
Abstract
Background:
There is currently no effective intervention for improving memory in people at increased risk for dementia. Cognitive training (CT) has been promising, though effects are modest, particularly at follow-up.
Objective:
To investigate whether adjunctive non-invasive brain stimulation (transcranial direct current stimulation, tDCS) could enhance the memory benefits of CT in amnestic mild cognitive impairment (aMCI).
Methods:
Participants with aMCI were randomized to receive CT with either Active tDCS (2 mA for 30 min and 0.016 mA for 30 min) or Sham tDCS (0.016 mA for 60 min) for 15 sessions over a period of 5 weeks in a double-blind, sham-controlled, parallel group clinical trial. The primary outcome measure was the California Verbal Learning Task 2nd Edition.
Results:
68 participants commenced the intervention. Intention-to-treat (ITT) analysis showed that the CT+Active tDCS group significantly improved at post treatment (p = 0.033), and the CT+Sham tDCS group did not (p = 0.050), but there was no difference between groups. At the 3-month follow-up, both groups showed large-sized memory improvements compared to pre-treatment (CT+Active tDCS: p < 0.01, d = 0.99; CT+Sham tDCS: p < 0.01, d = 0.74), although there was no significant difference between groups.
Conclusion:
This study found that CT+Active tDCS did not produce greater memory improvement compared to CT+Sham tDCS. Large-sized memory improvements occurred in both conditions at follow-up. One possible interpretation, based on recent novel findings, is that low intensity tDCS (used as ‘sham’) may have contributed biological effects. Further work should use a completely inert tDCS sham condition.
Keywords
INTRODUCTION
Mild cognitive impairment (MCI) is a syndrome where older individuals show objective and subjective cognitive impairment, although day-to-day functional abilities are relatively intact [1, 2]. Amnestic MCI (aMCI) refers to when memory dysfunction predominates and is usually associated with the highest risk for conversion to dementia [3, 4]. For aMCI, an effective intervention should therefore target memory, with the aim to improve performance to at least within the normal range for that person’s age. However, current evidence shows that no available treatments or interventions meet this standard [5, 6]. As better cognitive functioning is associated with the stability of MCI diagnosis over the longer term [7] and reduced risk of functional dependence [8, 9], improving memory in aMCI is therefore an important step towards slowing cognitive decline and reducing dementia conversion.
Of the studied interventions for MCI, computer administered cognitive training (CT) has shown promise and may be beneficial for improving cognition [1, 10]. CT has advantages that it is relatively inexpensive and can be completed by people at home. A meta-analysis of randomized controlled trials (RCTs) of CT indicated an overall small-sized effect for improving memory at post treatment [5]. These effects, however, tended to be further reduced at follow-ups [5, 11], for example, at 3- and 6-months post intervention. Due to these limitations, recent research has focused on augmentative strategies for enhancing the efficacy of CT, such as non-invasive brain stimulation.
Transcranial direct current stimulation (tDCS) is a safe, non-invasive form of brain stimulation which has demonstrated neuromodulatory effects [12–14]. The technique involves application of a small direct electrical current (usually 1-2 mA) to the brain via electrodes placed upon the scalp. Animal and human studies have shown that the presence of neural activity during tDCS is essential for causing neuroplastic changes following stimulation [15, 16]. Several small RCTs conducted in healthy younger and older adults have found that administering tDCS during CT can produce both enhanced [17, 18] and sustained [19–21] cognitive benefits compared to CT alone. The question of whether this approach has greater efficacy for improving memory in people with aMCI, however, remains unknown.
In this double-blind, sham-controlled RCT we tested whether administering CT during tDCS would cause greater improvement in memory in people with aMCI compared to CT during sham tDCS. Based on the results of preclinical studies, we hypothesized that CT combined with active tDCS would show significantly greater memory improvement compared to CT with sham tDCS. In addition, we predicted that memory benefits of CT with active tDCS would be maintained at 3-months follow-up.
