
Abstract
With the increase in the proportion of aged population due to the rapid increase of life expectancy, the worldwide prevalence rate of multiple neurodegenerative diseases including Alzheimer’s disease, Parkinson’s disease, and Huntington’s disease has been increased dramatically. The demographic trend toward an older population has drawn the attention to new drug discovery and treatment on age-related diseases. Although a panel of drugs and/or therapies are currently available for treating the neurodegenerative diseases, side effects or insufficient drug efficacy have been reported. With the long history in prescription of Chinese medicine or natural compounds for modulating aged-related diseases, emerging evidence was reported to support the pharmacological role of Chinese medicine in ameliorating the symptoms, or interfering with the pathogenesis of several neurodegenerative diseases. This review brings evidence about today’s trends and development of a list of potential neuroprotective herbal compounds from both the traditional and modern pharmacological point of view. With future projections, the potential hope and implication of using Chinese medicine as an alternative source for novel drug discovery for neurodegenerative diseases is proposed.
Keywords
THE AGING WORLD: PATHOGENESIS AND CURRENT THERAPY OF NEURODEGENERATIVE DISEASES
Based on the “World Population Ageing Report 2015” issued by the United Nations, it was postulated that the number of people in the world with age over 60 will accelerate from 901 million to 2.1 billion by 2050 [1]. The population of China is also aging. It was reported that by 2030, 358 million of population will be aged over 60, and younger generations will have a heavy burden of elderly care. Consistently,worldwide data have indicated an increasing prevalence of neurodegenerative diseases including Alzheimer’s disease (AD), Parkinson’s disease (PD), and less common neurodegenerative disease such as Huntington’s disease (HD) with age [2], which is worth our attention. It is still a big challenge for academia and pharmaceutical industries to discover a really powerful anti-neurodegenerative agent based on the high failure rate of the AD candidate compounds in the last two decades.
Alzheimer’s disease
Dementia is considered as one of the most important health problems in elderly, and AD has accounted for about 60% of all dementias among elderly in the world [3]. In the US, there are approximately 5 million of AD patients currently, and it is postulated to have more than 13 million of AD patients by 2050. The costs of care to AD patients is predicted to reach a huge amount of $1.2 trillion in the US by 2050 [4]. The systematic epidemiology analysis by Chan et al. reported the number of AD patients in China from 1999 to 2010 has been increased from 1.93 to 5.69 million [5]. AD is characterized by progressive loss of memory, cognitive and decision making deficits with problems in language ability. These symptoms were accompanied by various neuropsychiatric conditions such as anxiety, depression, or apathy [6]. Senile plaques containing amyloid-β (Aβ) peptide produced by sequential cleavage of the amyloid-β protein precursor (AβPP) via β- and γ-secretases [7], and neurofibrillary tangles (hyperphosphorylated microtubule-associated tau protein) in the neocortex, are highly correlated with neuropathological features and neuronal loss of AD. Formation of plaque and tangles is potentiated by various factors such as genetic, inflammation, and production of reactive oxygen species (ROS) [8]. The amyloid cascade hypothesis suggested the production of toxic Aβ aggregates lead to the pathogenesis of AD. The discovery of mutations in presenilin (PS1), which is involved in AβPP cleavage and Aβ production [9], has further supported the hypothesis. Although the amyloid hypothesis is widely accepted, with the recent failure of a clinical study of Aβ vaccination, new therapeutic strategy for AD, such as the use of immunotherapies with the antibodies or tau-targeted therapies, are currently under investigation [10].
Parkinson’s disease
With a prevalence of over 1,900 patients per 100,000 in people of age over 80, PD is characterized by the death of dopaminergic neurons in the substantia nigra region and Lewy body deposition in the midbrain. This is accompanied by movement disorder symptoms such as bradykinesia, rigidity, and resting tremor. Pathogenic risk factors of PD include microtrauma or focal cerebrovascular damage of brain, stimulation by toxins, drugs or pesticides, dysfunction of ubiquitin–proteasome system, oxidative stress and neuroinflammatory reactions, genomic factors which lead to conformational changes, misfolding and aggregation of proteins, and neuronal death [11]. Current pharmacological interference for PD includes the use of dopamineprecursors such as levodopa (L-DOPA); dopamine agonists such as amantadine, apomorphine, bromocriptine, cabergoline, pergolide, and ropinirole; monoamine oxidase (MAO) inhibitors such as selegiline; and catechol-O-methyltransferase (COMT) inhibitors such as entacapone [2]. However, motor fluctuations and dyskinesia are the major complications of L-DOPA therapy. Additional complications include gastrointestinal or cardiovascular problems, changes in neuroendocrine system, and psychiatric disorders after treatment of anti-parkinsonian drugs [12].
