
Abstract
Background:
Dementia is a frequent diagnosis in geriatric rehabilitation. Studies in patients with dementia on the development of their cognitive status during rehabilitation and its relation to functional outcomes have been scarce.
Objectives:
To describe the changes in cognitive status in patients with dementia during inpatient rehabilitation and to determine its association with patient characteristics and rehabilitation outcome.
Methods:
Cohort study in a geriatric rehabilitation center with data collection at admission and discharge. Outcome measures were change in global and domain-related cognitive functioning and its association with activities of daily living (ADL) and discharge home.
Results:
154 patients (mean age 83.7 years) diagnosed with mild to moderate dementia were included. Cognitive performance significantly improved from admission to discharge for all cognitive variables tested (p < 0.001 to 0.03). Change in global cognitive functioning, executive functions, and episodic memory were positively associated with ADL recovery. Change in global cognitive functioning predicted ADL improvements (β= 0.32; p = 0.006). Only 7.8% of patients, characterized by worse ADL and motor abilities as well as higher frailty scores at admission, deteriorated in global cognitive scores. In comparison to patients with stable or improved cognition, these patients showed least improvements in ADL-scores (4.1 versus 12.5) and a trend for higher institutionalization (50% versus 26.5%).
Conclusions:
The findings highlight the potential of patients with dementia to recover cognitive functioning during rehabilitation. Cognitive change represents an independent rehabilitation outcome and a prognostic factor for successful rehabilitation suggesting that specific interventions are indicated to maintain and enhance cognitive functioning in these highly vulnerable patients.
Keywords
INTRODUCTION
Dementia is increasingly prevalent among patients in rehabilitation. Depending on sample specifics and cut-off criteria up to 80% of geriatric patients undergoing rehabilitation have been classified as cognitively impaired [1 –3].
Although patients with dementia can achieve functional improvements during rehabilitation [4 –7], they represent a highly vulnerable patient group with increased rates of institutionalization and mortality as well as greater length of stay [8] and lower functional outcomes [5 , 10]. Despite its clinical relevance, our understanding is limited on how cognitive functioning and its change during rehabilitation influences rehabilitation outcomes and how to adapt programs to optimize rehabilitation success in patients with dementia. Further research has therefore been requested [4].
Acute illness and hospitalization are recognized as critical events for the development of additional cognitive decline in older patients [11 –13] with rates up to 50% being reported [12 , 15]. Different mechanisms and factors were discussed in this context. Setting related factors including limited mobility, bedrest, and polypharmacy, but also individual related factors such as age, preexisting impairment, or depression have been associated with the risk of cognitive decline. In particular for patients with dementia and therefore a reduced ability to adapt, the highly standardized, busy, and unfamiliar hospital environment does not meet the specific psycho-social needs of this population [16]. The mechanisms through which abovementioned factors in combination with an acute illness can impact neurocognitive functioning are likewise multiple, with evidence suggesting that frailty, delirium, hypotension, systemic inflammation, sedative, and analgesic medications, for example, may play a role in reduced homeostatic capacity and compensatory reserve to the acute stressors [17].
Cognitive decline was found to be associated with negative functional outcomes. In a large multicenter observational study for example, cognitively impaired patients with cognitive decline were 11.5 times more likely to decline in activities of daily living (ADL) [14, 15]. Therefore, it is an important but often disregarded question, if the post-acute geriatric rehabilitation setting contributes to cognitive recovery or promotes further cognitive decline, as the majority of studies in rehabilitation research focus on functional recovery alone. Up to now cognitive status has been handled as an invariant obstacle for functional outcomes, instead of considering it a modifiable rehabilitation outcome and a factor that influences functional recovery[9 , 18–20].
Only a few studies investigated change in cognitive functioning during rehabilitation [3 , 22]. Reported rates for cognitive improvement during rehabilitation differed from 7% in a study sample of stroke patients [22] up to 35% in older multi-morbid geriatric patients [3, 21], where low rates of additional decline (11%) were reported [21, 22]. Improvement in cognitive function was related to home discharge [22] and to positive change in motorperformance [21], again suggesting an association between cognitive and functional recovery.
