
Abstract
Keywords
INTRODUCTION
The aging population is a global challenge. Nonpharmacological interventions for individuals with mild cognitive impairment (MCI), such as aerobic exercise and mental activity, have been reported to significantly reduce the risk of further cognitive decline [1–7].
As attentional control is affected more often and earlier than memory and executive function among individuals with early MCI [8, 9], effective interventions should target at enhancing specific rather than global cognitive functions. A review of the studies on cognitive training for patients with MCI indicated that the majority of the intervention designs served multiple purposes. This perhaps explains why these interventions resulted in a nonspecific effect on improving cognitive function [5, 11]. This study aimed to test the efficacy of Chinese calligraphy writing training as a medium for training attentional control and working memory— a specific impairment in older adults in the early stage of MCI.
Chinese calligraphy writing involves using a brush to write Chinese characters, which have logographic outlook [12]. It is a mind-and-body activity that is culturally relevant to Chinese older adults [7, 13]. Mind-body practices hypothesize using the mind to influence body function [14]. Besides calligraphy, other common examples are guided imagery, Tai Chi, and Yoga. These practices are characterized with individuals engaging in concentration, and generation and visualization of mental images [15, 16]. Benefits brought by mind-body practices have been documented such as enhancing mental health [17], and global [18, 19] and specific cognitive function such as attention [20, 21] and spatial working memory [6, 22]. Previous clinical studies commonly classified calligraphy writing as a means of guided imagery or coordinated motor activity. Characters are written by mimicking a particular style and/or thinking about the semantic meaning of the written characters. There are five studies which explored the effects of calligraphy writing among clinical populations. Among them, only one study involved individuals with MCI. Kwok et al. [7] conducted a pilot study on an eight-week calligraphy therapy which was found to enhance general cognitive functions in the MCI participants. The other four studies reported that calligraphy writing benefited emotional stability in cancer survivors [23], stress control in individuals with stress [24], psychological adjustments in post-earthquake survivors [25], and blood pressure in hypertensive patients [26]. The current study was to fill the knowledge gap of whether calligraphy writing training would be effective for enhancing cognitive functions of individuals with MCI. Different from Kwok et al.’s study [7], we targeted at specific rather than general cognitive functions, and participants were followed-up for six months for testing long-lasting treatment effect of calligraphy writing training.
This study adopted a cognitive approach to designing calligraphy writing training in two ways (Fig. 1). First, the writing practice focused on encoding and attentional control processes where by the participant identified the “curve of the stroke” that composes the “shape of the character” unique to the style. Cambon et al. [27] revealed that training involving encoding of visual stimuli improved attention and memory of older adults. Second, mnemonic strategy (rehearsal, association, and imagery) [28] was reinforced when participant saw a Kai-styled character but wrote the character in a Hang-form. As the shape of a Kai-styled character is less square than a Hang-styled character, the Kai-to-Hang transformation would involve mnemonic strategy: 1) rehearsing the strokes of the Kai-styled character (in working memory); 2) associating the Kai-styled strokes with the learned Hang-styled strokes (retrieved from long term memory); and 3) imagining the character formed by the Hang-styled strokes (in working memory), before writing it with a brush. Previous studies on mental imagery identified attentional control, access to long term memory, and manipulation in working memory as the critical mental processes [29, 30]. Training involving mental rehearsal [31] and imagery [32] were found to effectively improve memory function among older adults. Therefore, we hypothesized that when compared with the control, individuals participating in the 8-week calligraphy training would show improvements in attentional control and working memory.

Hypothetical processes of transforming Kai to Hang styled character of (door, men) involved in the Chinese calligraphy writing. Learning began at the stroke level, as the participant was to associate the Hang- with the Kai-styled strokes. The steps involved in the Kai-to-Hang character transformation are: 1) encoding a Kai-styled character; 2) decomposing the character into Kai-styled strokes; 3) rehearsing Kai-styled strokes; 4) associating Kai-styled strokes with the learnt Hang-styled strokes; and 5) imagining the character formed by the Hang-styled strokes before writing it with a brush.
MATERIALS AND METHODS
Trial design
This was a randomized controlled trial with participants being randomly assigned into an experimental (Chinese calligraphy writing) or control group (learning use of tablet computer) in a 1:1 ratio. Block randomization method was used to maximize the chance that equal number of participants would be assigned to each group. The assessments were scheduled for the baseline, end of the intervention, and six months after the intervention.
