning methods. The developed intelligent system has potential application in public health in terms of efficient protocols and faster disposal of cases. Among all the classifiers, Sugeno stands first with an accuracy of 96.2% in predicting depression and 98.83% in predicting anxiety. This acts like a preliminary test to check the patient’s mental health. In case of undesirable results or to be on a safer side, the patient can be recommended to seek professional help to improve their mental health state.
To establish the corelation between depression and anxiety, this research has considered depression of only moderately severe and severe and if the person also has anxiety, then the anxiety severity would be moderate. Similarly, given a person with moderate to severe anxiety and if the person has depression, then the depression severity would be moderate.
Important factors responsible for depression and anxiety during ovarian cancer treatment is the physical condition of cancer, its perceived social stigma, feeling of being looked down by others due to social stigma, health and financial insecurity for the future, possible related health complications and perceived early mortality.