Huntington’s disease
HD is an inherited neurodegenerative disease characterized by motor disorder and cognitive problems in dementia, and is fatal in majority of cases. With an average onset age at around 40, psychiatric problems such as depression or anxiety were also observed in patients of HD. HD is more prevalent in European peoples with appropriately 10 to 15 patients out of 100,000 people. Pathogenesis of HD is caused by a mutation with an over 40 number of CAG trinucleotide repeat in the huntingtin (HTT) gene, resulting an excessively long polyglutamine tract near the N-terminus of HTT protein, which is responsible for early development of neurons [13]. Although currently there is still no effective therapeutic treatment to slow down the decline in motor or cognitive function in HD, symptoms such as chorea can be modulated by dopamine receptor blockers like haloperidol or dopamine-depleting agent such as tetrabenazine [14].
TRADITIONAL CHINESE MEDICINE (TCM) HERBAL PRESCRIPTION AND THEORIES FOR MODULATING AGE-RELATED NEURODEGENERATIVE DISEASES
TCMs has been prescribed in the Chinese community for more than 2,000 y for treating symptoms including forgetfulness, disorientation, insomnia, loss of consciousness, cramps, and seizures, which are highly related to aging or age-related diseases [15]. According to Chinese medicine theory, age-related neurodegeneration are attributed to the follow aspects: 1) The loss of kidney function (shen jing) is accompanied by a lack of nutrients to the brain, which leads to the gradual diminishing of the brain and causes dementia; 2) Heart and spleen function deficiency and a lack of blood (qi) flow that reaches the brain, leads to symptoms such as nervousness, palpitations, insomnia, anxiety, and a decrease in learning and memory ability; 3) The stagnation and stasis of blood (qi) in the peripheral organs lead to insufficient blood flow to the brain and causes the decline in memory [16, 17]. Currently, the top 10 popular anti-aging herbs are Heshouwu (Fleece-Flower Root) [18], Huangqi (Radix Astragali) [19], Renshen (Radix Ginseng) [20], Sanqi (Radix Notoginseng) [21], Ciwujia (Radix Acanthopanacis Senticosl) [22], Lingzhi (Ganoderma) [23], Gouqi (Fructus Lycii) [24], Hongjingtian (Radix et Rhizoma Rhodiolae kirilowii) [25], Jiaogulan (Herba Gynostemmatis Pentaphylli) [26], and Fengwangjiang (Royal Jelly) [27] in China [28]. Most of them are traditional TCMs prescribed for maintaining good memory and balanced body homeostasis, regulating age-related neurodegenerative diseases, or promoting longevity among Chinese people. Modern pharmacological researchers have confirmed part of their beneficial roles in term of anti-oxidation [21], anti-inflammation [29, 30], and anti-apoptosis properties [19].
As neurodegeneration is a complicated and multifactorial disease, Chinese medicine offers the advantage of modulating the systemic organs via synergetic effects of different compositions within a single herb. For example, the well-known TCMs such as Yuanzhi (Radix Palygalae) [31], Renshen (Radix Ginseng) [32], and Hehuanpi (Cortex Albiziae) [33] are prescribed to ameliorate memory loss; Gouqi (Fructus Lycii), Fuling (Poria), Gancao (Radix Glycyrrhizae), and Shichangpu (Rhizoma Acori Tatarinowii) are used to improve the cognitive function [34]. In addition, traditional herbal formulations such as “Kaixinsan” which are composed of 4 herbs, Radix Ginseng, Radix Polygalae, Rhizoma Acori Tatarinowii, and Poria, is a famous TCM formula for the treatment of mental disorders, forgetfulness, and depression possibly via the pCREB pathways [35]. Additional herbal formulations such as Danggui-Shaoyao-San, Tianma Gouteng Yin, and Jitai Tablet, are reported to exert their neuroprotective effects via ameliorating cognitive dysfunction in AD model [36], preventing degeneration of dopaminergic neurons in PD model [37], and improving behavioral impairments in PD mice [38], respectively. Ginkgo biloba extract EGb 761®, and a modified formulation of SuHeXiang Wan, were found effective in modulating cognitive behavior and neuropsychiatric symptoms of AD [39], Aβ-induced memory impairment, and Aβ levels in AD mice model [40], respectively. Furthermore, our previous work on Herbal Leonuri extract [41] has confirmed the cerebral protection effect of the herbal extract on stroke model via its anti-oxidation properties. Therefore, the Chinese medicine provides a rich source for theidentification and pharmacological research ofpotential neuroprotective compounds for therapeutic application.
