
Abstract
INTRODUCTION
Impairments in the ability to recognize facial affective expressions may lead to social dysfunction and difficulties with interpersonal communication for people with Alzheimer’s disease (AD). Such social and communicative impairments have been found to be unrelated to cognitive status [1]. The ability to identify facial emotions is critical for nonverbal communication [2]. This ability enables individuals to adapt to an environment and participate in social activities which is integral for a healthy life and leads to social interactions, social ties, and meaningful relationships [3]. The emotional abilities of people with AD merit increased attention [4] as preserved emotion recognition capacity is essential for their social health [5]. Facial emotion recognition is an essential part of social interaction; the face is the most visible aspect of non-verbal behavior and the central focus of attention during communication [6]. Deficits in emotion perception predict quality of life independently of variance predicted by mood and cognitive function, demonstrating the importance of emotion recognition for the well-being of older adults [7].
Emotion recognition in normal aging and in Alzheimer’s disease
There is a degree of facial emotion recognition capacity loss associated with normal aging. A deficit in the perception of negative emotions, specifically of anger, sadness, and fear, has been found in healthy older adults compared to younger adults, particularly related to the recognition of low intensity expressions [8–12]. These deficits are associated with the deterioration of the frontal and temporal lobes, including the amygdala [10, 13]. However, this deterioration is not necessarily related to impairments of emotional regulation, in fact healthy older people have been shown to exhibit better emotional regulation than younger adults; probably because of accumulated life experience and plasticity of medial prefrontal systems [14]. The role of arousal elicited by positive and negative emotional stimuli can also influence emotional regulation. It has been shown that healthy older adults tend to downregulate the positive affect associated with optimal outcomes and upregulate the positive affect associated with non-optimal outcomes [15]. Neurodegenerative diseases involving temporal lobe atrophy or damage have the propensity to elicit deficits in the recognition of emotions. Research has tended to investigate emotion recognition deficits in conditions such as frontotemporal dementia [16, 17] and related conditions, like semantic dementia [18] and primary progressive aphasia [19], probably because of their neuropathology which affects the specific neural substrates involved in emotion recognition and regulation. Not surprisingly, these studies found that these patients have impairments in emotion recognition [17].
Neuroanatomical changes in AD, specifically changes in anterior medial frontal cortex, medial temporal cortex, and the amygdala, have been related to social and cognitive difficulties in people with AD [20]. Such damage may underlie impairments in facial emotion recognition in AD, which increases with the progression of the condition [21–24]. Previous work yielded inconsistent results concerning the ability of people with AD to recognize facial expressions of emotions, which might be related to the profile of participants who were in different stages of the illness.
Several studies found deficits in emotion recognition in people with AD compared with healthy older adults [2, 25–37]. However, a smaller group of studies found no deficits [38–42], potential reasons for these inconsistencies are the use of different interfaces, diversity of stimuli, the level of cognitive effort demanded by the tasks, and the influence of confounding factors such as deficits in spatial and verbal processing [35]. The only literature review on this subject concluded that people with AD showed poorer recognition of facial expressions, showing particular difficulty recognizing sadness [43].
Some studies have considered the influence of the intensity of the expression on individuals’ capacity to recognize the emotion portrayed. Findings suggest that people with AD have more difficulty recognizing low intensity emotional facial expressions than high intensity [2, 45]. The cognitive abilities associated with emotion recognition in people with AD have also been investigated, suggesting that capacity to recognize facial expressions of emotions is mediated by top-down executive functions. People with AD have shown a higher cost when identifying emotions while executing a visual secondary task [46, 47]. Other studies suggested that emotion recognition capacity is mediated by cognitive status [21, 44]. However, people with AD can react to facial emotions even in severe stages of the disease [48].
The study of universal basic emotions
Although facial expressions are capable of portraying a wide range of different emotions and intensities, previous research has found six basic emotions that are universally identified: happiness, surprise, disgust, fear, sadness, and anger [49]. The pioneers in this field of research, Ekman and Friesen, developed a procedure for measuring visibly different facial movements: “The Facial Action Code” [50]. Based on this system, they designed a classic emotion recognition assessment test which required participants to choose which of the six emotion labels best described the facial expression (including the identification of a neutral expression). This test was the first of its kind and has since been widely used for assessments in this area of research [51, 52]. Similar tests have subsequently been developed including: the Penn emotion recognition test [53]; the Izard photographs [54]; and the Florida affect battery [55]. However, none of these instruments has been validated for older adults.
