
Abstract
Keywords
INTRODUCTION
Neuropsychiatric symptoms (NPS) are common features of all types of dementia, irrespective of disease etiology and disease stage [1]. They are a heterogeneous group of non-cognitive symptoms and behaviors [2] and are observed in high rates across the spectrum from mild cognitive impairment (MCI) to dementia. NPS are among the most challenging and costly aspects of dementia, and, if left untreated, are associated with hastened disease progression, worsened daily functioning, impaired quality of life, increased healthcare utilization, and accelerated placement in residential care [3].
Prevalence estimates of NPS are reported among 31%–50% of individuals with MCI [4–6] and 61%–97% of individuals with dementia [7, 8]. It is well accepted that the comorbid presentation of NPS in MCI is linked to higher progression to dementia [9–15] and that for patients with Alzheimer’s disease (AD), NPS are associated with an increased likelihood of progression from mild to severe dementia [16].
To help understand the etiology of NPS, a number of studies have attempted to sub-categorize individual NPS using associative clustering [17]. Commonly identified clusters in dementia include an affective syndrome and a psychotic syndrome, with frontal/hypomanic and hyperactivity syndromes being less consistently observed [18]. However, while a systematic review of NPS found low concordance of evidence for NPS clusters derived from the Neuropsychiatric Inventory (NPI) in dementia samples [18], some NPS may define potential sub-syndromes of AD. Interestingly, Forrester et al. [19] recently linked patterns of NPS in incident MCI to an increased likelihood of progression to dementia, demonstrating the severe symptom class (consisting of agitation, anxiety, apathy, night-time behaviors, inhibition) to have a 2-fold higher risk of progressing to dementia (hazard ratio (HR) = 2.69, 95% confidence interval (CI): 1.12–2.70), while the affective class (consisting of depression, anxiety, irritability, night-time behaviors) had a one-point-five-times higher risk of progressing to dementia (HR = 1.70, 95% CI: 1.12–2.70) when compared to the asymptomatic class.
The importance of NPS as an intrinsic aspect of prodromal stages of dementia (e.g., MCI) and an early marker of cognitive decline is increasingly being recognized [20]. For example, Geda and colleagues [21] have shown that in cognitively healthy older adults (aged >70 years), the presence of NPS, specifically agitation, apathy, anxiety, irritability, depression, are linked to an increased risk of developing MCI in comparison with cognitively healthy without NPS. The concept of ‘mild behavioral impairment’ (MBI) has been proposed to describe this late-life transitional state, where the presence of NPS in the absence of cognitive symptoms confers an increased risk of incident MCI and dementia [22].
Most of the studies on NPS to date have focused on highly selective clinical samples recruited from tertiary care centers [12, 23–25] or as subsamples of population-based cohorts [4, 26]. This means that there is a gap in our knowledge about the spectrum of NPS occurring in the population across different cognitive phenotypes, disorders, outcomes, and status. Likewise, there has been sparse epidemiological research on the pattern of NPS across diagnostic groups and specifically, normal ageing (i.e., cognitively normal). Understanding such patterns will help inform our understanding of risk states such as MBI, and will assist with clinical assessment [27, 28].
This paper examines the prevalence and pattern of NPS in a large epidemiological study of older adults that includes individuals with normal cognition, those classified as “cognitively normal, but at risk” (CN-AR; characterized by objective cognitive impairment, either asymptomatic or symptomatic, that do not meet the criteria for MCI or dementia), as well as those with clinical diagnoses of MCI and dementia. Specifically, this study investigates: 1) the prevalence of NPS across the spectrum from normal cognition to dementia in older adults; 2) the risk for dementia, MCI, and CN-AR based on the presence and number of co-morbid NPS; and 3) clusters of symptoms across diagnostic groups within the population and whether these clusters are associated with an increased risk of dementia, MCI, or CN-AR in comparison with those without cognitive impairment.
METHOD
Subjects
Subjects were sampled from wave four of the oldest cohort (aged 60–64 at baseline) of the Personality and Total Health Through Life (PATH) study [29]. The PATH study is a representative, community-based longitudinal cohort study which commenced in 2001. Follow-up assessments were every four years up to 12 years. Participants are residents of the city of Canberra and the adjacent town of Queanbeyan, Australia, and were randomly recruited through the electoral roll [29]. Enrolment to vote is compulsory for Australian citizens. The study was approved by the Australian National University Human Research Ethics Committee (Protocol: 2012/074) andparticipants provided written informed consent after receiving a complete description of the study.
