
Abstract
BACKGROUND:
Mounting evidence has demonstrated functional and cognitive-related benefits after Instability Resistance Training (IRT) in individuals, healthy as wellas patients presenting with neurological disorders. However, whether IRT may play a significant role in the postural control of older adults has not been established.
OBJECTIVE:
To evaluate the effects of 12- weeks of IRT on static postural control of older adults with subjective cognitive impairment.
METHODS:
In this randomized controlled trial, a total of 67 participants (aged 65 years and older) were randomly assigned to either 12 weeks of IRT (
RESULTS:
All groups increased AP displacement in the conditions of eyes open and closed. During the eyes-closed condition, only the IRT group increased the ML displacement. No between-group differences were detected in any postural control (
CONCLUSIONS:
12 weeks of IRT does not improve the static postural control in older adults with cognitive impairment.
Introduction
Mild cognitive impairment (MCI) is a well-establised risk factor for cognitive dysfunction, characterized as an intermediate clinical stage between age-related cognitive decline and dementia [1]. The prevalence of MCI increases with chronological age, ranging from 8.4% in people aged 65 to 69 years to 25.2% in individuals aged 80 to 84 years [2]. Although age-related cognitive decline may play a significant role in the onset of neurodegeneration, as in the case of Alzheimer’s Disease [1, 3, 4], cognitive deterioration may affect functional mobility, balance, and postural control, which contributes to a higher risk of falls [5, 6, 7, 8].
Studies have suggested that executive dysfunction (e.g., slow processing speed), neuromotor impairment (e.g., loss of motor units), and progressive failures of the vestibular system can lead to impairment of postural control in older adults with cognitive impairment [9, 10, 11, 12, 13, 14]. Individuals who have poor performance in executive function tasks usually present balance impairment [15, 16]. A systematic review showed that changes in specific parameters of body sway (e.g., higher displacement of the center of pressure (CoP) in the anteroposterior (AP) direction) might precede clinical diagnosis and indicate an early sign of impaired cognitive function [8, 9]. Thus, considering that cognitive deficits can adversely impact the postural control necessary to maintain proper balance [12, 15, 17], preventive and therapeutic interventions to promote postural balance in older individuals are of utmost importance.
Sherrington et al. [18] recently updated the state-of-art regarding the effects of exercise for preventing falls in older people living independently in the community. They outlined that multimodal training, which involves functional exercise and balance challenges, is the most powerful strategy for preventing falls. One strategy is combining moderate-intensity resistance exercise with instability devices or uneven surfaces – Instability Resistance Training (IRT). More than a decade of studies has demonstrated IRT’s efficacy for promoting functional mobility, muscle strength, and cognition in healthy individuals and those with neurological disorders. On the other hand, the effects of IRT on postural control of older adults with cognitive impairment have not been established. Previously, our group demonstrated that older adults with cognitive complaints who underwent IRT improved Timed Up and Go (TUG) performance – a marker of gait stability and postural balance [22].
In healthy older adults with signs and with established cognitive deterioration (e.g., Parkinson’s Disease), IRT protocols were able to improve force production of plantar flexors and knee extensors, promoting significant postural adjustments and limits of stability/verticality as well as contribute to positive changes presynaptic inhibitory mechanisms [21]. Considering that IRT is an exercise intervention that provokes higher neuromotor, vestibular system, and attentional demand [19, 20, 21], we hypothesized that compared with health education control, IRT would promote better postural control outcomes at the completion of the intervention. To shed light on the field, in this work, we examined whether 12 weeks of progressive IRT improved postural control in cognitively impaired older adults. Our primary hypothesis was that participants who underwent an IRT program would improve their static balance compared to a health education control group.
Methods
Study design and ethical aspects
This is a secondary analysis from a previous clinical trial that looked at IRT’s effects on cognitive outcomes. The study protocol and primary findings were published elsewhere [22, 23]. Herein, we explored the role of IRT on postural balance control in older adults with cognitive impairment. Participants were informed about the stages of the project and provided informed consent. The study was approved by the local Ethics and Research Committee (CAAE protocol 81016817.7.0000.5207) and prospectively registered in the Brazilian Registry of Clinical Trials under number RBR-4kqs22 [23]. This manuscript is reported according to the Consolidated Standards of Reporting Trials [24].