Emotion recognition as a capacity that can be rehabilitated
Despite growing evidence about the influence of emotional processing impairments for people with dementia and their social networks, treatment for AD has largely been concerned with cognitive and functional symptoms. Little has been done to address emotional recognition abilities of those with dementia and the potential for treatments in this area. Even though training of emotion recognition has been carried out with other clinical populations [56], to the best of our knowledge, the possibility to rehabilitate and enhance the emotion recognition ability in people with dementia of any type has yet to be investigated.
The objective of this research was to study if emotion recognition in people with AD could be learned and improved through a specific emotion recognition rehabilitation program. Our hypothesis was that people with AD who received rehabilitation of emotion recognition would improve their emotion recognition skills compared to people with AD whom received only cognitive stimulation or treatment as usual.
MATERIALS AND METHODS
Study design
The study was conducted at the Memory Clinic at Burgos University Hospital, following protocol approval by the local ethical committee. This was a single-blind, controlled trial comparing an experimental group (EG) that received 20 sessions of rehabilitation of emotion recognition (RER) and 20 sessions of cognitive stimulation therapy (CST), with an active control group (CG) that received 40 sessions of CST and a treatment as usual group (TAU). All participants understood and consented to participation in the trial, which lasted 6 months. The clinical trial registration number was CEIC 1381.
Participants
Potential participants were screened for eligibility by a neurologist and a clinical psychologist at the Department of Neurology of Burgos University Hospital. Participants all met DSM-IV criteria for dementia using the diagnostic algorithm and had AD [57]. They all had mild dementia (overall score = 1) on the Clinical Dementia Rating Scale [58], and ranked 3 on the Global Deterioration Scale [59]. They could communicate, hear and see well enough to participate in the study, had no major physical illness or disability, diagnosed psychiatric conditions, or intellectual disability. They all were living in the community at their homes, and had to be accompanied to the initial and last interviews by a caregiver.
Outcome measures
Participants were interviewed at baseline and within one week after finishing the treatment at which they completed all of the measures presented below. A follow up assessment of emotion recognition was carried out after one month. Researchers collected the proxy ratings of activities of daily living and qualitative changes observed during and after the treatment in structured interviews conducted with caregivers at the same time. Qualitative observations of the six autobiographical memories recall sessions, the stories recalled, the roles played by the participants, and their opinions about their participation were recorded in a diary by the session coordinator.
Emotion recognition was evaluated with Affect-GRADIOR, a touchscreen test designed by the INTRAS Foundation (García-Casal et al., unpublished data). It is an emotion recognition test validated for older adults and people with MCI and AD, with excellent internal consistency (ordinal Cronbach’s α= 0.96) and test-retest reliability (r = 0.840, p < 0.001). The test requires participants to identify the correct emotion from six basic emotions (happiness, surprise, disgust, fear, sadness and anger) and a neutral expression consisting of 91 stimuli, 13 per emotion (Fig. 1). The expressions are displayed by 13 different individuals (6 male and 7 female). The photographs are randomly presented on a 13.3 inches screen. After 33 seconds (maximum display time), if the participant does not provide an answer, the test automatically moves to the next stimuli, computing an error of omission. The assessment takes between 10 and 20 minutes depending on participants’ ability and cognitive status. The facial stimuli used in the Affect-GRADIOR program were different to the facial stimuli used in the rehabilitation phase. The test provides the following information: 1) total scores (xx/91) and partial scores per emotion (xx/13); 2) errors of commission (the participant chose the wrong answer), and errors of omission (the participant did not provide any answer); 3) total emotion processing speed and processing speed per emotion, calculated with the formula ([correct answers-(omission + commission errors)]/(reaction time/1000)), with a correction for negative values: ([correct answers-(omission + commission errors)]*(reaction time/1000)); 4) total precision of processing calculated with the formula (([correct answers-commission errors]/91)*100); and 5) learning curve (correct answers in the last 20 items – correct answers in the first 20 items).
