
Abstract
Background:
Computerized Cognitive Training (CCT) has been shown to improve cognitive function in older adults with mild cognitive impairment (MCI) or mood-related neuropsychiatric symptoms (MrNPS), but many questions remain unresolved.
Objective:
To evaluate the extent to which CCT benefits older adults with both MCI and MrNPS, and its effects on meta-cognitive and non-cognitive outcomes, as well as establish whether adapting difficulty levels and tailoring to individuals’ profile is superior to generic training.
Methods:
Older adults with MCI (n = 9), MrNPS (n = 11), or both (MCI+, n = 25) were randomized into a home-based individually-tailored and adaptive CCT (n = 21) or an active control condition (AC; n = 23) in a double-blind design. Interventions lasted 8–12 weeks and outcomes were assessed after the intervention, and at a 3-month follow-up.
Results:
Participants in both conditions reported greater satisfaction with their everyday memory following intervention and at follow-up. However, participants in the CCT condition showed greater improvement on composite measures of memory, learning, and global cognition at follow-up. Participants with MrNPS in the CCT condition were also found to have improved mood at 3-month follow-up and reported using fewer memory strategies at the post-intervention and follow-up assessments. There was no evidence that participants with MCI+ were disadvantaged relative to the other diagnostic conditions. Finally, informant-rated caregiver burden declined at follow-up assessment in the CCT condition relative to the AC condition.
Conclusions:
Home-based CCT with adaptive difficulty and personal tailoring appears superior to more generic CCT in relation to both cognitive and non-cognitive outcomes. Mechanisms of treatment effect and future directions are discussed.
Keywords
INTRODUCTION
Evidence for a link between high educational attainment and a cognitively-engaged lifestyle with risk of dementia in older age has been consistently found in epidemiological [1] as well as post-mortem studies [2]. Reflecting this is an ever-increasing interest in the potential of cognition-oriented treatments (COTs), including cognitive stimulation and cognitive training, which may enhance such protective factors to prevent, delay, or alleviate symptoms associated with cognitive and functional decline in older people throughout the continuum of cognitive health through to dementia. Relative to pharmacological interventions, COTs are considered relatively free of adverse effects, and encourage a cognitively healthy and engaged lifestyle. Numerous studies have examined the effects of cognitive training (CT) in cognitively healthy older adults [3 –5], in persons with mild cognitive impairment (MCI) [6 , 7–9], and in persons with mild to moderate dementia [10 –12]. CT refers to the repeated guided practice on (usually standardized) cognitive tasks designed to train specific cognitive abilities. The objectives of CT are typically improvement or maintenance of underlying cognitive abilities [13, 14], through training of single [4 , 9] or multiple [15, 16] cognitive domains, with or without the use of cognitive strategies [17]. Technological advances in recent years have led to the development of computerized cognitive training (CCT) platforms, which have largely replaced traditional, pen-and-paper based training [18], and a large scale industry of commercially-available CCT products has emerged. The exact mechanisms through which CT may improve cognitive functioning are not well understood, but are thought to involve the enhancement of neurobiological processes that underpin cognitive function, including synaptic activity, long-term potentiation, and the activation of diverse neural networks [19, 20]. In recent years, evidence has begun to accumulate showing that CT and more general cognitive stimulation changes both brain structure [21, 22] and function [23 –25]. To facilitate changes in neurobiological processes, CT programs are increasingly designed against recognized learning principles, including adaptive difficulty level of trained tasks, tailoring of training to individuals’ cognitive profiles, and the provision of feedback on performance.
Nonetheless, there is little support to date for the benefits of CT in relation to cognitive or non-cognitive outcomes in people with mild-to-moderate dementia ([14], but see [26]). More encouraging findings have been reported, however, in relation to cognitive outcomes among cognitively healthy older adults [27, 28] and in those at risk of dementia due to MCI [17 , 30], or mood-related neuropsychiatric symptoms (MrNPS) [31]. Individuals with MCI are of particular interest in the context of dementia prevention and risk reduction trials, as the underlying etiology in many cases is Alzheimer’s disease pathology, vascular disease, or both, and approximately 5% –10% of MCI patients will meet criteria for dementia annually [32]. It is unsurprising that interventions, including cognition-oriented treatment approaches, have increasingly targeted individuals with MCI, in the hope that when commenced at this early stage, they may improve cognitive abilities and help preserve independence in daily activities, and hence prevent or delay the onset of dementia.
Importantly, despite the tentatively supportive evidence base for CCT in MCI [6 , 33], a range of theoretical and methodological problems confound the design and implementation of these interventions, and the interpretation of study findings is often restricted by lack of adherence to reporting guidelines, such as the CONSORT Extension for Non-Pharmacological Interventions [34], restricting the conclusions that can be drawn regarding the efficacy and benefits of CCT in older adults in general and in persons at risk of dementia due to MCI specifically [35, 36]. In particular, CT studies, and psychosocial interventions more broadly, often lack a clear theoretical rationale to support specific intervention design decisions. For example, the rationale for designing CCT to target single versus multiple cognitive domains is often not explicitly stated, and a clear specification of the postulated “active ingredients” of the intervention is often lacking. This is especially the case in non-pharmacological interventions which typically include a range of non-specific components. A related issue concerns the nature of the condition to which the CCT is being compared. Although CCT interventions are sometimes evaluated against passive control conditions (e.g., no treatment, waitlist, etc.) [37, 38], the majority of trials tend to use an active control condition to account for non-specific intervention effects [8, 9]. In practice, however, the components of the active control conditions are often only broadly described, and the precise ways in which they differ from the experimental conditions are often unclear. A further methodological issue concerns the frequent exclusive focus on cognitive outcomes (sometimes using single measures) withoutexamination of the effects of CCT on clinically-meaningful outcomes for the person trained and for their close others, including meta-cognition, mood, functional independence, and caregiver burden.
Furthermore, in addition to their cognitive deficits, individuals with MCI frequently experience concurrently MrNPS. MrNPS are very common in the older adult population [39] and are thought to be an independent predictor of cognitive decline and dementia [40, 41]. Relative to persons with MCI alone, those with MCI and concurrent MrNPS have been shown to have poorer outcomes, including an accelerated progression to dementia [42, 43]. The extent to which CCT may be of benefit to individuals with both MCI and MrNPS is, however, unknown, as many trials of CCT exclude individuals with significant mood-related NPS from participation (e.g., [9]). Some studies have examined the impact of a cognitive-behavioral treatment on mood symptoms in mild AD [44], and others examined the impact of CCT on depressed older adults without cognitive impairment [31], or on ‘help seekers’ referring to a memory clinic on the basis of cognitive and/or mood-related complaints [45], but to the best of our knowledge, no study has concurrently examined the impact of CCT on older adults at risk of dementia due to MCI, MrNPS, or both, to evaluate the unique and combined effect of cognitive and MrNPS on treatment response.
