
Abstract
Keywords
INTRODUCTION
Frontotemporal dementia (FTD) is the second most prevalent type of dementia and typically occurs much earlier in life than Alzheimer’s disease (AD) [1, 2]. The behavioral variant (bvFTD) is the most frequent presentation in the clinical spectrum of FTD, accounting for approximately half of all FTD cases [3, 4]. Despite the heterogeneity in its clinical presentation, bvFTD is characterized by progressive personality and/or behavioral changes [5, 6] associated with bilateral symmetrical frontal and anterior temporal atrophy/hypometabolism [7].
The current criteria for the diagnosis of bvFTD are based on behavioral features and a neuropsychological profile that includes a relative sparing of episodic memory [8]. Severe amnesia is thus not contemplated as a possible clinical presentation of bvFTD in the current diagnostic criteria, but accumulating evidence suggests that memory can be notably impaired, even in early stages of the disease [9, 10]. Recently, several studies have indicated that episodic memory deficits are more frequent in bvFTD than previously believed, and that they may even be as severe as in AD [11–13]. With respect to the characteristics of their memory problems, bvFTD patients were supposed to exhibit more “frontal-executive” deficits, such as problems in organizing strategies during learning [14–16] or in retrieving information rather than storing it [14–17]. By contrast, AD patients have been claimed to show mainly consolidation deficits [14, 17]. However, some imaging studies have shown that temporo-mesial/hippocampal structures and the Papez circuit are affected in bvFTD, suggesting that amnesia could be due to defects in memory storage and consolidation processing [18–20] rather than a deficit of frontal lobe-based strategies of memory recall, as was previously suggested [14–17]. Accordingly, it has been claimed that bvFTD cannot be clearly distinguished from AD on the basis of memory test performance [9, 17], at least not on the individual level relevant for diagnostic classification [21].
To our knowledge, there are few studies in which memory performance and its neuroanatomical correlates has been simultaneously assessed in both AD and bvFTD [11, 23]. While some authors reported different neural correlates [11, 12], others described common neuroanatomical substrates underlying memory disturbance in both dementia categories [22, 23]. These inconsistencies across studies may be due to patient group characteristics such as severity of the disease, different episodic memory tests employed, or indeed the method of imaging analysis used in patient cohorts.
Episodic memory refers to the ability to consciously encode, store, and retrieve information about previously experienced events, and typically involves the recollection of details about the event embedded within a spatiotemporal framework. The Free and Cued Selective Reminding Test (FCSRT), is a multi-trial memory test that uses a “selective reminding” paradigm by presenting only the words not recalled, instead of all the to-be-remembered words, thus directing the subject’s attention to the words not recalled on the previous trial [24]. This test provides objective measures of the main processes of episodic memory: 1) encoding, which involves attentional processes; 2) consolidation; and 3) retrieval of the learned material. The cued recall technique used in the FCSRT aims at enhancing both the encoding and the retrieval phases, to control the effect of impaired attention and inefficient retrieval strategies due to executive dysfunction and therefore to identify a pure memory deficit [24].
Our main purposes were to assess episodic memory function by the FCSRT in a group of bvFTD patients comparatively with AD patients and analyze the relationship between episodic memory and brain metabolism measured using positron emission tomography imaging with 18F-fluorodeoxyglucose (FDG-PET).
METHODS
Subjects
Seventy-nine participants were recruited from the Cognitive and Behavioral Neurology Unit at our center. The total included 29 individuals with clinical criteria of AD, 26 with probable bvFTD, and 24 healthy controls (HC).
Patients were diagnosed using current diagnostic criteria [8, 25] after a comprehensive evaluation including: neurological history and examination, neuropsychological testing of memory, executive function, language, visuospatial and visuoperceptive function, and praxis, and structural magnetic resonance imaging (MRI) or computerized tomography (CT) brain scan. The exclusion criteria were: age before 45 or over 90, systemic disease with potential impact on cognition, presence of intracranial lesions or significant white matter disease, psychiatric disorder, changes on dementia drugs or other medications that could affect cognition in the last three months before recruitment, and severe visual or hearing impairments. HC group consisted of caregivers or patients’ companions without cognitive or behavioral complaints. The inclusion criteria for this comparison group were as follows: age over 18 and before 90, no acute systemic diseases in the last year, no central nervous system or systemic disorders that could affect cognition, no psychiatric disorder at the moment of evaluation, no visual, hearing, or physical impairments, MMSE score higher than 24 on the 30-point, less than 8 on Hamilton Depression Rating Scale, and Clinical Dementia Rating score equal to 0. All subjects and/or their legal representatives signed the informed consent for the study, which was approved by the institutional Ethics Committee.
Demographic and clinical data from participants was registered at the time of recruitment. Subjects were assessed using the Spanish version of the FCSRT [26, 27]. In addition to the FCSRT, other neuropsychological tests included in the NEURONORMA project [28] were performed in order to evaluate other cognitive functions: the Digit Span to assess attention and working memory; the Trail Making Test (A and B) to measure speed of attention, working memory, and divided attention; the symbol digit modality test (SDMT) to assess psychomotor speed; the Boston Naming Test (BNT) to evaluate language function; the Rey-Osterrieth Complex Figure Test (ROCF) to assess planning, organizational skills, and problem-solving strategies (copy), as well as visual episodic memory function (immediate and delayed recalls, and recognition subtest); the formal and semantic verbal fluency tasks (words starting with “p” and animals, respectively) to evaluate the spontaneous production of words; the Stroop test (A, B and C) to assess speed of attention, inhibition of, and overlearned response and flexibility, the Tower of London test (ToL) to measure planning, rule learning, and inhibition; and the Visual and Object Perception Battery (VOSP) to evaluate visuospatial and visuoperceptive skills. Scaled scores of each test were calculated by correcting raw scores for age and education. Following the NEURONORMA authors’ recommendations, a scaled score ≤6 (percentile ≤10) was considered deficient.
