
Abstract
Background:
White matter hyperintensities (WMHs) are related to cognitive dysfunction in the general population. The clinical relevance of WMHs in patients with Alzheimer’s disease (AD) and mild cognitive impairment (MCI) is, however, unclear.
Objective:
This meta-analysis aimed to quantify the association of WMHs and specific cognitive domains in patients with MCI or AD.
Methods:
PubMed (January 1990-January 2017) was searched for studies that used MRI to quantify WMHs, and measured cognitive functioning (≥1 predefined cognitive domain with ≥1 test) in a well-defined population of persons diagnosed with MCI or AD. Fischer’s Z was used as the common metric for effect size. Modifying effects of demographics, MMSE, and WMH location were examined.
Results:
Twelve cross-sectional studies on AD (total n = 1,370, median age 75 years) and 10 studies on MCI (9 cross-sectional, 1 longitudinal; total n = 2,286, median age 73 years) were included. The association between WMHs and overall cognition was significantly stronger for MCI (–0.25, –0.36 to –0.14) than for AD (–0.11, –0.14 to –0.08; QM = 10.7, p < 0.05). For both groups, largest effect sizes were found in attention and executive functions (–0.26, –0.36 to –0.15) and processing speed (–0.21, –0.35 to –0.12). No significant modifying effects of age and gender were found.
Conclusion:
WMHs have a medium-sized association with different cognitive functions in patients with MCI and a small, but statistically significant, association with cognition in AD. These result underscore the role of co-occurring vascular brain damage in MCI and AD.
Keywords
INTRODUCTION
White matter hyperintensities of presumed vascular origin (WMHs) are considered the most common marker of small vessel disease in the brain and are frequently found on brain MRI in the elderly [1]. Characterizing the impact of WMHs on cognitive functioning is of growing interest. In the general population, WMHs are associated with a small but consistent negative effect on cognitive functioning across different cognitive domains [2]. WMHs are also associated with an increased risk of developing Alzheimer’s disease (AD) [3]. Pathological evidence suggests that WMHs may play a role in the clinical symptoms of AD as individuals with WMHs require a lower neuropathological AD burden to develop cognitive impairment or dementia [4 –6]. There is also observational evidence of a synergistic contribution of both medial temporal lobe atrophy (MTA) and WMHs on cognitive impairment and dementia severity in AD [7]. This suggests that the presence of WMHs may modify the clinical phenotype of AD [8, 9].
Studies on the clinical significance of WMHs in patients with mild cognitive impairment (MCI) and AD have reported mixed results. Several studies suggest that patients with MCI or (early) AD and concurrent WMHs show greater cognitive dysfunction, particularly in executive functioning, compared to those with a low WMH burden [10, 11]. WMHs may predict conversion from MCI to AD [12] and have been associated with faster cognitive decline in patients with AD [11]. In contrast, other studies show no apparent association between WMHs and occurrence or progression of cognitive decline in AD [13]. Possibly, WMHs affect cognition in the early, but not the later stages of AD [5, 14], which might result of an increase of the relative influence of cortical atrophy on cognition compared with that of WMHs in the later stage of AD. An alternative explanation for these conflicting results may be that a clinical diagnosis of (probable) AD should not be made when there is evidence of substantial concomitant cerebrovascular disease, such as the presence of multiple or extensive infarcts or severe white matter hyperintensity burden [15] resulting in a possible underestimation of the effect of WMHs on cognition in AD. WMHs are, however a common radiological finding in older persons, both with and without AD and the relation with cognition in those patients with established cognitive impairment is not fully understood. The cognitive profile generally considered to be associated with WMHs is that of frontal-lobe dysfunction with impairments mainly in processing speed and executive functioning [16], possibly caused by disruption of interneuronal connectivity thought to be crucial to these cognitive processes [17]. Similar associations have been reported in patients with AD [7, 18] but the potential impact on other cognitive functions (memory performance in particular) has not been examined in detail. A previous meta-analysis in nondemented persons show that WMHs are not only associated with speed and executive functioning, but to a similar extent also with memory, language and visuoperception [2]. Whether this more global, diffuse profile of cognitive impairment is also present in patient with dementia remains to be evaluated.