In the current trial, we evaluated the effects of a home-based, adaptive, and quasi individually-tailored multi-domain CCT intervention, relative to an active control intervention in older adults with MCI, MrNPS, or both. A multi-domain training approach was preferred over a single-domain one to maximize the likely overlap between trained cognitive domains and cognitive processes underpinning cognition in day-to-day activities [46], which in turn should increase the likelihood of generalization of training gains to everyday function. In addition, there is some evidence that multi-domain CT can lead to more sustainable performance gains relative to single-domain CT [47]. A home-based intervention was preferred over a clinic/university-based intervention to maximize convenience and flexibility for trial participants, and because this more closely mimics real-world lifestyle changes and would allow participants to maintain this type of training beyond the duration of the trial. However, relative to clinic/university-based interventions carried out with the direct involvement of a clinician, home-based interventions are associated with poorer adherence and higher discontinuation rates [5]. To support maintained engagement, we augmented the intervention with behavior-change techniques (BCTs), drawn from a published taxonomy of BCTs [48], and the associated Theoretical Domains Framework [49]. The experimental and control interventions were evaluated against both cognitive and non-cognitive outcomes, immediately post-intervention and at a 12-week follow-up. Our primary aim was to evaluate the impact of the CCT intervention on a composite measure of global cognitive ability immediately (i.e., within 2 weeks) following the intervention. Secondary aims included the evaluation of maintenance of the benefits of CCT on global cognition three months post intervention, as well as the benefits of CCT in relation to a range of domain-specific cognitive abilities and non-cognitive outcomes (meta-memory, mood, and independent activities of daily living for the participant, and caregiver burden) immediately after the intervention and at a three months follow-up. Finally, we explored whether differences were evident in the extent to which older adults with MCI, MrNPS, or both, benefit from the intervention. The trial is reported in accordance with the CONSORT Extension for Non-Pharmacological Trials [50] (See checklist in the Supplementary Materials).
MATERIALS AND METHODS
Setting, design, and sample size calculations
The Canberra Computerised Cognitive Training Trial (CCCT Trial) was a double-blind randomized controlled trial completed in Canberra, Australia. Older adult participants preliminarily classified upon screening as having MCI, mood-related neuropsychiatric symptoms (MrNPS), or comorbid MCI and MrNPS (MCI+), were subsequently randomly assigned either to a tailored and adaptive CCT condition, or to an active control (AC) condition, as further described below.
Sample size calculations were completed using G-Power software (G-Power, V3.0). To detect a medium-sized effect for the impact of CCT on change in global cognitive ability of older adults with MCI immediately post-intervention, in a two-group, experimental versus active control randomized design, with the probability of making Type I error set at 0.05, and power set at 0.90, a total sample of n = 50 is required. Our effect estimation was based on the medium-sized effect (d = 0.33) of CCT on the main cognitive outcome found by Barnes and colleagues [7] in a similar trial design, with 22/25 participants per intervention arm. The trial was approved by the Human Research Ethics Committee at the Australian National University (Protocol 2013/589), was first submitted for registration with the Australian-New-Zealand Clinical Trial Registry (ANZCTR) on the 20/11/2013, and retrospectively registered on the 27/3/2014 (ACTRN12614000335695, https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=365222), approximately 6 weeks following the enrolment of the first participant (3/2/2014).
Participants and screening
Older adults (age >65) with self-reported memory difficulties, mood-related symptoms, or both, and who resided in the Australian Capital Territory or surrounding areas within the adjoining state of New South Wales (Australia), were invited to undergo screening for participation in the study. Participants were recruited through interviews in the local media (radio, TV), from a local memory clinic, and by word-of-mouth. A preliminary self-screening procedure was used to further verify that participants were fluent in English, had home access to a computer and internet connection, were able to nominate a close-other (e.g., relative, spouse, or close friend) who was prepared to complete several questionnaires at all assessment occasions, and were able to commit to between 8 and 12 weeks of training. The following criteria, based on self-report, led to exclusion from the study: existing diagnosis of dementia or other major neurological or psychiatric condition (not including depression or anxiety) likely to affect cognition, significant sensory or perceptual impairments likely to affect assessment or training, fewer than 6 years of formal education, previous participation in a cognitive training study, or a newly-prescribed (<3 months) mood- or cognition-stabilizing medication.
Participants who satisfied the basic eligibility criteria were invited to undergo further screening to confirm the presence of MCI, MrNPS, or both. The diagnosis of MCI was made using the National Institute on Aging-Alzheimer’s Association (NIA-AA) clinical criteria [50]. Specifically, a concern needed to have been expressed by either the participant, their spouse or a referring clinician regarding the participant’s cognitive function. Objective evidence of cognitive deficits in at least one (for clinician-referred participants) or two (for communitydwelling self-referred participants) cognitive domains was determined on the basis of the standardized neuropsychological evaluation described below. The criteria for self-referred individuals were slightly more stringent as the likelihood of performance being impaired on at least one test is high even among cognitively healthy older adults due to factors including fatigue, attentional fluctuation, or features of a specific test. In comparison clinician-referred individuals had already been identified as having MCI on the basis of clinical judgement which typically incorporated broader historical and contextual details into the clinical evaluation. Cognitive impairment was defined as a task-score falling at least 1.5SDs below an appropriate age and education adjusted normative mean. Preservation of functional independence was verified on the basis of scores on the informant-rated Bristol Activities of Daily Living Scale (BADL) [51], with scores >8, suggesting some compromise to functional independence, leading to exclusion from the study.
The presence of MrNPS was determined on the basis of informant rating on the Neuropsychiatric Inventory Questionnaire (NPI-Q) [52]. Participants with a minimum of one symptom rated to be of at least moderate severity in one of the following symptom domains met the MrNPS criterion: depression, anxiety, apathy, and irritability. Endorsement of any symptoms belonging to the psychosis spectrum (delusions and hallucinations) led to exclusion from the study. The preference for using an informant-rated over self-rated mood scale was largely driven by the need to exclude those individuals presenting with symptoms on the psychotic spectrum, and the assumption that these may be less likely to be detected on the basis of self-report.
Assessments
Face-to-face assessments, conducted by trained provisional psychologists (SW, HB) were completed at baseline (T0), upon completion of the intervention (T1), and at three months after completion of the training period (T2). All assessments were completed one-on-one with a trained examiner. All three assessments were identical, with the exception that the baseline assessment also included administration of the Addenbrooke Cognitive Evaluation, Third Edition (ACE-III) [53], as part of the screening procedure for cognitive impairment. The assessment included a battery of well-established and commonly used cognitive measures sensitive to a range of cognitive domains and a range of self and-informant-rated questionnaires covering the domains of memory awareness/meta-memory, mood and well-being, independence in day-to-activities, and caregiver burden. The complete set of assessment measures, the sub-tests administered/indices derived, and the composite scores towards which measures contributed is shown in Table 1. More detailed information regarding the assessment battery, including the cognitive domains covered by each measure, the full reference, and the source of the norms used (where applicable) are shown in Supplementary Table 1.