Global cognitive functioning was determined using Mini-Mental State Examination (MMSE) [29] and Addenbrooke’s Cognitive Examination (ACE) [30], which measures attention, memory, fluency, language, and visuospatial function. Furthermore, the validated Spanish versions of the following instruments were administered: the Interview for Deterioration in Daily Living Activities in Dementia (IDDD) [31] and the Functional Activities Questionnaire (FAQ) [32, 33].
FCSRT procedure
The Spanish version of the FCSRT was administered following the author’s instructions [27]. The 16 items to be learned were presented four at a time on a card, one printed word in each quadrant. The test started by asking subjects to read aloud each item. Afterwards, subjects should identify each item after its semantic cue was aurally presented. After identification of all 16 items, three recall trials were performed, each preceded by 20 seconds of counting backward to prevent recall from short-term memory. Each recall trial consisted of two parts. First, each subject had up to 90 seconds to freely recall as many items as possible. Next, aurally presented category cues were provided for items not retrieved by free recall. During the first two recall trials, if subjects failed to retrieve the item with the category cue, they were reminded by presenting the cue and the item together. The same procedure of recalling (freely and cued) was done after a 30-min interval, during which subjects were required to perform non-verbal tasks. The test allowed the measure of the following variables: 1) free recall of first trial (maximum score: 16); 2) total free recall (sum of free recall of each three recall trials; maximum score: 48); 3) total recall (sum of total free and cued recall; maximum score: 48), 4) free delayed recall (maximum score: 16); and 5) total (free plus cued) delayed recall (maximum score: 16).
bvFTD patients were divided into two subgroups according to their memory scores. We chose a delayed total recall on the FCSRT equal to six as cutoff, which had been previously demonstrated to be highly sensitive and specific for early AD. We designated bvFTD patients with delayed total recall scaled scores equal or below six as amnestic-FTD and those with memory scores above six as non-amnestic-bvFTD.
PET acquisition and pre-processing
All participants underwent FDG-PET brain scans with a Siemens Biograph TruePoint PET-CT using a 6-detector CT with a high-resolution lutetium oxyorthosilicate PET scanner. Clinical evaluation and PET imaging were obtained with an interval of less than 30 days. Studies were performed after 6-hour fasting and at rest. FDG (5 mCi) was administered intravenously. The CT scan parameters were the following: kVp/effective mAs/rotation 130/40/1; slice thickness 3 mm; reconstruction interval 1.5 mm, and pitch 0.75. Two raters blinded to clinical diagnosis performed independent visual analysis of each FDG-PET brain scan on a Siemens Leonardo workstation. Cerebral metabolic brain pattern was consistent with clinical diagnosis in all cases [34]. Statistical parametric mapping (SPM8) software (The Wellcome Trust Centre for Neuroimaging, Institute of Neurology, University College of London, UK) was used for imaging preprocessing and statistical analyses. Images were first transformed from DICOM to NifTI-1 format using MRIConvert version 2.0 (Lewis Centre for Neuroimaging, University of Oregon, Eugene, OR, USA). The images of all subjects were spatially normalized to the reference space of the Montreal Neurological Institute employing our own workgroup template [35] and later underwent smoothing with full width at half maximum of 12 mm. Images were normalized to the whole cerebellum as reference region (cerebellum normalization) [36].
Clinical data analysis
Statistical procedures of clinical data were performed using IBM® SPSS Statistics for Mac 20 (IBM, Chicago, USA). Demographic and clinical characteristics were compared among groups using the one-way analyses of variance (ANOVA) or the Kruskal Wallis test or the Mann-Whitney U test for continuous variables and the chi-square test or Fisher’s exact test for categorical ones. The latter were expressed as frequencies, whereas continuous variables were expressed as mean±standard deviation (SD). Bonferroni post hoc test was used to adjust for multiple comparisons. The correlation between the total delayed FCSRT score and performance on the other neuropsychological tests was analyzed using Spearman correlation coefficient (rs) Statistical significance was considered whenp≤0.05.
Voxel-based imaging analysis
Brain glucose metabolism of each diagnostic category was compared with the group of HC using the two-sample t test with age and gender as covariates. Brain PET images of amnestic and non-amnestic-FTD subjects were compared using the two-sample t test with age, gender, and cognitive performance on the MMSE as covariates. In addition, multiple regression analysis was employed to establish the correlation between total recall and total delayed recall score on the FCSRT and brain metabolism, with age, sex, and cognitive performance on the MMSE as covariates. An uncorrected p value of <0.001 or a family-wise error rate (FWE) corrected p value of 0.05 were used as a statistical threshold. Clusters of at least 50 voxels were considered significant. Results from the SPM map were further represented on MR images using the MRIcron viewer (2012 version).