Participants, eligibility criteria and randomization
Older adults living in the community and who had subjective cognitive complaints or probable cognitive impairment [Montreal Cognitive Assessment (MoCA)
Participants were randomized after the completion of baseline assessments. The randomization sequence was generated remotely by an independent researcher using free and open-source software (WINPEPI 11.61). Using a series of random numbers, participants were stratified by sex and age, and they were randomly allocated to (1) Instability Resistance Training (IRT), (2) Traditional Resistance Training (RT), or (3) Health Education Control (CON).
Example of instability progression in exercise wall ball squat.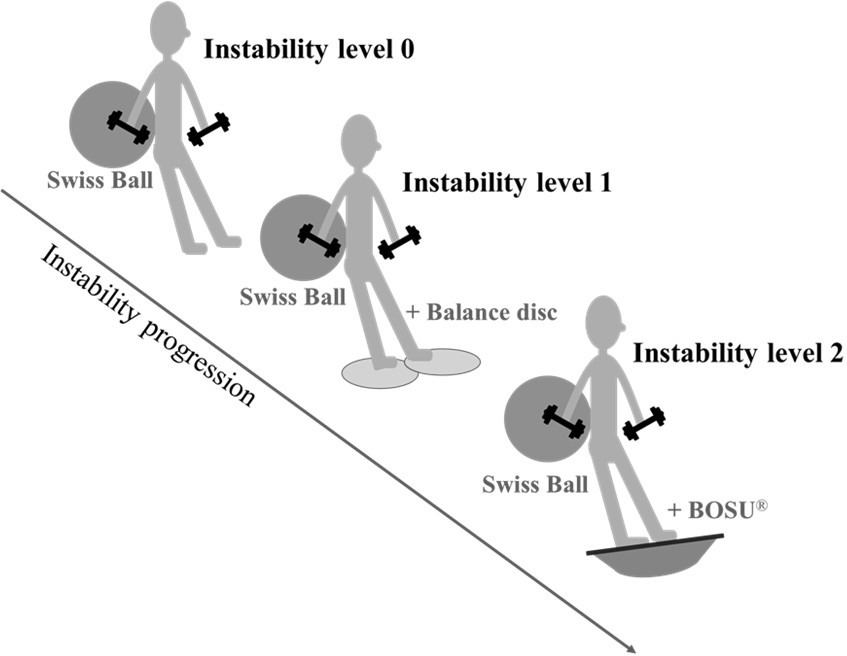
The sample size calculation was performed using the GPower 3.1.9.2 software program (Universitat Düsseldorf, Germany) [26]. The number of participants was calculated based on an 80% probability of detecting an effect size of 0.40 [27], an alpha of 5%, and a correlation of 0.5 between measurements (baseline and follow-up). Thus, a minimum sample of 66 participants was determined, with 22 per group.
Intervention groups
Interventions were delivered from August 27 to November 23, 2018. Before beginning the training program, therapists conducted workshops to properly provide exercise and health education sessions.
RT program was distributed in 3 mesocycles of four weeks, with a frequency of 3 times a week on alternate days (Monday, Wednesday, and Friday). The training program consisted of 7 exercises in an alternating follow-up setup (wall ball squat, chest press using free weights, horizontal leg press, seated cable row, pelvic elevation, standing calf raise, and abdominal exercises) using free weights and machines (Physicus, Auriflama – SP, Brazil) performed at the same time of day (morning). The prescription involved three fixed sets and repetitions ranging from 10–15 repetitions maximum (RM). For the abdominal exercise, the prescription involved performing three sets of 15–30 RM or time ranging from 10–30-s of isometric contractions. The recovery interval between sets was 60 to 90-s, and between two to 3-min between exercises. The exercise protocol was based on the American College of Sports Medicine (ACSM) recommendations for resistance training for older adults [28].
The IRT group performed the same training program as the RT group. However, in this proposal, instability devices (balance disc, physioball, BOSU
A minimum load of free weights and machines characterized the first week of training (both groups). The main objective at this stage was to provide learning of the exercises and guarantee safety in the execution, meaning familiarization. All participants were instructed to maintain a constant movement speed in the proportion of approximately 1:2 (concentric and eccentric phases, respectively) and to maintain focus during the exercises. Training progression and load readjustment were performed according to the ACSM recommendations [28], so when the upper limits of the target zone were completed for three consecutive training sessions, the load was increased by 2–5% for upper limb exercises and 5–10% for lower limb exercises for the next session. Additionally, all sessions were supervised by trained therapists to ensure that the exercise was performed correctly.