Participants
Four hundred and fifty-four community-dwelling older adults were screened between June 2012 and March 2014. The selection criteria were: 1) aged 60 to 85; 2) score on the Montreal Cognitive Assessment (MoCA) [33, 34] was 19 to 26 [35]; 3) score on the Dementia Rating Scale was 0.5 or below [22, 36]; 4) self-report of cognitive decline; 5) independent in daily living activities; 6) education level of three years or more and able to read simple Chinese characters; and 7) willing to write with a soft brush and computer tablet. Individuals who had a history of neurological or mental disorders were excluded from the study. The CONSORT diagram describing subject flow from first contact to completion of the study is presented in Fig. 2. A total of 354 participants were excluded as they did not meet inclusion criteria (n = 229), decline to participate (n = 108), or other reasons (n = 17). As a result, 99 older adults entered into the study. Block randomization was conducted as soon as 20 to 24 participants who satisfied the inclusion criteria were gathered. Central randomization was used by submitting the names to a member who was not involved in the study process. Each of the participant was then randomly assigned to experimental or control group by drawing lot method (drawing names out of a concealed box on 1:1 ratio). There was no change to this method after commencement of the trial. The number of participants assigned to the two groups was 48 and 51, respectively. Four participants withdrew due to medical reasons before commencing the training program (two in each group). Five and two participants in the experimental and control group respectively did not complete all the three assessment occasions. The final sample sizes were smaller than the planned sample sizes which were 146 with 73 in each of the two arms (0.4 effect size for cognition stimulation training in MCI participants, power = 80%, two-sided test, p = 0.05). Ethics approval of this study was granted by the institution in which the study was carried out. All participants gave their informed consent before they entered into the randomization.
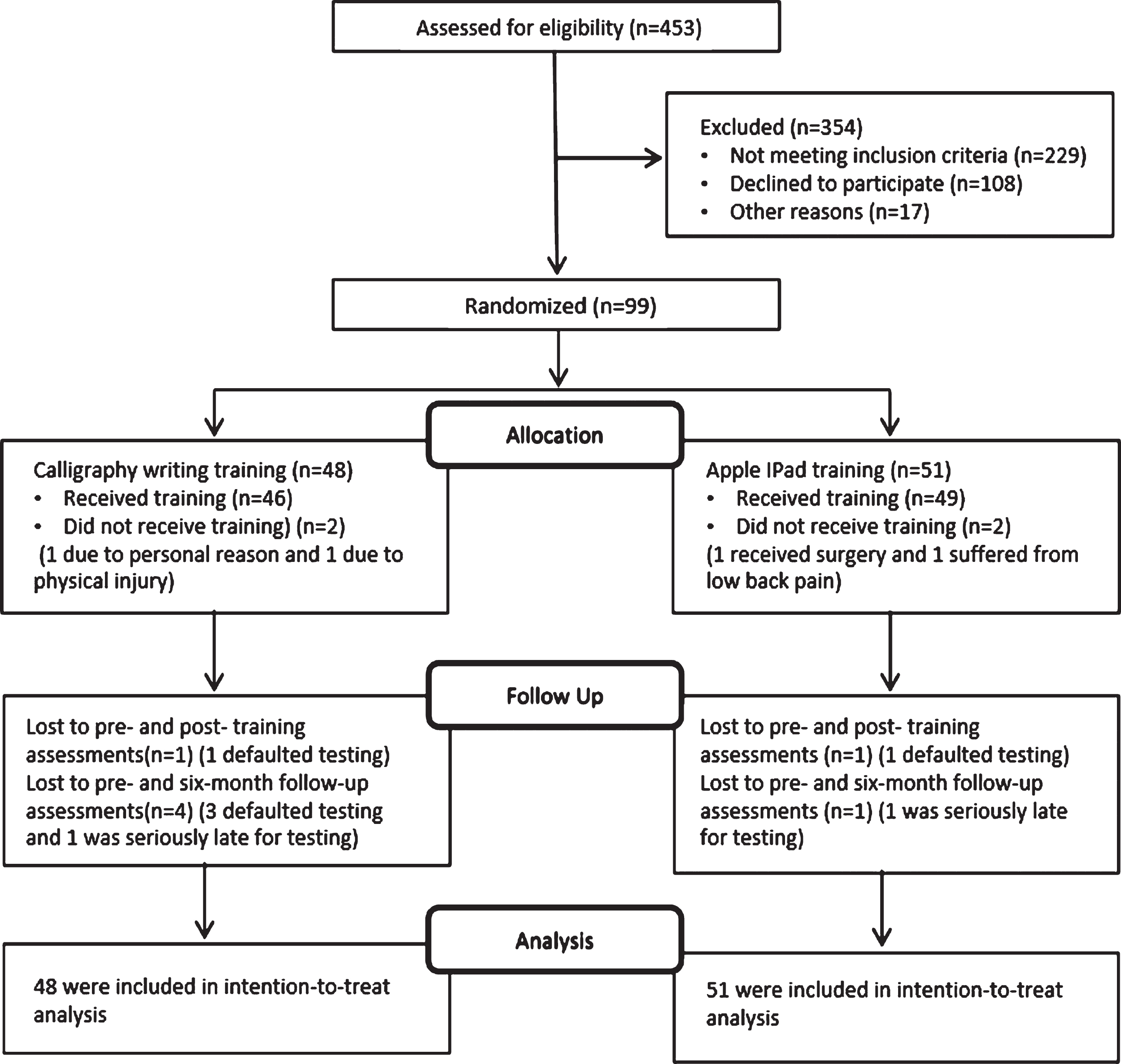
CONSORT flow diagram for the study.
Interventions
Both the calligraphy writing and tablet computer trainings were conducted in a group format (8 to 12 participants). It was eight weeks in duration with two 1.5 hour sessions each week. The total time of the training was 24 hours.
Chinese calligraphy writing training (experimental)
For the calligraphy training, participants learned and practiced writing of Chinese calligraphy using a soft brush pen. Each session was led by a professional calligraphy master and a research assistant. The 16 sessions were divided into two parts. The first eight sessions were for participants to learn writing basic strokes, while the second eight sessions were to learn writing characters. Learning of the strokes and characters involved Kai-to-Hang script transformation. The participants were