However, it may not be valid to generalize these results to patients with dementia in geriatric rehabilitation because of heterogeneous study samples of patients with and without cognitive impairment, setting specifics, lack of uniformity in cognitive assessment, and etiology of cognitive impairment, e.g., dementia, delirium, or depression. This differentiation is important as appropriate interventions between these conditions vary. As a consequence of the limited research in this area and methodological limitations of existing studies not only knowledge about the development of cognitive status during rehabilitation in patients with dementia and its relation to other functional outcomes, but also associated questions of interest have been left unanswered so far: Longitudinal [23] and cross-sectional [24] studies suggested associations not only between decline in global neuropsychological performance and functional performance but also for executive and memory functions [25]. Insights on the course of specific cognitive sub-domains during rehabilitation which may show different change patterns [11] and whose effect on functional recovery may also vary, are lacking. In addition, for clinicians the degree of individual change is highly relevant. Unfortunately, reliable criteria for the evaluation of significant individual change are neither available for most neuropsychological instruments nor have they been specified for patients with dementia. Therefore, reliable cut-offs for individual change have to be calculated for this specific target group. Moreover, an understanding of patient characteristics that would specify patients with cognitive decline and their capacity to improve is currently lacking. However, it has to be regarded as fundamental for the identification of vulnerable patients and the development of personalized rehabilitation programs, which would optimize cognitive rehabilitation outcomes in patients with dementia.
Our study therefore aimed, in a population of geriatric rehabilitation patients with mild to moderate dementia, 1) to assess the prevalence of change in global and domain specific cognition and to calculate the degree of improvement and decline based on sample specific reliable criteria for change; 2) to analyze differences in demographic, medical, or psychosocial variables in subgroups of patients which were associated with improvement or decline; and 3) to explore associations between cognitive change and ADL-change, as well as discharge home, as indicators for rehabilitation success.
MATERIALS AND METHODS
The present study is part of the model project Geriatric Rehabilitation for Demented Patients Study (GREDE) which was conducted at the Center for Geriatric Medicine, University of Heidelberg,Germany. The GREDE project has been described in previous publications [26, 27] and was approved by the Ethics Board of the Medical Faculty, University of Heidelberg in accordance with the Helsinki Declaration. Written informed consent was obtained from all participants or their legal representatives.
We present a cohort study of inpatients more than 65 years of age, consecutively recruited in two rehabilitation wards between 02/2011 and 12/2011 with data collection at admission and follow-up before discharge. Inclusion was based on the diagnosis of mild to moderate dementia as secondary diagnosis. Exclusion criteria were medical and/or psychological conditions not allowing the application of neuropsychological and functional assessments such as acute confusion (delirium), aphasia, severe visual or auditory impairment, severe psychiatric disorders, severe functional-motor deficits, inadequate German language level, orthopedic instability, and acute medical conditions.
Screening for cognitive impairment was performed using the Mini-Mental State Examination (MMSE) [28]. In patients with mild to moderate cognitive impairment (MMSE 17–26), dementia diagnosis was confirmed by a geriatrician according to core criteria for all-cause dementia [29]. Different types of dementia were diagnosed based on a standardized approach, including clinical history, physical and neurological examination, neuroimaging, laboratory tests, and neuropsychological testing [29 –31]. Each participant received personalized rehabilitation, depending on individual abilities and rehabilitation needs based on comprehensive geriatric assessments. Interventions included exercise, adaptive techniques, assistive technology, and psychologic and social interventions. Specific cognitive training was not part of interventions. The coordinated multidisciplinary team of health professionals involve physicians, nurses, physical and occupational therapists, speech language pathologists, psychologists, therapeutic recreation therapists, and social workers.