Participants assigned to the health education group received weekly group meetings to provide health education activities. These included lectures on the prevention and treatment of chronic diseases, discussions on the importance of maintaining a healthy lifestyle, and light-intensity stretching and relaxation sessions throughout 12 weeks.
Descriptive measures
The participants’ general characteristics, such as gender, age, education level, and clinical history, were obtained through an interview. We measured body mass (kg) and height (meters) and then calculated body mass index (kg/m
Static postural control
A ground reaction force platform (Model OR6-7, 3.05, AMTI, USA) was used to assess the static postural control of the participants through linear recordings of the center of pressure (CoP) in the anteroposterior and mediolateral axes. Data were collected at 1000 Hz and low-pass filtered (2nd order, zero-phase-lag, Butterworth, cutoff frequency of 5 Hz). The parameters were characterized according to the oscillation time and frequency, and the extracted data included the anteroposterior (AP) and mediolateral (ML) displacements (in cm) of the total CoP oscillation.
Platform calibration was performed with the participants remaining in a bipedal stance, with their feet comfortably apart (hip width) and looking at a fixed target for 10-s. Trials were performed under bipedal support with eyes open and closed. Participants were asked to stand on a force platform in the same posture and keep it for 30 s with eyes concentrating on a black cross marked 1.5 m away on the wall. CoP area was calculated considering 93% of the data points, with the first and last second removed to avoid initial oscillations and anticipation effects, respectively. At the end of the evaluation, all recorded data were stored on a laptop, and the signals were processed using a standardized MATLAB
Statistical analysis
Statistical procedures were performed using the SPSS version 22 software program (IBM SPSS Corporation, New York, USA), considering a
Results
A total of 167 participants underwent an initial screening, of which 94 were excluded for not meeting the inclusion criteria. Considering the 73 participants who met the eligibility criteria, six were excluded (one for refusing to participate in the evaluations and five for personal reasons). Thus, after completing the baseline assessments, 67 participants were randomized to the IRT (