RESULTS
Clinical and demographic characteristics
Demographic and clinical characteristics of subjects are shown in Table 1. There were no statistically significant differences on age or education among the three groups. bvFTD subjects showed a higher frequency of males than AD patients (bvFTD versus AD: 61.5% versus 24.1%; adjusted p = 0.015), but no differences were found between HC and the two dementia groups with regard to gender.
Demographic and clinical data in bvFTD, AD, and healthy controls
Data presented as the mean (standard deviation) or as the percentage (n). Statistical significance was considered when p≤0.05 (Mann Whitney U test for quantitative variables; chi-square test or Fisher’s exact test for qualitative variables; Kruskal Wallis test for comparing quantitative variables between more than two groups). bvFTD, behavioral variant of frontotemporal dementia; AD, Alzheimer’s disease; HC, healthy controls; SD, standard deviation; FAQ, Functional Activities Questionnaire; IDDD, Interview for Deterioration in Daily Living Activities in Dementia; ACE, Addenbroke’s Cognitive examination. abv FTD versus AD, adjusted p = 0.015. bbv FTD versus HC, adjusted p = 0.018; AD versus HC, adjusted p < 0.001. cbv FTD versus HC, adjusted p = 0.002; AD versus HC, adjusted p < 0.001.
HC scored higher on MMSE than the other two groups (HC versus bvFTD: 27.54±2.64 versus 22.86±5.89, adjusted p < 0.001; HC versus AD: 27.54±2.64 versus 21.24±5.33, adjusted p < 0.001). BvFTD and AD groups were comparable with respect to functional level and cognitive performance on screening tests.
Episodic memory performance
For all subtests of verbal memory, bvFTD patients performed significantly lower than control subjects and better than AD patients (see Fig. 1A-C). With regards to visual memory performance, bvFTD patients scored significantly lower than AD patients, with no differences with the control group (Table 2).
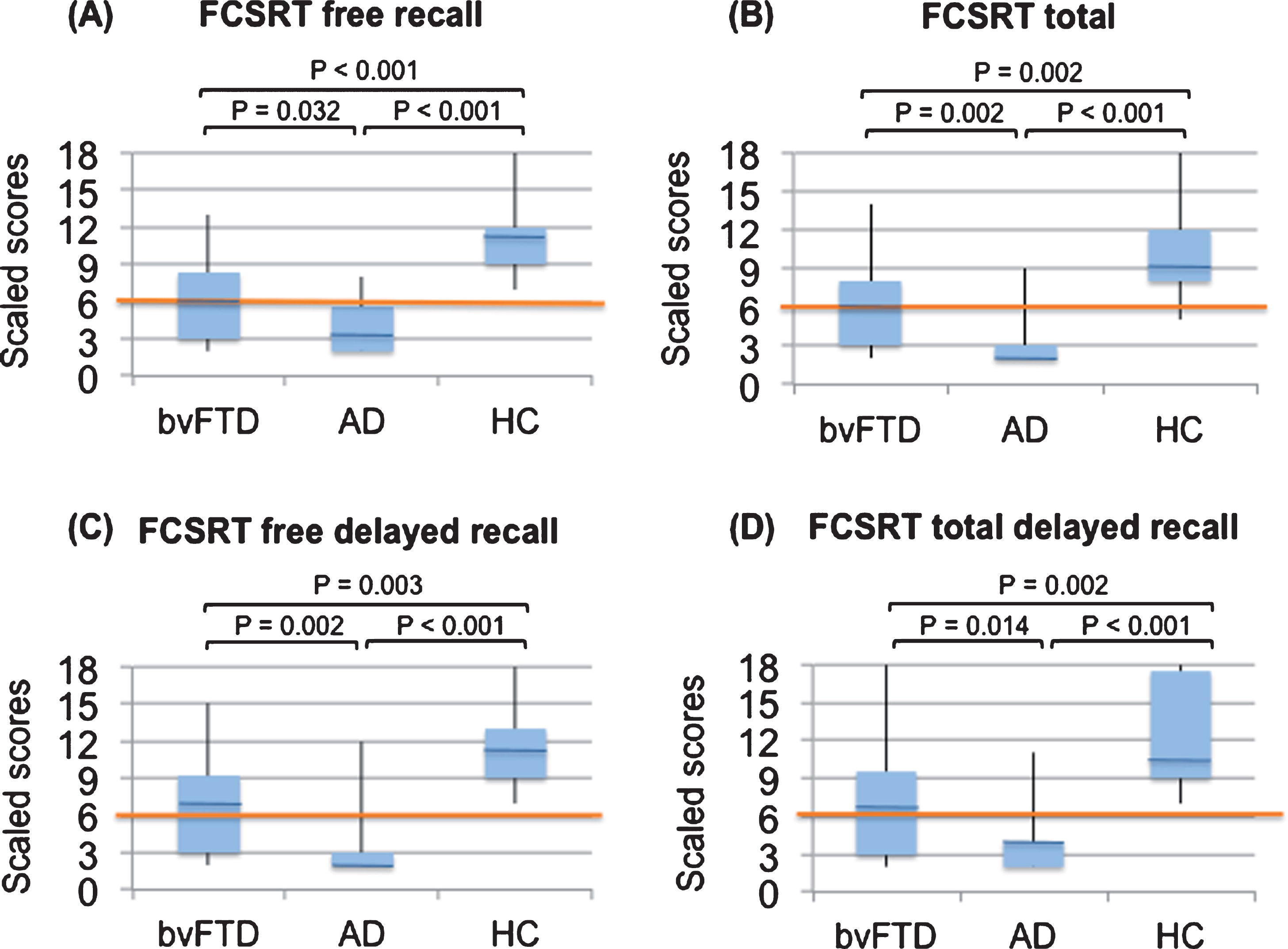
Scaled scores in the Free and Cued Selective Reminding Test during the free total A), total B), free delayed C), and total delayed D) recalls. bvFTD, behavioral variant frontotemporal dementia; AD, Alzheimer’s disease; HC, healthy controls.