MODERN PHARMACOLOGICAL ROLE OF TCMS AND THEIR MOLECULAR MECHANISMS IN REGULATING NEURODEGENERATIVE DISEASES
Autophagic degradation of neurodegenerative disease proteins
Autophagy is a cellular system responsible for delivering cellular protein, organelles, or invading microorganisms to lysosomal degradation. With a variety of physiological and pathophysiological roles such as starvation adaptation or clearance of cytoplasmic constituents extensively reported in the past decades, the pathological role of autophagy in cancer, aging, and neuro-degenerative disorders have also been well studied [42]. It was reported that the ubiquitin-proteasomal system is responsible for cellular degradation of unwanted or excessive proteins and organelles [43]; however, membrane-bound proteins, aggregated, and oligomeric neurodegenerative disease proteins, which are too large to pass through the narrow barrel of the proteasome, are degraded by autophagy [44]. Examples of these proteins include HTT protein with long mutant polyglutamine (polyQ) tracts [45, 46], and A53T/A30P mutant α-synuclein protein, which contributes to the pathogenesis of HD and PD respectively, can be degraded by autophagy [45–51]. Autophagy was reported to play a protective role in alleviating the levels and hence, the toxicity of both mutant huntingtin and α-synuclein [52, 53], suggesting the pharmacological activation of autophagy may be beneficial to regulate neurodegenerative diseases [54].
Concomitantly, recent studies have reported the identification of novel autophagic enhancers from TCMs as potential neuroprotective agents. Our previous work have identified onjisaponin B [55] and a partially purified bioactive fraction from Radix Polygalae [56] as novel autophagic activators that are able to accelerate the degradation, and decrease the toxicity of mutant α-synuclein and HTT protein in cellular models. Furthermore, we have reported the active component, neferine, isolated from the lotus seed embryo of Nelumbo nucifera, can also attenuate the protein level and toxicity of mutant HTT through autophagy [57]. Hederagenin and α-hederin isolated from Hedera helix are reported to activate autophagy, promote degradation of neurodegenerative diseases proteins, and improve motor deficits in mice treated with neurotoxin, MPTP [58]. Recently identified TCMs, such as arctigenin from Arctium lappa (L.), are able to accelerate the autophagic clearance of Aβ [59]; isorhynchophylline, an alkaloid from Uncaria rhynchophylla, facilitates the autophagic degradation of α-synuclein in neuronal cells [60], with improvement in cognitive deficit of Aβ- rats [61]; neuroprotective effects of baicalein from Scutellaria baicalensis [62], and resveratrol from red wine or food [63] were also suggested to be executed possibly via autophagy. All of the above findings have suggested the potential therapeutic roles and new directions for isolating novel autophagic activators from TCMs for neuro-therapy.