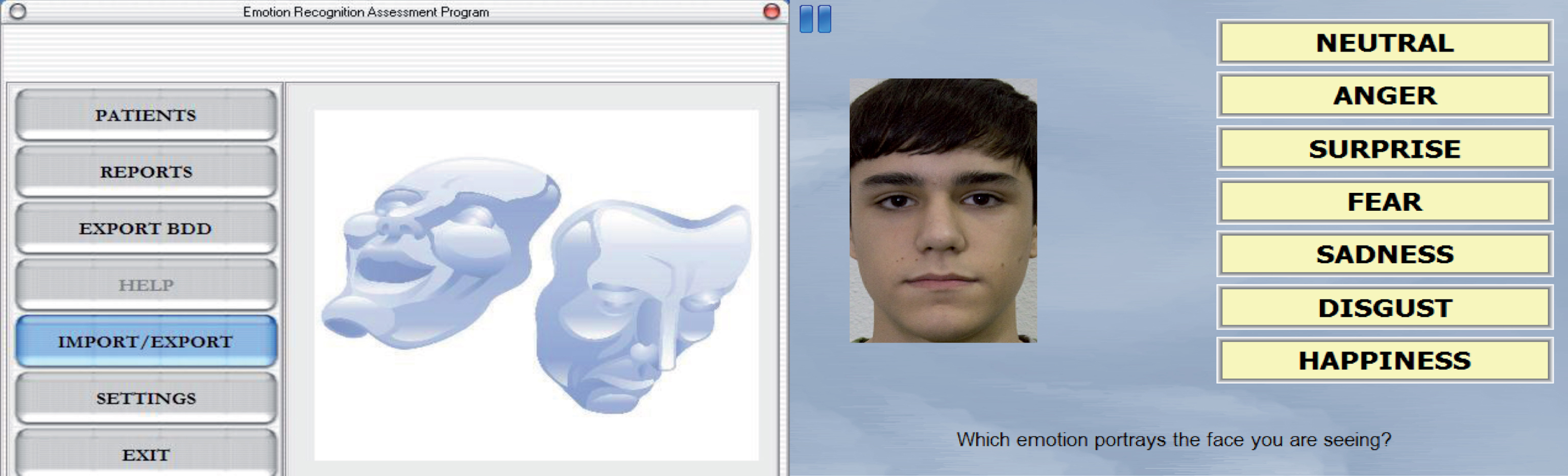
Affect-GRADIOR emotion recognition test.
General cognitive capacity was assessed with the Mini-mental State Examination (MMSE), a brief but widely used generic test of cognitive function, with higher scores indicating better cognition [60]. The Spanish version has good reliability and validity [61]. Depression was assessed with the short version of the Geriatric Depression Scale (GDS). A brief test for depression screening that consists of 15 items and the score ranges from 0 to 15. The cut off point for depression is 5, with higher scores indicating severer depression [62, 63].
Procedure
Thirty-six participants were consecutively allocated as they received a diagnosis to the experimental group (n = 12), the active control group (n = 12), and the TAU group (n = 12). Random allocation was not possible due to ethical issues regarding waiting lists for treatment provision, thus consecutive allocation was employed. Participants completed 20 weeks of treatment. Rehabilitation sessions were conducted by a clinical psychologist trained in “Training of Affect Recognition” program [64] and CST [65] and based on a treatment manual. Sessions lasted 90 minutes and were held twice a week in small groups of 5 to 6 people. Participants were blind to the allocation and to the objectives of the research; the informed consent stated that they accepted to participate in a research project about the efficacy of cognitive stimulation.
The rehabilitation of emotion recognition (RER) intervention used in this study is based on the “Training of Affect Recognition” (TAR) program developed by Wölwer & Frommann from Düsseldorf University. TAR is a computer-based treatment with a touchscreen interface [64, 66]. The program was originally developed for people with schizophrenia and comprises 12 sessions divided in three modules. During the first module participants learn to identify and discriminate the prototypical facial signs of the six basic emotions (happiness, surprise, disgust, fear, sadness, and anger) and the neutral expression. The second module aims at a more holistic processing mode with fast decisions, relying on first impression, nonverbal processing, and recognition of facial expressions with small intensities. The third module deals with the role of facial emotions in social, behavioral, and situational contexts [66]. In this study, TAR was modified adapting the tasks to the aesthetics and interests of older people. Two revision sessions and a fourth module of six sessions concerning the generation of autobiographical memories were added. This modification was made based on previous findings regarding the benefits of reminiscence for people with AD [67] and the evidence that autobiographical memory for emotional events is better preserved in AD [68]. The fourth module required participants to generate autobiographical memories related to the six basic emotions: surprise, disgust, fear, sadness, anger and happiness. One emotion was considered per session. Once each participant had recalled an autobiographical memory related to an emotion (with the help of group techniques), the stories were enacted through role-play. Each session ended with a review of the stories told and the roles each participant played.