Mean (SD) scores for amnestic-FTD, non-amnestic-FTD, AD, and HC on demographics, clinical data and neuropsychological tests
Data presented as the mean (standard deviation) or as the percentage (n). Results reflect scaled scores on each test, adjusted by age and education. A scaled score ≤6 was considered deficient. Statistically significant p values are shown in bold (chi-square test or Fisher’s exact test for qualitative variables; Kruskal Wallis test for quantitative variables). FTD, frontotemporal dementia; AD, Alzheimer’s disease; HC, healthy controls; ROCF, Rey-Osterrieth Complex Figure Test; FCSRT, Free and Cued Selective Reminding Test; ToL, tower of London; VOSP, visual object and space perception. aSignificant difference compared with non-amnesic-FTD subjects. bSignificant difference compared with control subjects. cSignificant difference compared with AD.
The analysis of the distribution of FCSRT delayed total recall scores using the Kolmogorov-Smirnov and the Shapiro-Wilk tests revealed that the scores were not normally distributed in the bvFTD group (Kolmogorov-Smirnov: p = 0.013; Shapiro-Wilk: p = 0.015), which could be confirmed by a visual check of the histogram distribution. We observed that half of the bvFTD sample (n = 13)presented deficient scaled scores (amnestic-FTD), while the rest of bvFTD patients (n = 13) performed well on this memory subtest (non-amnestic-FTD).
Characterization of amnestic and non-amnestic-bvFTD patients
Table 2 displays demographic, clinical data, and neuropsychological scores of amnestic-FTD, non-amnestic-FTD, AD, and HC. There were no significant differences in age, gender, education, illness duration, working memory (digit span), other executive cognitive scores (TMT, SDMT, Stroop, ToL, verbal fluencies), language (BNT), or visuospatial and visuoperceptive skills (VOSP) between amnestic and non-amnestic-FTD subjects. Amnestic-FTD scored lower than non-amnestic-FTD on ROCF subtests, but these differences did not reach statistical significance. Within bvFTD sample, FCSRT delayed total recall raw scores showed a low correlation with TMT B (rs : –0.464; p = 0.034) and SDMT (rs : 0.452; p = 0.030). There was no significant correlation among FCSRT delayed total recall scores and the rest of neuropsychological tests administered other than the FCSRT (Table 3). When amnestic and non-amnestic-FTD subgroups were analyzed separately, we neither found any significant correlation among FCSRT total delayed recall nor the other cognitive tests performed (Table 3).
Correlation among FCSRT total delayed recall raw scores and other neuropsychological tests in bvFTD, amnestic-FTD, and non-amnestic-FTD groups
Statistically significant p values are shown in bold. bvFTD, behavioral variant frontotemporal dementia; ROCF, Rey-Osterrieth Complex Figure Test; FCSRT, Free and Cued Selective Reminding Test; ToL, tower of London; VOSP, visual object and space perception.
Amnestic-bvFTD patients performed similarly to AD patients for each episodic verbal memory score, with both groups scoring significantly lower than non-amnestic-FTD and HC (p < 0.001). For non-amnestic-FTD subjects, performance on FCSRT total recall, free delayed recall, and total delayed recall were comparable to HC (Table 2, Fig. 2).

Mean scaled scores on Free and Cued Selective Reminding subtests for amnestic-FTD, non-amnestic-FTD, AD, and HC. FTD, frontotemporal dementia; AD, Alzheimer’s disease; HC, healthy controls; NS, non-significant.
Voxel-based PET imaging analysis
bvFTD group showed bilateral hypometabolism in anterior cingulate, prefrontal, and temporal regions (p < 0.05 FWE). Patients with AD presented hypometabolism in posterior cingulate, and bilateral temporal (inferior and middle temporal gyri, subgyral region) and parietal cortex (precuneus, angular gyrus) (p < 0.05 FWE). For more details, see Supplementary Table 1.
Compared with non-amnestic-FTD subjects, amnestic-FTD showed significantly bilateral lower metabolism in inferior temporal gyri and uncus (Brodmann areas - BA- 20 and 28) (p < 0.001) (Figs. 3 and 4; for more detailed information see Supplementary Tables 2 and 3). Within the bvFTD group, FCSRT total delayed recall score showed an inverse correlation with bilateral inferior temporal gyri and right uncus metabolism (BA 20) (p < 0.001) (Fig. 5B; Supplementary Table 4). Similarly, FCSRT total recall was inversely associated with metabolism in right parahippocampus, right uncus, and left inferior temporal gyrus (BA 28, 36 and 20) (p < 0.001) (Fig. 5A; Supplementary Table 4), and FCSRT free delayed recall with left inferior temporal and superior frontal gyri metabolism (BA 28, 36 and 20) (p < 0.001) (Supplementary Table 4). In AD sample, FCSRT total delayed recall showed an inverse association with bilateral uncus and parahippocampal gyri metabolism (BA 36) (p < 0.001) (Fig. 5B; Supplementary Table 5). Likewise, FCSRT total recall was inversely correlated with bilateral parahippocampal gyri and right fusiform gyrus metabolism (BA 20, 36) (p < 0.001) (Fig. 5A; Supplementary Table 5). FCSRT free delayed recall did not correlate with glucose metabolism in any region.