Assessment measures included in the evaluations
ACE-III, Addenbrooke Cognitive Examination, Third Edition; SydBat, Sydney Language Battery; RAVLT, Rey Auditory Verbal Learning Test; RCFT, Rey Complex Figure Test; MARS, Memory Awareness Rating Scale; MMQ, Meta Memory Questionnaire; CDR, Clinical Dementia Rating; GDS, Geriatric Depression Scale; GAI, Geriatric Anxiety Scale; AES, Apathy Evaluation Scale; NPI-Q, Neuropsychiatric Inventory-Questionnaire; ZBI, Zarit Burden Interview; BADL, Brixton Activities of Daily Living. *ACE-III was only administered during the screening portion of the baseline assessment, and not at the post-training or follow-up assessment sessions.
Blinding and randomization
Following the baseline assessment and confirmation of eligibility, participants were randomized, stratified by baseline diagnostic classification (MCI, NPS, MCI+NPS) into the experimental and control conditions described below. Randomization sequences were produced by a computer (http://www.randomizer.org) and were concealed from study personnel by a researcher unrelated to the study who provided the group allocation for each participant upon request from the principal investigator. Participants were unaware of their group allocation and were told that they would be allocated to one of two versions of the training program which differed in some aspects. Participants were not told of any specific hypothesis associated with any of the training versions, and were therefore unlikely to be able to guess the condition to which they were allocated. In addition, research staff completing the post-intervention and follow-up assessments were blind to intervention conditions. Finally, the researcher assigned to orient participants to their intervention and provide support throughout the intervention period was unaware of participants’ baseline diagnostic groupclassification.
Interventions
Both the experimental (CCT) and active control (AC) conditions received complex, multi-domain interventions involving repeated practice on standardized, game-like computer tasks, psychoeducation, and a range of behavior-change techniques used to optimize engagement, adherence, and perseverance. Table 2 summarizes all intervention components included in the experimental and control conditions and the way in which these components were operationalized. Both groups trained on a commercially-available computerized cognitive training platform (CogniFit™), which has been used in several previous studies involving various populations, including persons with insomnia [54], dyslexia [55], multiple sclerosis [56], unipolar and bipolar disorders [57], and healthy older adults [58, 59]. The behavioral components of the interventions (further described below) were largely developed in a bottom-up fashion with reference to the taxonomy of BCT and theoretical domains framework outlined by Michie and colleagues [49, 60].
Description of the intervention components included for the adaptive training and active control groups
Experimental condition
The CogniFit General Training program consisted of 33 tasks designed to train a broad range of cognitive abilities. A list of all 33 tasks and the cognitive domains they were designed to target appears in Supplementary Table 2. In the first session, CogniFit performs a baseline cognitive evaluation which is composed of 15 assessment tasks (different from the 33 tasks used for training), yielding 17 domain-specific scores and a global cognitive score. The score obtained on this baseline evaluation is then used by the program to assign participants at each session to training tasks based on their pattern of cognitive strengths and weaknesses. The methodology by which CogniFit calculates cognitive scores and tailors training tasks according to individual cognitive profiles has been described previously [57, 59]. In addition, the level of difficulty of tasks was continuously adapted on the basis of the participant’s performance, with successful completion of one level of difficulty resulting in an increased difficulty on the subsequent trial.
CogniFit training sessions involve the completion of three tasks, delivered by the program in one block, and participants were instructed to complete two-sessions (i.e., six tasks) on each day they trained. At the end of each block of three tasks, participants in the experimental condition received feedback about their performance in the form of a score that they could track as the training progressed.
Active control
Participants in the Active Control (AC) also trained on the CogniFit platform, underwent the same baseline cognitive assessment included in the first training session, and trained on the same 33 training tasks as participants in the experimental condition. Unlike participants in the experimental condition, however, training task allocation was not tailored to their cognitive profile. Instead, participants were provided with a pre-determined randomly generated schedule of tasks, which ensured that all tasks were presented a similar number of times. In addition, across training sessions, difficulty level of tasks remained stable, such that participants would always commence a task from the same difficulty level, even if they have improved in their performance. Finally, participants in the AC condition did not receive feedback on their performance at the end of each training session.
Other training components and materials
A range of techniques, adapted from behavior-change framework described by Michie and colleagues [60], were used to ensure close matching of the experimental and control conditions on all but the postulated ‘active ingredients’ of the CCT intervention, and to optimize intervention adherence and compliance. As can be seen in Table 2, a wide range of techniques was employed throughout the intervention period. A detailed intervention manual/instruction booklet, participant diary, and weekly phone call were all used to implement these BCTs, as described in Table 2. The complete manualized protocol is available from the authors on request.
Training dose
Very little evidence exists to support decisions regarding frequency and duration of cognitive training trials, and dose-response relationships have not been systematically studied in relation to this type of intervention. In making dose-related decisions, researchers need to balance scientific and pragmatic considerations, and in most trials in this area,participants have trained between 6 and 12 weeks. In the meta-analysis by Lampit and colleagues [61], the authors found that training more than 3 times a week was no more effective than training 2-3 times per week. Based on our own experience in an RCT of a home-based educational dementia risk reduction intervention [62], we asked participants to complete 2 training sessions a day (together lasting approx. 20–30 min), 3 days a week, for a minimum of 8 weeks and a maximum of 12 weeks, allowing us to perform some exploratory analyses concerning ‘dose-response relationships’.
Procedure
Following baseline assessment and allocation to an intervention condition, participants and their informants were visited in their homes by a research assistant who provided an orientation to the CogniFit Program, including a range of behavior change techniques, as specified in Table 2. In brief, the researcher assisted the participants in accessing their CogniFit accounts for the first time, and guided them through the completion of the CogniFit baseline cognitive evaluation, providing practical assistance with task instructions as required. During these sessions, participants were also provided with a participant diary in which the goal setting and behavioral contract (their commitment to train) components of the intervention were recorded. Participants were shown how to use the diary supplied to monitor and record their training sessions, as well as their mood prior to each training session.
Each participant received a Participant Booklet during the orientation session. The booklet contained basic background information on the study and training requirements, suggestions for setting up the training environment according to ergonomic principles, and instructions for logging onto the prescribed CogniFit training website, and beginning and finishing a training session on the website (including screen-shots). While the section outlining how to use the CogniFit™ website differed between the groups (due to minor differences in the appearance of the training platforms for the CCT and AC conditions), all other sections of the booklet were kept identical between groups.