Measurements
The characteristics of the study participants included age, gender, number of medications,indication for geriatric rehabilitation by diagnostic groups, pre-existing delirium according to medical records, depressive symptoms (Geriatric Depression Scale, 15-item version) [32], frailty (Clinical Frailty Scale, range 1–9) [33], physical activity (Physical Activity of Inpatient Rehabilitation questionnaire, PAIR, range 0–7) [34], length of stay (days), living arrangement (community dwelling versus institutionalized), cognitive status (MMSE range 0–30) [28], motor status (Hierarchical Assessment of Balance and Mobility, HABAM, range 0–67) [33] and ADL with the Barthel Index (range 0–100) as a well-established index for scoring functional status and improvement in the rehabilitation setting [35]. We used a modified German version (Hamburger Classification Manual for the Barthel Index) administered by observation of the patient‘s performance in a care setting by a trained nurse [36].
Outcome measures
Cognitive functions commonly affected in patients with dementia were assessed by the Consortium to Establish a Registry for Alzheimer’s Disease Neuropsychological Assessment Battery (CERAD-NAB) [37] subtests which includes aspects of 5 different cognitive domains: executive functioning (verbal semantic fluency (VF): number of animal names generated in 60 sec.), language semantic memory (modified version of the Boston Naming Test (BN): naming 15 objects presented as line drawings, maximum score (MS) = 15); episodic memory encoding and recall (Word List-Learning (WL): sum of words learned in three trials in a 10-word learning list, MS = 30 and Word List –delayed recall (Recall): delayed recall of the 10 words presented in WL, MS = 10); visuospatial abilities (Constructional Praxis (CP): figures –copy, MS = 11) and speed of information processing (Modified Trail Making Test from the Nuremberg Gerontopsychological Inventory [38] (TMT): connecting numbers, mean time of 2 trials, max. 300 s). For global cognition the demographically corrected total score (TS) for the CERAD-NAB developed by Chandler was calculated by summing six subtest scores (VF; BN; WL; Recall; Recognition Discriminability: the difference of false positives and true positives in WL recognition) [39]. The CERAD TS (MS = 100±adjustments for the influences of demographic variables) provides an effective global measure of cognitive functioning which is regarded as being superior to simplified tests such as the MMSE [40].
ADL change (discharge –admission scores) and change in living arrangement (new institutionalization) for patients admitted from home were also used as outcome variables.
Statistical analysis
Means±standard deviation, median (range) or frequency (n, %) were used to describe characteristics of the sample. To test for change between admission and discharge in the different cognitive outcome variables dependent samples t-tests were used. Effect sizes were calculated as Cohen’s d [41]. Values≥ 0.2 indicate small,≥0.5 medium and≥0.8 large effects.
In lack of external criteria for meaningful short-term change in dementia patients, we computed reliable change indices and reliable change index intervals (RCI) as cut-off criteria for individual change for each cognitive variable according to Jacobson and Truax [42]. This approach takes into account the re-test reliability of the assessment instrument and variability specific for the study sample. Based on RCIs which represent respective raw score criterions to evaluate whether a person‘s individual change score from admission to discharge is considered as improved or declined. Each subject was classified into 3 subgroups for each cognitive domain: the cognitive gain group (GG) with individual change exceeding the RCI; a no-change group (NCG) within the RCI boundaries; and a loss group (LG) below the RCI.
Depending on data, differences between cognitive change groups in clinical variables, change in ADL-status, and new institutionalization was assessed using Chi-square-test, Kruskal-Wallis-test, one-way ANOVA with respective post-hoc tests (Chi-square, Mann-Whitney-U, LSD) in case of overall significance. We considered the Barthel Index as quasi-interval and used parametric analyses with admission and change scores with the advantage of increased statistical power and the future comparison of multiple trials [43]. Partial correlations were used to analyze the association between change in different cognitive test scores and ADL-change-scores controlled for admission ADL and the respective admission cognitive score.
