
Abstract
Keywords
INTRODUCTION
Dementia with Lewy bodies (DLB) is often overlooked and misdiagnosed as Alzheimer’s disease (AD) due to overlap in clinical presentation [1, 2]. Both DLB and AD are preceded by a prodromal period, generally denoted Mild Cognitive Impairment (MCI). It is acknowledged that pathology-specific treatments will need to target disease during the prodromal period or earlier. Therefore, it is important to identify patients during this phase. There is an extensive literature on the prodromal phase of AD, but a limited literature on prodromal DLB.
Patients with fully manifest DLB have a characteristic neuropsychological and neuropsychiatric profile which is distinct from patients with AD [3–6]. There is emerging evidence that even at the stage of MCI, DLB, and AD patients have different neuropsychological profiles. In a few early studies, patients with prodromal DLB more frequently exhibited fronto-executive, visuospatial, and attentional deficits compared to those with prodromal AD [7, 28]. Prodromal AD patients more frequently had a prominent episodic memory deficit, which was present in only a minority of prodromal DLB patients [7].
Fluctuations in cognition, spontaneous parkinsonism, and REM sleep behavior disorder (RBD) were more frequently observed in prodromal DLB compared to prodromal AD in some studies [7, 28]. However, the literature is less consistent regarding the core feature of visual hallucinations [7].
The aim of the present study was to replicate the early findings in a large sample of patients from a non-academic setting. We therefore aimed to determine whether there are differences in the neuropsychological profile and clinical features of patients with prodromal DLB compared to prodromal AD and stable-MCI in an unselected sample of MCI cases.
MATERIALS AND METHODS
Study design
The present study was a retrospective, longitudinal, observational study that used an unselected sample to test the hypothesis that patients with prodromal DLB have a different cognitive and neuropsychiatric profile compared to patients with prodromal AD and stable-MCI.
Setting
The data used for the present study came from a Memory Clinic database. The Memory Clinic is part of the Old Age Psychiatry Service in Essex, UK and provides specialized multidisciplinary assessments with emphasis on screening, early diagnosis, and follow-up of patients at high risk of developing dementia. The clinic is part of the National Health Service, based in a general hospital and covers inner city, suburban, and rural areas with variable socioeconomic status. There is limited private provision of psychiatric diagnostic services in the UK and therefore the clinic benefits from near-complete coverage of the local population.