In all, the role of WMHs in cognitive functioning in patients with MCI and AD is unclear. This meta-analysis therefore aims to provide an overview of the size and nature of the association between WMHs and specific cognitive domains in persons with MCI or AD.
MATERIALS AND METHODS
Study selection
This meta-analysis aimed to include all published studies that provided an estimate of domain-specific cognitive functioning related to the presence of WMHs in a well-defined sample of persons with MCI or dementia of the Alzheimer type. The analysis was performed according to the methodology of the PRISMA statement [19, 20]. PubMed (1 January 1990 to 1 January 2017) and bibliographies from included papers were used to identify relevant publications. The literature search was limited to papers that were written in English and concerned humans. The following search terms were used in full or truncated versions: “white matter hyperintensities”, “white matter lesions”, “WML”, “WMH”, “WMHI”, “small vessel disease”, “SVD” or “leukoaraiosis” in combination with “cognition”, “Mild Cognitive Impairment”, “MCI”, “dementia” or “Alzheimer”. Titles and abstracts were scanned and potentially eligible papers were collected in full-text versions. Reference lists were inspected for additional papers. RPK and EvdB independently judged eligible papers according to the inclusion criteria. In case of disagreement a consensus judgment was made.
All cross-sectional and longitudinal studies were included if they 1) concerned cerebral WMHs, 2) used MRI to identify and quantify the WMHs, 3) addressed one or more predefined cognitive domains with one or more validated neuropsychological tests in 4) a well-defined sample of persons with MCI or AD, and 5) adjusted the analysis or matched the exposed and un-exposed groups for the basic confounders age, sex and level of education. Studies that assessed cognitive functioning with a global screening instrument, such as the Mini-Mental State Examination (MMSE), or reported a composite measure of cognition only were not included. Figure 1 shows a flow chart of the search.
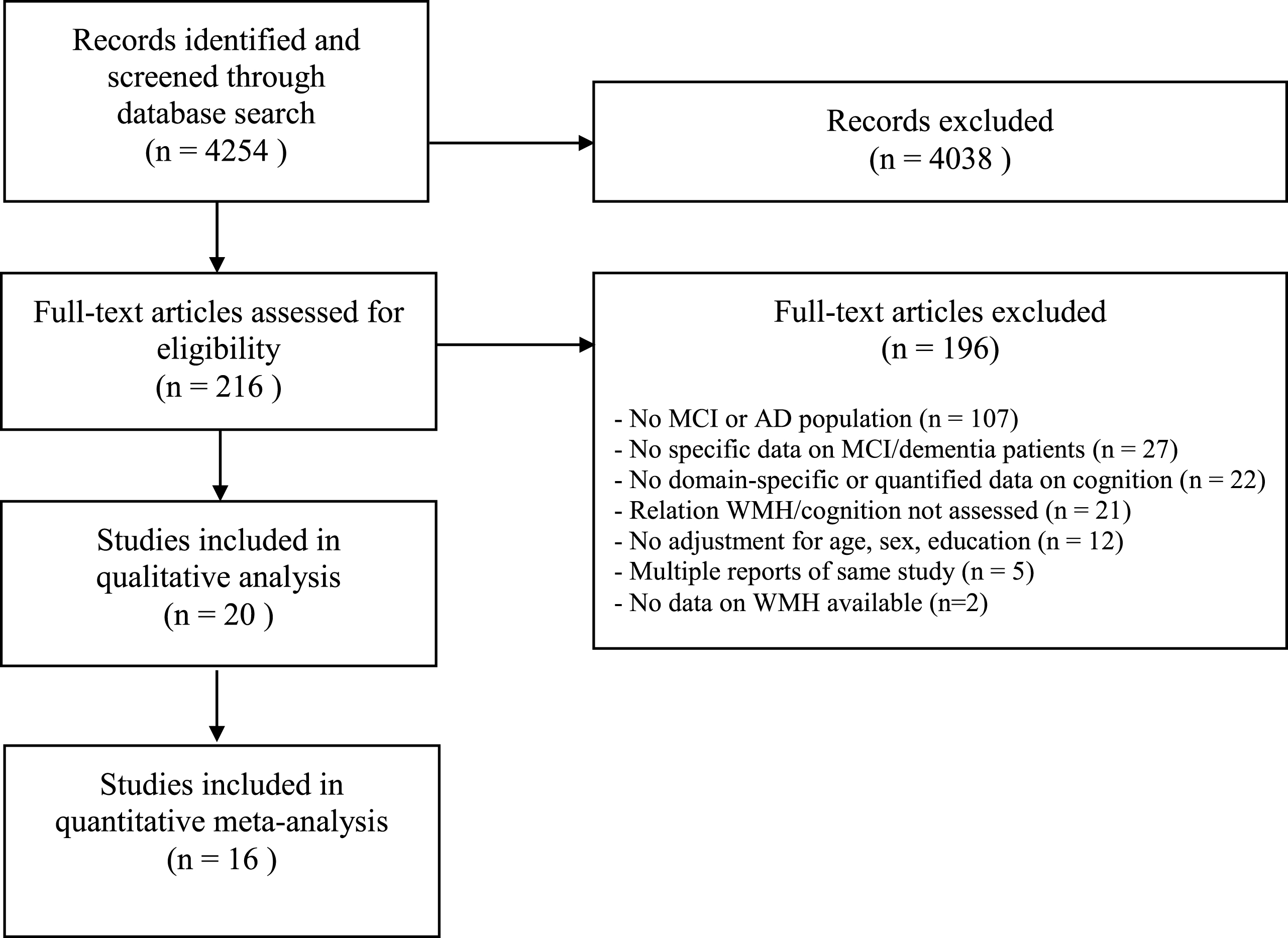
Flow-chart literature search.
The present review focuses on the relation between WMHs and cognition in MCI and AD. When studies included a mixed MCI/dementia sample (without providing data for the specific subgroups separately), the study was included in either the dementia-group or the MCI-group, based on the diagnosis of the majority of included patients. Studies in samples with vascular dementia (VaD) or patient samples including both patients with AD and patients with VaD were excluded. Samples of patients