
Abstract
Background:
Links between physical activity and dementia are based primarily on cross-sectional data or studies with unsatisfactory follow-up.
Objective:
We leveraged three decades of follow-up from an established cohort to determine whether physical activity in midlife is associated with late-life cognition and dementia.
Methods:
The Johns Hopkins Precursors study (n = 646) enrolled participants from 1948–1964 and administered questions about physical activity, from which we calculated metabolic equivalents (MET h/day), and exercise from 1978-present. Cognitive tests were administered in 2008. Dementia was adjudicated through 2011. To characterize associations with midlife physical activity, we used linear regression for cognitive tests and Cox proportional hazards models for dementia onset. Models adjusted for age, sex, smoking, diabetes, and hypertension.
Results:
No physical activity measure from 1978 was associated with late-life cognition or onset of dementia. Both MET h/day (β= 0.007, 95% CI: 0.002, 0.013) and regular exercise (β= 0.357, 95% CI: 0.202, 0.513) in 2006, however, were associated with better cognition in 2008.
Conclusion:
Findings from this 30-year cohort study that physical activity measured recently, but not in mid-life, is associated with late-life cognition fits with null findings from randomized trials and other observational studies with extensive follow-up. Cross-sectional findings may be misleading due to reverse causation.
INTRODUCTION
Dementia is a relentlessly progressive, ultimately fatal neurodegenerative disorder affecting anestimated 35.5 million people worldwide [1–3]. While our understanding of the pathophysiology of dementia has advanced substantially in recent decades, there are unmet needs for early preventive strategies [2, 4]. Recommendations for behavior modification have potentially greater population effects than guidelines for stricter hypertension or glucose control.
Physical activity and regular volitional exercise have been identified as potentially modifiable risk factors for dementia and cognitive decline [5, 6]. The estimated population attributable risk for dementia associated with physical inactivity is potentially greater than for diabetes, midlife hypertension, depression, smoking, or cognitive inactivity [7]. However, findings from short-term intervention trials of physical activity on cognition have been largely null [8, 9]. A recent Cochrane review failed to find any association between aerobic exercise interventions and cognitive performance among cognitively healthy older adults, even among the subset of trials demonstrating improved cardiorespiratoryfitness [10].
The association between physical activity and cognition has biological plausibility [11]. Cardiovascular benefits of physical activity may reduce the vascular contribution to dementia. In mice models, physical activity is associated with less accumulation of amyloid-β plaques implicated in dementia [12]. Aerobic exercise upregulates hippocampal levels of brain-derived neurotrophic factor [13]. Physical activity also improves blood flow to the brain and reduces blood viscosity, which are associated with better cognitive performance [14]. However, the timing and dosing of these effects in humans, as well as the causal attributions, are unclear. Available prospective data on the relationship of physical activity in middle and later life with cognitive performance in later life are lacking or unsatisfactory, due to cross-sectional study designs, assessment of physical activity in persons already 65 years of age or older, and short durations of follow-up which fail to rule out reverse causation. Many observational studies show physical activity levels in older age concurrently measured alongside cognitive performance are associated with lower short-term risk of dementia [15] and higher cognitive performance [16–18]. A systematic review of risk factors for cognitive decline noted the low quality of evidence for physical activity; further, no studies had more than eight years between physical activity assessment and cognitive assessment [19].
Physical activity and exercise measured within 10 years of cognitive assessment or dementia onset cannot exclude the possibility that lower activity levels are a consequence of subclinical cognitive deterioration, or that physical activity is a proxy for life engagement for other lifestyle characteristics such as cognitive activities. Assessment of physical activity during middle age provides a stronger argument against bias due to reverse causation because subclinical cognitive impairment is unlikely to affect reports of physical activity in middle age [20].