Participants
A total of 1,848 new patients were seen at the Memory Clinic between 1994 and 2015. Of these, 560 patients (30.3%) had an initial diagnosis of MCI and were therefore considered for the present study (see Fig. 1). Inclusion criteria were patients who had a diagnosis of MCI at initial assessment with a minimum of 12 months of follow-up.
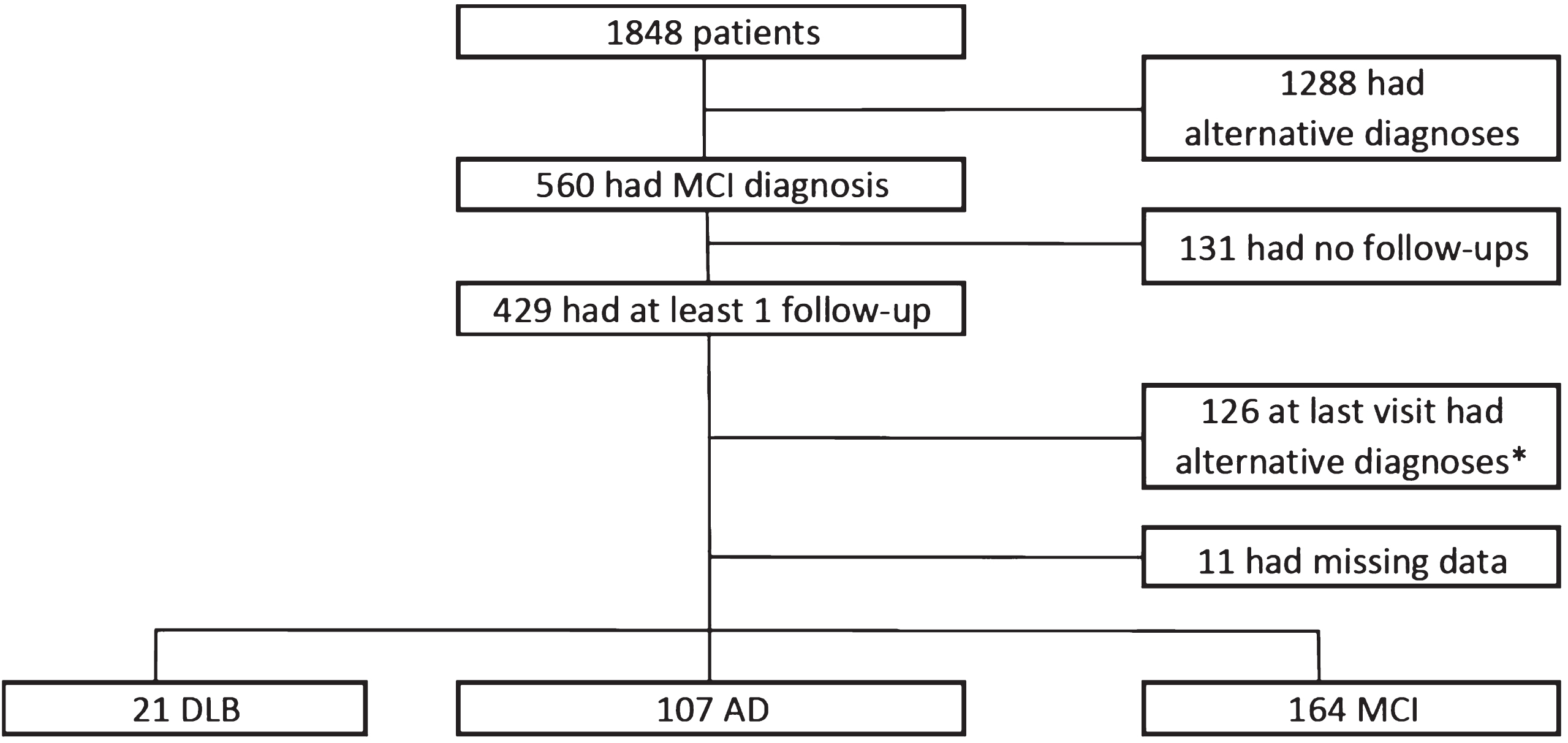
Flowchart showing diagnoses at baseline and follow-up. DLB, dementia with Lewy bodies; AD, Alzheimer’s disease; MCI, Mild Cognitive Impairment. *126 patients had alternative diagnosis at last follow-up: Subjective Cognitive Impairment = 50; Vascular Dementia = 37; Psychiatric disorders = 6; Frontotemporal Dementia = 5; Unspecified Dementia = 5; Other neurological disorders = 7; Other = 16.
All patients referred to the Memory Clinic underwent a comprehensive medical and psychiatric assessment and a physical examination by a Doctor. Comprehensive neuropsychometric testing was performed by a Psychologist. Following this, a multidisciplinary team of Old-Age Psychiatrists, Clinical Psychologists, and Memory Clinic Nurses assigned a consensus diagnosis according to published criteria [9–11]. At each yearly follow-up, the same process was repeated, again assigning a consensus diagnosis which was recorded on the clinical database.
Ethical review
The present study was reviewed and received approval from London –South East Research Ethics Committee with reference number 15/LO/1752.
Data collected at baseline and yearly intervals
Data collected for each patient at baseline included age, gender, years of education, medical and psychiatric history, mental state examination, and physical examination (including full neurological examination). Schedules performed included the Clinical Dementia Rating (CDR) [12] and Modified Hachinski score (at baseline only) [13]. The presence of DLB features was assessed and recorded at each visit, with support from the Clinician Assessment of Fluctuation Scale [14], Mayo Sleep Questionnaire [15], and the Unified Parkinson Disease Rating Scale part III (UPDRS) [16]. Patients with significant depressive or anxiety symptoms fulfilling ICD-10 diagnosis of a mood disorder or a neurotic, stress-related, and somatoform disorder were excluded. In the very early stages of the study, before some of the above scales were available, a locally devised checklist was used to capture sleep disorders andfluctuations.