Novel herbal compounds with neuroprotective effects via regulating different signaling pathways
Our previous findings suggested that leonurine, an alkaloid isolated from Herba leonuri (HL), exerts its neuroprotective effect against cerebral ischemia/reperfusion-induced mitochondrial dysfunctions in middle cerebral artery occlusion model of rat brain, via its anti-oxidation and anti-apoptosisproperties [41]. Besides, leonurine decreased the infarct volume and further improved neurological deficit of stroke rats. The protective effects on ischemic stroke models were confirmed to be executed via an increase in the activities of anti-oxidation enzymes, such as glutathione peroxidase and superoxide dismutase, with the decrease in mitochondrial ROS production and adenosine triphosphate (ATP) biosynthesis [64]. In addition, SCM198 (4-guanidino-n-butyl syringate), a new compound from HL, was proved to attenuate the neurotoxin (6-OHDA)-induced apoptotic cell death in dopaminergic cells and improve rotational behavior in 6-OHDA-induced motor deficit rat model via an increase in superoxide dismutase antioxidant activity with a decrease in levels of ROS [65]. Furthermore, SCM-198 was confirmed to ameliorate the recognition ability, spatial memory, cognitive deficits, and promote survival of neurons in AβPP and PS1 transgenic mice [66], suggesting the potential therapeutic value of TCMs on neuroprotection (Fig. 1).
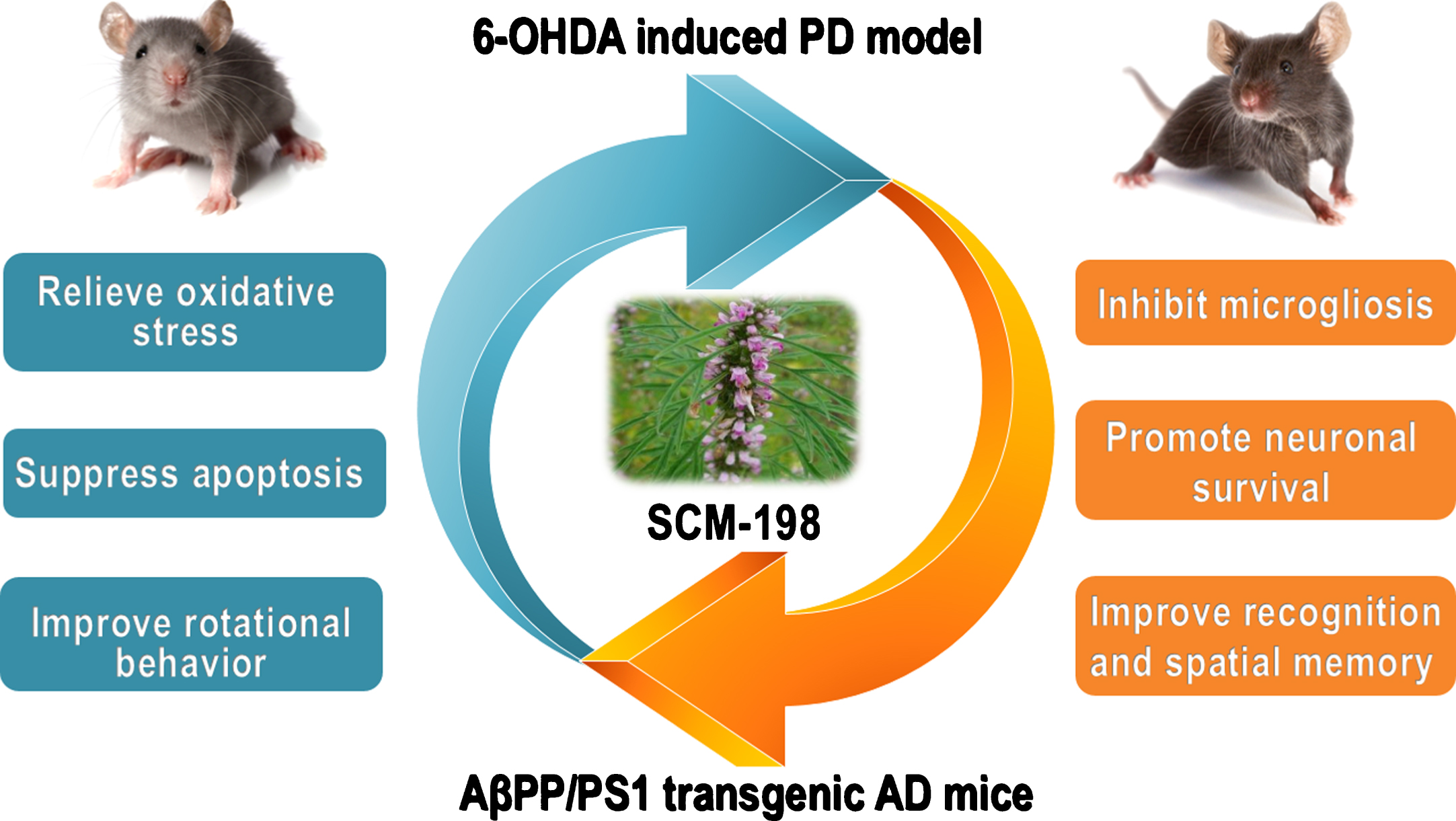
SCM-198, derived from Herba leonuri, shows neuroprotective potential in both 6-OHDA induced PD mice and AβPP/PS1 double-transgenic AD mice.