MATERIALS AND METHODS
Trial design
The study used a double-blind, sham-controlled, parallel group, experimental design. Participants were randomized by a computer-generated random number sequence (1 : 1 ratio) to: 1) computer administered cognitive training combined with active tDCS (CT+Active tDCS), or 2) computer administered cognitive training combined with sham tDCS (CT+Sham tDCS). Randomization was stratified based on estimated premorbid IQ (i.e., low average, average, high average, superior) and was assigned according to a computer-generated randomization sequence by the unblinded tDCS treater. Both conditions required attendance for 15 sessions, conducted over 5 weeks (3 sessions per week) at the University of New South Wales, Sydney. To allow for contingencies (e.g., non-attendance due to unforeseen circumstances), participants were allowed to complete a minimum of 2 and maximum 3 sessions in any one week and were required to complete the total 15 sessions. Primary and secondary outcome measures were completed at pre-treatment, post treatment (end of the treatment course), and at 3-months follow-up after the intervention. Participants and assessors were blinded to the participant’s group allocation until the entire study was completed. The blinded assessors were different from the tDCS administrator. The planned sample size for the study was 75 (34 per group+10% attrition). This sample size was calculated to detect a clinically meaningful difference in scores on the primary outcome measure between the two conditions in the study (equivalent to d ≥ 0.7, 2-tailed). The CONSORT diagram is shown in Figure 1. The study was approved by the University of New South Wales Human Research Ethics Committee. The study was registered at clinicaltrials.gov, identifier NCT01653431.

CONSORT Flow Chart.
Participants
Participants were enrolled from January 2013 until January 2018. Inclusion criteria were: aged 60–85 years and a diagnosis of aMCI (single or multiple domain) consistent with published recommendations [22]. Diagnosis of aMCI was based on formal screening by author AM using the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS: 23), the Wechsler Test of Adult Reading (WTAR: 24) as a measure of estimated premorbid IQ, and the Bayer-Instrumental Activities of Daily Living (Bayer-ADL: 25) as a measure of functional status. Participants were permitted to use concomitant medication, although this was required to remain unchanged over the duration of the study. Exclusion criteria were: inability to provide informed consent; medication changes in the two weeks prior to obtaining informed consent; concurrent medication likely to affect mental performance (e.g., benzodiazepines), or treatment with a cholinesterase inhibitor; history of drug or alcohol abuse or dependence current or in the last 3 months; current, diagnosed Axis 1 psychiatric comorbidity (sub-clinical symptoms were permitted) or neurological disorder (apart from aMCI), recent (within last 6 months) head injury, or history of seizure or stroke or serious medical condition likely to affect cognition; or insufficient proficiency in English to complete study procedures. All participants provided written informed consent.
Transcranial direct current stimulation
The anode was placed over the F3 electrode site (overlying the left dorsolateral prefrontal cortex: L-DLPFC) identified on the scalp using an EEG cap based on the 10/20 system) and the cathode over F8 (electrode sizes 5×7 cm, 35 cm2). Conductive rubber electrodes covered by sponges soaked in saline were used, held in place by a head band. Active tDCS involved an initial ramp up over 30 s followed by 30 min at 2 mA. After this, the machine was left on in a default mode (which involved delivery of a continuous current of 0.016 mA) until CT was completed (approximately 45–60 min). For sham tDCS, the current was gradually increased to 1 mA over 30 s and then left on for 30 s before being ramped down over another 30 s. Following this, the machine was similarly left on in default mode until CT was completed so as to not disrupt the session. For both conditions, the device was not turned off to preserve participant blinding. The tDCS administrator was not blinded. The tDCS machine used was an Eldith DC Stimulator (NeuroConn, Germany). Immediately after each session an adverse effects symptom checklist was administered [26]. Blinding was assessed at post treatment by asking participants to guess their tDCS condition.
Computer administered cognitive training
CT was administered using COGPACK (Marker Software, Version 8.1, Germany). This software was chosen because it had previously been found effective for improving memory in older adults [27]. CT included exercises to train skills important for learning and memory (i.e., working memory, processing speed, attention); training on these exercises occurred during the first 30 min of the session. Memory CT tasks were chosen to practice two mnemonic memory strategies (categorization and association) taught prior to the commencement of the first session. The memory CT tasks were commenced in the final 15 min of each session. CT tasks were standardized for each session and included both adaptive tasks and tasks programmed to progressively increase in difficulty across the intervention. CT commenced 5 min after the onset of active or sham tDCS and continued for approximately 45 to 60 min.
Outcome measures
The primary outcome measure was Total Learning T score (age and education adjusted) on the California Verbal Learning Task 2nd Edition (CVLT-II; 28), a non-trained test of verbal memory. Secondary outcomes included: Paired Associates Learning (PAL) and Rapid Visual Information Processing (RVIP) from the CANTAB computerized battery (Cambridge Cognition Limited), Symbol Digit Modalities Task (SDMT: 29), Choice Reaction Time (CRT), Cognitive Failures Questionnaire (CFQ: 30), Bayer-ADL, Montgomery Åsberg Depression Rating Scale (MADRS: 31), and Quality of Life Enjoyment and Satisfaction Questionnaire (Q-LES-Q: 32). For the cognitive outcomes, validated parallel forms were used where available (for CVLT-II, PAL and SDMT).