Cognitive testing included Mini-Mental State Examination (MMSE) [17], the CAMCOG-R [18], Wechsler Memory Scale (third edition abbreviated) Logical Memory Test (WMS LMT) [19], and tests of executive function (Trail Making Tests A and B, category and letter fluency (FAS)). Additionally, a 10-item word recall task was used where scores reflect the mean of 3 tries to recall the list [20].
Subdomains of the CAMCOG-R (maximum scores) are: Orientation (10), Language comprehension (9), Language expression (21), Remote memory (6), Recent memory (4), New learning (17), Attention/calculation (9), Praxis (12), Abstract thinking (8), and Perception (9). The CAMCOG-R includes a task of drawing a clock showing a specific time. On the CAMCOG-R, this is part of the praxis subdomain and is scored out of 3. However, the ACE-R [21] scoring rubric was applied to this item and it was scored out of 5. At each follow-up, all schedules and cognitive testing were repeated with the exception of the modified Hachinski score. Any additional medical or surgical history was also recorded.
At baseline, all patients had a dementia blood screen, and structural imaging performed. Imaging was preferentially MRI but CT was performed where MRI was contraindicated or where the patient was unable to tolerate MRI. Imaging reports included Fazekas score for vascular pathology [22]. At follow-up, imaging was only repeated where there was a specific clinical indication.
For the diagnosis of MCI, the Petersen et al. criteria were used [11]. Prior to the publication of these criteria, we were using broadly similar criteria and a retrospective check confirmed that the minority of patients who were assessed before the publication of the Petersen et al. criteria did indeed fulfil the Petersen et al. criteria. Patients with MCI were divided into amnestic and non-amnestic categories based on their performance on the WMS LMT [19]. At follow-up, established criteria were used for the diagnosis of clinically probable AD and DLB [9, 10] by a multidisciplinary consensus. Other diagnostic groups were excluded from the study, including patients with Subjective Cognitive Impairment (subjective cognitive complaints but performance not below 1.5 standard deviations of the norm expected for age on WMS LMT [19]), vascular dementia [23], Parkinson’s disease dementia [24], and frontotemporal dementia [25].
Statistical analysis
Statistical analyses were carried out using IBM SPSS version 19. We calculated baseline group characteristics for three groups of patients with MCI: those who remained stable (stable-MCI), those who declined to DLB (DLB-MCI), and those who declined to AD (AD-MCI). Data for continuous variables were not normally distributed; therefore these were compared using Kruskal-Wallis tests. Mann-Whitney U-tests (two-tailed) were used to make pairwise comparisons only where the ANOVA was significant at p < 0.05. Chi-square or Fisher’s exact tests were used to determine whether there were group differences on categorical variables. Where the 3-group test had a p < 0.05, pairwise analyses were performed.
RESULTS
Of the 1,848 patients seen at the memory clinic, 560 patients had an initial diagnosis of MCI, 496 had AD (no significant vascular pathology on MRI or CT) or AD with cerebrovascular disease (presence of small vessel ischemia on MRI or CT, Fazekas score 1-2 [22]), 192 had Subjective Cognitive Impairment [26], 141 had other neurological disorders, 130 had vascular dementia, 115 had a psychiatric disorder, 67 had DLB, 43 had frontotemporal dementia, 30 had dementia unspecified, 15 had alcohol related cognitive decline, 11 had Parkinson’s disease dementia, and 48 had other diagnoses.
Of the 560 MCI patients, 429 had a minimum of one-year follow-up. One hundred and sixty-four remained MCI (stable-MCI) while 107 progressed to AD and 21 to DLB at last follow-up. For the whole cohort, the mean follow-up was 2.8 years. One hundred and twenty-six patients were excluded due to alternative diagnoses at follow-up and 11 were excluded due to missing data (see Fig. 1).
The demographic details of the three groups are listed in Table 1. The stable-MCI patients were younger and this reached statistical significance versus patients who converted to AD. As expected, UPDRS score was higher in the MCI patients who converted to DLB compared to patients who converted to AD as well as patients with stable-MCI. There was a greater proportion of males in the DLB-MCI group relative to the other two groups. The patients with stable-MCI had longer follow-up as they continued to be followed-up clinically whereas the patients progressing to dementia were referred to treatment clinics.