Of the 2,551 older PATH subjects at baseline, 1,644 completed the fourth wave of assessments. 1,417 subjects completed the informant-based PATH Neuropsychiatric Symptoms sub-study (PATH-NPS) at wave four. Of these, 40 were classified as having dementia (17 probable AD; 7 possible AD; 1 probable vascular dementia; 1 Lewy body dementia; 3 dementia with Parkinson’s disease), 133 were classified as having MCI (39 amnestic single domain; 47 amnestic multiple domain; 34 non-amnestic single domain; 12 non-amnestic multiple domain); 397 were classified as CN-AR; and 847 were cognitively normal. Figure 1 presents the sample selection flow chart, including information on cognitive status of subjects.
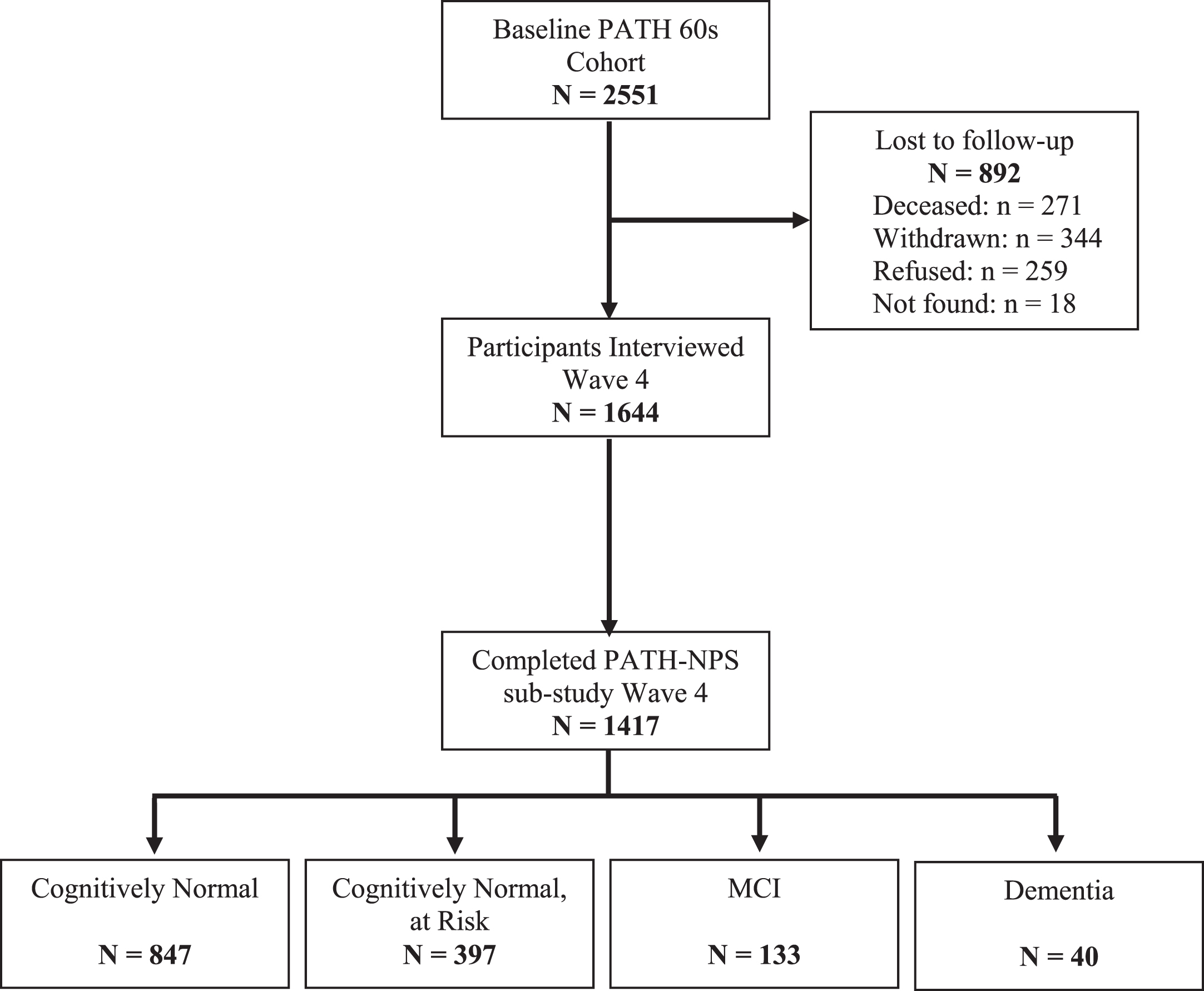
Sample selection flow-chart.