Two linear models were applied to determine if additional to ADL admission scores, global cognitive change scores (model 1) or global cognitive admission scores (model 2) are predictive factors for ADL change. Influences of variables are given asregression coefficients β and general fit of the models are reported by the coefficient of determination R2.
For each statistical test, a two-sided p-value≤0.05 indicated statistical significance. Statistical analysis was performed using the SPSS statistics 23.0 (IBM, Armonk, NY, USA).
RESULTS
Participants
Among 637 persons screened for eligibility, 174 patients were enrolled. Twenty patients (11%) dropped out before follow up (for study flow and reasons for exclusion see Fig. 1). The study sample included 154 multi-morbid patients with mild to moderate dementia (MMSE mean 21.6±2.6). Mean age was 83.7±5.9 years, and functional capabilities were reduced with an average ADL score of 59±18.2 (Table 1). Mean length of stay was 22.7±6.7days.
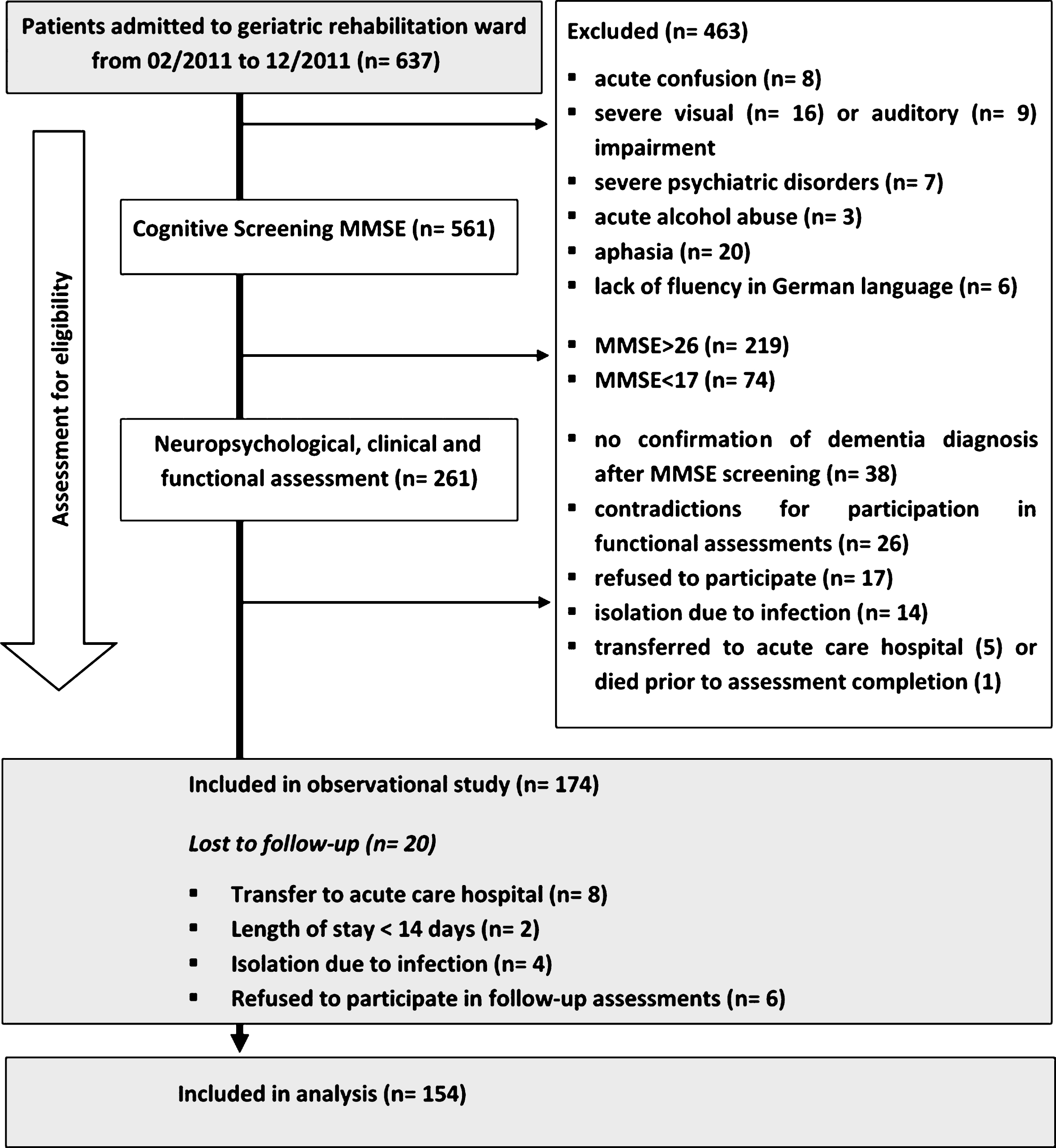
Patient recruitment and follow-up flow diagram.