Demographic and clinical data for the groups
MCI, Mild Cognitive Impairment; DLB, dementia with Lewy bodies; AD, Alzheimer’s disease; AMCI, amnestic MCI; NAMCI, non-amnestic MCI; UPDRS, unified Parkinson’s disease rating scale; IADL, instrumental activities of daily living; RBD, rapid eye movement sleep behavior disorder. Values for continuous variables are mean (standard deviation). Δ For length of follow-up, values are median (range). Categorical variables are compared with Chi Square; Continuous variables are compared with Kruskal-Wallis for 3-way group comparisons and Mann-Whitney U-test for 2-way group comparisons. a and b are used to denote pairs that differ at p < 0.05. #1 MCI-DLB case, 3 MCI-AD and 6 stable-MCI cases had missing data for years education. ∧1 MCI-AD and 2 stable-MCI cases had missing data for duration of cognitive difficulties. *4 MCI-AD Cases and 25 stable-MCI cases had missing data for IADL.
There was a greater proportion of patients with amnestic MCI subtype in the AD-MCI group relative to the other two groups. There was a higher frequency of parkinsonism, visual hallucinations, fluctuating cognition, and RBD in the DLB-MCI group but this only reached significance for parkinsonism, fluctuating cognition, and RBD (see Table 1).
DLB-MCI patients performed significantly worse than AD-MCI patients and stable-MCI patients on letter fluency and the clock drawing test. DLB-MCI patients performed significantly better than AD-MCI patients on the new learning subscale of CAMCOG-R. For a full list of results on cognitive testing, see Tables 2 and 3.
Scores for patients at time of conversion to dementia or last follow-up are shown in Tables 4–6. Three patients with a DLB diagnosis had dopamine transporter SPECT imaging (all 3 cases had abnormalscans with reduced uptake in the striatum). No autopsies were available. During post-diagnostic follow-up, DLB patients developed further typical features which increased the certainty of the DLB diagnosis (95% had parkinsonism, 71% had visual hallucinations, 57% had fluctuations, and 38% had RBD).
Neuropsychological test scores for the groups
MCI, Mild Cognitive Impairment; DLB, dementia with Lewy bodies; AD, Alzheimer’s disease; MMSE, Mini-Mental State Examination; WMS LMT, Wechsler memory scale logical memory test; TMT, trail making test. Values are mean (standard deviation). Variables are compared with Kruskal-Wallis for 3-way group comparisons and Mann-Whitney U-test for 2-way group comparisons. a and b are used to denote pairs that differ at p < 0.05. #1 DLB-MCI case, 1 AD-MCI case and 1 stable-MCI case had missing data for word recall. ‡2 stable-MCI cases had missing data for TMT-A due to non-completion. Δ 9 DLB-MCI cases, 27 AD-MCI cases and 38 stable-MCI cases had missing data for TMT-B due to non-completion. *1 DLB-MCI case, 9 AD-MCI cases and 15 stable-MCI cases had missing data for Clock drawing test.
Cambridge Cognitive Examination-Revised test scores for the groups
MCI, Mild Cognitive Impairment; DLB, dementia with Lewy bodies; AD, Alzheimer’s disease; CAMCOG-R, Cambridge Cognitive Examination-Revised. Values are mean (standard deviation). Variables are compared with Kruskal-Wallis for 3-way group comparisons and Mann-Whitney U-test for 2-way group comparisons. a and b are used to denote pairs that differ at p < 0.05.
Demographic and clinical data for the groups at follow-up
MCI, Mild Cognitive Impairment; DLB, dementia with Lewy bodies; AD, Alzheimer’s disease; IADL, instrumental activities of daily living; UPDRS, unified Parkinson’s disease rating scale; RBD, rapid eye movement sleep behavior disorder. Values for continuous variables are mean (standard deviation). Categorical variables are compared with Chi Square; Continuous variables are compared with Kruskal-Wallis for 3-way group comparisons and Mann-Whitney U-test for 2-way group comparisons.a,b, and c are used to denote pairs that differ at p < 0.05.