Statistical analyses
Statistical analyses were conducted using the Statistical Package for the Social Sciences (SPSS) for Windows, Version 22.0 (IBM corp., Armonk, NY). Baseline differences between groups in demographics and the primary outcome were examined using chi-square tests (for categorical variables) or t-tests (for continuous variables). The primary analysis was intention-to-treat (ITT). A secondary per-protocol analysis was conducted for the primary outcome only. Changes in primary and secondary outcomes following the intervention were examined with separate mixed effects models. The models included effects for Condition (i.e., CT+Active and CT+Sham tDCS), Time (pre-treatment, post treatment, 3-month follow-up), and Time by Condition interaction. Subject was included as a random factor. Post hoc pairwise comparisons (Least Significant Difference method) were conducted to interpret main effects. Differences in the frequency of reported non-serious adverse events between conditions were compared with chi-square tests. The integrity of blinding for participants’ guesses (i.e., ‘active’ or ‘sham’) was compared against the assigned intervention with a chi-square test. Statistical tests were two-tailed and significance was set at p < 0.05.
Baseline demographic and clinical data for the ITT sample (N = 68)
CT, computer administered cognitive training; CVLT-II, California Verbal Learning Test – Second Edition.
RESULTS
One hundred and forty-three participants were formally screened against the eligibility criteria (Fig. 1). Following randomization, 4 participants withdrew from the study. Thirty-three participants commenced receiving CT+Active tDCS and 35 participants CT+Sham tDCS. Data from the 68 participants who commenced treatment were included in the ITT analysis. Baseline demographic and clinical characteristics were comparable in the two stimulation conditions; for details, see Table 1.
Primary outcome
In the ITT analysis, verbal memory significantly improved from baseline to post treatment in the CT+Active tDCS group (p = 0.033) and not in the CT+Sham tDCS group (p = 0.05); however, there was no significant Time by Condition interaction. Secondary per-protocol analysis showed significant improvement from baseline to post treatment in both the CT+Active tDCS (p = 0.016) and CT+Sham tDCS (p = 0.037) groups and the Time by Condition interaction was non-significant. Table 2 shows the results from the primary analysis across the entire study period for the ITT sample (N = 68). Post hoc tests showed significant improvement from post treatment to 3-month follow-up in both conditions (Fig. 2). From pre-treatment to 3-months follow-up, significant large-sized memory improvements were observed in both conditions (CT+Active tDCS: Cohen’s d = 0.99; CT+Sham tDCS: d = 0.74).
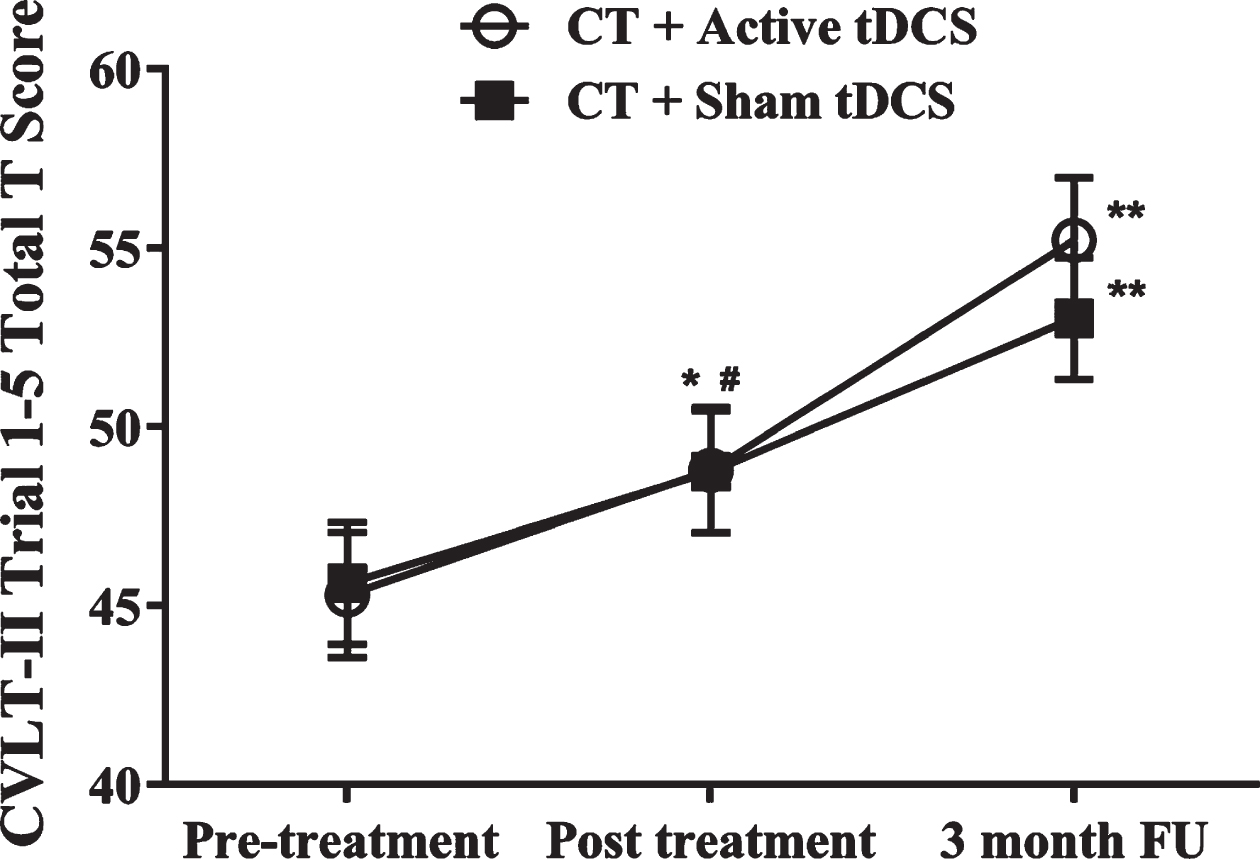
Mean (SE) Change in Verbal Memory by Treatment Group. Change from pre-treatment: *p < 0.05,#p = 0.05. Change from post treatment, **p < 0.01. CVLT-II is the California Verbal Learning Test 2nd Edition.
Cognitive, mood and functional outcomes (Raw means, SD, and ITT analysis)