Change of cognitive performance on group and individual level
Sociodemographic and clinical characteristics of participants (n = 154)
Total range of scores are given in brackets behind the variable, with higher scores indicating less impairment in MMSE, ADL, and HABAM; for frailty and depression higher scores indicate higher degree of frailty and depressive symptoms; MMSE, Mini-Mental State Examination; AD, Alzheimer’s disease; VaD, vascular dementia; MD, mixed dementia; ADL, Barthel Activity of daily living; HABAM, Hierarchical Assessment of Balance and Mobility; afor persons without actual brain image type of dementia was not defined.
Global and all domain specific cognitive performances increased significantly during the 3-week rehabilitation phase (range p < 0.001 to 0.03). Effects sizes (range d = 0.17 to 0.70) indicate small to medium effects and were highest in global cognitive functioning (CERAD TS, d = 0.70) and the episodic memory task (WL, d = 0.64).
Based on subgroup classification by Reliable Change Index 44.8% of patients showed improvement (GG), 47.4% stabilization (NCG), and 7.8% deterioration (LG) with regard to their global cognitive functioning (Table 2), indicating that a large proportion of patients either improved their cognitive scores on admission or remained stable with fewer patients demonstrating declining scores.
Change in cognitive status from admission to discharge, Reliable Change Index Intervals (RCIs) and proportion of change
Presented are change of cognitive performances from admission to discharge (discharge–admission mean values±SD) and p-values for Dependent-Sample t-tests; ahigher scores indicate better performance except of Trail Making Test; magnitude of change is given as Cohen’s d values≥0.2 indicate small, ≥0.5 medium and≥0.8 large effects; SD, standard deviation; CERAD TS, CERAD Total Score; RCI, Reliable Change Index Interval: criterion to evaluate whether a person’s individual change score from admission to discharge is considered as a significant reliable improvement or decline; bclassification into cognitive change groups are made on basis of RCIs: GG, cognitive gain group: exceeding the RCI in a positive direction, NCG, no-change group: falling within the RCI boundaries, LG, loss group: exceeding the RC in a negative direction.
Characteristics of global cognitive change groups
Comparisons between global cognitive change groups indicated no differences at admission for global cognitive functioning, age, sex, depressive symptoms, number of medication, length of stay, or type of dementia. However, patients in the LG showed significantly worse ADL and mobility admission scores and a higher degree of frailty in comparison to both other sub-groups. Additionally, this group showed lower ADL change scores than patients with cognitive stability or improvement (4.1 versus 12.0 and 13.0 respectively) and a trend for higherinstitutionalization rate (Table 3).
