
Abstract
Background:
An improved understanding of the role of neuropsychiatric symptoms (NPS) in the course of Alzheimer’s disease (AD) has recently emerged. NPS lead to hospitalization and caregiver stress, but are more variable during the course of the disease than other symptoms. Knowledge about the role of specific NPS in disease progression and prognosis is especially limited.
Objectives:
To examine the relationship between specific NPS and AD severity during a 5-year follow-up period, and to determine which baseline NPS predict AD progression.
Methods:
236 persons with very mild (CDR 0.5) or mild (CDR 1) AD at baseline and their caregivers were followed up for five years as part of the ALSOVA study. The Neuropsychiatric Inventory was used to assess NPS, and AD severity progression was measured with the Clinical Dementia Rating Sum of Boxes. Data was analyzed with Generalized Estimated Equations and Linear Mixed Models.
Results:
The baseline NPS that best predicted AD progression were delusions, agitation, and aberrant motor behavior, while AD severity during follow-up was associated with hallucinations, delusions, agitation, apathy, aberrant motor behavior, and sleep and appetite disturbances.
Conclusions:
Persons with mild AD presenting delusions, agitation, and aberrant motor behavior at the time of diagnosis could have a more rapidly progressing disease, and some NPS are associated with AD severity. These results highlight the importance of evaluating NPS at the time of AD diagnosis, and the need to offer additional support to persons presenting delusions, agitation and aberrant motor behavior, and their caregivers.
INTRODUCTION
A better understanding for the role of neuropsychiatric symptoms (NPS) in the course of Alzheimer’s disease (AD) has emerged during recent years. In contrast to previous assumptions that NPS were observed only in more severe stages of AD, we now know that they appear frequently in very early and even prodromal phases of the disease [1–3]. NPS typically get worse as AD progresses, but also fluctuate during the course of the disease more than other symptoms [3]. Eventually they affect almost all persons with AD [4] and are associated with caregiver stress, early nursing home placement, and hospitalization [5]. While imaging has revealed some of the underlying neurobiological causes for the occurrence of NPS in AD, the relationship between primary AD pathology and NPS remains unclear [4]. Dillon et al. [3] summarize that NPS probably arise through interaction among psychological, social, and biological causes.
The Neuropsychiatric Inventory (NPI) [6] is the most commonly used scale for assessing NPS in cognitive disorders, allowing for the assessment of a broad spectrum of neuropsychiatric symptoms [3]. Although NPI has reasonably good validity and reliability [3], there is limited information about its positive and negative predictive values and responsiveness [7]. While several studies have explored the NPI factor structure, their results were variable, possibly related to differences in the populations included in the studies [7–9]. Thus, the information provided in the item scores may be more relevant than the overall score because NPI items have little correlation with one another [7] and different symptoms have different trajectories [10].
Although the prevalence of NPS varies widely across different studies, the most frequent symptom observed in persons with AD is apathy, followed by depression, aggression, anxiety, and sleep disorders, and the least common symptom is euphoria [11].
As a whole, the prevalence and severity of NPS tends to increase during the course AD [11, 12]; however, the appearance of separate symptoms vary during the course of AD and between studies. Differences for example in disease duration, age, education, the severity of cognitive impairment, and evaluation method are factors explaining the heterogeneity observed in the prevalence of specific symptoms between studies [11].
The number or severity of neuropsychiatric symptoms at baseline has been associated with rapid AD progression [13–18]. Faster progression of dementia has been associated with psychotic and affective symptoms, hallucinations, and agitation [13, 18-20]. Instead, psychotic and maniac symptoms have been associated with faster cognitive decline [14, 19]. In other studies, sleep disturbances [21], apathy [21, 22], affective symptoms [16], hallucinations [22], and psychotic symptoms [14] were associated with functional decline. Longitudinal trajectories of apathy, aberrant motor behavior, and sleep disorders have been found to be highly reliable predictors for mortality [23]. Apathy was the strongest neuropsychiatric predictor of time to death, which supports its role in the pathogenesis of the disorder.
Previous studies have analyzed the relationship of NPS and AD severity with cross-sectional data, or reported the progression of NPS during a follow-up. However, given the individual variability in the course of AD, it could be more useful to evaluate NPS in relation to AD severity during follow-up.
AD diagnostics have substantially improved, but research and clinical practice have not focused on care after diagnosis. There is still no medication that can enhance memory or intercept AD processes, but recognizing and treating NPS at the time of diagnosis and throughout the course of the disease could promote the well-being of persons with AD and their families. Unfortunately, there is limited knowledge of the appearance of specific NPS on AD progression, and their prognostic value.
Our aims are to identify which patient related clinical characteristics (e.g., gender, age) are associated with the progression of NPS, to determine which baseline NPS may predict the progression of AD and which NPS are associated with AD severity during the 5-year follow-up period.
METHODS
Subjects
This study is a part of the ALSOVA follow-up study. The ALSOVA study was designed to examine the effects of early rehabilitation for persons with very mild or mild AD and their caregivers on the institutionalization but also to investigate AD progression and evaluate monitoring methods [24].