Primary and secondary outcomes
Our primary outcome was change in global cognitive ability immediately following the intervention, relative to the baseline evaluation. Global cognitive ability was measured in terms of scores on a composite measure derived from all the cognitive measures included in the assessment (described below). A range of secondary cognitive and non-cognitive outcomes was explored. Secondary cognitive outcomes included change in global cognitive ability at the 12-week follow-up assessment and change in domain-specific cognitive abilities immediately after the intervention and at the 12-week follow up assessment. We also examined change in self-reported memory functioning (contentment, mistakes, and strategy use), awareness of memory deficits (based on discrepancy scores on the self and informant versions of the MARS), mood (self-rated symptoms of depression and anxiety, and informant-rated symptoms of apathy), and independence in activities of daily living (based on informant ratings), and caregiver burden.
Statistical analyses
Analyses were conducted using IBM SPSS Statistics (V.22) and Stata (StataCorp, Texas, USA, V.13). Data preparation included the inspection of data for completeness, outliers, and variable distributions.
Scores on all cognitive measures except the ACE-III, Syd-Bat, and Sniffin Sticks were converted to Z scores using age and, where available, education and gender corrected norms (See Supplementary Table 1 for details). In addition, when more than one score was derived from a test (e.g., immediate and delayed recall measures), a total score for that test was derived by computing the average Z score of all indices from that test. The Global cognitive score was the mean of the Z scores of all cognitive measures. A composite Delayed Memory score was computed as the mean Z score of the delayed recall trials of the Logical Memory, RAVLT, and RCFT tests. A composite Learning and Memory score was computed as the mean Z score of the total score of each memory test. Finally, a Non-Memory composite score was calculated from the following measures: RCFT (copy), Phonetic, semantic, and switching fluency, digit-span, digit-symbol coding, and trail-making A+B. Scores on the self-reported (GDS, GAI) and informant-reported (AES) mood scales were also converted into Z scores against the baseline mean and SD of the MCI-only group (in which no mood symptoms were reported on the NPI at study entry). A composite mood score was then computed from the mean Z score of each of the three scales. Memory Functioning Discrepancy scores (MFS) were calculated from the self and informant rating on the MARS, using the procedure described by the scale authors [63]. Scores close to zero reflect good agreement between the participant and the informant regarding memory functioning, whereas positive and negative scores reflect an overestimation and an underestimation on behalf of the participant, respectively. Raw scores were used in the analyses of all other measures.
All analyses were completed using an intention to treat (ITT) approach. Baseline characteristics of the two intervention conditions and three diagnostic groups were compared using Analysis of Variance for continuous variables and Chi-Square tests for categorical variables. Due to participant discontinuation, and to the fact that central assumptions of the General Linear Model (uncorrelated observations, homogeneity of variance) are typically not met in the context of repeated measurements in a clinical trial, we used Linear Mixed Models (LMM) to model the association between predictors and each of primary and secondary outcome variables. The followingspecifications were used in all fitted models:
In relation to each outcome measure of interest, we compared the fit statistics (Bayesian Information Criterion, BIC) of three primary models. The basic model included the fixed main effects of intervention condition (CCT versus AC; reference condition), baseline diagnostic group (MCI, NPS, MCI+; reference group), and we compared basic models in which assessment occasion was specified as a fixed effect (T0; reference occasion, T1, T2) with models in which it was specified as having a random slope. The second model included the above terms (with assessment occasion as a fixed effect), as well as the two-way interactions (between occasion and intervention condition, occasion and diagnostic group, diagnostic group and intervention condition). Finally, the third model included all the above, as well as the three-way interaction between assessment occasion, intervention condition, and diagnostic group. Participants were specified as having random intercepts in all models. Model parameters were estimated using Restricted Maximum Likelihood Method, and an Unstructured Covariance was specified to model the covariance structure of both the residuals and the random factors. Following the rule of thumb provided by Seltman [64], a reduction of greater than 2 points in the BIC was generally considered a relative improvement in the model and used as the basis for model selection. When change in BIC was not useful in model selection, model simplicity and significance of estimates were used as the basis for modelselection. In relation to each outcome measure, only the selected model is presented in the results.
For each of the primary and secondary outcomes, Effect sizes (ES) were calculated as the standardized group differences in change scores between baseline and post-intervention assessment, as well as between baseline and follow-up assessments (Cohen’s d). For the composite cognitive scores, we also computed for each participant the difference in composite scores between the baseline and post-intervention assessments, and between the baseline and follow-up assessments, and then compared the relative risk (RR) with an improvement of 0.5SD as the ‘clinically meaningful’ criterion.
RESULTS
Recruitment, retention, and intervention adherence
Participant recruitment took place between February and November 2014. Flow through the study is depicted in the CONSORT Flow Chart in Fig. 1. A total of 188 persons expressed interest (females = 119), of whom 88 met basic criteria based on self-screening and proceeded to undergo full screening. Of these, 76 underwent full baseline assessment (described below), and 45 were found eligible for inclusion (MCI = 8, MCI+MrNPS = 25, MrNPS = 12).