The computer based exercises were projected on a widescreen with an 800×600 resolution with an Epson VS240 SVGA 3LCD projector. The sessions were delivered in a group setting and participants had the opportunity to discuss the right option before introducing the answer in their individual touchscreens. Each exercise was led by a participant in consecutive order, and the facilitator guided the group to the right answer through appropriate questions when necessary. The modifications were piloted with five people with AD in two sessions. In the first session, they received the modified TAR, and, in the second session, they completed the autobiographical memory recall task. Feedback from the pilot sessions from participants and facilitators were: 1) to project the computer based exercises onto a larger screen; 2) to do the revision exercises at the end of the sessions (and not at home); 3) and to discuss each exercise in a group before providing the individual answer. The findings from the pilot sessions were included in the treatment manual.
The CST intervention received by the experimental group and the active control group was based on the principles of cognitive stimulation developed by Spector et al., including mental stimulation, seeking new ideas, thoughts and associations, and using hints and implicit learning [65, 69]. The treatment was manualized [70], and each session was divided in three modules: 1) Welcome and reality orientation (15 min); 2) Cognitive Stimulation group dynamics and exercises working on memory, praxis, gnosis, language, attention, executive functions, and calculation (60 min); 3) and closing and group review of the aspects worked during the session (15 min).
Participants from the EG received CST and RER sessions on alternate days (one RER and one CST session per week). Participants from the CG received 40 sessions of CST (two per week). The contents of the 20 CST sessions received by the EG was the same as the first 20 CST sessions of the CG. The subsequent 20 CST sessions received by the EG was based on similar material to that covered in the first 20 sessions. Participants of the TAU group received pharmacological treatment for dementia (Table 1) and did not receive any psychosocial intervention during the study. Participants from the EG and the CG also received TAU. The decision to have an experimental group that received a combined treatment and to include an active control group that received only CST was based on three reasons. Firstly, as it was the first time that this type of treatment was offered to people with dementia, we could not grant its efficacy. As a consequence, the Ethics Committee of the hospital proposed that we should offer a combined treatment. Secondly, improvement of the ability to recognize emotions could be a consequence of increased social interaction; social contact could work as a natural training in emotion recognition. Including an active control group in which the participants experienced social interaction (i.e., CST) without emotion recognition rehabilitation enabled investigation as to whether improvement in emotion recognition was due to the RER treatment rather than social interaction. Thirdly, since emotion recognition capacity is based on top-down cognitive processes, improvement of this ability could be a consequence of cognitive stimulation. Thus, having a cognitive stimulation group as a control enabled the consideration as to whether improvement in emotion recognition is associated with cognitive stimulation.
Means, frequencies and p-values of the sociodemographic variables of the participants
Note: ACH, anticholinesterases; AD, Alzheimer’s disease; ADEP, antidepressants; BENZ, benzodiazepines; CDR, Clinical Dementia Rating; CST, Cognitive Stimulation Therapy; GDS, Global Deterioration Scale; GDS-Y, Geriatric Depression Scale (Yesavage); M, mean; MEM, memantine; n, number of participants; PRE – POST, time between pre and post assessments in days; RER, rehabilitatoin of emotion recognition; RF, pharmacological treatment for Risk Factors (diabetes, hypertension, cholesterol); SD, standard deviation; TAU, treatment as usual.