Cognitive function states and clinical diagnoses
Diagnostic procedures used to determine cognitive function states and clinical diagnoses at Wave 4 are published elsewhere [30]. In summary, for the 1,644 participants assessed at Wave 4, their data was screened for signs of decline based on the following criteria: a previous PATH diagnosis of dementia or a mild cognitive disorder, or evidence of current objective cognitive impairment (based on performance ≤6.7th percentile on at least one cognitive measure, or Mini-Mental State Examination (MMSE) ≤24), and evidence of subjective decline on the Memory and Cognition Questionnaire (MAC-Q) [31] or decline on the MMSE of >3 points since wave 3, or consistent MMSE ≤24 at waves 3 and 4 [30].
Clinical diagnoses were based on a case file review by a research neurologist and confirmed following a consensus diagnosis with a clinician specializing in psychiatry. Case files were reviewed by the research neurologist and included neuropsychological test data, informant data, structural brain MRI scans to aid differential diagnosis of dementia subtypes, self-reported medication list, and contact of participant for further clarification of details relevant to diagnosis [30]. Inter-rater reliability indicated high agreement between the neurologist and psychiatrist in the independent review of a subsample of29 cases [30].
Clinical diagnosis of dementia was made using the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (DSM-IV). MCI was assessed using the Winblad [32] criteria for MCI. Subjects were considered CN-AR if they did not meet the Winblad [32] criteria for MCI or the DSM-IV criteria for dementia; but demonstrated signs of impairment as identified by the screening criteria outlined above [30]. Individuals who did not meet any of the above criteria were classified as cognitively normal.
Informants
Informants were nominated by the PATH participant and provided information on the participants’ physical and mental health via a telephone interview. PATH participants provided written consent to contact the nominated informant. Informants were predominantly spouses (49.8%), children (33.7%), or a close friend (9.5%).
Measures
NPS were assessed using the NPI, a structured informant interview with established reliability and validity [33]. The NPI assesses the presence, frequency, and severity of 10 neuropsychiatric symptom domains (delusions, hallucinations, agitation/aggression, dysphoria/depression, anxiety, irritability, disinhibition, euphoria, apathy, aberrant motor behavior) and two neurovegetative domains (sleep and night-time behavior change, and appetite/eating change).
Each domain is scored by multiplying the domain frequency (scored 1–4) by the domain severity (scored 1–3), resulting in domain scores ranging from 1–12. If a symptom is absent the domain is scored as zero. Higher scores indicate greater symptom frequency/severity. Symptoms were considered clinically relevant if the domain score was ≥4 [8, 34].
Socio-demographic measures for age, gender, and education were obtained using self-report. Education was reported as completed years of education.
Statistical analyses
Demographic characteristic and NPS prevalence rates were assessed using IBM SPSS Statistics 22.0. Latent Class Analysis (LCA) was undertaken in MPlus v7.2. LCA identifies unobserved population heterogeneity and derives substantively meaningful groups of people who are similar in their responses to NPI. The objective was to categorize people into classes using the observed items and identify items that best distinguish between classes. The number of classes was determined by comparing solutions of different models with varying numbers of classes. Nested models can be compared to test whether the more complex model fits the data significantly better than the more parsimonious model. The fit of the two models can be compared by the Lo-Mendell-Rubin (LMR) Likelihood Ratio Test and the Vuong-Lo-Mendell-Rubin (VLMR) Likelihood Ratio Test, as well as information criterion indices including the Bayesian Information Criterion (BIC) and Akaike’s Information Criterion (AIC) or the sample-size-adjusted BIC (BIC_adj). Entropy values between 0 and 1 indicate the extent to which participants are correctly designated an appropriate class, with higher values reflecting better classification. A series of multinomial regression analyses were conducted in STATA v14 to 1) determine the risk associated with the presence and number of co-morbid NPS on cognitive impairment category (i.e., dementia, MCI, and CN-AR) when compared to the cognitively normal cohort; and 2) whether, in comparison with the cognitively normal cohort, class membership was associated with cognitive impairment category (i.e., dementia, MCI, and CN-AR).
RESULTS
Socio-demographic characteristics are presented in Table 1. As would be expected, the diagnostic cohorts differed significantly in age (F(3, 1399) = 5.36, p = 0.001), years of education (F(3, 1340) = 5.56, p = 0.001), and MMSE scores (F(3, 1397) = 146.9, p < 0.001).