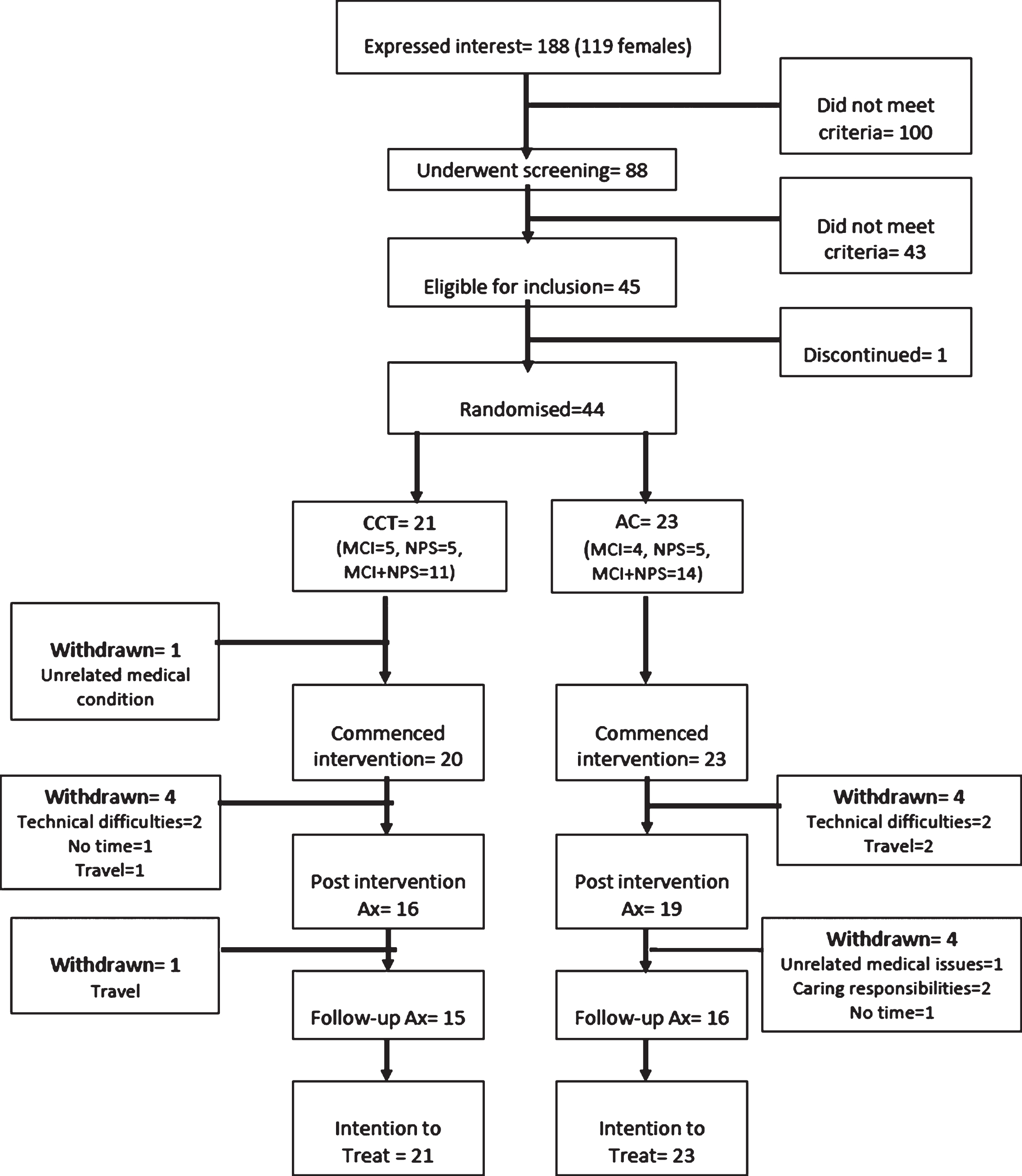
CONSORT flow chart for the CCT in MCI and NPS trial.
Of the 45 participants who underwent the baseline assessment, two participants withdrew before and immediately after randomization, and 43 commenced the intervention (CCT = 20, AC = 23). Following the intervention, 80% (n = 16) of CCT participants and 78% (n = 18) of AC participants returned for an evaluation, whereas 75% (n = 15) of the CCT and 67% (n = 16) of the AC participants returned for the three-month follow-up assessment. No adverse events were recorded that may have contributed to the drop-out rate. Participants in the CCT group trained for an average of 48.6 sessions (SE = 7.05, range: 1–118). Among CCT participants, 18 (90%) completed at least 20% of the minimum prescribed intervention dose (9 sessions), 15 (75%) completed at least 50% of the minimum prescribed dose (24 sessions), and 13 (65%) completed 80% of the minimum prescribed dose (38 sessions). When examining adherence only among CCT participants who were retained at the post-intervention assessment (n = 16), these figures were 16 (100%), 15 (93.8%), and 13 (81.3%) for 20%, 50%, and 80% of the minimum prescribed dose, respectively. For participants in the AC condition, adherence data was only available from their self-recorded data in participant diaries, and from the 10 diaries returned by participants at the post-intervention assessment, adherence at 80% of the minimum prescribed intervention dose was 100%.
Participants who completed at least 80% of the minimum prescribed intervention were more likely to return for post-intervention, χ 2(1) = 15.16, p < 0.001, and follow up χ 2 (1) = 15.09, p < 0.001 assessments. No statistically-significant differences were found between participants who did and did not complete the follow-up assessment on any demographic, cognitive, or functional measure, although a trend suggested that non-completers rated themselves as making fewer day-to-day memory mistakes at baseline than those who completed the study, t(43) = –1.83, p = 0.07. Of those who did not complete the study, 61.5% were assigned to the active control condition, and 33.3% of control participants did not complete the study (versus 25% among those assigned to the CCT group).
Baseline demographic characteristics for the intervention conditions (CCT, AC) and diagnostic groups (MCI, MrNPS, MCI+), and mean scores (SDs, range) on all outcome measures at the three assessment occasions are shown in Tables 3 and 4. No differences were found at baseline between intervention conditions on any of the demographic or outcome measures. Participants with MrNPS alone were less impaired at baseline on all composite cognitive scores than participants in both the MCI (all ps but the composite learning score <0.05) and the MCI+ group (all ps < 0.001). These participants had also resided in Australia for a shorter time, relative to participants with MCI+ (p < 0.01). Participants with MCI, however, rated themselves as more content with their memory functioning than both participants with MrNPS (p = 0.05) and participants with MCI+ (p < 0.01), and had lower scores on the composite mood score than participants in both the MrNPS group (p < 0.01) and participants in the MCI+ group (p = 0.02), and their informants reported lower caregiver burden scores relative to those with MrNPS (p = 0.05).
Cognitive outcomes
In relation to each cognitive and mood-related outcome measure, Table 5 shows estimates and standard errors (SE) associated with fixed and random effects. Figure 2 shows a panel of cognitive outcomes by assessment occasion, intervention condition, and diagnostic group.