that were selected based on a specific (vascular) risk factor or disorder, such as diabetes, hypertension, or Parkinson’s disease were excluded. In most studies, patients with a history of (major) stroke were excluded. When more than one paper reported on the same population (i.e., Clinical Research Center for Dementia of South Korea (CREDOS) trial), the paper with the largest sample size and/or the most detailed information on WMHs and/or cognitive functioning was included.
Data extraction and data-analysis
Data on the design, sample size, and demographics of the included studies were extracted by two observers (RPK and EvdB), as well as characteristics of the imaging, MCI or AD diagnosis, definition of the WMHs and definition of the cognitive outcome measures (Tables 1 and 2). Quantifiable data on the relation between WMH and cognition were extracted. Given considerable heterogeneity in data presentation, Pearson’s or Spearman’s r was used as the common metric for the effect size across studies as correlations can be calculated from most types of data. Negative correlation coefficients indicate that WMHs were associated with worse cognitive performance. When r was not reported it was calculated from available means and standard deviations, exact values of p, F, T and regression coefficients [21]. To normalize the distribution and to make the effect sizes amenable to parametric statistical analysis, Fisher’s z transformation was performed on each r (z = 1/2 ln [(1+r)/(1-r)]) [22]. All analyses were conducted on Fisher’s z scores. A common guideline for interpretation of correlation coefficients in (neuro)psychological studies is: small effect size, r = 0.1 –0.23 (i.e., 1–5% explained variance); medium, r = 0.24–0.36 (5–13% explained variance); large, r = 0.37 (>13% explained variance) orlarger [23].
Characteristics of cross-sectional studies in dementia
ns, not specified; WMH, white matter hyperintensities; MMSE, mini mental-state examination; AD, Alzheimer’s disease; aMCI, amnestic mild cognitive impairment; PV, periventricular; SOB, sum of boxes; CHAP, Chicago Health and Aging Project; ICV, intracranial volume; a Clinical Dementia Rating presented as mean score (0–2) or total score defined as sum of boxes; b Dichotomous score defined as present/absent or ordinal score defined as no/minimal/moderate/severe, Continuous score defined as WMH expressed in ml or visual rating score; c WMH severity expressed as mean (±sd) volume in ml, mean (±sd) % of intracranial volume, mean (±sd) visual rating or otherwise specified; c All included studies adjusted for or matched on age, sex and educational level, additional adjustments are listed.