PAL, Paired Associates Learning; RVIP, Rapid Visual Information Processing; CFQ, Cognitive Failures Questionnaire; Bayer-ADL, Bayer-Instrumental Activities of Daily Living; Q-LES-Q, Quality of Life Enjoyment and Satisfaction Questionnaire; MADRS, Montgomery Åsberg Depression Rating Scale.
Secondary cognitive outcomes
Results for the secondary non-trained cognitive outcomes are shown in Table 2. At 3-months follow-up, significant improvements from pre-treatment were observed for visual memory (PAL), attention and working memory (RVIP), processing speed (SDMT), and subjective cognitive functioning (CFQ). For each of these outcomes, however, there was no significant Time by Condition interactions.
Mood, quality of life, and instrumental activities of daily living
Significant mood improvement was observed in both conditions, although there was no significant Time by Condition interaction (Table 2). Quality of life did not improve across the study period. Instrumental activities of daily living significantly improved in both conditions from pre-treatment to 3-month follow-up, although the Time by Condition interaction was not statistically significant.
Participant blinding
At post treatment, 18/28 (64%) in the CT+Active tDCS group, and 15/31 (48%) in the CT+Sham tDCS group correctly guessed their condition. There was no significant difference between groups (χ2 (1) = 0.97, p = 0.33), indicating that blinding was preserved.
Tolerability
No serious adverse effects were reported. There were no significant differences between conditions in the frequency of the following reported adverse events: redness, tingling, mild burning, pain, nausea, light headedness, headache, blurred vision, fatigue, other (ps > 0.05). For the ITT sample, the most common adverse events reported across all sessions were: tingling (25.9%), redness (16.2%), mild burning (11%), and itching (10.5%).
DISCUSSION
An effective intervention for improving memory in aMCI remains elusive. In this study, we investigated whether combining CT with active tDCS would produce superior memory improvements compared to CT with sham tDCS. Results showed no significant differences between conditions for any outcome, indicating that CT with active tDCS was not superior to CT with sham tDCS. At 3-months follow-up, both conditions showed significant large-sized improvements in verbal memory when compared to pre-treatment (primary outcome).
In both conditions, significant improvements were observed from pre-treatment to post treatment for the non-trained cognitive measures of verbal and visual memory, attention and working memory, and processing speed, as well as subjective cognitive function, mood, and instrumental activities of daily living. These results are in line with studies of CT alone with comparable or larger sample sizes which have shown modest memory and other cognitive improvements from pre to post treatment [11, 34]. Consistent with these studies, the current results showed cognitive improvements of similar magnitude at post treatment, suggesting that there may be no additional benefit from adding active tDCS or sham tDCS. These cognitive gains were then generally maintained or slightly reduced at the 3-month follow-up assessment, similarly to findings of studies of CT alone [5].