to read a stroke/character presented in Kai script (or Kaishu) but to write it in Hang script (or Xingshu). Details of the implementation of the training sessions are presented in the Supplementary Material. An App was custom designed with which the participants practiced writing Hang-styled strokes for 15 minutes on a tablet computer before writing with soft brush pen on paper. There were two purposes for using a tablet computer for learning. First, the participants would be motivated by this method, as most of the older people were fond of using technology to assist learning. Second, the training received by the control group was learning how to use an Apple iPad, and so the use of the tablet computer by the participants would reduce the between-group effect brought by the contact with the tablet computer in the control group. On average, the participants wrote four to eight characters in one session. The master demonstrated the writing and provided verbal feedback to the participants with assistance from the research assistant throughout the session.
Tablet computer training (control)
The participants learned in 16 sessions the functionality of Apple iPad. The training was conducted by the research assistant and a part-time helper. At the beginning of each class, the participants spent 15 minutes using a pen to copy the characters of a poem printed in Kai script onto a piece of paper (see Supplementary Material).
Procedure of data collection
Screening of the potential participants was conducted by Research Assistant A (RA-A) assisted by a group of occupational therapy trainees who received training on test administration. Demographic information on age and gender as well as medical history was obtained and recorded. Participants who satisfied the inclusion criteria were referred to Research Assistant B (RA-B) who contacted the participants regarding the logistics of commencing the calligraphy or the tablet computer training. RA-B then contacted the participant and scheduled the time for the baseline assessment. RA-A was responsible for administering all the clinical instruments in the baseline and subsequent assessment occasions. RA-A did not have knowledge about the group membership of the participants. Training was provided to RA-A on the administration of all the clinical instruments. Each participant was to complete three assessments: baseline (within two weeks before the intervention), post-training (within two weeks after completing the intervention), and six-month follow-up (within two weeks after six months following the intervention). Five clinical measures were used to capture the between-group treatment effects. They were the Digit Span Test (Backward) (DST-Backward), Color Trails Test (CTT), Symbol-Digit Modalities Test (SDMT), Geriatric Depression Scale-Short Form (GDS-SF), and Consortium to Establish a Registry for Alzheimer’s Disease-Neuropsychological Assessment Battery (CERAD-NAB). The clinical measures were administered according to random sequence.