Descriptive of socio-demographic variables
CN-AR, cognitively normal but at risk; MCI, mild cognitive impairment; MMSE, Mini-Mental State Exam; NPI, Neuropsychiatric Inventory; ApoE, apolipoprotein E; ɛ4–/ɛ4– =ɛ2/ɛ2 + ɛ2/ɛ3 + ɛ3/ɛ3; TIA, transient ischemic attack. NB: Medical Comorbidities are based on self-report at Wave 4.
Informant relationship type (i.e., spouse, child, friend, other) was not associated with higher reporting of NPS (χ2 (3, N = 1417) = 4.33, p = 0.228), with 39.9% of spouses, 39.4% of children, 30.6% of friends, and 40.6% of informants representing other relationship types reporting NPS among participants. Similarly, no significant differences were either observed between informant relationship type and frequency of the individual NPI domains.
Neuropsychiatric symptom prevalence rates
Of the 1,417 community-dwelling older adults in this study, 38.9% (n = 551) were reported to have any NPS. The most commonly reported NPS were: depression (19.8%; CI = 17.9–22.1), agitation (12.3%; CI = 10.6–13.8), sleep disturbance (12.1%; CI = 10.4–13.9), irritability (10.4%; CI = 8.8–12.1), appetite disturbance (6.5%; CI = 5.3–7.9), apathy (6.1%; CI = 4.9–7.5), disinhibition (5.7%; CI = 4.5–7.0), anxiety (4.7%; CI = 3.7–5.8), aberrant motor behavior (2.0%; CI = 1.4–2.8). Delusions (1.5%; CI = 0.9–2.2), euphoria (1.1%; CI = 0.6–1.7), and hallucinations (0.7%; CI = 0.3–1.2) were the most uncommon symptoms. Noteworthy, of the 551 participants with NPS, 51.4% reported two or more comorbid NPS, with 42.7% presenting with between two and four comorbid symptoms, while 8.7% presented with five or more comorbidsymptoms.
Prevalence rates of NPS across the spectrum from cognitively normal to dementia are presented in Fig. 2. As expected, significant differences in NPS were reported between the diagnostic cohorts (χ2 (3, N= 1417) = 74.7, p < 0.001). The highest proportion of NPS being reported among the dementia cohort (80%) and the MCI cohort (53.4%). Interestingly, high rates of NPS were nonetheless found in both the CN-AR cohort (47.1%) and the cognitively normal cohort (30.8%).

Prevalence of individual neuropsychiatric symptoms according to cognitive domain. The lighter shaded areas in the graphs represent clinically significant symptoms (i.e., domain score ≥4). Whiskers indicate 95% confidence intervals for the entire sample. CN-AR, cognitively normal but at risk; MCI, mild cognitive impairment.
Association between neuropsychiatric symptoms and cognitive impairment
The risk associated with the presence and number of co-morbid NPS on dementia, MCI, and CN-AR state are reported in Table 2. Presence of NPS were associated with a 3-fold increased risk of dementia (relative risk ratio (RRR) = 3.13; 95% CI = 1.19; 8.25), with a 2-fold increased risk of MCI (RRR = 2.23; 95% CI = 1.31–3.78) and a 1.5-times increased risk of CN-AR (RRR = 1.53; 95% CI = 1.06–2.21). Importantly, the presence of additional co-morbid NPS symptoms were associated with an additional 1.5-times increased risk of dementia (RRR = 1.53; 95% CI = 1.26–1.85), but not MCI or CN-AR.
Risk of dementia, MCI, and CN-AR associated with presence of neuropsychiatric symptom and each additional co-morbid symptom
RRR, relative risk ratio; CI, confidence interval; CN-AR, cognitively normal but at risk; MCI, mild cognitive impairment; NPI, Neuropsychiatric Inventory.
Neuropsychiatric symptom clusters in PATH
Cluster analysis of individual NPS (does not present NPS/presents NPS) were conducted on those who reported two or more NPS to examine whether different symptom clusters were indicative of differential diagnosis (n = 283). Model fit indices supported a model whereby symptoms clustered together in four classes (Table 3). Despite a larger entropy score, a model with a 5th class was not considered as even with 750 random starts, the best Log-Likelihood value was not replicated, suggesting that the solution could be due to local maxima. Hence the results of a 5th class were not considered admissible. In comparing the 3 and 4 class models, Goodness of Fit Indices (GFI) supported the 4th class model. The Log Likelihood, AIC, and BIC_adj were lower than those GSI reported with the 3 class model and Entropy remained high at 81%. In addition, a significant bootstrap Likelihood Ratio test suggested that the 4 class model was a better fitting model than the 3 class model.