The main finding from this study is that tDCS imparted no additional benefit compared to results expected with CT alone. This is consistent with the conclusion from a recent meta-analysis of 7 controlled studies of CT combined with tDCS in healthy adults [35]. The data from sham-controlled studies conducted in clinical samples, however, is limited. A study in participants diagnosed with Parkinson’s disease (n = 22) reported significant cognitive improvements on several tasks following 10 combined CT+tDCS sessions, though found no significant differences between the active and sham conditions [36]. A small double-blind controlled study in participants diagnosed with schizophrenia (n = 10) also reported no significant differences between conditions for clinical outcomes following 10 combined sessions [37]. In contrast, in a pilot study of participants with depression, significantly greater cognitive improvement at 3-weeks follow-up was observed with CT combined with active tDCS compared to both CT with sham CT and sham CT with active tDCS after 5 sessions [38].
Several considerations are pertinent to the main finding of a null outcome. First, it is possible that practice effects on the non-trained cognitive tasks may have contributed to the significant behavioral effects and/or obscured any true between-group effects. The current study employed ‘gold standard’ methods to minimize these effects (i.e., utilizing randomized and counterbalanced alternate test forms and demographically adjusted scores for standardized neuropsychological tests), though practice effects cannot be totally discounted. Another consideration is that the dose of tDCS (2 mA, 30 min, 15 sessions) may not have been optimal. tDCS dosage has been shown to influence stimulation effects (e.g., [39]) and the dose-response curve is complex and likely to be non-linear [40–42]. A further consideration regarding dosage is the sham tDCS approach used in this study. In both conditions, a constant small sized tDCS current (0.016 mA) was delivered during CT for the remainder of each active tDCS session, and for the entire duration of every sham tDCS session. This was due to the tDCS device being left ‘on’ in a default setting, as switching the tDCS machine ‘off’ during the session could have compromised participant blinding and disrupted the CT session. A recent large clinical trial of tDCS in depression used a similar very low intensity sham condition and found significant therapeutic effects [43]. A subsequent study then showed that this level of stimulation had biological effects [44]. These findings are recent and novel, are yet to be replicated, and were not known at the time this study was designed. Thus, it is possible that, in this study, the ‘sham’ condition may have had some biological effects.
Interestingly for the primary outcome (verbal memory), significant delayed improvements were observed after the intervention in both conditions. This additional improvement resulted in overall clinically significant mean improvements for verbal memory (i.e., effect sizes > 0.7) in both conditions, which is equivalent to ‘normalizing’ memory functioning for people with an aMCI diagnosis [23]. This effect was specific to verbal memory, with limited or no further improvements observed for the secondary cognitive outcomes. It is in contrast to prior studies of CT alone, where improvements following CT tend to decrease over time at follow-up assessments in the absence of either further intervention or booster sessions [5, 34]. It is speculative but possible that this delayed verbal memory improvement may have been due to the combined intervention (CT with active or sham (low intensity) tDCS). Interestingly, other studies of CT with tDCS in healthy and other clinical populations have similarly observed delayed cognitive effects at follow-up assessments after the intervention [20, 38]. Notwithstanding, in the absence of additional control conditions, the possibility that this delayed verbal memory improvement or other cognitive improvements were due to practice and/or non-specific study effects cannot be ruled out.
Limitations to this study include that both conditions involved CT administered with tDCS, which may have affected treatment outcomes. We therefore cannot conclude that CT with tDCS is not superior to CT without tDCS. Further, the sample size was relatively modest. Notwithstanding, to the best of our knowledge this is the largest trial to-date to investigate this combined approach in a clinical sample.
Conclusions
Both groups significantly improved over the treatment period; however, CT with active tDCS was not superior to CT with sham tDCS for improving memory in aMCI. Unexpectedly, further improvement in verbal memory occurred in both groups over the 3-month follow-up period, suggesting further research into this combined intervention is warranted. Future study of this combined intervention would benefit from employing a factorial study design (i.e., also including ‘sham CT and active tDCS’ and ‘sham CT and sham (inert) tDCS’ conditions), or alternatively including an ‘inert tDCS’, a different tDCS condition (e.g., a different stimulation duration or electrode montage), or a ‘sham CT’ condition as controls.
Trial Registration
Clinicaltrials.gov identifier NCT01653431.
Footnotes
ACKNOWLEDGMENTS
This work was funded by the Dementia Australia Research Foundation, the Thomas Foundation and the Centre for Healthy Brain Ageing (CHeBA). The authors would like to thank the research assistants Bronwyn Hegarty, Jessica Elmasry, Kevin Yeung and Nicholas Chand for their assistance with data collection. We thank all participants for their contribution to the study.