We used self-reported measures of physical activity. Although there are understandable limitations of self-reported physical activity, it has been a standard approach to physical activity assessment for decades. Notably, self-reported low and moderate types of physical activity can be less reliable than direct measurements of fitness or activity levels [21]. Thus, in our study we considered physical activity due to vigorous and moderate activities, which has greater reliability [21]. Moreover, previous research has documented that self-reports do not necessarily correlate well with objective measures of a wide array of constructs, from physical activity [22] to cognitive performance [23]. Self-reported measures incorporate qualitatively more information than objective measures such as a person’s emotions and self-awareness of their own functioning, and is thus a critical reason for the recognition in clinical practice for patient-reported outcomes research (e.g., PROMIS) [24].
Despite longitudinal evidence and randomized trials to the contrary, the prevailing notion persists that midlife physical inactivity is a risk factor for dementia [25]. We evaluated the prospective association between physical activity and exercise in midlife on cognitive performance and impairment in later life. We used up to 30 years of longitudinal data from the Johns Hopkins Precursors study, which has followed participants since they were students in medical school with mailed questionnaires about self-reported exercise, physical activity, and physical limitations. The cohort is medical graduates, a relatively homogeneous population offering a novel opportunity in the study design to control for premorbid amounts of education and cognitive enrichment [26]. We hypothesized greater volume and intensity of regular physical activity in later life, but not midlife, are associated with higher cognitive performance and lower risk of dementia in latelife.
MATERIALS AND METHODS
Participants
The Johns Hopkins Precursors study enrolled medical graduates from 1948–1964 who have been followed annually with mailed health questionnaires since graduation. The original cohort included n = 1,337 participants (n = 1,216 men and n = 121 women), most of whom are white. Rates of follow-up are above 72% for years used in this study. Information about mortality is known for 99% of the cohort [27]. We excluded participants with no cognitive testing in either 2005 or 2008 (n = 655). Of the 682 with cognitive testing in 2005 or 2008, n = 646 answered the 1978 questionnaire and comprise the study sample (n = 598 men and n = 48 women). Study procedures have been reviewed by the Johns Hopkins University School of Medicine Institutional Review Board.
Primary outcomes
An adjudication committee of physicians assigned dementia diagnoses and dates of onset based on medical records. Additionally, five cognitive tests were administered in 2005 and 2008: the Telephone Interview for Cognitive Status (TICS; test-retest reliability: 0.96) [28], animal naming (test-retest reliability: 0.77), phonemic fluency (test-retest reliability: 0.82; count of F, A, and S words produced) [29], Hopkins Verbal Learning Test (HVLT; test-retest reliability: 0.74) [30], and the Brief Test of Attention (Cronbach’s α: 0.91) [31]. These tests have been validated in older adults and described elsewhere in this cohort [32]. The 2008 cognitive endpoint was of interest; we forward-filled missing cognitive data in 2008 with 2005 data if available (n = 151, 22%) because we did not expect meaningful cognitive change over the short interval. Correlations between 2005 cognitive tests and their 2008 counterparts in these data ranged from r = 0.38 to r = 0.61, which are marginally lower than each tests’ test-retest reliability and reasonable to expect given modest changes.
To summarize overall cognitive performance, we averaged together standardized versions of the cognitive tests into a general cognitive composite z-score with mean 0 and variance 1. We used 2005 cognitive test scores for participants who did not complete the 2008 assessment. Particularly among adults over age 70, some age-related changes are expected in cognitive performance, on the order of about 0.05 standard deviation units annually [33]. This effect corresponds to approximately 0.26 words/year on the animal fluency task or the HVLT, or 0.2 points on the TICS. When we adjusted for these potential decrements between 2005 and 2008 among participants whose 2005 scores we used, no inferences changed.