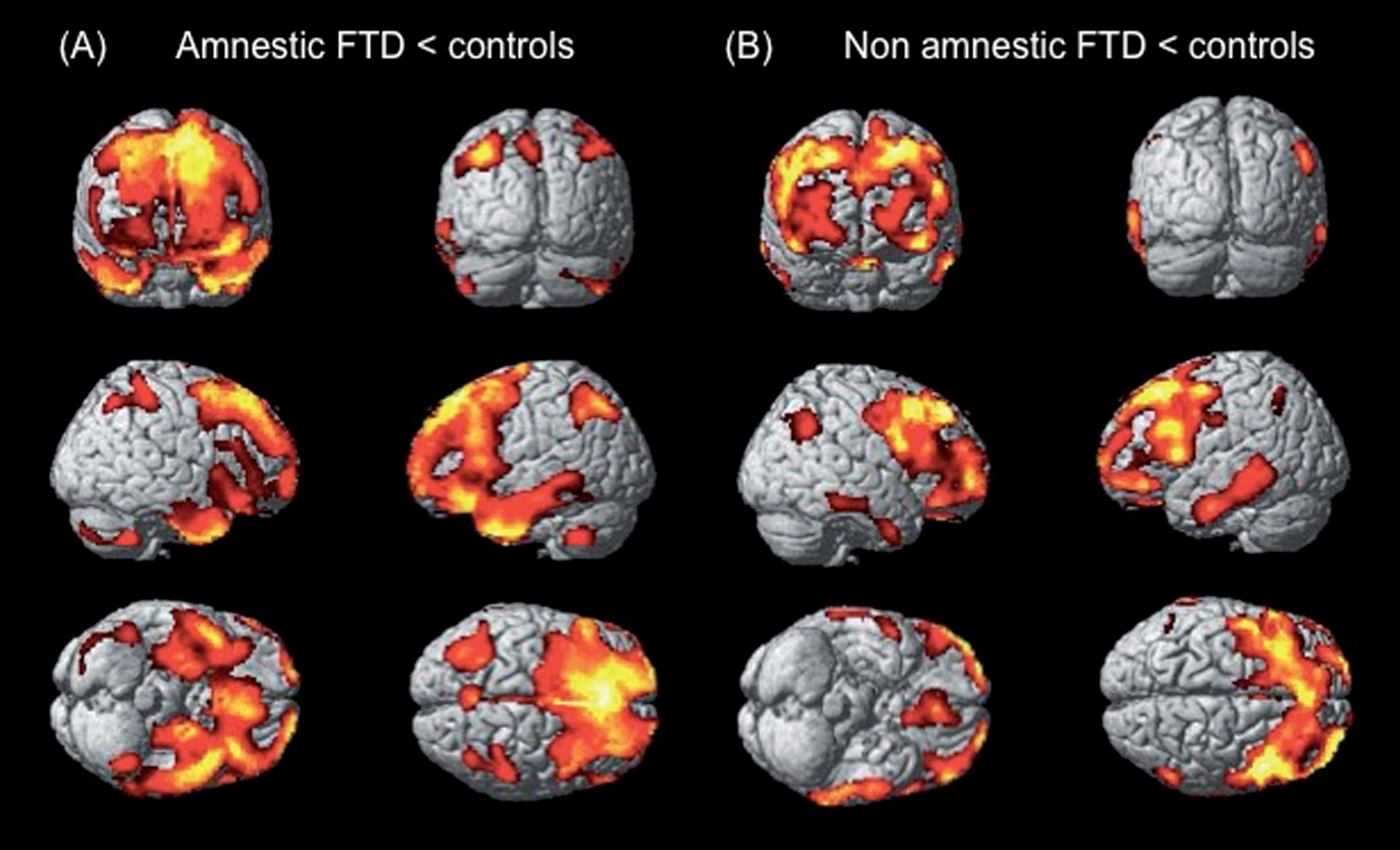
Regions of hypometabolism in amnestic-FTD A) and non-amnestic-FTD B) subjects displayed on MRI template (tridimensional view). Analyses were performed using SPM by comparing the groups of amnestic-FTD (n = 13) versus healthy controls (n = 24) and non-amnestic-FTD (n = 13) versus healthy controls (n = 24). A two-sample t test with an uncorrected p value <0.001 and an extent threshold of 50 voxels was used. See Supplementary Table 2 for detailed description of anatomical locations. FTD, frontotemporal dementia; SPM, Statistical Parametric Mapping.