Goodness of Fit indices for a series of latent class analyses of the neuropsychiatric symptom in the PATH Through Life Study
AIC, Akaike Information Criteria; BIC, Bayesian Information Criteria; BIC_adj, sample-size adjusted BIC; LRT, likelihood ratio test. ***p < 0.001; *p < 0.05; significance values reflect the difference in likelihood between k classes and k-1 classes.
Figure 3 shows the proportion of participants reporting NPI symptoms by class. Class 1 (termed: frontal/low comorbidity) was characterized by extremely high prevalence of agitation (87.9%), disinhibition (60.6%), and irritability (69.7%) and a low number of comorbid symptoms (93.9% presenting with only two to four comorbid symptoms). Class 3 (termed: affective/low comorbidity group) was characterized by high prevalence of depression (79.0%) and low numbers of co-morbid symptoms (92.7% presenting with two to four comorbid symptoms). Similarly, Class 4 (termed: sleep/low comorbidity) was characterized by extremely high prevalence of sleep disturbance (100%) and low numbers of co-morbid symptoms (92.7% presenting with two to four comorbid symptoms). In contrast, Class 2 (termed: high prevalence/high comorbidity) was characterized by a high number of co-morbid symptoms (100% presenting with five or more co-morbid symptoms) and higher prevalence of each symptom compared to the other classes: agitation (93.3%), depression (80%), apathy (76.7%), disinhibition (66.7%), irritability (63.3%), and sleep disturbance (86.7%).
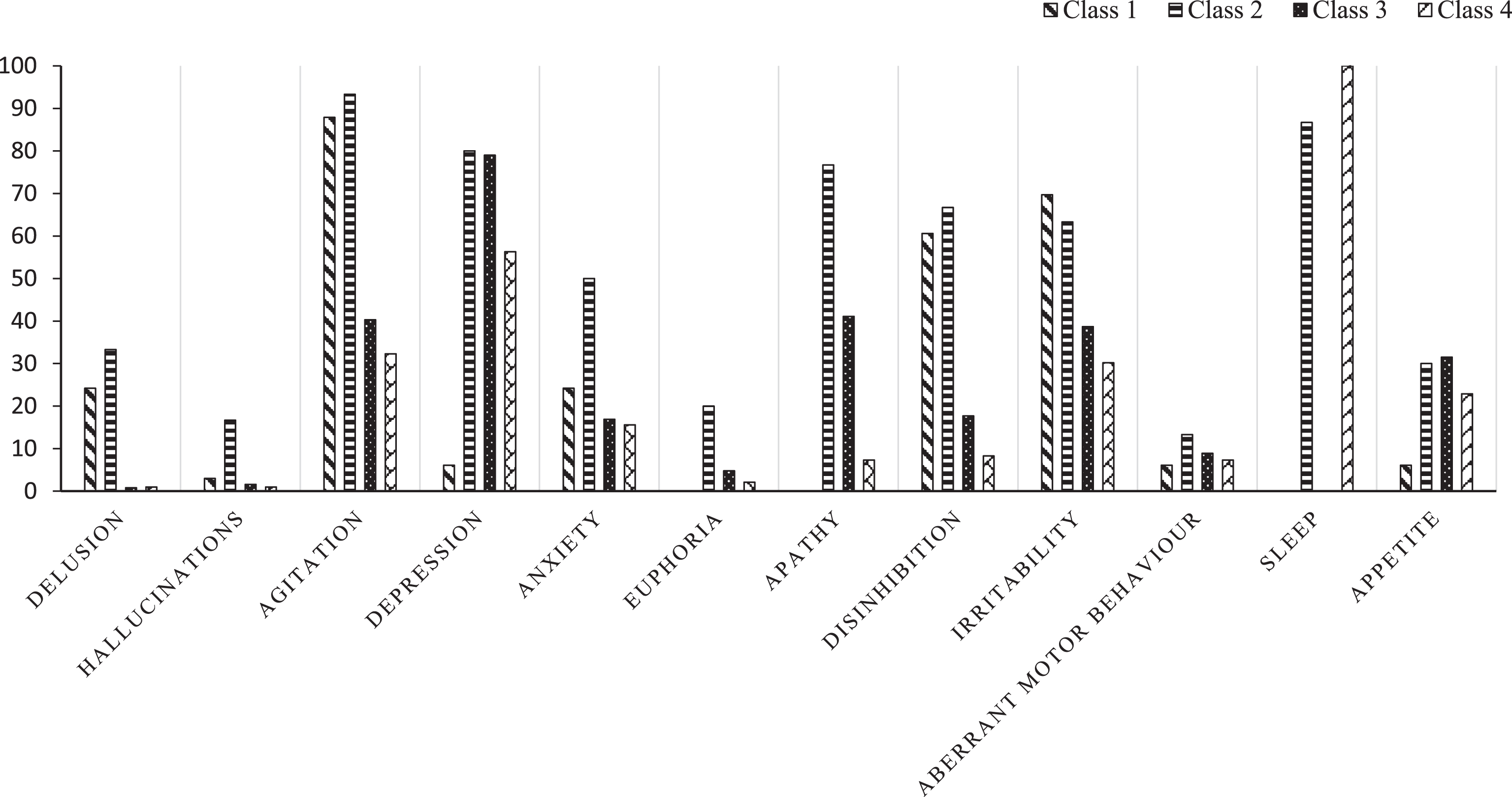
Proportions of individuals with reporting individual neuropsychiatric symptoms within each class (Class 1 = frontal/low comorbidity group; Class 2 = high prevalence/high comorbidity group; Class 3 = affective/low comorbidity group; and Class 4 = sleep/low comorbidity group).