Characteristics of cross-sectional studies in mild cognitive impairment
ns, not specified; WMH, white matter hyperintensities; MMSE, mini mental-state examination; MCI, mild cognitive impairment; aMCI, amnestic mild cognitive impairment; PV, periventricular; DWMH, deep with matter hyperintensities; CREDOS, Clinical Research Center for Dementia of South Korea; aClinical Dementia Rating presented as mean score (0–2) or total score defined as sum of boxes; bDichotomous score defined as present/absent or ordinal score defined as no/minimal/moderate/severe, Continuous score defined as WMH expressed in ml or visual rating score; cWMH severity expressed as mean (±sd) volume in ml, mean (±sd) % of intracranial volume, mean (±sd) visual rating or otherwise specified; cAll included studies adjusted for or matched on age, sex and educational level, additional adjustments are listed.
The included studies used variable classification of cognitive domains, therefore, all tests were regrouped into the domains general intelligence, memory, processing speed, attention and executive function, perception/construction, and language according to a predefined classification of tests per domain [24], see Supplementary Table 1.
In the meta-analysis, an overall r value (and 95% confidence interval (CI)) was calculated based on all available correlation coefficients, expressing the magnitude of associations across studies, weighted for sample size [25]. Stouffer’s Z provided an indication of the statistical significance of the effect. In addition, the overall effect size was used in a random effects model to determine the total heterogeneity of the effect sizes (Q T ) and tested against the χ 2 distribution (with n-1 degrees of freedom) [26]. A significant Q T implies heterogeneity. The I2 statistic was also calculated to quantify the percentage of total variation across studies due to heterogeneity [27]. To explore publication bias, the fail-safe number N R was computed (Rosenthal’s method: α <0.05). All analyses were performed with MetaWin version 2.0 [28].
The difference between the overall effect size for MCI versus AD and for the individual cognitive domains was examined with the Q-statistic (Q M ), determining whether or not there is a difference among group means. It is performed by partitioning the total heterogeneity Q T in the variation in effect sizes explained by the model (Q M ) and residual error variance unexplained by the model. A significant Q M implies a difference between the cumulative effect sizes for MCI versus AD and for the individual cognitive domains [25]. In secondary analysis, potentially modifying effects of age, MMSE-score, WMH definition, and WMH volume were explored in a similar fashion.
RESULTS
The search yielded 4,254 studies. Twenty studies met the inclusion criteria (19 cross sectional, 1 longitudinal). Ten studies included patients with AD only, 8 studies included only patients with MCI, and two studies include both patients with AD and patients with MCI. The total number of participants was 3,656 including 1,370 AD patients and 2,286 participants with MCI. Characteristics of the included studies are shown in Tables 1 and 2. AD diagnosis was mostly based on the criteria by McKhann et al. [15] (5 probable AD, 2 probable or possible AD, 5 not specified). Dementia severity varied, but overall severity was mild to moderate (Clinical Dementia Rating <2; median MMSE = 22, range 13–26). Seven out of 10 studies on MCI focused on patients with amnestic MCI, mostly based on the criteria by Petersen et al. [29, 30]. Median age was 75 (range 67 to 81) in AD studies and 73 (66 to 76) in MCI studies.
WMHs were either measured with a visual rating scale (64% of the studies), such as the Fazekas, Scheltens, or Junque scale [31 –33], or with (semi)-automated volumetric segmentation techniques (36% of the studies).
Memory and attention and executive functioning were the domains that were examined most frequently (Table 3), including 1,294 and 1,213 participants with AD and 1,949 and 2,286 participants with MCI for these domains, respectively. The domains general intelligence, processing speed, perception/construction and language were examined less frequently, including 76, 578, 261, and 685 participants with AD and 0, 240, 1,628, and 1,711 participants with MCI, respectively. From 2 AD studies and 4 MCI studies, no quantitative estimate of effect size could be calculated. The results of these studies were presented by means of direction of effect in Table 3.
Results of cross-sectional studies on the relation between white matter hyperintensities and cognitive functioning
Data are presented as Pearson’s correlation coefficient, negative coefficients indicate that greater prevalence and severity of WMH is associated with worse cognitive performance. cognitive domain not evaluated; - greater prevalence and severity of WMH is significantly associated with worse cognitive performance; = no significant association between prevalence and severity of WMH and cognitive performance.