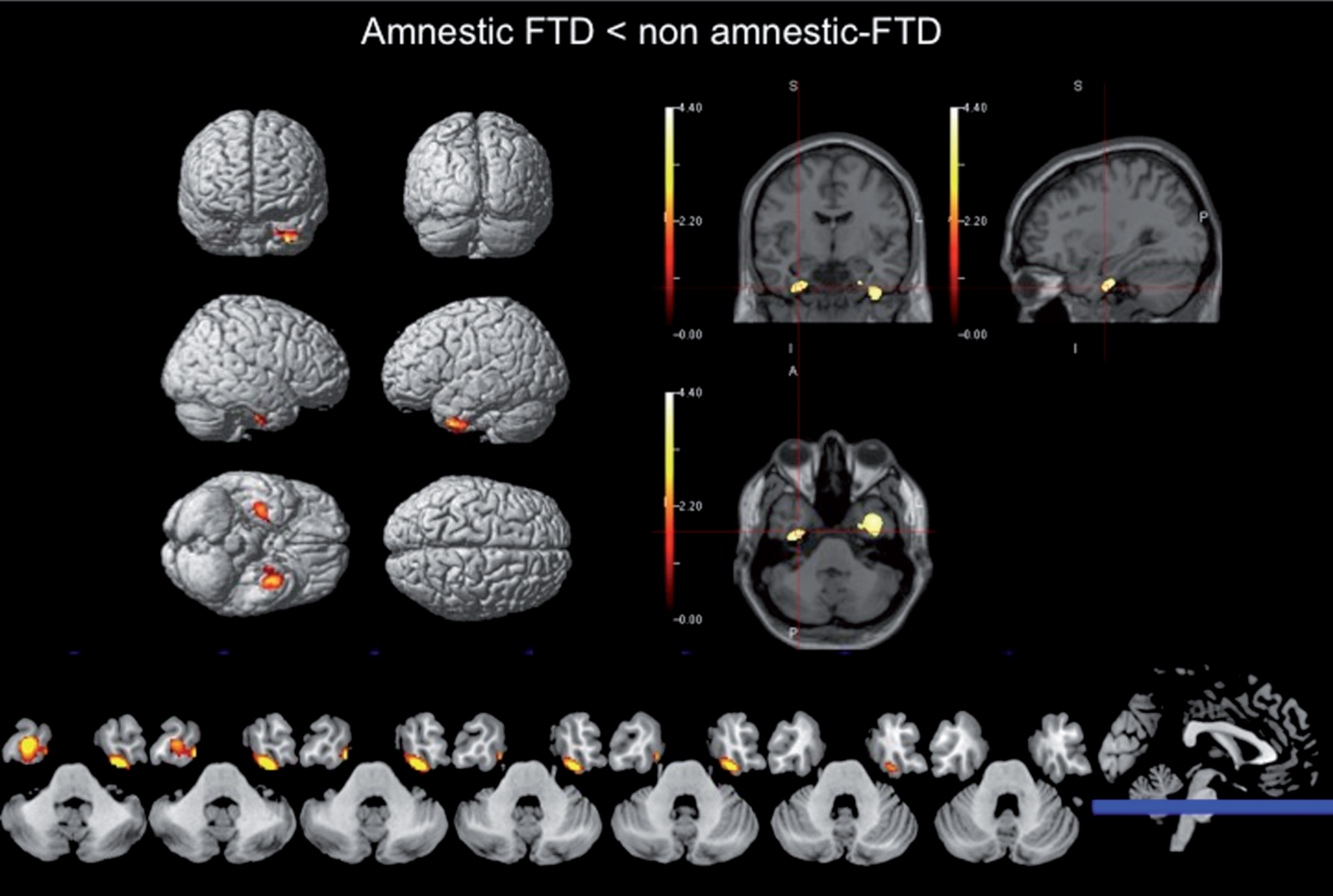
Differences in regional metabolism between amnestic and non-amnestic-FTD patients. Regions of hypometabolism in amnestic-FTD subjects are displayed on MRI template (tridimensional view plus representative axial slices; neurological orientation). Analysis was performed using SPM by comparing the groups of amnestic-FTD (n = 13) versus non-amnestic-FTD subjects (n = 13). A two-sample t test with an uncorrected p value < 0.001 and an extent threshold of 50 voxels was used. Supplementary Table 3 gives precise locations of all significant clusters. See text for detailed description of anatomical locations. FTD, frontotemporal dementia; SPM, Statistical Parametric Mapping.
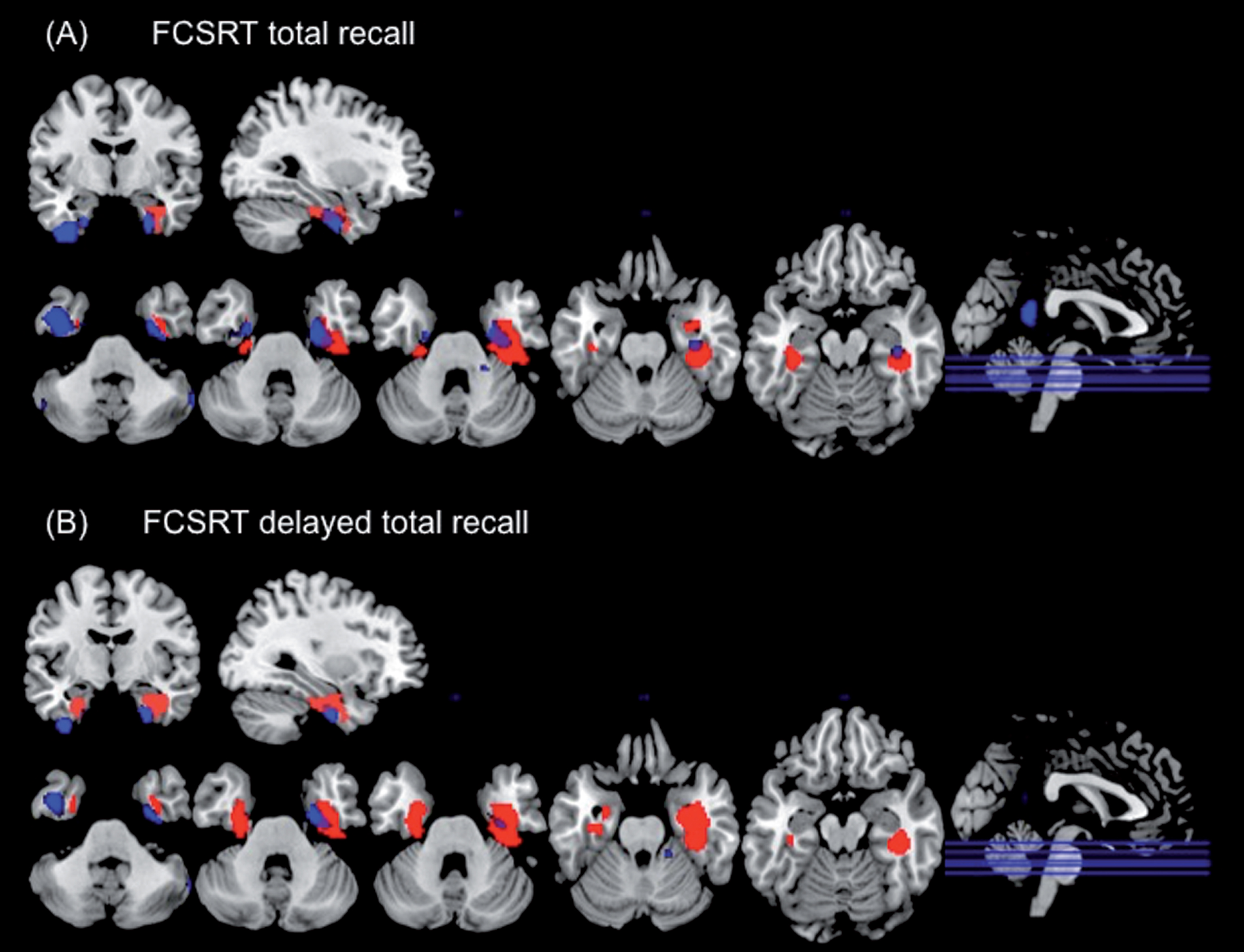
Regions of inversed correlated metabolism with the Free and Cued Selective Reminding Test total A) and delayed total B) recalls in patients with bvFTD (in blue) and AD (in red) (p value <0.001). Significant clusters are displayed on a MRI template (representative coronal, sagittal and axial slices; neurological orientation). bvFTD, behavioral variant frontotemporal dementia.
DISCUSSION
This study assessed episodic memory function in bvFTD patients compared with AD patients and HC, and analyzed the relationship between episodic memory and brain metabolism measured using positron emission tomography imaging with 18F-fluorodeoxyglucose (FDG-PET).
When considering the distribution of the FCSRT scores, we observed two clearly distinct profiles of memory performance in bvFTD patients: half of them (amnestic-FTD) showed a deficit in episodic memory similar to that observed in AD patients, whereas the other half (non-amnestic-FTD) had similar performance to that of control subjects. Recent studies have suggested that bvFTD could be associated with severe anterograde amnesia. Severe amnesia has been observed in up to 15% of pathologically confirmed bvFTD patients, even in the initial stages of the disease [37–39]. More recently, some studies have demonstrated that episodic memory deficits in bvFTD are common and that they may even be as severe as in AD [11–13]. Because phenocopy patients, who display typical behavioral features of bvFTD but do not progress to dementia [40], show preserved episodic memory and cognitive function on neuropsychological testing, it has been suggested that the mixture of phenocopy and bvFTD could have led to an underestimation of memory impairment in previous studies of bvFTD [9, 10].