Association of neuropsychiatric symptoms class with risk of cognitive impairment
We compared whether different classes of symptom cluster were associated with risk for dementia, MCI, or CN-AR in comparison with those without cognitive impairment (Supplementary Table 1). A series of multinomial regression analyses showed that, in comparison with the cognitively normal cohort, class membership was not significantly associated with cognitive impairment category (dementia, MCI, CN-AR).
Sensitivity analysis
Given the unbalanced sample sizes of the cohort, a Monte Carlo simulation on a number of our results were run to examine the extent to which our estimates were impacted by unbalanced group size. The Monte Carlo simulations revealed our model estimates were within the 95% CI of each replication for between 94% and 95% of the simulations. Power estimates for individual estimates to reject the null hypothesis (that is, the estimate of type 1 error) were mostly between 0.99 and 1.00. Of the 18 parameters estimated in each simulation (variances, means, regression coefficients), only two reported power estimates below 0.99 (both were >0.70). Overall, we were satisfied that our results in Supplementary Table 1 are valid and that cognitive diagnosis is unrelated to symptom cluster.
DISCUSSION
Three important findings were made: 1) prevalence of any NPS was relatively high and increased progressively from 30.8% in those with normal cognition to 80% in those with dementia; 2) a higher number of comorbid symptoms were associated with greater risk of dementia, and 3) latent class analysis revealed four NPS-classes, however NPS-class was not associated with severity of cognitive impairment.
Prevalence of NPS
NPS are common features of all types of dementia, irrespective of disease etiology and disease stage [1]. They are a heterogeneous group of non-cognitive symptoms and behaviors [2] and are observed in high rates across the spectrum from MCI to dementia. NPS are among the most challenging and costly aspects of dementia, and, if left untreated, are associated with hastened disease progression, worsened daily functioning, impaired quality of life, increased healthcare utilization, and accelerated placement in residential care [3].
Findings from this study show a high prevalence of NPS across the spectrum from cognitively normal to dementia in this population-based sample. As expected, those with MCI and dementia reported the highest prevalence of NPS (53.4% and 80%, respectively). This is consistent with previous reports of NPS in community-based samples of clinical groups, where NPS have been reported in 61% –97% of individuals with dementia [7, 8] and 31% –50% of individuals with MCI [4–6, 8]. These finding are or particular clinical relevance as it is well accepted that the comorbid presentation of NPS in MCI is linked to higher progression to dementia and that for patients with AD, NPS are associated with an increased likelihood of progression from mild to severe dementia [35].
Despite not meeting the diagnostic criteria for MCI, our CN-AR cohort reported similar proportions of NPS (47.1%) to the MCI cohort. This may, in part, be explained by the fact that the CN-AR cohort represents a cognitively ‘at-risk’ subgroup within the cognitively normal spectrum who do not meet criteria for MCI but who, in a clinical setting, would likely be considered to have subjective cognitive complaints. Our findings provide further support to the idea that NPS is an early marker for neurodegeneration that precedes significant cognitive impairment [20], and that NPS should be explored in those presenting with cognitive complaints [36].
The prevalence of NPS among the cognitively normal group (30.8%) was comparable to that previously reported by Geda et al. [5] in the Mayo Clinic Study of Ageing (25%, aged 70–89 years), but higher than that described by Okura et al. [37] who reported 18% prevalence of NPS in cognitively normal participants aged 71 and older, drawn from the Ageing Demographics and Memory Study. Differences in sensitivity of the NPI versus its brief form (NPI-Q) may account for the differences in NPS prevalence between PATH and prospective studies that have used the NPI-Q.