Patient’s description and comparison of subgroups for global cognitive change
Total range of scores are given in brackets behind the variable with higher scores indicating less impairment in CERAD TS, MMSE, ADL, HABAM, and PAIR. For frailty and depression higher scores indicate higher degree symptoms; p-values for aunivariate ANOVA, bChi-square, cKruskal-Wallis test applied to test between cognitive change groups; ++significant differences between LG and both other cognitive change groups; +significant difference between LG and GG; CERAD TS, CERAD Total Score; MMSE, Mini-Mental State Examination; PAIR, Physical Activity of Inpatient Rehabilitation Questionnaire; AD, Alzheimer’s disease; VaD, vascular dementia; MD, mixed dementia; ADL, Barthel Activity of daily living; HABAM, Hierarchical Assessment of Balance and Mobility; GG, gain group; NCG, no-change group; LG, loss group; SD, standard deviation.
Association between cognitive and functional change and prediction of ADL change
After controlling for ADL and cognitive admission scores partial correlations indicated significant small to moderate positive associations between ADL change and change in global cognitive functioning (r = 0.23; p = 0.004) as well as episodic memory (WL, r = 0.20; p = 0.01) and executive functioning (VF, r = 0.16; p = 0.05). For all other cognitive change scores, no significant correlations with ADL change was found (Table 4).
Relationship between change in cognitive scores and change in ADL functioning.
Presented are coefficient r and p for partial correlations between change scores in cognition and ADL, controlled for ADL and cognitive admission scores; CERAD TS, CERAD Total Score; ADL, Barthel Activity of daily living.
The two linear models identified global cognitive change (β= 0.32; p = 0.006) and ADL admission score (β= –0.27; p < 0.001) as predictive variables for ADL change (model 1): lower ADL functioning at admission and higher improvements in global cognitive functioning during rehabilitation were associated with higher ADL improvements. The two variables accounted for about 20% of variance in ADL-change (overall R2 = 0.196). In contrast, global cognitive admission scores were not predictive for ADL change (p = 0.15) in model 2 (Table 5).
Prediction of ADL change by cognitive scores and ADL admission scores
Given are coefficients and p-values for 2 linear models using ADL-change scores as dependent variable; β, regression coefficient; R,2 coefficient of determination indicates the proportion of the variance in the dependent variable that is predictable from the independent variables; CI Confidence Interval; ADL, Barthel Activity of daily living.
DISCUSSION
The present study provides relevant results on cognitive change during inpatient rehabilitation and its association with functional rehabilitation success in patients with dementia. Significant improvements could be identified for all cognitive variables during rehabilitation. On an individual level, a highproportion of patients improved or was classified as stable, while only a very small group declined in cognitive performance according to sample-specific, reliable criteria for change. Patients whose cognitive performance declined were characterized by higher functional dependency and frailty at admission. This group showed a trend toward institutionalization after rehabilitation. Positive change in global cognitive functioning as well as in executive and episodic memory function was positively associated with ADL-change. Change in cognitive functioning but not cognitive status on admission was predictive for change in ADL-functioning.
Change of cognitive performance on group and individual level
Our sample showed significant improvements in cognitive functions during rehabilitation. Globalcognitive performance, but also performance in executive functioning, language semantic memory, episodic memory, visuospatial abilities, and speed of information processing, significantly improved. This finding was rather unexpected, as patients with dementia were found to be a highly vulnerable patient group for negative rehabilitation outcomes [5 , 9] and negative patterns of cognitive change after hospitalization were found even in older individuals without profound cognitive impairment on admission [11, 12].
Even if geriatric rehabilitation primarily focuses on improving physical function our results suggest that the structured dementia friendly environment with clear daily routines, early mobilization, physically but also cognitively demanding therapies might have contributed to stabilization and recovery of cognitive dysfunction.
We specified our findings on group level by proportions of change on individual level. In the absence of reliable criteria for meaningful short-term change in our target group we calculated reliable change indices and intervals (RCIs). Reports of change rates are rather unusual in rehabilitation research, even though in combination with the criterion used to determine change, it is the most meaningful information for clinicians to evaluate change in a given patient group. The calculated RCIs for our sample exceeded group mean differences for change by far and represented rather high and conservative cut-offs for improvement or decline. According to these RCIs, a considerable proportion of patients were classified as improved, only a small minority of patients declined in cognitive performance. Different proportions of change were found for the cognitive domains with highest rates of improvement for the composite score of global cognitive functioning, episodic memory, language semantic memory, and executive functioning. Inhomogeneous patterns of change suggest that cognitive effects of hospitalization are global in nature but can affect some cognitive functions more than others.