Outcome measures
The DST-Backward [37] assessed the participants’ auditory attention and working memory. The participant was read a series of digits and was required to recall and say the digits heard in a reversed order. The CTT [38], measure of attentional control, evaluated visual tracking, and attention in CTT1 and divided attention in CTT2. The participant was required to draw paths among digital circles in a consecutive order or among digital circles in a consecutive order and alternating color. The test construct was found to be relatively culture free for use among Chinese subjects [39]. The SDMT [40] was used to evaluate progressing speed and switching attention. The verbal form was employed. The SDMT was previously applied to the Chinese population and found to have good psychometric properties [41]. The GDS-SF assessed symptoms of depressive mood among older adults [42] and individuals with MCI [43]. The Chinese version of the GDS-SF was reported to have good psychometric properties for use among older Chinese individuals [44]. The CERAD-NAB assessed the participant’s verbal episodic memory [45]. The three subtests included immediate recall/encoding (J4), delayed recall (J6), and word recognition (J7). The Chinese version of the CERAD-NAB was validated by Liu et al. [46].
Data analysis
Independent t-tests or Chi-square was used to test the between-group differences in the demographic characteristics and scores on the clinical measures taken at the baseline assessment. The effects of intervention were analyzed according to the intention to treat principle, using a linear mixed model. Patient identification was specified as the random effect and Time (baseline, post intervention, and follow-up) and Group (calligraphy writing and control) were specified as the fixed effects. For each dependent measure, a 2 (Group)×3 (Time) linear mixed model for repeated measures was conducted. Significant interaction effects were followed with multiple comparisons using paired t-tests. No multiple imputation was needed for the linear mixed modelling and the Last Observation Carried Over method was used for replacing missing data in the post-hoc tests. Effect sizes were computed with Cohen’s d statistics (0.21 <small effects <0.5; 0.51 <medium effects <0.8). The IBM SPSS v.20 was used for conducting the analyses, and the significance levels for post-hoc comparisons were set at p≤0.025 (DST-Backward and SDMT (verbal)) and p≤0.017 (CTT and CERAD-NAB) after Bonferroni adjustments.
RESULTS
No significant between-group differences were revealed in the age, gender composition, and types of MCI (Table 1). The mean ages of the participants were 69.4 and 68.1 years for the experimental and control group, respectively. The mean scores on the MoCA were 24.5 and 24.4, respectively. Significant Group×Time effects were revealed on the scores of the DST-Backward (Sequence: p = 0.036; Span: p = 0.016) and CTT2 (p = 0.045) of the CTT (Tables 2A, B). Marginally significant interaction effects were found on the scores of CTT2-CTT1 (p = 0.058) of the CTT. Other comparisons for scores on the SDMT, CERAD-NAB and GDS-SF were not significant.
Demographic characteristics of the MCI participants in the Chinese calligraphy writing training (experimental) and tablet computer training (control)
MoCA, Montreal cognitive assessment; *between-group comparisons were conducted using t-tests or Chi-square test; #based on CERAD-NAB J4 cut-off <15/30.
Mean scores and their standard deviations (in bracket) on scores of different clinical outcome measures of participants in the Chinese calligraphy writing (experimental) and tablet computer training groups (control) for the baseline, post-training and six-month follow-up assessment occasions
DST-Backward, Digit Span Test (Backward); CTT, Color Trail Test; SDMT, Symbol-digit Modalities Test (Acc., Accuracy Rate; Correct, Correct Attempts; Total, Total Attempts); GDS, Geriatric Depression Scale.
Summary of results of mixed linear model analyses on score of different clinical outcome measures of participants in the Chinese calligraphy writing (experimental) and tablet computer training groups (control) for the baseline, post-training and six-month follow-up assessment occasions
DST-Backward, Digit Span Test (Backward); CTT, Color Trail Test; SDMT, Symbol-digit Modalities Test (Acc., Accuracy Rate; Correct, Correct Attempts; Total, Total Attempts); GDS, Geriatric Depression Scale. Statistical significance levels for post-hoc comparisons for DST-Backward and SDMT (Verbal) are *p≤0.025, CTT and CERAD-NAB are *p≤0.017; **p≤0.01; ***p≤0.001.