CONSORT flow diagram. RT, resistance exercise training; IRT, instability resistance training.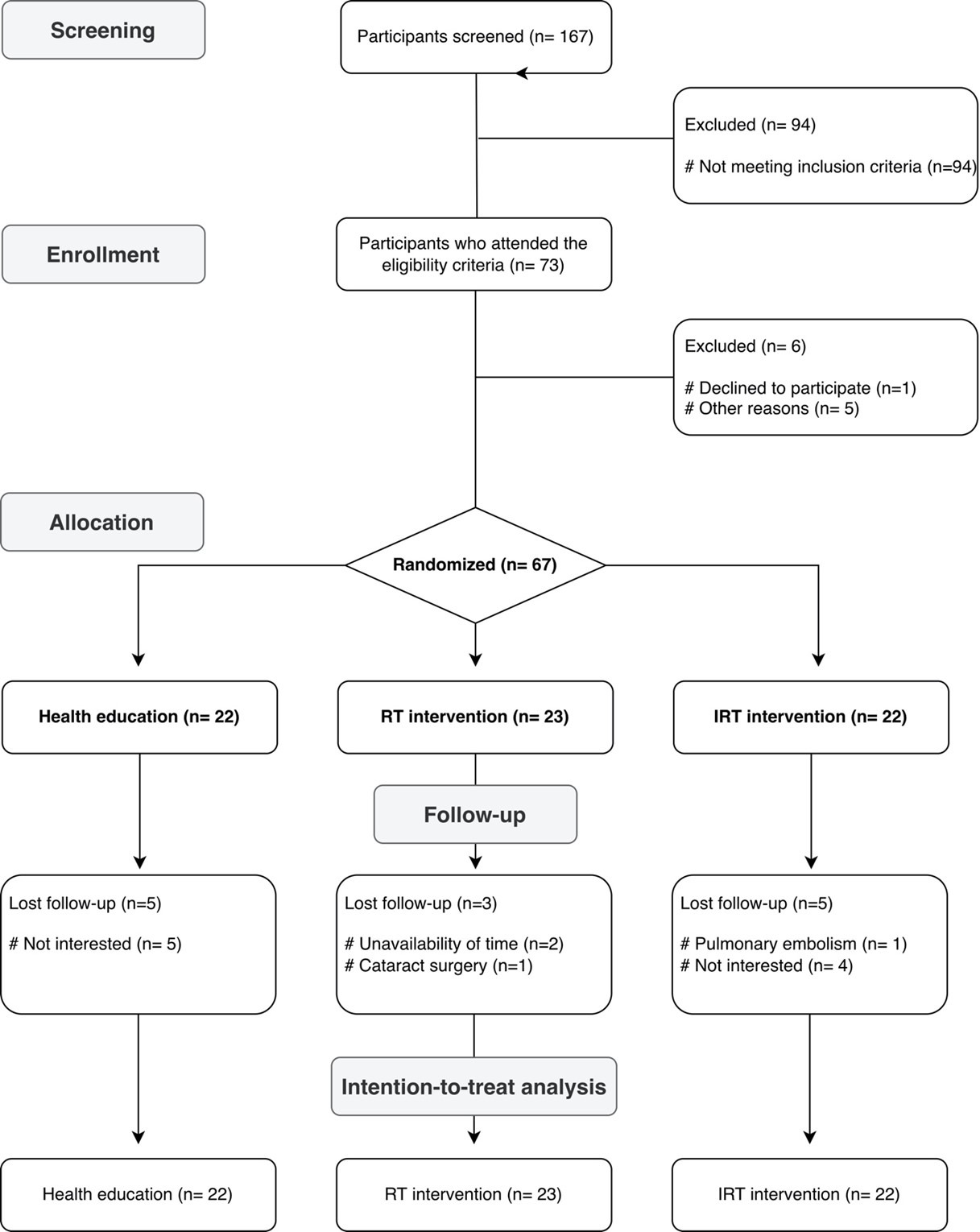
Baseline characteristics of participants according allocation group (
IRT, instability resistance training; RT, resistance exercise training; CON, control; BMI, body mass index; MoCA, Montreal Cognitive Assessment; AP, anteroposterior; ML, mediolateral; OE, open eyes; CE, closed eyes. Note: Data are presented as mean (SE) or absolute (%) values.
Static postural control performance in the anteroposterior (A-P) and mediolateral (M-L) CoP sway in the two experimental (IRT and RT) and control groups at baseline and follow-up.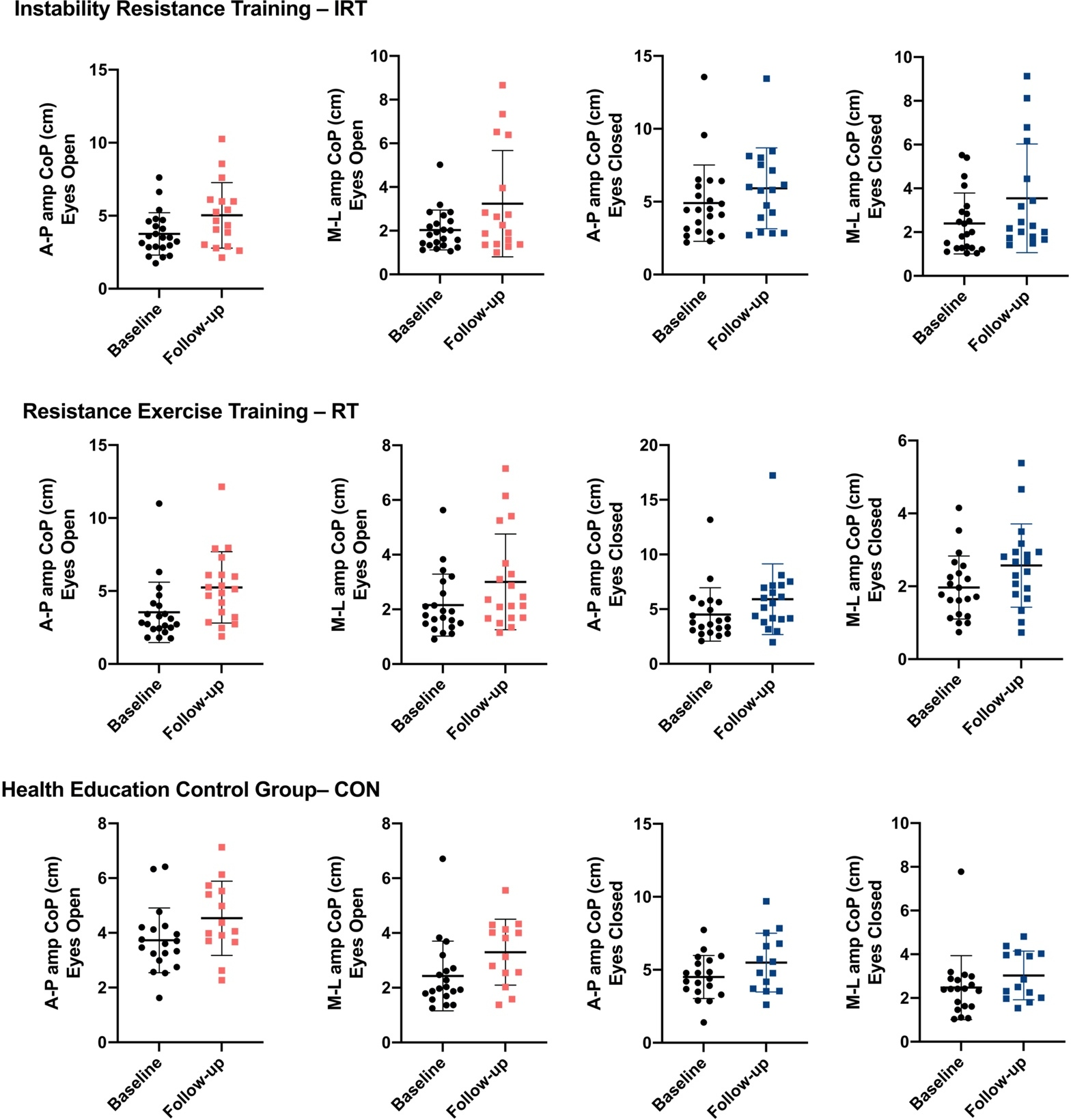
Table 1 presents descriptive information about the participants’ characteristics according to the intervention group (Table 1). There was a higher prevalence of women with a mean age of 71 years (77%), overweight (mean BMI
Figure 3 shows the results of training with resistance exercises on static postural control of participants during the standing position using bipedal support with eyes open and closed (Fig. 3).
In the condition with eyes open, the three groups increased AP (IRT: 1.243; 95% CI: [0.635; 1.852];
Despite the within-group changes in the aforementioned variables, no between-group differences were detected in any postural control markers after the intervention (
This exploratory study examined the effects of resistance exercise with and without instability devices /surfaces on static postural control indicators in older adults with cognitive impairment. The key findings revealed that compared with the control group, both training protocols (IRT and RT) did not promote significant changes in static postural control (AP and ML displacement of CoP during eyes opened and closed paradigms) at the completion of the 12-week intervention.