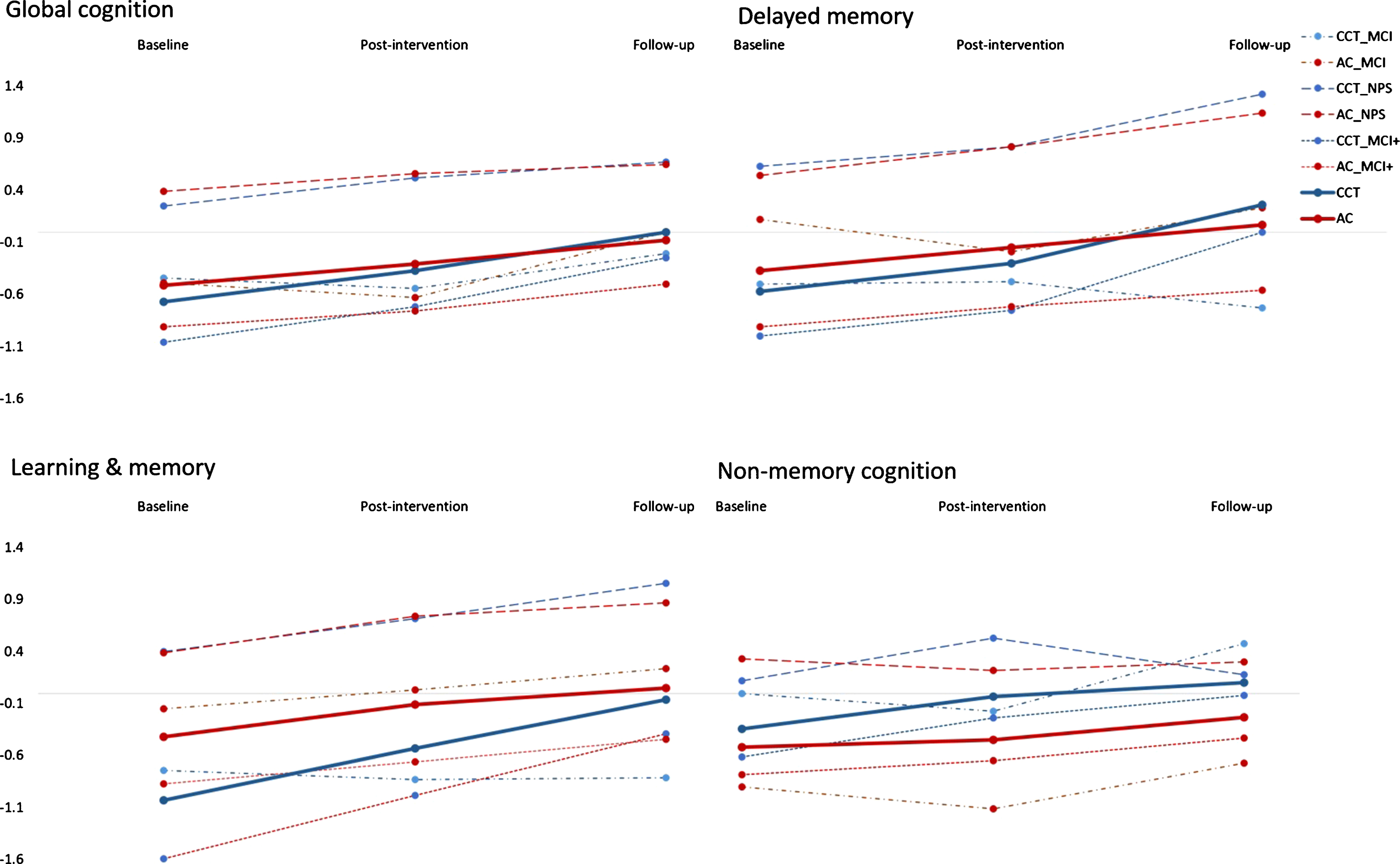
Cognition panel showing composite cognitive scores by Time, Intervention Condition, and Diagnostic Group.
Demographic and baseline characteristics
aDifferent from the MCI+NPS group at p < 0.01; bDifferent from the both the MrNPS and the MCI+ groups at p < 0.01; GDS, Geriatric Depression Scale. No significant differences found between intervention and diagnostic groups on any measure. As one participant withdrew prior to being randomized, the combined CCT and AC groups had 44 rather than 45 participants.
Means (SD), and range of scores on all outcome measures at the three assessment visits, by intervention condition, and baseline diagnostic group
Linear Mixed Model Fixed and random effects and estimates –cognitive and mood outcomes
* p < 0.05, ** p < 0.01, *** p < 0.001.
Global cognitive ability
Assessment occasion was associated with global cognition, with scores at the follow-up (T2) assessment being significantly better than at baseline (T0), t(63) = 2.21, p = 0.03. Global cognition was also associated with diagnostic group; participants with MrNPS alone performed better overall than participants with MCI+, t(37) = 5.5, p < 0.01. Finally, the interaction between assessment occasion and intervention condition was also significant; relative to the baseline assessment, participants in the CCT condition showed greater improvement at the follow-up assessment, t(62) = 2.5, p = 0.01.
Delayed memory
Assessment occasion, diagnostic group, and the interaction between occasion and intervention condition all had a significant effect on the composite delayed memory score. Relative to baseline (T0), scores at the follow-up assessment (T2) were higher, t(61) = 1.94, p = 0.05, participants with MrNPS scored overall better than participants with MCI+, t(42) = 3.33, p < 0.01, and improvement over time was greater in the CCT condition at the follow-upassessment, t(60) = 3.04, p < 0.01.
Learning and memory
Assessment occasion, diagnostic group, and the interaction between occasion and intervention condition all had a significant effect on the composite delayed memory score. Relative to baseline (T0), scores at the follow-up assessment (T2) were higher, t(57) = 1.93, p = 0.05, participants with MrNPS overall scored better than participants with MCI+, t(41) = 2.93, p < 0.01, and improvement over time was greater in the CCT condition at the follow-upassessment, t(57) = 2.79, p < 0.01.
Non-memory composite
Assessment occasion, intervention condition, diagnostic group, and the interaction between occasion and intervention condition all had a significant effect on the composite non-memory score. A trend suggested that relative to baseline, performance on the non-memory composite improved by the follow-up assessment, t(58) = 1.8, p = 0.06. Participants with MrNPS scored overall better than participants with MCI+, t(41) = 4.4, p < 0.01, and improvement over time was greater in the CCT condition at the post-intervention assessment, t(57) = 2.5, p < 0.01. In addition, scores of participants with MrNPS declined more rapidly by the follow-up assessments, relative to participants with MCI+, t(56) = –2.10, p = 0.04.
Mood outcomes
A non-significant trend suggested that participants with MrNPS-only had lower overall mood than participants with MCI, t(59) = –1.7, p = 0.08. None of the two-way interactions were found to be significant, but a three-way interaction was found suggesting an improvement in mood scores involving MrNPS–only participants in the CCT condition at the post-intervention assessment, t(57) = 2.21, p = 0.03. The results of the Linear Mixed Models of scores on individual mood measures can be seen in Table 5. The three-way interaction shows that participants with MrNPS in the CCT condition reported fewer depression symptoms immediately following the intervention, but by the time of the follow up assessment, their informants reported greater apathy, as did the informants of participants with MCI-only.
Meta-memory outcomes
Linear Mixed Model Fixed and random effects and estimates –Meta memory and care burden
MFD, Memory Functioning Discrepancy.
Activities of daily living and caregiver burden
Overall, participants were found to have slightly reduced independence in ADLs by the follow-up assessment, t(60) = 4.0, p < 0.01. However, a trend was found suggesting an improvement in activities of daily living (as reflected in the informant-rated BADL) among participants in the CCT condition at the follow up assessment, t(60) = –1.8, p = 0.07. Improved independence in ADLs was also reported for participants with MrNPS-only at the follow-up assessment, t(59) = –2, p = 0.05.