Symptom burden
In addition to the presence of any NPS, NPS burden was also significantly associated with dementia, such that each additional NPS conferred a 1.5-fold increased risk of dementia. This relationship was not apparent for MCI or CN-AR. The results are consistent with previous reports that dementia diagnosis is associated with a greater number of NPS [4, 19]. Studies of longitudinal trajectories of NPS from MCI to dementia [24, 38] report that although most of those with MCI (90%) demonstrate a low NPS burden that is stable over time [38], those who demonstrate increasing NPS burden (7%) or a high NPS burden at baseline have a 1.74 [38] to 2.55 [24] fold increase in risk of progression to dementia at follow-up. Together, this data supports the view that the neurodegenerative processes underlying dementia are accompanied by an accumulation of NPS, which can occur in advance of or in concert with cognitive impairment, adding further validation to the MBI construct. In our sample, between 14% and 27% of individuals without dementia (i.e., normal to MCI) had an NPS burden of 2 or more symptoms. Such individuals may be at a much higher risk of progression to dementia and may benefit from closer monitoring in a clinical setting than those with one or no NPS. Future follow-up of the PATH sample will be able to examine the predictive utility of NPS burden in dementia risk assessment.
Clusters of neuropsychiatric symptoms
To help understand the etiology of NPS, a number of studies have attempted to sub-categorize individual NPS using associative clustering [17]. Commonly identified clusters in dementia include an affective syndrome and a psychotic syndrome, with frontal/hypomanic and hyperactivity syndromes being less consistently observed [18]. However, while a systematic review of NPS found low concordance of evidence for NPS clusters derived from the NPI in dementia samples [18], some NPS may define potential sub-syndromes of AD. Interestingly, Forrester et al. [19] recently linked patterns of NPS in incident MCI to an increased likelihood of progression to dementia, demonstrating the severe symptom class (consisting of agitation, anxiety, apathy, night-time behaviors, inhibition) to have a 2-fold higher risk of progressing to dementia (HR = 2.69, 95% CI: 1.12–2.70), while the affective class (consisting of depression, anxiety, irritability, night-time behaviors) had a 1.5 times higher risk of progressing to dementia (HR = 1.70, 95% CI: 1.12–2.70) when compared to the asymptomatic class.
Cluster analysis of NPS across the whole sample revealed four main classes reflecting: 1) frontal/low comorbidity; 2) high prevalence/high comorbidity; 3) affective/low comorbidity; and 4) sleep/low comorbidity. To the best of our knowledge, our study is the first study that has examined NPS-clustering in a population-based sample with participants across the spectrum from cognitively normal to dementia.
The most prevalent NPS cluster was the ‘affective/low comorbidity’ class, which comprised 44% of all participants with multiple NPS (or 8.8% of all participants), and was characterized by a high prevalence of depression, apathy, agitation, and irritability. This NPS-class is similar to the symptom pattern commonly reported in studies of MCI samples [5, 40], and also the ‘affective’ cluster reported in studies of dementia samples [18]. In our study, 28% of all those with dementia (n = 11) and 19% of those with MCI (n = 25) were classified as having an affective/low comorbidity NPS pattern. This affective syndrome may be the predominant NPS pattern in MCI and AD [18]. For example, Lyketsos et al. [41] reported 28% of participants with AD in the Cache County study demonstrated an NPS syndrome characterized by high NPS burden as well as high prevalence of apathy, irritability, depression, and aberrant motor behavior. In our study, the affective syndrome had a low NPS burden, and likely reflects the fact that analysis by Lyketsos et al. [41] was restricted to those with AD, whereas our sample was clinically heterogeneous. Accordingly, ‘high comorbidity/high prevalence’ was a rare but distinct cluster in our study, accounting for 1–4% of those without dementia, and 10% of those with dementia. A similar ‘severe’ cluster was observed by Forrester et al. [19] which accounted for 7% of their clinically referred MCI sample (n = 540) and had a high risk of progression to dementia at two-years follow-up.
The second most prevalent NPS-class in our sample was termed ‘sleep disturbance/low comorbidity’ and was apparent across all cognitive categories (cognitively normal: 4%; CN-AR: 10%; MCI: 8%; dementia: 25%). The high prevalence of sleep disturbance in dementia and MCI has been previously observed [8, 42] and some studies suggest it may be associated with progression to dementia, possibly involving vascular etiology [43, 44].