Treatment effects on attention
Significant improvements were observed in the experimental group in scores of CTT2 from baseline (Mean = 151.3 s) to post-training (Mean = 119.6 s) (p < 0.001, d = –0.439), which was not the case for the control group (p = 0.753, d = –0.043) (Fig. 3). The improvement trend was also observed in the scores on the CTT2-CTT1 for the experimental group (p < 0.01). For the long-lasting effects, participants in the experimental group maintained the significant improvements in the scores of CTT2 at the follow-up (Mean = 132.5 s) (p = 0.014, d = –0.291), which was not the case for the control group (p = 0.484, d = –0.066).
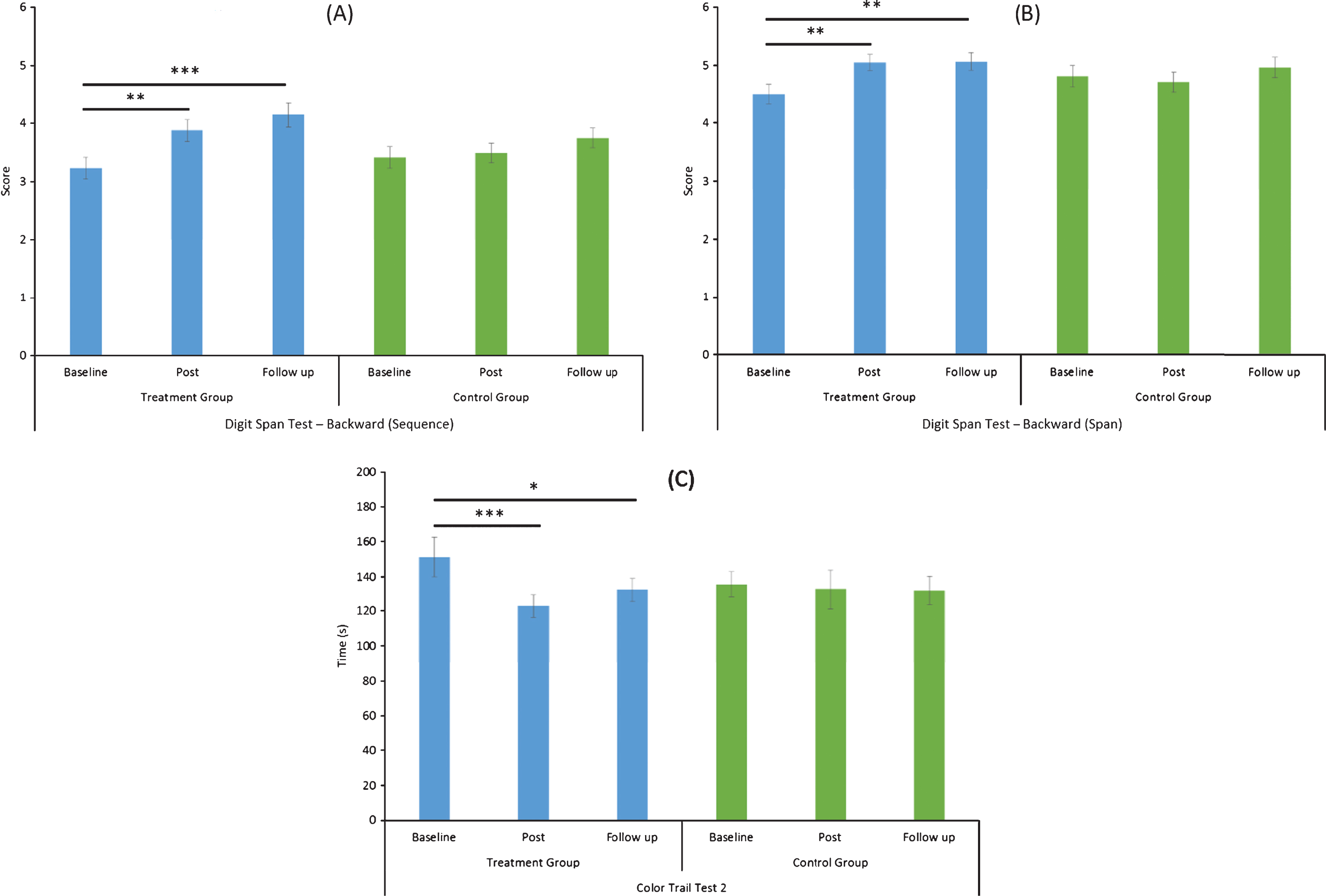
Within group comparisons on score of (A) Digit Span Test – Backward (Sequence), (B) Digit Span Test – Backward (Span), and (C) Color Trail Test 2 for the baseline, post-training and six-month follow up assessment occasions. Horizontal lines indicate significant post-hoc comparisons with paired t-tests (*p-value≤0.017; **p-value≤0.01; ***p-value≤0.001, two-tailed). Error bar =±1 standard error of mean.