Salidroside isolated from Rhodiola sachalinensis protects cells against cytotoxicity and oxidative damage induced by accumulation of Aβ [67, 68]. Furthermore, salidroside possess its neuroprotective effect via improving the impaired hippocampal neurogenesis by scavenging ROS in the streptozotocin induced AD rat model [69]. Curcumin, a well-known natural product with potent anti-inflammation and anti-oxidation effects, was reported to bind plaques, reduce and inhibit the formation Aβ oligomers and fibrils in mice model [70]. Huperzine A, an alkaloid extracted from the plant Huperzia serrate, is commonly used in China to treat AD [71]. Clinicaltrials have demonstrated the protective effect of huperzine A in improving memory deficits in patients with senescent forgetfulness symptoms [72]. It was reported that huperzine A can rescue neural stem cells from apoptosis induced by Aβ peptide [73]. Besides, huperzine A can work as a potential therapeutic agent for AD via inhibiting acetylcholinesterase in primary cultures and reduces neuronal toxicity induced by glutamate [74].
Recently, the neuroprotective effects of natural product, garlic (Allium sativum) extract were studied. For example, Allium sativum extract co-cultivated with Hericium erinaceus mycelium showed neuroprotective effects in ischemic in vivo model [75]. Treatment of garlic extract and methionine can attenuate toxic effects induced by neurotoxicant mercury possibly via their anti-oxidation properties [76]. Allium vegetable is one of the rich sources for organic sulfur-containing compounds. It has been proven that diallyl disulfide, diallyl trisulfide, and S-ally cysteine, which are the key ingredients of garlic, are hydrogen sulfide donors. In fact, the lack of hydrogen sulfide contributes to pathogenesis of arterial and pulmonary hypertension, AD, liver cirrhosis, and gastric mucosal injury [77]. Therefore, identification of organic molecules that can regulate the formation of hydrogen sulfide is important. Concomitantly, our group reported that S-propargyl cysteine (ZYZ-802), a novel hydrogen sulfide-modulated agent, can modulate ischemic heart disease [77], and improve spatial learning and memory deficits induced by lipopolysaccharide-mediated neuro-inflammation through regulating the hydrogen sulfide pathway [78]. All these have suggested the neuroprotective role of hydrogen sulfide-modulated agent present in natural product or TCMs.
PERSPECTIVE: THE USE OF TRADITIONAL TCMS FOR MODULATING NEURODEGENERATIVE DISEASES AND CHALLENGES
Current therapeutic approaches and challenges for neurodegenerative diseases
With the continuous extension of human life expectancy followed by an increasing number of patients with dementia (especially AD), researchers focus not only on the pathogenesis of AD, but also on the discovery of drugs for prevention or treatment of the disease. However, up to now, there is still no effective treatment for AD, and only treatmentsattempting to counterbalance the disturbance by neurotransmitters are available for relieving the symptoms currently. For example, 3 cholinesterase inhibitors, donepezil, rivastigmine, and galantamine are approved drugs for the treatment of mild to moderate AD now [79, 80]. Besides, anti-psychotic and anti-depressant drugs such as serotonin reuptake inhibitors (fluoxetine and fluvoxamine) [81] are available for alleviating the behavioral symptoms of dementia [82].