Neuropsychological test scores for the groups at follow-up
MCI, Mild Cognitive Impairment; DLB, dementia with Lewy bodies; AD, Alzheimer’s disease; MMSE, Mini-Mental State Examination; WMS LMT, Wechsler memory scale logical memory test; TMT, trail making test. Values are mean (standard deviation). Variables are compared with Kruskal-Wallis for 3-way group comparisons and Mann-Whitney U-test for 2-way group comparisons. Letters a and b are used to denote pairs that differ at p < 0.05. Δ 12 DLB cases, 58 AD cases, and 52 stable-MCI cases had missing data for TMT-B due to non-completion.
Cambridge Cognitive Examination-Revised test scores for the groups at follow-up
MCI, Mild Cognitive Impairment; DLB, dementia with Lewy bodies; AD, Alzheimer’s disease; CAMCOG-R, Cambridge Cognitive Examination-Revised. Values are mean (standard deviation). Variables are compared with Kruskal-Wallis for 3-way group comparisons and Mann-Whitney U-test for 2-way group comparisons. a and b are used to denote pairs that differ at p < 0.05.
DISCUSSION
In this large cohort, we found that already at the stage of MCI, there are clear differences in clinical features between patients who developed DLB, patients who progressed to AD, and those who remained stable. There are also clear differences on a number of cognitive tests. MCI patients who progressed to DLB were significantly more likely to have parkinsonism, fluctuating cognition, and RBD even at this early stage. They also had more frequent visual hallucinations, although this was only a trend. On cognitive testing, patients that later progressed to DLB performed worse at baseline on letter fluency and on a visuospatial task compared to patients that progressed to AD.
Overall, our results are in keeping with the findings of previous studies. Our finding that patients with prodromal DLB are more likely to have RBD, cognitive fluctuations, or parkinsonism is in keeping with the existing literature [7, 28]. Some studies have found visual hallucinations to be more common in DLB-MCI patients [8], however in our study this was only a trend.
This study strengthens the concept of prodromal DLB [29] and suggests that the core and suggestive features of DLB can be present a number of years before the manifestation of significant cognitive decline and functional impairment. The presence of these features in MCI patients should alert clinicians that this could be the early stages of DLB. Performing more in-depth cognitive assessment can also add support to the diagnosis of prodromal DLB. We found impairment in visuospatial ability, and this is consistent with the findings of previous studies [7, 28]. We also found a significant difference in letter fluency relative to prodromal AD or stable-MCI which is consistent with the existing literature [8, 27].
The diagnosis of prodromal DLB is important. Any successful disease modifying treatment for DLB will have to be pathology-specific and will need to be introduced at the earliest possible stage of the disease course. This is also relevant to AD trials which depend on the study cohort having specific AD pathology. Contamination of prodromal AD cohorts by prodromal DLB could be a major obstacle to success.
The strengths of this study include that it is the largest cohort of its kind in Europe and the second largest worldwide [7]. Furthermore, it reports on an unselected incidence cohort from a secondary care service serving a local population with a clear catchment area and very limited alternative private provision. All patients underwent an identical comprehensive assessment at each follow-up and only a very small number of cases had missing data. All diagnoses were made by consensus in a multidisciplinary team and patients had a good length of follow-up.
This study had some limitations. Diagnosis was made according to the present diagnostic criteria based on clinical features only without the support of dopamine transporter scan in the majority of cases. No cases had polysomnography. The observed differences are at a group level and do not allow clinicians to accurately predict the outcome for individual patients. This will most probably require additional biomarkers to support the clinical diagnosis of prodromal DLB. Another limitation is the lack of neuropathological confirmation of diagnosis which will require a long-term follow-up. Lastly, only a small proportion of the initial MCI cohort converted to DLB although this is consistent with the lower incidence of DLB compared to AD.
Footnotes
ACKNOWLEDGMENTS
We thank the patients and carers who took part in the study. We are grateful to Aidan O’Keefe who provided statistical advice. We are also grateful toDr. Rodney Walker for providing helpful comments on an earlier draft of the manuscript.
There was no specific funding source. The project was carried out as part of an MSc degree with University College London as the sponsor. Tim Whitfield was funded by the UK National Institute for Health Research network.