Our findings are contrary to the results for change rates based on simple scores for global cognition in non-demented patients [21, 22]. Here the authors described similar rates of decline (11%) but considerably lower rates of improvement, in stroke patients (7%) [22] and in older multi-morbid patients as well (35%) [21]. Even though we used conservative criteria for change, 45% of patients in our study improved in global cognitive functioning. This result is encouraging for clinicians working in geriatric rehabilitation and for their patients as well. On the same note, these findings reflect the cognitive burden of acute illness and hospitalization in dementia patient as gains should not be interpreted as an amelioration of the dementia immanent cognitive impairment but rather as a sign of recovery from the negative, symptom-promoting impact of acute illness and/or from hospitalization [16]. This clinical phenomenon has been described by Inouye and other groups [44, 45]who found cognitive improvements in 39% of their older patients, with a considerably higher proportion among their patients with dementia (55%), suggesting a higher vulnerability in this patient group. Our results exceed the latter findings by specifying the phenomenon of cognitive change within a clearly defined study sample of inpatients with diagnosed dementia using validated neuropsychological instruments for the evaluation of improvement, stability or decline in global and domain-specific cognitive performance during geriatric rehabilitation.
Characteristics of global cognitive change groups
Analysis of subgroups according to RCI classification of change revealed no differences between groups in age, depression, or pre-existing delirium according to medical records while these conditions were found to be related with cognitive [21] and functional recovery in other studies [22]. Interestingly cognitive status at admission, the variable most often used to explain rehabilitation success [9 , 18–20] did not differ between subgroups in the present study.
The group with cognitive decline (LG) appeared to be a specific clinical subgroup, characterized by lower ADL and mobility scores and higher frailty scores on admission. Furthermore, the LG was the group with least ADL improvements and showed a trend to a higher rate of patients who could not return home. The lack of significance in this latter outcome may be interpreted as a consequence of the small size of the LG. This aspect should be revaluated in a future study.
Our approach does not allow us to speculate on causality for cognitive change. However, for the present sample of multi-morbid patients with reduced functional and cognitive resources, our results suggest that the high vulnerability and diminished reserve to compensate stressors, which was indicated by higher admission dependency and frailty scores in the LG, might have precipitated the observed cognitive decline in combination with a negative rehabilitation outcome. These factors were found to be associated with negative health outcomes andcognitive decline in other longitudinal studies [46 –48]. For clinicians, this could be an important clue to identify patients at risk for negative outcomes early at admission.
Association between cognitive and functional change and prediction of ADL change
We found significant correlations of change in ADL scores and change scores in global cognitive functioning, executive functions, and episodic memory. Even if these correlations were small to moderate, they indicate that recovery in global and certain specific cognitive domains were not independent from ADL recovery. Global as well as specific cognitive functions contribute differently to ADL functioning. While the authors are not aware of comparable change data from the rehabilitation setting, results are in line with findings in outpatients, where lower status in global as well as executive and memory functions was associated with more substantial errors in everyday functioning, the latter compromising the ability to live independently [49], and predicting lower global scores of ADL [25, 50]. These results indicate global, executive, and memory functions as relevant cognitive sub-domains for ADL-functioning.
Additionally, the two linear models underscore the predictive value of global cognitive change for ADL-recovery, a variable barely noticed as being predictive for ADL-recovery so far. Together with ADL admission scores global cognitive change accounted for about 20% of the variance in ADL gains which confirms the relevance of cognitive for functional change [14] in dementia patients. Nevertheless, it also indicates that there are other important predictors of ADL gains that were not the focus of the present study and therefore were not accounted for in ouranalysis.