It is known that cognitive impairment affects postural control mechanisms, and specific changes in body sway parameters may often precede the clinical diagnosis of cognitive decline [8, 9, 15]. It is believed that cognition deficits cause a reduction in sensorimotor skills, progressive failures of the vestibular system, and impairments in the processing of visuospatial information and executive functions. This significantly reflects in maintaining posture and balance [9, 10, 11, 12, 13, 14]. Different studies have shown that postural control is negatively affected by the degree of cognitive impairment [9, 13, 15, 32, 33].
In this context, it was expected in this study that 12 weeks of IRT would promote better results in static postural control of older adults with cognitive impairment compared to the health education group. However, contrary to expectations, neither the traditional TR nor the IRT was superior to the CON after the intervention period. In this regard, although some studies report improvements with isolated resistance training or using instability devices in the balance of healthy older adults [20, 34, 35], it is not yet clear whether individuals with cognitive impairment respond similarly to training compared to people without cognitive complaints [36]. Therefore, it is necessary to consider that the investigated population has specific characteristics of cognitive involvement that can affect the ability to respond to the intervention since these subjects have more pronounced difficulties in sensory, vestibular, and proprioceptive integration, which are essential for maintaining control posture [13, 36, 37, 38].
Another factor that must be considered is related to the training program with unstable devices. Although not all exercises directly involve muscle groups that help to maintain the center of mass over the base of support in our protocol, previous evidence led us to hypothesize that motor complexity and a challenging intervention could be enough to promote positive responses in control posture [21, 22, 29], considering that a similar intervention study observed that the IRT promoted postural adjustments that favored the improvement of body alignment and stability limits in older adults with Parkinson’s disease (PD), whose cognitive dysfunction is a common feature [21]. However, the real mechanisms and specific characteristics of the training protocol capable of increasing the balance function in these individuals have not yet been fully defined [36].