Primary exposures
Surveys of physical activity and exercise occurred as early as 1978 and were repeated in 1986, 1989, 1993, 1995, 1997, 2003, and 2006. Participants were asked the number of hours in a usual day over a typical week they spent doing vigorous activities (e.g., digging in the garden, strenuous sports, jogging, heavy carpentry, bicycling on hills), doing moderate activities (e.g., housework, light sports, walking, yardwork, bicycling on level ground), doing or sedentary light activities (e.g., sitting, office work, driving, eating), and sleeping. We assigned a metabolic equivalent (MET) value to each category of activity, where 1 MET represents energy expended per hour sitting quietly. Assigned MET values were 7 for vigorous activities, 4 for moderate activities, 1.5 for light activities, and 0.9 for sleeping [34]. In the main analysis, to more directly test effects of strenuous physical activity as opposed to less energetically demanding activities such as sitting, we constructed a MET-hours variable comprised only of moderate and vigorous activities, representing average self-reported metabolic equivalents expended in a typical day during the past week in vigorous and moderate activities.
In addition to hours per typical day spent doing certain categories of physical activity, participants were also asked, “At least once a week, do you engage in any regular exercise such as brisk walking, jogging, bicycling, etc., long enough to work up a sweat?” Correlations between the exercise variables collected in 3-4 year intervals ranged from r = 0.3 to r = 0.4. While these correlations are, as expected, lower than two-week test-retest reliabilities of physical activity questions (0.4 < r < 0.6) [35], the time delay was much longer in the present study and thus suggests acceptable test-retest reliability allowing for modest natural changes.
We considered four physical activity variables, each available in 1978 and 2006. First, we used continuous MET h/day in the past week expended on vigorous and moderate activities. Second, to test whether strenuous energy expenditure in particular is more predictive of cognitive health than non-exercise physical activity, we identified participants in the highest decile of self-reported 1978 MET h/day to identify high-activity participants. Third, we identified participants in the lowest decile of self-reported overall 1978 MET h/day to classify low-activity participants, to evaluate whether benefits of physical activity on cognitive performance are stronger among participants with lower levels of physical activity [8, 36]. Fourth, we used regular exercise in the past week.
Of n = 646 participants in the study, n = 460 (71%) had available data on MET h/week and n = 562 (87%) answered whether they exercised regularly in 1978. The potential for any differential response bias in 1978 is minimal due to the 30-years of follow-up between the exposure and cognitive outcome. We used multiple imputation with iterative chained equations to impute missing physical activity data (n = 186 for MET h/week and n = 84 for regular exercise) based on 20 random draws [37, 38]. Parameter estimates were averaged across datasets and standard errors were calculated using Rubin’s rules [39].
Analysis plan
We used means and proportions to characterize the sample. We then used linear regression for the general cognition z-score and Cox proportional hazards survival analysis for dementia onset to characterize associations with physical activity. Regression models were estimated in the overall sample and, to test for cohort differences, stratified by median age (45 years in 1978). Demographically-adjusted models were adjusted for age, sex, and smoking status in 1978. Fully adjusted models additionally adjusted for body mass index (BMI), hypertension, and diabetes.
Trajectories of physical activity
Next, to determine whether different patterns of change in physical activity over the life course confer risk of cognitive impairment or dementia, we estimated growth mixture models of the continuous MET h/day in the past week between 1978 and 1997 to identify groups defined by trajectory of change in physical activity, which were used to predict cognitive performance and dementia status. We considered only time between 1978 and 1997 to avoid using physical activity data too proximal to cognitive testing. Background information about growth mixture models implemented here are in the Supplementary Material.
Sensitivity analyses
We conducted four sets of sensitivity analyses. First, we stratified the sample by sex to determine whether associations were stronger in women (e.g., [40]) or men (e.g., [41]). Second, we repeated regressions for each cognitive test in place of the general cognitive z-score to test domain-specific cognitive correlates of midlife physical activity. Third, we analyzed separately the hours reported sleeping and doing vigorous, moderate, and light activities. Fourth, we repeated the growth mixture models of the continuous MET h/day among participants who never reported health limitations in doing moderate or vigorous activities on the MOS SF-36, administered in 2001.