Association between WMH and cognition in MCI and dementia
The overall weighted effect size of the association between WMHs and cognition in all cognitive domains and for MCI and AD taken together was -0.16 (95% CI –0.22 to –0.12). The test for heterogeneity was not significant (Q T = 44.2, p = 0.59, I2 = 0%). The fail-safe number of studies was 648.9, indicating that at least 649 unpublished null-findings were needed to render the effects of WMH on cognition statistically non-significant. There was a significantly larger association between WMHs and cognition for MCI (–0.25, 95% CI –0.36 to –0.14, I2 = 0%) than for AD (–0.11, 95% CI –0.14 to –0.08, I2 = 0%; QM = 10.7, p < 0.05).
One included study had a longitudinal design [34]. The results of this study showed that in 337 patients with MCI (mean age 69.4±7.9; MMSE 27.1±2.1) the presence of WMH was significantly associated with decline in executive functioning over 3 years.
Effect on individual cognitive domains
Table 3 and Fig. 2 show the effects for individual cognitive domains. The overall effect sizes for each domain ranged from small to medium-size. Effect sizes tended to be largest for attention & executive functions (–0.26, 95% –0.36 to –0.15) and processing speed (–0.21, 95% –0.35 to –0.12). Smaller effect sizes were shown for memory (–0.10, 95% CI –0.15 to –0.07), visuoconstruction (–0.13, 95% CI –0.33 to 0) and language (–0.06, 95% CI –0.12 to 0.07). The Q-statistic showed that there was no overall significant difference in effect size between the individual cognitive domains (QM = 7.6, p = 0.12). Post hoc pairwise comparisons indicated a larger effect for attention and executive functions compared to memory (QM = 5.5, p < 0.05) and language (QM = 4.2, p < 0.05), but no other statistically significant differences (all p > 0.05).

Results of the quantitative meta-analysis for AD (upper panel) and MCI (lower panel).
Analysis of demographics and WMH location
There was no modifying effect of mean age or gender distribution of the study population on the relation between WMHs and cognition. Analogous to the results of the primary analysis on the difference between MCI and dementia, studies with a higher mean MMSE score showed larger effect sizes (Q M of slope = –0.01 (standard error 0.006), p < 0.05). There was a (modest) threshold effect, indicating larger effect sizes in studies with a mean MMSE score >24 points (–0.23, 95% CI –0.32 to –0.0.16 versus –0.10, 95% CI –0.13 to –0.06) for studies with mean MMSE ≤24 (p < 0.05).
Although the effect size was larger for the volumetric mode (r=–0.21, 95% CI –0.32 to –0.12) than for the visual mode (–0.13, 95% CI –0.17 to –0.09) there was no statistically significant modifying effect of WMH measurement (Q M = 1.38, p = 0.27). The potential modifying effect of WMH volume (Tables 1 and 2) could not be analyzed because of heterogeneity in data presentation (either as volume in ml, % of intracranial volume, visual rating score or proportion of participants classified as ‘severe’ by theauthors).
Ten studies provided data on the relation between WMH location and cognitive functioning (Table 4). The majority of these studies (8/10) distinguished periventricular and deep or subcortical WMHs. One study examined WMHs is different regions of the brain (e.g., frontal, parietal, temporal, occipital) and one study presented data for WMHs in three pre-defined networks. Due to considerable variability in data presentation meta-analysis was not feasible. Descriptive analysis showed a significant relation between cognition and WMHs in periventricular, but not subcortical/deep regions in 4 studies. With regard to specific cognitive functions the strongest relations were found for measures of executive functioning.
Relation between WMH location and cognitive functioning
+, relation between WMH location and cognition; –, no relation between WHM location and cognition; PV, periventricular; SC, subcortical; D, deep; CS, centrum semiovale; BG, basal ganglia.
DISCUSSION
This meta-analysis showed that the presence of WMHs is associated with a medium-sized decrease in cognitive functioning in patients with MCI and a small decrease in AD. These effects were observed across different cognitive domains.