For the amnestic-FTD subgroup, scores of free, total, free delayed, and total delayed recalls were not significantly different from those in the AD group. Therefore, after administering the FCSRT to bvFTD patients, we found that 50% of bvFTD patients had severe amnesia in which FCSRT total recall as well as total delayed recall performance were similar to that observed in AD, suggesting a real deficit in memory storage (memory consolidation process) [41].
These two different episodic memory profiles in our bvFTD sample cannot be explained by differences on severity of the disease, gender, or aging, because both subgroups were comparable at functional scores, time of illness, ages, or gender. These findings are in contrast with a recent large bvFTD cohort study [42], in which verbal and visual memory impairments were mostly associated with moderate to advanced stages of bvFTD. Similarly, a well-characterized Pick disease cohort study [43] found that episodic memory disturbance was often a late finding. However, a recent longitudinal study found that both bvFTD and AD subjects displayed impaired memory function at baseline, which continued to decline more rapidly in bvFTD group [44]. Differences in memory profiles neither can be explained by distinct severity of executive dysfunction or other cognitive function because amnestic-FTD and non-amnestic-FTD patients did not differ on any executive variables, and we did not find a correlation among FCSRT scores and tests measuring executive tasks. These results showed that prefrontal cortex dysfunction does not account solely for the memory deficits seen in bvFTD. Similarly, a recent study [45] also found that memory deficits in bvFTD cannot be solely explained by executive dysfunction occurring in these patients. Besides, different episodic memory profile in our bvFTD sample can neither be explained by different performance on other cognitive functions, like language, visuospatial, or visuoperceptive abilities, because both subgroups had similar scores on these tests and FCSRT scores were not significantly correlated with such variables.