RESULTS
Table 1 presents descriptive statistics for the overall sample and by median age group in 1978. The study sample was on average 47 years old in 1978 (median 45 years; range 38, 63) and 93% male (Table 1). To describe the age structure of the cohort, Supplementary Figure 1 shows a line for each participant across age and calendar year. The sample had a healthy mean BMI (23.7 kg/m2) in 1978 and low prevalence of hypertension (8.8%) and diabetes (0.8%) (Table 1). By 2006, 54% (n = 275) and 12% (n = 61) had hypertension and diabetes, respectively. The incidence of dementia was 4.3% (n = 28), with a mean onset at 77 years. Most participants reported regular exercise in 1978 (74%), expending on average 21 MET h/day (Table 1). Demographic and health characteristics did not differ by age group. Participants not tested in 2008 were on average younger by 2 years in 1978 than participants not seen for cognitive testing in 2008 (p < 0.01), and did not differ in the overall number of MET h/day reported (p = 0.51), BMI (p = 0.18), or sex (p = 0.28).
Baseline demographic characteristics of the cohort (n = 646)
Midlife physical activity and cognitive performance
Figure 1A shows a scatterplot of general cognitive performance in 2008 by average MET h/day in 1978. There is no discernible relationship (r = 0.01), despite substantial variability in both exposure and outcome. Parametric analyses in Table 2 yield similar inferences. In the full sample and subgroups stratified by the median age 45 years in 1978, no 1978 activity measure, whether continuous MET h/day, membership in the top or bottom decile of physical activity, or engagement in regular exercise, was associated with general cognitive performance in either demographic-adjusted or fully adjusted models.

Scatterplot of general cognitive performance in 2008 with MET h/day in 1978 and 2006: Results from Precursors (n = 646).
Associations between physical activity measured at two times over the life course and later life cognitive function: Results from Precursors (n = 646)
*p < 0.05; 95% CI, 95% confidence interval. +MET h/day in moderate or vigorous activity. Note. The cognitive score is in Z-score units (mean 0, SD 1), thus the decimal places. MET hours are in units of metabolic equivalent hours per day, so represent the self-reported MET hours per typical day during the past week. Demographic-adjusted models are adjusted for age and sex. Fully-adjusted models are adjusted for age, sex, smoking, diabetes, and hypertension in 1978.
Later-life physical activity and cognitive performance
Regular exercise in 2006 and MET h/day expended in 2006, a time more proximal to cognitive testing, was associated with better cognitive performance (Table 2). Figure 1B shows the latter association in a scatterplot (r = 0.14).
Midlife physical activity and onset of dementia
To assess the relationship between midlife physical activity and time to onset of dementia, Table 3 shows hazard ratios with 95% confidence intervals (CI) in the overall sample and in subgroups defined by median age in 1978 for each physical activity variable. As with continuously measured general cognition, no physical activity exposure in 1978 was associated with onset of dementia. More physical activity in 1978 was actually marginally associated with greater risk of onset of dementia (hazard ratio (HR) = 1.36, 95% CI: 0.91,2.03).
Hazard ratios from survival analysis of time to dementia for physical activity measured at two times over the life course: Results from Precursors (n = 646)
*p < 0.05; HR, hazard ratio; 95% CI, 95% confidence interval. +MET h/day in moderate or vigorous activity. Note. METS are in units of metabolic equivalent hours per day, so represent the self-reported MET hours per typical day during the past week. Demographic-adjusted models are adjusted for age and sex. Fully-adjusted models are adjusted for age, sex, smoking, diabetes, and hypertension in 1978. Coefficients for exercise represent the ratio of hazard for dementia comparing those who reported exercising in 1978 versus those who did not report exercising.
Means by trajectory class of MET h/day over time from growth mixture models: Results from Precursors (n = 646)
Later-life physical activity and onset of dementia
Greater physical activity and exercise measured in 2006, as hypothesized, was modestly inversely associated with risk of dementia (Table 3). Among participants aged 45 and older in 1978, MET h/day in 2006 was associated with lower dementia risk (HR = 0.94, 95% CI: 0.89, 1.00) (Table 3).