The ‘frontal/low comorbidity’ symptom cluster was the least prevalent in our study, accounting for 0% to 3% of each cognitive category (total n = 33). This syndrome included high prevalence of agitation, disinhibition and irritability— a cluster that has been reported in dementia samples, and in conjunction with aberrant motor behavior [18]. Its low prevalence in the sample is also consistent with the literature. Disinhibition is rare in MCI [39, 40] and more common in later stage AD [45]. It is also associated with frontal atrophy [46] and has been reported to discriminate AD and vascular dementia from frontotemporal dementia [45]. Frontotemporal neurodegeneration is also associated with early behavioral symptoms in the absence of cognitive impairment, which may explain why this cluster had a similar prevalence across cognitive categories.
NPS clusters and relationship to cognitive impairment
Symptom patterns were not associated with risk of cognitive impairment in the current study. This is in contrast to studies that have linked patterns of NPS in incident MCI to an increased likelihood of progression to dementia at follow-up [19]. The current findings may be explained by the fact that cluster analyses are dependent on the sample composition, and that inclusion of different dementia types and symptom severity are likely to greatly influence the type of clusters obtained. In fact, most of the studies on NPS to date have focused on highly selective clinical samples recruited from tertiary care centers [12, 24] or as subsamples of population-based cohorts [4, 19], making it difficult to understand the evolution of NPS across the spectrum from normal to MCI and dementia.
Follow-up of our sample may help identify baseline NPS clusters that may be more likely to progress to dementia. The clinical heterogeneity of our sample relative to most other studies, and the small sample size of some of the clusters, may explain the lack of an association between clusters and cognitivecategories.
Implications
The concept of MBI has been proposed as a late-life transitional state between normal cognitive aging and dementia (i.e., prodromal stage of dementia), in which the presence of later-life onset NPS in cognitively normal individuals or those with MCI confers an increased risk of developing dementia [22]. The current findings highlight the importance of NPS and the need for clinicians to consider the presence of NPS in cognitively normal as a possible risk state. Longitudinal follow-up of this PATH sample will be important to track the evolution of MBI in relation to cognitive decline and diagnosis [27]. Future research will also need to investigate how current symptom clusters compare to the symptoms contained in the five MBI domains, to determine their prognostic value for cognitive decline and dementia incidence.
Although our cluster analysis validates a number of NPS syndromes identified in the literature, we found that the number of co-morbid symptoms are a stronger correlate of cognitive impairment than the pattern of NPS symptoms as captured by the NPI and, as such, may be a more reliable index of progression.
Strengths/limitations
The cross-sectional design of the present study precluded investigation of changes in prevalence of NPS over time and risk of progression to cognitive impairment. However, future follow-up of the PATH cohort will examine longitudinal trajectories of NPS. As a population-based cohort, the PATH sample enabled us to examine NPS across a broader cognitive range. However, as might be expected, there were substantial differences in the sample sizes between the four cognitive function cohorts, with only 32 participants with dementia reporting NPS compared to 261 cognitively normal participants who reported NPS. Given the unbalanced sample sizes of the cohort, a Monte Carlo simulation on a number of our results were run to examine the extent to which our estimates were impacted by unbalanced group size. Overall, we were satisfied that our results are valid and that cognitive diagnosis is unrelated to symptom cluster. While the NPI is the most widely applied measure to assess NPS, both in a clinical and research setting, data are acquired from the informant, making the results susceptible to caregiver recall and interpretation bias. Strengths of the study include the large population-based sample, detailed neurocognitive assessments and consensus diagnoses. The limited age range is both a strength and weakness, as it reduces the impact of age on results but also reduces generalizability of findings to a wider age-range.
Footnotes
ACKNOWLEDGMENTS
MEM is supported by the Australian National Health and Medical Research Council (NHMRC) and Australian Research Council (ARC) Dementia Research Development Fellowship #1102028. RB is supported by the ARC Centre of Excellence in Population Ageing Research Project No. CE110001029. ZI is funded by the Hotchkiss Brain Institute with support from the Alzheimer Society Calgary. KJA is funded by NHMRC Fellowship #1102694. Wave 4 of the PATH Through Life Study was funded by NHMRC Grant #1002160. We would also like to acknowledge support from the Australian Research Council (ARC) CE110001029. We thank the study participants, PATH Interviewers, Kristine Koh, Trish Jacomb, and Karen Maxwell. We acknowledge the contribution of Helen Christensen, Peter Butterworth, Nicolas Cherbuin, Andrew McKinnon and Simon Easteal.