Global cognitive admission scores, a predictor of functional rehabilitation outcomes in other studies [7 , 19], did not significantly predict ADL change in the present study. Our results suggest that within a defined range of cognitive impairment (MMSE 17–26), the success of functional rehabilitation can be achieved despite cognitive impairment on admission but that a decline in cognitive function negatively impacts functional recovery. These findings highlight the need to shift the focus of interest from cognitive status to cognitive change as an important predictor for rehabilitation success in patients withdementia.
Limitations
Two limitations with reference to interpretation of cognitive change should be addressed: First, even if the reliable change index approach provides strictly conservative criteria for individual change thussetting the limits high for classification of change, we have to reflect upon confounding influences of practice effects as our test-retest interval is comparatively short. To our knowledge, data about the presence and magnitude of practice effects as well as normative data to correct for these effects among persons with dementia in the CERAD battery are lacking. However, research indicates that persons with cognitive deficits in general do not show marked effects of repeated neuropsychological testing within short [51, 52] or longer re-test intervals [53]. It is suggested, that (other than healthy subjects) persons with dementia do not recall the circumstances and details of the test situation. This failure of helpful recall when being tested for the second time, would even be indicative for cognitive impairment, reaching a critical threshold that overwhelms practice effect [53, 54]. Accordingly, even if we cannot fully exclude practice effects, the magnitude of such an effect, if any, should be very mild and not fundamentally compromise results as the study sample comprises of older persons with dementia typical impairmentsincluding deficits in memory, cognitive adaptability, and flexibility.
Second, although delirium was an exclusion criteria for study participation and although we controlled for differences between change groups due to pre-existing delirium, undetected conditions like sub-syndromal delirium might have influenced some of the presented results.
A weakness in using the Barthel Index Scale as ADL-measure could be a possible ceiling effect in high-functioning persons, what could make it difficult to reliably assess differences in status and change and entails risk of diminished statistical power [55]. However, in our sample, no clustering at the highest possible admission or discharge scores was evident. The same was true for floor effects. Therefore we suppose that such effects did not bias ourfindings.
Future research
The present study has provided empirical data to support future lines of rehabilitation research focusing on cognitive status and its course during rehabilitation. In future studies, additional personal and setting related risk factors as well as protective factors should be identified and reflected in geriatric rehabilitation programs for patients with dementia as secondary diagnosis. Interventions have to take into account the functional and cognitive vulnerability of the patients. A longitudinal study design that would cover the whole course of acute illness, hospitalization, and long-term recovery would help to integrate our findings into a broader framework of rehabilitation for patients with dementia with a special focus on functional and cognitiverecovery.
Conclusions and recommendations
Our results show the high potential to improve global and domain specific cognitive functioning of patients with mild to moderate dementia in geriatric rehabilitation. Change in cognitive status was positively associated with and predictive for ADL recovery regardless of severity of cognitive impairment. Our findings underscore that cognition in patients with dementia cannot be seen as a stable and negligible condition but rather a vulnerable state. It is an independent outcome measure which impacts functional rehabilitation success. Therefore, health care professionals should assess and monitor cognitive functioning in patients with dementia through the whole phase of hospitalization and rehabilitation. The implementation of programs that maintain and enhance cognitive functions in this population should be intensely supported.
Footnotes
ACKNOWLEDGMENTS
We thank Carolin Barz, Christian Bexten, Nils Bruemleve, Andrea Fickelscherer and Sabine Türner for support in data collection and patientrecruitment.
This study was supported by the Baden Württemberg Foundation, the Dietmar-Hopp Foundation. ID was supported by a doctoral research fellowship of the Ministry of Science, Research and the Arts Baden-Württemberg, Germany. The funding source had no role in the design and conduct of the study; collection, management, analyses and interpretation of the data; preparation, review or approval of the manuscript.