Trajectories of physical activity and cognitive performance
Growth mixture analysis suggested a model with two classes in the sample defined by level and trajectory of MET h/day from 1978–1997 provided better fit than models with one or three classes (Supplementary Table 1). Figure 2 shows physical activity trajectories of the two classes, which differ in baseline physical activity but not in rate of change over the 19 years of follow-up with 5 study visits. Neither general cognitive performance (β= 0.07, 95% CI: –0.11, 0.25; 0.00 is the reference) nor dementia (Odds Ratio = 0.82, 95% CI: 0.33, 2.03; 1.00 is the reference) were associated with trajectory class membership.
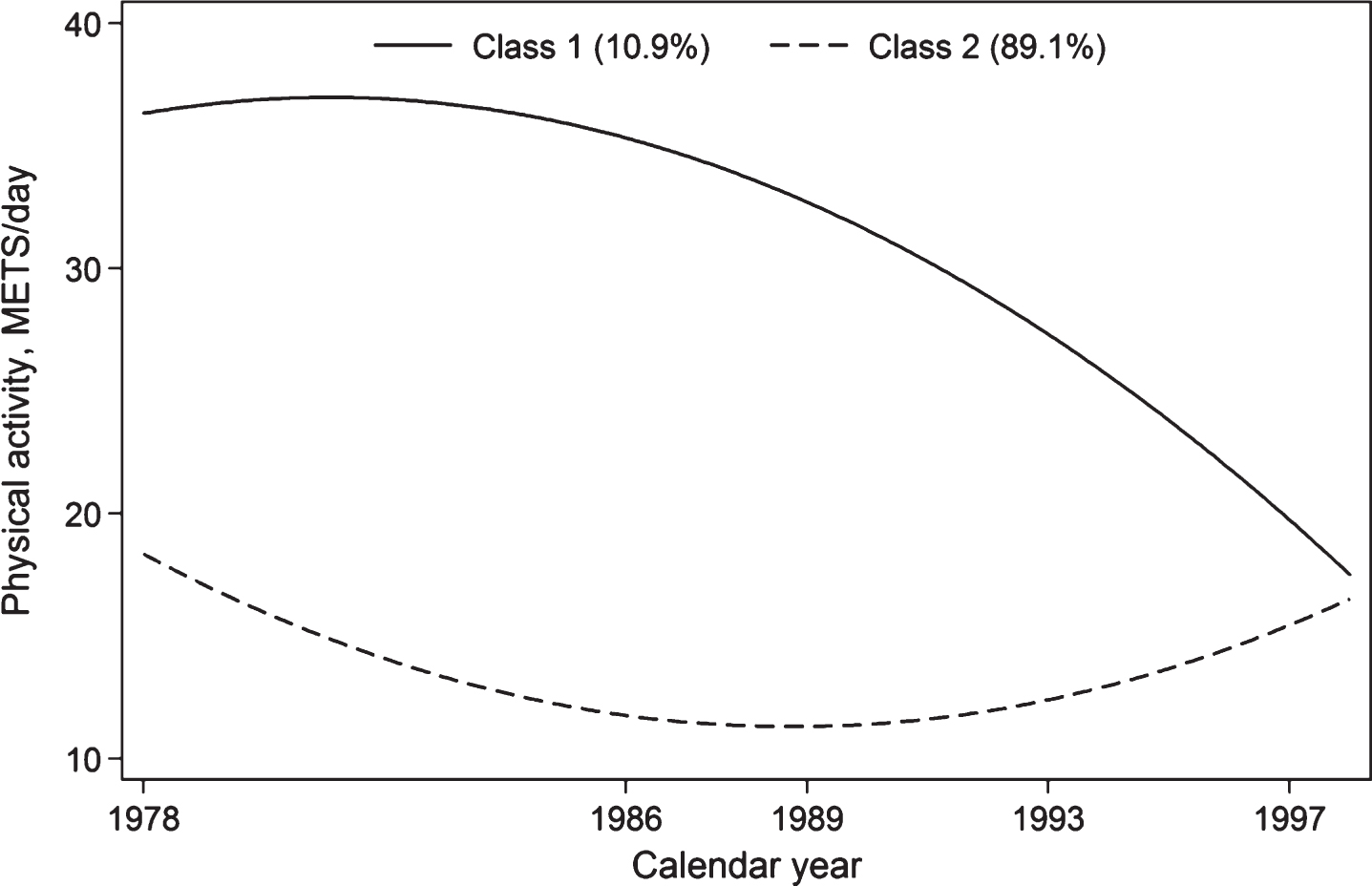
Trajectory of MET h/day: Results from Precursors (n = 646).