Data analysis
Variables were plotted and checked for normality of distribution using Shapiro-Wilk tests. Baseline characteristics of the three groups were compared using independent t tests and X2 tests as appropriate. Data was analyzed with parametric and nonparametric statistics depending on the distribution of the variables. All p values were 2 tailed with a significance level of 0.05. When primary analysis reached statistical differences, post hoc analysis where carried out with Dunnett’s T3 test corrected for multiple comparisons. Effect sizes and their respective standard errors (SE) and confidence intervals were estimated as Standardized Mean Change Index (d MR ) for within-group comparisons, and as Standardized Mean Index difference (d C ) for between-group comparisons, and corrected for small sample sizes [71]:
By convention, an effect size of 0.2, 0.5, and 0.8 was considered small, moderate, and large, respectively [71]. The statistic software IBM® SPSS® (Version 19.0) was used to run the analysis. To facilitate the intuitive comprehension of the direction of the changes, a positive value was assigned to the effect sizes that implied an improvement, and a negative value to those that implied deterioration.
RESULTS
The three groups were equivalent at baseline in all the sociodemographic variables of interest (Table 1). Of the 36 participants, there were four dropouts: one in each group because they decided to leave the treatment and a second one in the CG because the patient suffered a cerebrovascular accident. There were two dropouts at the follow up in the EG group because the participants were on summer holidays. The mean number of sessions attended by participants in the EG was 32.91 (SD = 5.26) and by participants in the CG was 37.00 (SD = 5.76). The difference in the mean number of sessions attended between groups was not statistically significant (p = 0.104). There was no significant difference between the three groups in terms of the time elapsed between pre- and post-assessments (p = 0.697, Table 1).
All groups showed the same pattern in the emotions that were better recognized at both baseline and post assessments: happiness, surprise, neutral, sadness, disgust, anger, and fear, in that order (Fig. 2).

Correct answers per emotion before and after the intervention.
Correlations of emotion recognition with MMSE and depression
Correlations in pre-test scores showed a significant correlation between cognitive status measured with MMSE and happiness speed of processing (r = 0.408, p = 0.002). No significant correlations were found between MMSE or depression measured by GDS and the other dependent variables. Thus, MMSE or GDS were not entered as covariates in the statistical analysis.
Within group analysis
The effect of each variable was analyzed in the three groups using independent t tests or Wilcoxon tests, depending on their distribution. After treatment, the group that received rehabilitation of emotion recognition (EG) improved in general emotion recognition (p = 0.005) from 39.73 (±8.04) to 48.18 (±7.83) correct answers, and had less total errors of commission (p = 0.003) (Table 2). When emotions where analyzed separately, the participants significantly improved their recognition of surprise (p = 0.013), disgust (p = 0.018), and neutral expression (p = 0.014). The experimental group also showed an improvement in their precision of processing (p = 0.004) and their processing speed (p = 0.004). The processing speed for the different emotions improved for disgust (p = 0.041) and neutral expression (p = 0.016).
Effect sizes for significant results were large for the total correct answers, the errors of commission, the precision of processing, the processing speed, the recognition of disgust and neutral expression, and the processing speed for neutral expression. A moderate effect size was found for the processing speed of disgust. Effect sizes were also calculated for non-significant results; as this study has a small sample size, the reported effect sizes may be indicative for future investigations and confirmatory studies. For non-significant results, effect sizes were moderate for the recognition of anger and the processing speed for happiness and anger. Finally, small effect sizes were found for the recognition of sadness and surprise. A small negative effect size was found for the minimum reaction time.
Within group changes in facial emotion recognition after treatment
Note: *p < 0.05; asmall effect size; bmoderate effect size; clarge effect size; CST, cognitive stimulation therapy; d MR , standardized mean change index; M, mean; n sample size; RER, rehabilitation of emotion recognition; S DMR , standard error; S.D., standard deviation; TAU, treatment as usual.
The group that received only cognitive stimulation therapy (CG) did not experience any significant differences in their scores after treatment (p > 0.05). The effect sizes showed a positive moderate effect over the maximum reaction time and the processing speed for neutral expression and a positive small effect for the mean reaction time, the recognition of disgust and neutral expressions and the processing speed for happiness and disgust. A negative moderate effect was found over the recognition of happiness and a small negative effect over the mean reaction time and the processing speed for sadness and fear.