Other than the symptomatic approach, treatments that aim to regulate the pathogenesis of the disease are under extensive investigation. These ‘disease-modifying’ drugs, which focus on interfering the progression of disease at different levels, for example, modulation of deposition of Aβ plaques and formation of neurofibrillary tangle or tau protein, are under clinical trials or experimental validation. For example, Aβ lowering agents such as β-secretase enzyme BACE1 inhibitor (CTS-21166) and γ-secretase inhibitor (LY-450139), are under Phase I and Phase III clinical trials, respectively. However, inhibition of BACE1 led to toxic side effect due to the other essential physiological roles of BACE1. Besides, due to the large size of the active site of BACE1, compounds with binding affinity to BACE are unlikely to cross the blood brain barrier [6]. Similarly, other than Aβ, γ-secretase can also cleave other transmembrane proteins which are essential for growth and development, such as notch receptor 1, and therefore affect the development of BACE1 inhibitors or γ-secretase inhibitors as potential therapeutic agents of AD [83]. Drugs interfering with tau deposition (methylene blue, phenothiazine, or methylthioninium chloride) [84] or tau phosphorylation (pyrazolopyrazines, lithium, pyrazolopyridines, aminothiazole AR-A014418, or sodium valproate) [85] are under clinical trial evaluation. Other approaches, such as the use of anti-inflammatory (NSAIDs), or oxidation drugs, such as vitamin E, Ginkgo biloba, natural polyphenols including blueberries, green tea, curcumin, ω3 fatty acids, red wine, folate, vitamin B6, and vitamin B12, are also under intensive investigation [6].
Up to now, levodopa remains the most effective therapy for alleviating the symptoms of PD; however, severe side effects such as “wearing off” effect, dyskinesia, fluctuations, and other motor deficits remained unresolved [86]. Other than pharmacological approaches, neurosurgical treatment via deep brain stimulation is an alternative treatment of PD [87]. Although many management strategies have been made with progress in enhancing the effect of PD therapy with minimum side effects, in addition to modulate the disease by the symptomatic approach, advance treatments targeting the pathogenesis of the disease are highly desirable.
The use of TCMs as new therapeutic approach for modulating aged-related neurodegenerative diseases
This report has highlighted the discovery of new chemicals from TCMs or natural products for modulating age-related neurodegenerative diseases from different approaches (Fig. 2), for example, accelerating the clearance of neurodegenerative disease proteins via induction of autophagy. Rapamycin, a well-known mTOR inhibitor, is effective in inducing the clearance of mutant proteins via autophagy [53]. However, mTOR inhibitors possess side effects by inhibiting immunological function, cellular protein synthesis, and proliferation; therefore, identification of novel compounds that activate the mTOR-independent induction of autophagy, has become an alternative approach in neuro-therapeutic drug discovery. For example, lithium which is naturally present in grains and vegetables, can activate autophagy via inhibition of inositol monophosphatase, leading to depletion of free inositol and decrease in myo-inositol-1,4,5-triphosphate (IP3) levels [48], together with a significant decrease in mutant huntingtin and α-synuclein level, suggesting the therapeutic potential of autophagic enhancer in neuro-therapy.

Schematic diagram showing the modulation of age-related neurodegenerative diseases via the anti-inflammation, anti-oxidation, anti-apoptosis, and autophagy effects exerted by the listed popular TCMs in the Chinese local community. By combining the traditional therapeutic effects of the herbal compounds reported in ancient literature with modern pharmacological mechanisms reported in scientific literature, the hope of developing TCMs as potential neuroprotective agents is highlighted.
Although the use of TCMs may serve as an alternative way to prevent or treat aged-related neurodegenerative diseases, incorrect dosage, unknown molecular targets and mechanisms, or high toxicity of herbal decoction due to its complexity of compounds formulation remain the major obstacles in developing TCMs for therapeutic uses [88]. However, with a long history in prescribing TCMs for preventing or modulating or age-related disorders, dementia, or its symptoms in the Chinese local community [89, 90], interlinking modern neuropharmacology with therapeutic effect of TCMs has been a highlighted research field in these past decades. By combining advanced isolation and accurate characterization analysis on the chemical compositions of herbalformula, for example, by using ultra-performance liquid chromatography coupled to (quadrupole) time-of-flight mass spectrometry UHPLC-(Q)TOF-MS [56], together with modern biotechnology including computation docking [91], proteomics [92], and other advanced technology such as molecular bio-probe labeling on herbal compounds, live cell imaging, or genetic knockout and RNA interference technology [93], all lead to breakthroughs in the pharmacological research in TCM study and provide us with hope for developing TCMs as alternative medicine for modulating neurodegenerative diseases.