Sensitivity analyses
Supplementary Table 2 shows linear regression and survival analysis results stratified by sex. There were no sex differences in the strength of associations between physical activity variables in 1978. However, in 2006, both greater MET h/day in a typical week and regular exercise were significantly associated with better cognitive performance in women, but not men.
Supplementary Table 3 provides linear regression results for the five cognitive tests in place of the general cognitive score. As with the main analysis, there were no associations with physical activity in 1978 but there were in 2006, especially for regular exercise.
Supplementary Table 4 provides associations of general cognitive performance in 2008 with hours reported sleeping and doing vigorous, moderate, and light activities in both 1978 and 2006. Consistent with main analysis, we found no associations with 1978 physical activity variables. Among physical activity variables collected in 2006, less sleep and more vigorous and light activities were associated with greater cognition.
Repeating the growth mixture analysis among participants with no reported health limitations in vigorous or moderate physical activities did not change inferences: neither general cognitive performance (p = 0.49) nor dementia (p = 0.28) were associated with trajectory class membership.
DISCUSSION
Our objective was to test the prospective association of self-reported physical activity and exercise during midlife with cognitive performance and dementia risk in later life. We found no such relationship across different ways of characterizing physical activity during midlife in the overall sample, among men or women, or for specific cognitive tests. Instead, consistent with reverse causation, we detected associations of self-reported physical activity in later life with late life cognition assessed within two years of cognitive testing. Most participants in this sample do not change their physical activity patterns greatly over the life course, and trajectories do not predict cognitive performance or dementia risk.
Our findings may explain the null findings in many randomized trials of physical activity and exercise on cognitive outcomes [9, 42]. In the large LIFE trial, a 24-month moderate-intensity physical activity program was not associated with general or domain-specific improvements [9]. Lautenschlager and colleagues [43] reported results of a 6-month physical activity intervention that improved cognitive performance on one of five cognitive tests at 6 months, but was not maintained at 12 or 18 months, thus failing to demonstrate a dose-response relationship. Several trials reporting a relationship between improved physical activity and slower cognitive decline broke randomization or reported positive results for a post-priori subgroup [8, 44]. Liu-Ambrose and colleagues [45] reported resistance training in women slowed declines in executive functioning, but they also counterintuitively reported reduced brain volumes in the intervention group.
Our findings are consistent with other studies of midlife physical activity and later-life risk of dementia and cognitive performance [46–48]. The few prospective studies that have assessed physical activity during midlife long before the cognitive assessment have produced mixed results. Chang and colleagues [49] used 26 years of follow-up from 4,495 adults in the AGES-Reykjavik study aged 51 on average at the physical activity assessment and found a 40% reduced risk of dementia (OR = 0.60; 95% CI: 0.40, 0.88). Andel and colleagues [46] reported a relationship between regular exercise in midlife (mean age 48 years) and risk of dementia 31 years later (OR = 0.34, 95% CI: 0.16, 0.72) using the Swedish Twin registry. However, this relationship was not maintained in a matched co-twin control analysis, suggesting it may be attributable to unmeasured shared familial and genetic characteristics. A similar narrative was found in a study of Finnish twins aged 24–60 at physical activity assessment: unmatched associations with dementia (based on ICD codes without adjudication) were significant but matched twin analyses were not [47]. Another study reported data from the CAIDE study in which moderate, but not low, levels of physical activity assessed at age 51 were associated with greater risk of dementia after 28 years of follow-up [48].