In comparison with non-amnestic-FTD, amnestic-FTD patients showed significant bilateral lower metabolism in anterior parahippocampal and inferior temporal gyri. Likewise, within the bvFTD group, FCSRT total and delayed total recall performance was inversely correlated with right parahippocampal and bilateral inferior temporal metabolism. Similarly, within AD subjects, FCSRT total and delayed total showed an inverse correlation with right fusiform gyrus and bilateral parahippocampal metabolism. Unlike bvFTD, inferior temporal metabolism was not associated with FCSRT scores in AD patients.
In agreement with our results, previous studies have found a similar degree of episodic memory impairment among bvFTD and AD patients [11, 23]. While some authors reported different neural correlates [11, 12], other studies described common neuroanatomical substrates associated with memory disturbance in both bvFTD and AD [22, 23]. Using atrophy ratings, Pennington et al. [11] found that neural correlates differed (temporal and frontal areas in AD versus frontal in bvFTD), although memory performance was alike between both dementia groups. Similarly, Frisch et al. [12] reported that memory performance was associated with different brain regions in both patient groups: whereas in AD patients test performance was mainly correlated with changes in the parieto-mesial cortex, performance in FTD patients was correlated with changes in frontal cortical as well as subcortical regions. Dermody et al. [22] found that hippocampal atrophy strongly correlated with prospective memory integrity in both patient groups, however, dissociable neural substrates were also identified across dementia syndromes. Likewise, Irish et al. [23] also described regions commonly implicated in episodic retrieval across groups, namely the right temporal pole, right frontal lobe, left paracingulate gyrus, and right anterior hippocampus. Nevertheless, divergent anterior versus posterior neural networks were implicated exclusively in bvFTD and AD, respectively. Several studies have demonstrated a similar degree of hippocampal atrophy in bvFTD to that observed in AD, especially in bvFTD pathology with transactive response DNA binding protein-43 inclusions [18, 19], and has been shown to correlate robustly with episodic memory dysfunction in this group [23]. Using structural magnetic resonance imaging data and postmortem brain evaluations, Hornberger et al. [18] showed that the atrophy in memory-network brain regions was not circumscribed to the hippocampus in bvFTD and that Papez circuitry was affected in its entirety, including subcortical regions such as the fornix and anteriorthalamus.
In contrast to our work, previous imaging studies focused on episodic memory function in bvFTD, using neuropsychological tests such as the Recognition Memory Test [46], the Rey Auditory Verbal Learning Test [47], or the visual and verbal memory subtests from the Wechsler Memory Scale [48]. The FCSRT differs from these tests of episodic memory in that it controls for individual differences in attention and cognitive processing through the implementation of a “controlled learning” study procedure in which the examinee searches for study items in response to a category cue. The controlled learning approach of the FCSRT uniquely maximizes encoding specificity and learning through the promotion of deep semantic processing. In addition, the FCSRT uses a controlled distraction procedure (counting backwards) before each recall trial, thus ensuring that items cannot be recalled from working memory, and that recall relies exclusively on episodic memory. The utility of this cued selective reminding paradigm in the detection of AD-related memory dysfunction has been widely reported [24, 49–53]. A poor performance on the FCSRT has also shown a high correlation with atrophy in the medial temporal lobe [41, 54–56], neurofibrillary lesions in parahippocampal regions that are the earliest targets of AD pathology [57], and was significantly associated with cerebrospinal fluid biomarkers of AD, thereby supporting the accuracy potential of this paradigm in the early detection of AD [58, 59]. Therefore, the FCSRT is a very accurate tool to measure verbal episodic memory, being an excellent marker of medial temporal lobe integrity not only in AD but also in bvFTD, as shown by our results.
There are some limitations of our study. On one hand, autopsy data were not available. Nevertheless, our diagnostic classification was based on international clinical criteria with FDG-PET support, which have demonstrated a good correlation with pathological findings [60–62] and increases confidence of clinical diagnosis [34]. However, we cannot completely exclude the possibility that some of the bvFTD cases, in particular those who performed very poorly on the memory tasks, may have underlying AD pathology. Likewise, the possibility of having included patients with frontal presentations of AD (behavioural-dysexecutive variant of AD) as bvFTD subjects cannot be ruled out [63]. Further studies with neuropathological confirmation, or at least in vivo amyloid-PET imaging data, represent an important area of future enquiry. On the other hand, our neuroimaging results did not survive conservative corrections for multiple comparisons (i.e., Family-Wise Error) and were therefore reported uncorrected at p < 0.001. Given our sample size, and the application of a cluster extent threshold of 50 contiguous voxels, we are confident that our results do not represent false positive findings, however, it will be important to replicate these findings in a larger patient cohort using corrected neuroimaging results.
Our results reinforce that bvFTD patients could present a true amnesia affecting storage and consolidation abilities, which seems to be independent from executive and other cognitive functions. Besides, the findings of the present study support that episodic memory disturbances in bvFTD and AD share common neural substrates, involving both parahippocampal regions. In addition to these Papez circuit areas, inferior temporal lobe regions were also related with episodic memory deficits in bvFTD.
In conclusion, our findings suggest that bvFTD could have an amnestic presentation due to a true consolidation deficit, with involvement of structures implicated in the Papez circuit, as occur in AD, and also inferior temporal lobe regions. These results contribute to understand the mechanisms underpinning memory impairment in bvFTD, which may be relevant to further revisions of the current diagnostic consensus criteria.