The TAU group experienced a deterioration in their capacity to identify sadness (p = 0.02) and the processing speed for sadness (p = 0.033). The effect sizes showed a positive moderate effect over the minimum reaction time, the learning curve, and the recognition of anger; and a positive small effect over the errors of omission, the recognition of surprise, and the processing speed of surprise. A negative large effect was observed over the processing speed for sadness and a negative moderate effect over its recognition. Finally, a small negative effect was found over the errors of commission, the processing speed, the recognition of fear and the processing speed for fear.
Between group analysis
The treatment effect was defined in this study as the change in post-test score from the pre-test score. The effect of each of the variables was analyzed in the three groups using the Kruskal-Wallis test. The three groups were equivalent at baseline in all the variables (p > 0.05) (Table 3). Thus, all the significant differences found after the interventions were interpreted as treatment effects. A positive between-group treatment effect was found after testing for total correct answers (χ2 (2) = 6.937, p = 0.031), errors of commission (χ2 (2) = 8.904, p = 0.012), precision of processing (χ2 (2) = 6.655, p = 0.036), processing speed (χ2 (2) = 8.400, p = 0.015), learning curve (χ2 (2) = 6.736, p = 0.034), correct answers for sadness (χ2 (2) = 8.297, p = 0.016), correct answers for disgust (χ2 (2) = 9.542, p = 0.008), and processing speed for disgust (χ2 (2) = 10.728, p = 0.005). Post hoc tests of mean comparisons were performed with paired Dunett’s T3 tests adjusted for multiple comparisons, showing significant differences between EG and TAU in total correct answers (p = 0.021), errors of commission (p = 0.002), precision of processing (p = 0.021), processing speed (p = 0.001), correct answers for sadness (p = 0.016), correct answers for disgust (p = 0.005), and processing speed for disgust (p = 0.002). No significant differences between EG and CG and between CG and TAU were found.
Effect size analysis found small to large effect sizes in measures of emotion recognition comparing the EG to the CG and to TAU except for reaction times that got slower in the EG (Table 3).
Between group changes in facial emotion recognition after treatment
Note: *p < 0.05; asmall effect size; bmoderate effect size; clarge effect size; d c = standardized mean index difference; CG, control group; EG, experimental group; M, mean; n, sample size; RER, rehabilitation of emotion recognition; S dc , standard error; S.D., standard deviation; TAU, treatment as usual.
Autobiographical memories recall
The participants of the EG could evoke personal stories linked to each of the six basic emotions with great accuracy and pleasure, contributing to strengthen affective bonds between them. All the participants stated that they enjoyed the six autobiographical memories sessions as they could share personal stories that they would not share in a different context.
Follow up
A follow up assessment of the emotion recognition capacity was performed one month after the post treatment assessment. Of the 11 participants in the EG, only 9 could be assessed. The results of the within group comparison (Table 4) showed no significant differences with post measures, with the exception of processing speed for surprise, which improved (p = 0.015).
Within group changes in facial emotion recognition at 1 month follow up
Note: n, sample size; *p < 0.05.
DISCUSSION
This study investigated if emotion recognition ability could be rehabilitated in people with AD. The main findings were 1) that the capacity to recognize facial expressions of emotions can be improved through specific rehabilitation in people with AD; 2) that the emotions more sensitive to the treatment were disgust, surprise, and neutral expression; 3) and that gains were still present at a one month follow up. These findings present a new opportunity concerning rehabilitation for people living with Alzheimer’s disease and have implications for improving quality of life.
The group that received RER improved in their overall emotion recognition capacity while the control group that received CST remained stable and the TAU group experienced deterioration. The experimental group improved in their capacity to recognize disgust, surprise, and neutral expressions. The capacity to recognize the neutral expression is of particular interest, as it is more likely to be misinterpreted according to the affective state of the perceiver [72], leading to misunderstandings in interpersonal communication. The neutral expression and surprise are the most ambiguous facial emotions; this may explain why rehabilitation was more effective with these two emotions. As an emotional expression, disgust is easily characterized (a frown and wrinkled nose), which might also explain why it was easy to recognize once participants were familiar with the characterization. The rehabilitation effects were maintained over the one month post-intervention follow up period with the exception of the processing speed for surprise, which improved.