Treatment effects on working memory
Significant increases were observed in the experimental group in the mean sequence score on the DST-Backward from the baseline (Mean = 3.2) to post-training (Mean = 3.9) (p = 0.002, d = 0.498), as well as the mean span score from the baseline (Mean = 4.5) to post-training (Mean = 5.0) (p = 0.009, d = 0.499). In contrast, participants in the control group did not show significant differences between the two assessment occasions (sequence: p = 0.671, d = 0.063; span: p = 0.506, d = 0.091). Despite CERAD-NAB is measure of memory function, it is noteworthy that both the experimental (p < 0.001, d = 0.711) and control groups (p < 0.001, d = 0.829) showed significant increases in immediate recall (J4) after completing the training programs. Similarly, significant increases in scores on the word delay recall (J6) were observed in both experimental group (p < 0.001, d = 0.450) and control group (p < 0.001, d = 0.514).
For the long-lasting effects, participants in the experimental group showed sustained significant increases in the mean sequence score of the DST-Backward at follow-up (Mean = 4.2) (p < 0.001, d = 0.665) and in the mean span score of DST-Backward at the follow up (Mean = 5.1) (p = 0.008, d = 0.505), which were not observed in the control group (sequence: p = 0.104, d = 0.263; span: p = 0.298, d = 0.153).
The significant improvements in participants’ performances on the two CERAD subtests appeared to maintained regardless of the memberships. For the experimental group, the increases in the scores on J4 (from 19.2 to 22.6) (p < 0.001, d = 0.800) and J6 (from 6.6 to 7.8) (p < 0.001, d = 0.580) were comparable to those on J4 (from 19.1 to 22.9) (p < 0.001, d = 0.987) and J6 (from 6.8 to 7.7) (p < 0.001, d = 0.613) for the control group.
DISCUSSION
The results supported the hypothesis that the 8-week calligraphy training improved specific cognitive functions of the participants with MCI. The most significant finding was that the treatment effect had a moderate effect on augmenting working memory, and to a lesser extent attentional control function. A general effect of calligraphy training on improving verbal episodic memory was also observed which however was not differed from that of the computer training for the control group.
The Kai-to-Hang-styled character transformation process adopted in calligraphy writing training heavily involved attentional control and working memory. The improvements in the attentional control were reflected by the significant increases in the CTT2 and to some extent CTT2-CTT1 score of the CTT from baseline to post-training. CTT2 is a measure of divided attention while CTT2-CTT1 reflects attentional control [26]. Encoding of a Kai-style character and decomposing its strokes would tap on attentional control, while the Kai-to-Hang transformation would tap on divided attention. Our results are consistent with those reported by Kwok et al. [7], which showed that a piloted calligraphy writing protocol was beneficial for improving attention function of patients with MCI. It is however noteworthy that when individual with amnestic MCI (n = 9 based on CERAD-NAB J4 cut-off <15/30 [46]) were excluded from the analysis, the post-training effect on the CTT2 scores in the experimental group remained statistically significant (p < 0.001) but the long-lasting effect became marginally significant (p = 0.095). This suggested the possibility that the treatment effect of calligraphy writing training might have acted differently between the non-amnestic and amnestic MCI participants. As the number of amnestic MCI participants was rather small in this study (9 and 6 for experimental and control group, respectively) for justifying further sub-group analyses, future study should explore possible differential effects of the training on amnestic versus non-amnestic individuals.