A possible speculation would be that a more specific exercise program involving muscles that act in balance control or mainly integrate physical-cognitive training (dual task) is more likely to obtain such benefits [36, 39, 40, 41], as it has been proven that the domains of cognition and postural control are interrelated and share neural substrates in older adults [42]. Thus, although the IRT requires a greater attentional demand during its execution [21], perhaps adopting strategies focused on combining physical training associated with cognitive tasks performed simultaneously may be more advantageous to improve postural control of older adults with cognitive déficits [36].
Despite this, clinical trials carried out with populations that also have postural instability have shown significant results from training using unstable devices/ surfaces in improving this component [21, 43]. However, the postural control system acts differently in dynamic and static activities. These studies could observe this effect only when dynamic evaluation measures or more challenging balance tasks (for example, Balance Evaluation Systems Test – BESTest; single-legged condition) [21, 43]. Considering that more significant challenges to postural control may be better to indicate differences in body stability [42], the assessment of only one static test in this study and without any additional challenge for maintaining posture may not have been sensitive enough to detect possible changes with training.
This hypothesis is supported by analyzing a study that investigated shared neural substrates of postural control and cognitive status in older adults with normal cognition, mild cognitive impairment, or dementia [42]. When using computerized metrics of postural sway while performing tasks that require varying levels of visuospatial attention, no significant associations were found between cognitive status and postural sway during conventional tasks, for example, standing on flat or foam surfaces with eyes open or closed on a force platform. In contrast, significant results were observed when examined in a more challenging condition requiring higher levels of visuospatial attention – one visual tracking task (VT) – significant results were observed. Thus, the use of VT promoted a greater demand for maintenance postural control, probably due to the increased need for cognitive information, such as attention [42]. Therefore, measures that include postural and cognitive elements may enable the detection of more subtle changes in this outcome [42].
This study has a few limitations that should be mentioned. Firstly, the current study is a secondary analysis from a trial that primarily investigated the effects of IRT on the cognitive functioning of older people. Further experimental studies are needed to address this specific issue and shed light on the field. Secondly, our study explored the role of IRT on static postural control by withdrawing exteroceptive stimuli (e.g., eyes closed) during bipedal upright posture. We acknowledge that analyzing the role of IRT from challenging paradigms (e.g., unipedal support) or conditions that require dynamic postural control (e.g., gait) would provide a unique opportunity to understand balance and posture adaptations of motor complexity training. Our findings cannot be interpreted considering the participant’s features. Generalizations covering other age groups (e.g., nonagenarians), multimorbidity, and individuals with neurological issues should be made cautiously.
Conclusion
In conclusion, this exploratory study showed 12 weeks of moderate-intensity resistance training combined with instability devices/surfaces did not improve static postural control among cognitively impaired older adults residing in the community. Further randomized trials are needed to clarify IRT efficacy on the balance and posture outcomes of older people.
Author contributions
CONCEPTION: Bruno Remígio Cavalcante, Mariana Ferreira de Souza and Rodrigo Cappato de Araújo.
PERFORMANCE OF WORK: Vinicius Yan Santos Nascimento, Bruno Remígio Cavalcante, Francis Trombini de Souza, Mateus Santos Silva, Dayane Tays da Silva, Mariana Ferreira de Souza and Rodrigo Cappato de Araújo.
INTERPRETATION OR ANALYSIS OF DATA: Vinicius Yan Santos Nascimento, Bruno Remígio Cavalcante and Rodrigo Cappato de Araújo.
PREPARATION OF THE MANUSCRIPT: Vinicius Yan Santos Nascimento, Bruno Remígio Cavalcante and Rodrigo Cappato de Araújo.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: Vinicius Yan Santos Nascimento, Bruno Remígio Cavalcante, Francis Trombini de Souza, Mateus Santos Silva, Dayane Tays da Silva, Mariana Ferreira de Souza and Rodrigo Cappato de Araújo.
SUPERVISION: Bruno Remígio Cavalcante, Mariana Ferreira de Souza and Rodrigo Cappato de Araújo.
Ethical considerations
All participants provided informed consent. The study was approved by the local Ethics and Research Committee (CAAE protocol 81016817.7.0000.5207). This trial was prospectively registered in the Brazilian Registry of Clinical Trials under number RBR-4kqs22.
Funding
None.
Footnotes
Acknowledgments
We want to thank all study participants. Vinicius Yan Santos Nascimento was supported by the Fundação de Amparo à Ciência e Tecnologia do Estado de Pernambuco (FACEPE).
Conflict of interest
The authors have no conflicts of interest to report.