In concordance with previous studies [9, 28], participants had more difficulties in recognizing negative emotions than happiness and surprise. Our results contradict those reporting a deterioration in capacity to recognize happiness in people with AD [27]. However, findings reporting that people with AD have more difficulty recognizing negative emotions than positive emotions may be an artifact of only having one positive emotion from which to choose [73]. Studies with a wider range of positive emotions (e.g., love, interest, inspiration, gratitude, serenity) are recommended.
The improvement in processing speed for emotions in the EG compared to the CG and the TAU group suggests that there is a specific cognitive ability linked to the processing of emotions that is relatively independent from general cognitive functioning. Previous literature suggests that emotion recognition capacity is mediated by cognitive deficits [21, 26]. However, our results suggest that emotion recognition capacity must be specifically rehabilitated, since it did not improve with cognitive stimulation but did improve with specific facial emotion recognition rehabilitation. Furthermore, no correlations were found between cognitive status and emotion recognition capacity at baseline. The negative effect sizes of the EG in comparison to the CG and the TAU group, in relation to reaction time measures after treatment, might be explained as a consequence of more detailed processing of the stimuli, in which the participants analyzed the facial action units [50] to arrive to a conclusion, thus taking them more time to give an answer. Miller et al. found that emotion recognition deficits in AD patients were not associated with significant changes in behavior. This is contrary to findings in people with frontotemporal dementia where deficits in emotion processing are more likely to coincide with behavioral changes. People with AD might be equipped to use other emotional cues (like prosody, body posture, gestures, and verbal explanations) or cognitive skills to guide their perception of emotions. It would be interesting to investigate if the improvement in the emotion recognition capacity is associated with improvements in social interaction in people with AD, and if people with other forms of dementia can also benefit from rehabilitation in emotion recognition.
It is well established that emotion influences memory performance, for example people with AD have better recall of sad and happy stories than of neutral stories [74]. There is a link between emotion and the way that memories are encoded and recalled [75], as emotional memories may be more easily accessible or more vivid. This influence appears to be preserved in people with AD; for example, the retention of the emotional phase of the story differs significantly from that of the neutral phases [76]. Further evidence supports a beneficial effect of emotion in memory, as the emotional material is more accurately recalled than the neutral material [68]. Orbital and ventromedial prefrontal cortex is particularly involved in retrieving autobiographical episodic memories, with an emphasis on emotional episodes and memory for context [77] and in emotion recognition [78]. Participants in the EG found the recall of autobiographical memories associated to the six basic emotions stimulating and entertaining. Future research should assess the relationship between the improvement of emotion recognition and ability to recall and encode autobiographical memory.
The present study has some limitations. Randomization was not possible, in order to compensate for this, the groups were matched in the variables sex, age, education, urban or rural residence, and civil status. The study was performed with a small number of participants, although corrections for small sample sizes were employed in the statistical analysis to address this issue. Even though the different components of the RER treatment were adapted for people with AD, and two pilot sessions were carried out to receive suggestions from the participants in the design of the treatment, the complete RER intervention had not been validated for people with dementia. In order to address this limitation, each RER session was assessed at the end, and the suggestions of the participants and the professionals were included in the RER manual. This study analyzed multiple outcomes and could have been corrected for multiple comparisons. However, as the study is exploratory and the hypothesis is clearly defined, the correction for multiple comparisons is not recommended because it implies inflating type 2 error [79]. As a consequence, the results should be seen as hypothesis generating, not as definitive findings, meaning more confirmatory research is recommended.
Conclusions
The results of this study suggest that there is capacity to improve the recognition of facial expressions of emotions through specific rehabilitation in people with AD. The emotions that are more sensitive to the treatment are disgust, surprise, and the neutral expression. These findings have implications for the design of better interventions for people with Alzheimer's disease that may lead to improved quality of life and social interactions of this population. Further research is needed to confirm these results, including randomized controlled trials, studies regarding the retention of the effects, and identification of the potential neural mechanisms involved.
Footnotes
ACKNOWLEDGMENTS
We would like to thank all participants and caregivers for their participation in the study and the following persons for their kind contributions: Visitación de las Heras, nurse in the department of neurology, for her help in the recruitment and care for study patients; and Teresa Cid Bartolomé, engineer in INTRAS Foundation, for her advice on technical aspects of Affect-GRADIOR program.