Concerning care burden, an occasion-by-intervention condition interaction was found, and examination of the estimates suggested that, relative to participants in the AC condition, there was a greater reduction in caregiver burden ratings by caregivers of participants in the CCT condition, t(53) = –2.3, p = 0.02. Interestingly however,examination of the three-way interaction suggested that within the CCT condition, caregiver burden of participants with MrNPS only was rated as greater, at the follow-up assessment, t(51) = 2.0, p = 0.05, with a similar trend observed at the post-intervention assessment, t(52) = 1.8, p = 0.07.
Effect sizes (Cohen d, and relative risk) associated with each outcome measure at in post-intervention, and at follow-up
Table 7 shows effect sizes associated with outcome measures at the post-intervention and follow-up assessments (relative to the baseline assessment). For all outcome measures, Cohen’s d statistic for the standardized mean difference in change scores is displayed, along with the Standard Error (SE) of the estimate and the 95% confidence interval. Estimates corresponding to medium (0.5–0.75) and large (>0.76) effect sizes appear in bold. For the cognitive outcome measures (composite cognitive scores), relative risk values, representing the likelihood that a score would improve by at least 0.5SD in CCT versus AC participants are also displayed. As can be seen, the CCT condition was associated with a large treatment effect for global cognition immediately post-intervention, and for global cognition, delayed memory and learning and memory scores at the 3 month follow-up assessment. The CCT condition was also associated with a medium treatment effect for learning and memory scores immediately following the intervention and for the composite non-memory score 3 months following the intervention. The probability of the global cognitive score improving by at least 0.5SD was 7.4 times greater for participants in the CCT condition immediately post-intervention, and 3.1 times greater at the 3-month follow-up assessment. In addition, immediately following the intervention, the relative probability for improvement in the non-memory composite score could not be calculated as the AC condition had no such cases, whereas 5 of 16 (31%) of participants in the CCT condition showed an improvement of at least this magnitude.
Effect Size, with SE and 95% confidence intervals associated with each outcome measure at Post-intervention and follow-up assessment. Relative Risk (RR) included for cognitive outcomes only
Effect size sign reversed for ease of interpretation. Positive effect size favors the CCT condition. *Relative Risk could not be calculated as the probability of improvement in the AC condition was 0.
Associations between total training time (TTT), demographics, baseline, and outcome measures (in the CCT group only)
No relationship was found between total training time (TTT; number of training sessions completed, based on data automatically generated by CogniFit) and selected demographic or outcome measures at baseline. TTT was positively associated with theCogniFit total score at the end of the training (r = 0.61, p < 0.01), as well as with the non-memory composite score (r = 0.50, p = 0.04). The association between TTT and the non-memory composite score at follow up also approached significance (r = 0.49, p = 0.06). No other significant associations were found. None of these relationships reached significance when baseline scores on the non-memory composite were controlled, although the association with the final CogniFit assessment scores was not as affected (r = 0.47) as the associations with the non-memory composite score at the post-intervention (r = 0.21) and follow-up assessments (r = 0.36).
DISCUSSION
Summary of findings
The current study extends the existing body of knowledge in demonstrating cognitive and selected non-cognitive benefits associated with a home-based, quasi-tailored. and adaptive CCT, targeting older adults with cognitive impairment, mood-related symptoms, or both, over and beyond the benefits of a non-adaptive/non-tailored active control training condition. Relative to participants in the AC condition, those in the CCT condition showed improved performance on the non-memory composite cognitive measure immediately following the intervention period. The effects of the CCT intervention on performance in other cognitive domains were not statistically apparent immediately following the8-12-week intervention, but were clearly detectable by the follow-up assessment, three months following the conclusion of training. Specifically, at the three-month follow-up, participants in the CCT condition showed a greater improvement in their performance on composite measures of global cognition, learning, and delayed episodic memory, relative to the active control condition.
Importantly, while some trials of CCT targeting older adults with MCI have reported maintenance of gains in performance during a follow-up assessment [8], the current study supports the finding from other recent studies (e.g., [65]) that found that training-related gains in persons with MCI may actually be further consolidated over the course of three months following the conclusion of the formal intervention period. While the possible mechanisms accounting for this continued improvement are yet to be elucidated, these findings, if replicated, have implications for the common accounts according to which training-related cognitive gains rapidly decay following the cessation of training [66]. Of note, Cheng and colleagues, in a study focused on healthy older adults, found that multi-domain CCT, such as the one used in the current study (but with a different program), was associated with long term improvement in cognitive test scores (over 12 months) relative to single-domain training [47].
Examination of the Cohen’s d effect sizes (Table 7) supports and extends the findings from the Linear Mixed Models analyses, showing large effect sizes at the follow-up assessments in relation to the learning, delayed memory, and global cognitive composites, as well as showing a medium effect size for the non-memory composite. In addition, immediately following the intervention, the learning and global cognitive composites showed a medium and large effect size, respectively. When examining the proportion of participants in each intervention condition who showed improvement in their performance on a cognitive composite (defined as an improvement of at least 0.5SDs relative to the baseline evaluation), the relative “risk” (RR) of improvement was found to be RR = 7.4 for global cognition in favor of the CCT condition post intervention, and RR = 3 in favor of the CCT condition at the follow-up assessment. Hence, while at the group level, improvements on global cognitive scores were more pronounced for the CCT condition at the follow-up assessment, the RR statistics clearly show that the CCT conditions was associated with a greater number of “responders” immediately following the intervention.
No training-specific effect was found in relation to self-reported memory functioning. Instead, participants in both intervention conditions reported greater contentment with their memory functioning at the post-intervention and follow-up assessments relative to the baseline evaluation. Across intervention conditions and diagnostic groups, by the follow-up assessment participants were rated to have a modest decline in their independence in activities of daily living, however, informant-reported burden of care had decreased only among participants in the CCT condition at the follow-up assessment.
Across time and intervention groups, participants with mood-related neuropsychiatric symptoms (MrNPS) outperformed participants with MCI+ MrNPS on all cognitive composites. Although baseline comparisons of cognitive functioning between MCI participants with and without MrNPS failed to reach significance, examination of effect sizes (approx. d = 0.5) suggest that this was mainly due to the small sample size (data not shown). These effect sizes, favoring participants with MCI alone, are in keeping with the ones reported in others studies [67]. No evidence was found in the current study however of a three-way interaction between intervention condition, diagnostic group, and assessment occasion, tentatively suggesting that participants with MCI+ MrNPS are not disadvantaged relative to participants with MCI-only when undertaking a home-based CCT program.