Improvements in working memory of our participants were revealed by the significant increases in the sequence and span scores of the DST-Backward between baseline, and post-training and follow up occasions. The Kai-to-Hang transformation would demand working memory particularly visualize the Hang-styled strokes and the character before writing it with an ink brush. The treatment effects were found ranging from weak to moderate which were not modified by excluding the amnestic MCI participants from the analysis. Our results are somewhat different from those of Kwok et al. [7], which reported nonsignificant effects of the calligraphy therapy on improving memory function. This perhaps is because of their use of the Mini-Mental State Examination, which measures global cognitive function instead of specific memory function as outcome measure in their study. Rapp et al. [47] used memory strategy training and revealed nonsignificant effect on improving memory function among MCI participants. On the contrary, Rozzini et al. [43] demonstrated that computer-based memory training resulted in significant improvements in memory, attention, and visuospatial functions among the MCI participants. Cheng et al. [48] employed multi-domain cognitive training (includes mental games, map reading, handcraft making, and physical exercise), which was found to enhance memory function of community-dwelling non-demented individuals. Other studies employed cognitive training targeted on improving several cognitive components, resulting in improvements in global cognitive function [49, 50]. The results of this study suggest that calligraphy writing training can produce outcomes comparable to these activities.
It is noteworthy that both calligraphy writing training and tablet computer training (serving as control) exerted very strong effects on improving memory function. Both interventions were found to increase scores on J4 and J6 of the CERAD-NAB which measure immediate recall/encoding and delay recall functions, respectively. Nevertheless, the findings tended to suggest that calligraphy writing training was still effective for augmenting memory functions of the MCI participants. By the same token, tablet computer training may also be beneficial for the participants in terms of improving memory function.
Among different mind-and-body practices, calligraphy writing training in this study yielded smaller treatment effects on attentional control (weak to medium effect size) than Yoga for women with climacteric syndrome (medium to large effect size) [51]. Besides, these effects were comparable to other studies employing calligraphy therapy for improving concentration function among patients with nasopharyngeal carcinoma [23] but smaller than the effect sizes yielded in Kwok et al.’s [7] study on improving general cognitive function (large effect size). The improvements in the working memory and attentional control functions suggest the notion that calligraphy writing training is likely to induce plastic changes in brain of the MCI participants. Plausible plastic changes are evident from the significant long-lasting effects revealed in the calligraphy writing training group on working memory function. This proposition is supported by the findings that the brains of MCI participants were able to recruit new neural circuits under demanding cognitive tasks [52]. Future study can explore the training-related neural changes using brain imaging method.
There are limitations in our study. The participants recruited for this study had slightly higher cognitive ability than that stipulated in Gill et al. [35]. The mean MoCA score was around 24.5±3, so the majority of the participants fell within 21 to 27. This is higher than the referent 19 to 26 range. The results could have been different if the participants belonged to a group with lower cognitive ability. Participants in each of the experimental and control groups were mixed types, i.e., amnestic (smaller proportion) and non-amnestic MCI. These limit generalization of the results of this study to those who share similar characteristics. When compared with simple randomization, the use of block randomization method in this study could have introduced biases in assigning participants to the experimental and control groups. Future study should use simple randomization to avoid the potential biases. The final sample size of this study was smaller than that estimated at the beginning of the study. This may lower the power of the statistical analyses. Future study should test the treatment effect of calligraphy writing training with a larger sample size. The outcome measures used in this study might have biased the results, as the DST-Backward and CERAD-NAB did not require visual processing, which was heavily involved in the calligraphy writing. Use of outcome measures involving visual processing would yield results specific to the intervention. The cognitive approach adopted in this study to strengthen the Kai-to-Hang style transformation is different from that of previous studies. The results should be interpreted with caution and cannot be generalized to interventions that target at relaxation and emotional calmness by using Chinese calligraphy writing. Future study can extend the cognitive approach to calligraphy writing training and explore its effect on enhancing emotional adjustment in terms of changes in blood pressure and heart rate.
In conclusion, findings of this study support the positive effect of the eight-week Chinese calligraphy writing training on improving working memory and to a lesser extent attentional control of participants with early MCI. The possible treatment effects are likely to be attributable to the Kai-to-Hang style transformation process involving in writing the Hang-styled characters with an ink brush. Future research should test the treatment effect beyond an eight-week training duration. Study should be extended to home-based and self-paced training, which is a feasible and sustainable model for service provision.
Footnotes
ACKNOWLEDGMENTS
We would like to thank the organizations that participated in this study and their staff for providing the facilities for conducting the training. We are in debt to the older adults who completed the screening and/or the eight-week programs. This study was supported by the Health and Medical Research Fund [HMRF 09101331], Food and Health Bureau, and Hong Kong SAR Government.