In the general population WMHs have a small but consistent negative association with cognitive functioning across different cognitive domains [2]. The present meta-analysis showed that WMHs are also associated with cognitive functioning in persons with MCI or AD. This finding underscores the importance of mixed pathologies in these patients. Indeed, there is increasing awareness that presence of other pathologies, in many cases vascular lesions, is the rule rather than the exception in patients with pathologically proven AD [35]. While the association with vascular brain disease by no means negates the importance of neurodegenerative mechanisms in AD, an additive or even synergistic association between vascular and neurodegenerative mechanisms may be hypothesized [36]. Recent results in autosomal dominant AD event suggest that WMHs are a core feature of AD [37]. Vascular brain damage could be additive to concomitant AD pathology in producing more severe cognitive dysfunction than either process alone. Indeed, in a mixed sample of cognitively normal, MCI and AD patients the presence of WMHs predict 1-year decline in MMSE score, irrespective of key MRI markers of AD [38]; see also [8, 9]. In our analysis, one longitudinal study met the inclusion criteria. The prognostic value of WMHs in the progression of cognitive decline in persons with established cognitive impairment thus needs further evaluation. Previous studies, using a cognitive screening instrument only, showed that the presence of WMHs is indeed associated with cognitive decline in patients with MCI [10] or AD [39].
With regard to the cognitive functions that are affected, our domain-specific analysis showed that the association between WMHs and cognition was present across different domains. Although the overall analysis showed no statistically significant difference between the domains, post hoc pairwise comparisons indicated the largest effect sizes for attention and executive functioning, a cognitive domain that is traditionally associated with vascular brain damage. Interestingly, there was also a significant association with the memory domain, which is more closely related to AD.
Data on the effect of WMH volume or location on cognitive functioning were limited and heterogeneous in nature. Our analysis suggests that periventricular WMHs are more strongly related to cognition than subcortical/deep WMHs. This finding is similar to what is found in the general population [2]. The previous suggestion of a threshold effect on cognition when >3% of the white matter is damaged [40] could not be tested in the present analysis.
Several limitations of this meta-analysis have to be discussed. First, considerable heterogeneity between the included studies existed, for example in the way WMHs are measured, defined or analyzed. For this reason, we used strict inclusion criteria to eliminate as much heterogeneity as reasonably possible, resulting in nonsignificant heterogeneity and I2 values of 0%. Second, the studies in this meta-analysis included patients with AD or MCI and our results are thus only applicable to these populations. Very few studies have thus far looked at the impact of WMH on cognition in other dementia subtypes, such as fronto-temporal dementia or Lewy body dementia [41, 42]. Moreover, not all persons with (amnestic) MCI progress to AD and the etiology of the nonanmnestic MCI participants (3 out of 9 included studies) is unknown. Third, the present meta-analysis is observational in nature and no causal relation between WMHs and cognition can be inferred. The relative contribution of WMH and AD pathology cannot be disentangled based on the present meta-analysis and although a synergistic contribution of WMH and AD pathology has been suggested [7] no such effects can be inferred from the present analysis. One could hypothesize that WMHs are merely an etiological marker for other small vessels disease pathologies, including microbleeds, lacunes or micro-infarcts. Fourth, although the effect sizes were similar across different cognitive domains, there was indeed a selection bias where >90% of the studies assessed memory and executive functioning, but only 33% assessed perception/construction and 5% assessed general intelligence. Nevertheless, this does not negate a possible additional effect of vascular brain damage on cognition in patients with AD. Fifth, the risk of both AD and cerebrovascular disease differs with race/ethnicity but this potentially modifying variable was not specifically examined in the studies included in our meta-analysis. Finally, our analysis did not allow for comparison of the individual cognitive processes that comprise a broader cognitive domain (for example working memory versus episodic memory processes or semantic versus letter fluency) that could be differentially impacted by vascular or neurodegenerative changes in the brain.
The finding that WMHs contribute to cognitive dysfunction in patients with AD might offer opportunities for treatment and prevention strategies. Indeed, vascular care in patients with AD with vascular brain damage slows the progression of WMHs [43]. Whether this in turn prevents or delays cognitive decline is to date unknown. Timing of such an intervention is probably an important modifying factor [44].
In sum, this meta-analysis showed a medium-sized association between WMHs and cognitive functioning in patients with MCI and a small, but consistent association in those with AD. These effects were observed across all major cognitive domains. These results underscore the role of vascular brain damage in the clinical presentation of dementia, also in the context of other neurodegenerative pathologies, but more data are needed with regard to progression, extent and location of the WMHs.
DISCLOSURE STATEMENT
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/17-0573r2).