Across intervention conditions and assessment occasions, participants with MCI-only reported greater contentment and less frequent memory mistakes relative to participants with MrNPS, or MCI+ MrNPS. Interestingly, participants with MrNPS-only in the CCT condition, reported less frequent use of memory strategies at both the post-intervention and follow-up assessments. These same participants tended to underrate their memory performance relative to their informant, at the follow-up assessment. No intervention-specific effects on mood were found when considering all diagnostic groups, however, our findings tentatively suggest that participants with MrNPS-only in the CCT condition showed improved mood (including fewer depressive symptoms) at the post-intervention evaluation, as reflected in thecomposite mood score.
Possible mechanisms of intervention effects
Understanding the cognitive, behavioral, and neurobiological mechanisms through which training-related cognitive improvements occur is key to efforts to design effective cognition-focused interventions grounded in solid scientific principles. A comprehensive discussion of the micro and macro neurobiological mechanisms that have been implicated in training-related cognitive improvements is beyond the scope of this paper, but relevant reviews are available [68, 69]. Briefly, training-related cognitive improvements are commonly believed to be the result of neuroplastic changes at the synaptic level, as well as at the level of brain structure and function. Arguably, the adaptive difficulty level and personal adaptation of task allocation to target relative cognitive weaknesses act as further enablers of these neuroplastic processes. Cognitive mechanisms that account for improved test performance may involve more rapid information processing speed and more cost-effective, consistent, and spontaneous use of cognitive strategies and principles. At the behavioral level, the systematic use of BCTs in this study, drawn from a published taxonomy [70], may have contributed to the development and maintenance of motivation and capability (including self-efficacy). While these behavioral determinants are likely to play a role in adherence to the treatment protocol and in maintaining behavior, it is not possible to say at this point whether these determinants have a direct impact on cognitive and other outcomes, but this needs to be systematically addressed in future studies if researchers are to optimize the use of BCTs to improve outcomes. It is worth noting, however, that despite using several BCTs in a well-articulated fashion, the discontinuation rates of approximately 20% appeared to be of similar magnitude to that observed in previous studies. The current study, in which the experimental and control conditions were different only in relation to task difficulty, the individual assignment of tasks based on one’s cognitive profile, and the provision of immediate and recurrent feedback, support the hypothesis that these intervention features add to the more general, possibly practice-related effects of generic and non-adaptive training, especially in the longer term.
In the present study, participants were given the option to train for a period ranging between 8 and 12 weeks, allowing us to conduct exploratory analyses concerning dose-response relationships within a single trial. In practice, the percentage of participants who completed at least 80% of the minimum prescribed intervention program was only around 65% (for participants in the CCT condition), and several participants (n = 4) completed more than the maximum prescribed dose, which resulted in an even wider range of “dose”-related data. When examining the associations between the total amount of time spent training and various outcomes, the only significant associations observed were with the final score on the computerized assessment delivered by CogniFit and the non-memory cognitive composite, but these associations dissipated once the baseline non-memory composite scores were controlled. The reasons for these observations are unclear but the small sample size is implicated. Indeed, all participants in the CCT condition who have trained for more than the minimum amount of sessions prescribed have been classified as “responders” in that they showed an improvement of at least a 0.5SD in their global cognitive composite score by the follow-up assessment. It is also possible that the frequency with which participants train is more closely associated with cognitive outcomes than the overall number of sessions. As dose-response relationships in home-based CCT are likely to be influenced by multiple moderating factors, further studies, specifically designed to address dose-response relationships are required to better understand this issue in the context of cognitive training in the older adult population.
Limitations
The current study had a number of limitations that likely impact on the strengths of the conclusions. First, objective data regarding adherence to the prescribed intervention were only available for the experimental condition (through the automatic reports generated by CogniFit), and while the subjectively reported adherence data from the control condition suggested excellent adherence, the reliability of these reports cannot be verified. Hence, whether the two groups trained on average a similar amount of time is not clear. It is worth noting that there is some evidence suggesting unsupervised home-based CCT may be associated with lower adherence [5], which may have contributed to the lower gains observed relative to clinic/university-based training [61]. Second, our sample size calculations failed to fully consider the range of factors recommended by Ard and Edland for power calculations in clinical trials in AD [71], including the specific statistical test to be used and associated assumptions, the trial design, and the within-group variance in change scores on the main outcome measure. Further, although the trial was reasonably powered to detect treatment effects as reflected in the interaction between assessment occasion and intervention condition on the primary and secondary outcomes, and the moderate-to-large effect sizes found at the post-intervention and follow-up assessments are encouraging, the trial was insufficiently powered to reliably detect complex interactions between assessment occasion, intervention condition, and diagnostic group. These analyses were exploratory and our conclusions regarding relative intervention gains in the different diagnostic groups are therefore essentially preliminary and tentative, and await further confirmation in a larger, more definitive trial. A related limitation concerns the use of Linear Mixed Models to analyze our data, which, while a more flexible procedure that makes fewer data assumptions relative to the traditional linear method, does include an assumption of normality in the distribution of the residuals, which is unlikely to have been met in relation to some of the secondary outcome measures (e.g., BADL scores). Hence, greater caution must be taken in the interpretation of findings related to these outcomes. In addition, as data on whether participants have improved in their performance of the online tasks on which they trained are not available, we are unable to directly verify the assumption that improvement on neuropsychological measures followed from improvement on training measures. Given the large number of training tasks (n = 33) and the timeframe for the intervention, opportunity to practice and improve performance on a given task may have been quite limited. Finally, the sample in this study reflects the commonly well-educated population in the Australian Capital Territory, and hence may not represent the older adult population in the broader Australian society. Although this likely increases the likelihood of self-selection bias, higher baseline scores on cognitive measures also means that detection of improvement in test scores becomes more difficult. In this sense, the findings of the current study may be even more applicable to less educated individuals, and, indeed, findings from the large ACTIVE trial suggest that less educated individuals may benefit more than highly educated individuals from some types of cognitive training [72].
Conclusions
With the limitations noted above in mind, the current study supports the claim that home-based, unsupervised adaptive, and quasi-individualized CCT may lead to benefits for both cognitive and selected non-cognitive outcomes in older adults with MCI, MrNPS, or both. Furthermore, these benefits may be further consolidated in the months immediately following training cessation. No compelling evidence was found to suggest that older adults with MrNPS superimposed on their mild cognitive impairment are less likely to benefit from such an intervention as far as cognitive outcomes areconcerned.
Footnotes
ACKNOWLEDGMENTS
The authors wish to thank all the participants who took part in this study. We further wish to thank CogniFit for donating the CCT platform for use in the current study, and for providing technical support.
The trial was supported by grants from the Australian Dementia Collaborative Research Centre, and the Alzheimer’s Australia Dementia ResearchFoundation.
The dataset used and analyzed during the current study is available from the corresponding author on reasonable request.