Participants in the Precursors study, by virtue of having attended a selective medical school, represent a highly homogeneous sample in which to evaluate risk factors for cognitive impairment. Cognitive decline is typically a more compelling marker of brain damage than impairment at one occasion, because decline is less susceptible to extraneous, time-invariant factors such as years of education which precede onset of dementia [26]. Previous studies may have been more vulnerable to residual confounding by such factors since they included a diverse cross-section of people with respect to education, socioeconomic status, and the like. The Precursors Study is less susceptible to this bias because the study effectively restricts the extent of variation in levels of this cognitive reserve. This study composition might also be considered a potential limitation regarding generalizability across a broad range of adults. We used epidemiologic data to make inferences regarding a biologically plausible mechanism by which physical activity affects cognitive decline in later life and dementia risk, and we have no prior expectation that exercise affects cognition differently depending on one’s educational status. Certainly, levels of physical activity may vary by background variables such as race, sex, and socioeconomic status and confounding might differ by background, but potential loss in generalizability may be balanced by considerable gain in internal validity. Restricting the sample’s composition is a research design akin to statistically controlling very well for confounders.
Limitations of our study include limited sample size and a low number of progressions to dementia, which may have limited our power to detect associations. We note that despite the limited sample size, we did detect associations with physical activity measured two years prior to cognitive testing, thus replicating findings of many existing studies. A related limitation is although we found no sex differences, the small number of women (n = 48) in our study precludes our ability to confidently generalize findings to women; we provided analyses stratified by sex in Supplementary Table 2. Previous research suggests men and women may self-report physical activities differently [22]. Likewise, the study’s generalizability to racial and ethnic minorities is limited. Additionally, data on physical activity and exercise were prospectively collected, but based on self-report. Self-reported measures of light or moderate physical activity without objective validation are susceptible to misclassification [50], although we are unaware of evidence that such errors would differ by subsequent levels of late-life cognitive impairment. Another limitation is that, by virtue of being physicians, participants may have less vascular burden affecting associations we investigated. This healthy participant bias is underscored by the low prevalence of hypertension (8.8%) during midlife in this sample compared to other samples such as the ARIC study (32.8%). Another limitation is that coarsely binned measures of physical activity make it difficult to precisely discriminate the benefits of lifestyle activities not typically categorized as physical activity or volitional exercise, which may be important for health, functioning, and cognitive status with aging. A further study limitation is that more cognitive impaired participants may be less likely to give an accurate report of their physical activity in 2006. Inaccuracies in 2006 physical activity reporting would be expected to weaken associations, unless the measurement error is differential. Any potential differential measurement error could induce either conservative or anti-conservative biases relative to an association. Such a bias would be unlikely to affect associations with physical activity in mid-life, given the 30-year period between assessments. A final limitation is that detected associations might be the product of differential loss to follow-up: participants who died before cognitive testing in 2008 may have had poorer or better levels of physical activity. In this study, 67% of those who answered the physical activity information in 1978 received cognitive testing later in life, so there is a potential for attrition bias. As noted earlier, this is unlikely, since the participants with data in 1978 did not differ in the overall number of METs reported (p = 0.51) with respect to whether they were or were not seen for cognitive testingin 2008.
In conclusion, the prevailing notion that higher levels of physical activity protect against cognitive impairment in later life may result from the artifact of reverse causation. While physical activity is strongly recommended for many reasons, our data suggest cognitive health may not be one of those reasons. It is probably unrealistic to assume one component of a healthy lifestyle, such as physical activity, can be the magic bullet for prevention of a complex multifactorial condition [19].
Footnotes
ACKNOWLEDGMENTS
This work was supported by grants AG01760, DK02856, and DK07732 from the National Institutes of Health, Bethesda, MD. Dr. Gross was supported by K01-AG050699 from the National Institute on Aging. Dr. Schrack was supported by K01-AG048765 from the National Institute on Aging. Conclusions contained herein do not necessarily reflect the views of funders.