This study included 236 persons with very mild (Clinical Dementia Rating (CDR) 0.5) or mild (CDR 1) AD and their caregivers from three Finnish hospital districts. The participants were recruited within one year of AD diagnosis, from April 2002 to September 2006. The last follow-up visits concluded during the year 2011. Subjects were diagnosed with AD according to the criteria set by the National Institute of Neurological and Communicative Disorders and Stroke and Alzheimer’s Disease and Related Disorders Association (NINCDS-ADRDA) [25] and the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) [26]. Subjects were diagnosed in the memory clinic by a geriatrician or a neurologist, and diagnoses were verified by a study neurologist. All subjects went through diagnostic evaluation including brain imaging (CT or MRI), and were advised to initiate AD-targeted drug therapy at the time of diagnosis or at the baseline visit. Inclusion criteria for participants were very mild (CDR 0.5) or mild (CDR 1) AD at baseline, age ≥65, fluency in Finnish, and the absence of co-morbid conditions influencing cognition. Subjects and their caregivers participated in annual study visits with a study nurse and a psychologist. End-points of the study were institutionalization and death. A detailed description of the study design is presented in our previous papers [24].
Measures
The neuropsychiatric inventory (NPI) is a structured interview designed to obtain data from the caregiver or other informant. The NPI includes twelve behavioral and psychological domains that are typically related to AD: delusions, hallucinations, agitation, anxiety, depression, apathy, disinhibition, irritability, euphoria, aberrant motor behavior, sleep disturbances, and appetite disturbances. The caregiver is asked whether every NPS domain is present, and the severity (1 = mild, 2 = moderate, 3 = severe) and frequency (1 = less than once a week, 2 = once a week, 3 = several times in week, 4 = daily or continuously) of each relevant domain is scored. Both dichotomous (not present/present) and continuous (severity x frequency) are used. The symptoms were considered as “present” if it got other value than zero, that is even it was mild or present less than once a week.
CDR is a scale based on a semi-structured interview and was developed to stage the severity of AD in clinical and research settings [27–29]. It is a commonly used instrument that provides a global score (0.5 = questionable, 1 = mild, 2 = moderate, or 3 = severe dementia) as well as a more detailed quantitative index, the CDR sum of boxes score (CDR-sb; range 0–18). The CDR-sb is calculated by adding the score (0–3) of six domains (memory, orientation, problem solving, community affairs, home and hobbies, self-care). It combines information obtained from the caregiver or other informant with that obtained from the person with AD, and track changes that have emerged from the person’s previous level due to cognitive problems. In our analysis, the CDR-sb score was used as an index of AD progression.
Statistical analyses
Descriptive statistical methods such as means and percentages were used to characterize the data. To analyze which baseline characteristics are associated with the progression of NPS, a linear-mixed effect model for repeated measures was used. The NPI total score was log-transformed to correct skewness of the variable. A value of one was added to the NPI score before transformation because the minimum value was zero. To find the best predictors, the association of all selected variables was analyzed with univariate analyses separately, then multivariate analysis was conducted by reducing variables until only statistically significant variables remained.
To analyze which baseline NPS are associated with the progression of the disease, a generalized estimated equations model (GEE) with a normal probability distribution, identity link function, and unstructured correlation matrix structure was used. The association of all neuropsychiatric symptoms was analyzed with univariate analysis separately, then multivariate analysis was conducted by reducing least significant variables one by one until all were statistically significant to find the best symptom combination. Quasi-Likelihood under Independence Model Criterion (QIC) and Corrected Quasi-Likelihood under Independence Model Criterion (QICC) were used to compare models.
To analyze which NPS are associated with AD severity (CDR-sb) during the 5-year follow-up, a linear-mixed effect model (LMM) for repeated measures was used. We used variance component covariance structure. In the analyses, NPS and demographic variables (age, gender, education) were fixed effects, patient factor was a random effect, and CDR-sb was predicted variable. The association of all neuropsychiatric symptoms was analyzed with univariate analyses separately, followed by multivariate analyses, which was conducted by reducing least significant variables one by one until all were statistically significant to find the best symptom combination. This procedure should prevent the risk of multicollinearity as well. Several information criteria [–2 restricted Log Likelihood, Akaike’s Information Criteria (AIC), Hurvich and Tsai’s Criterion (AICC), Bozdogan’s Criterion (CAIC), Schwartz’s Bayesian Criterion (BIC)] were used to compare models. Since the LMM and GEE models include all available observations from study participants in analyzes, rather than only those who remained in the study, participant attrition is also accounted for and an advantage is gained over conventional repeated measures regression, which only consider study participants with full follow-up data. P < 0.05 was considered significant in all analyses, and all statistical analyses were conducted by IBM SPSS for Windows, version 21.0.
Ethical considerations
The ethics committee of the Kuopio University Hospital (64/00) gave a favorable opinion to the study, and the study was approved by the Finnish Supervisory Authority for Welfare and Health and the Finnish Ministry of Social Affairs and Health. The study was undertaken in accordance with the Helsinki Declaration. Participants were provided with written and oral information about the study and an initial visit was arranged shortly after diagnosis with persons who provided written informed consent to participate. Participation was voluntary and confidentiality was assured. A consent form was signed by both the caregiver and the person with AD patient, and the caregiver also provided proxy consent on behalf of the person with AD.
RESULTS
The baseline characteristics of study participants and mean NPI (SD) scores over the 5- year follow-up are summarized in Table 1. Of the initial study population of 236 participants and their caregivers at baseline, the participation numbers for subsequent follow-up visits were 197, 168, 131, 82, 73, respectively. The most common reasons for drop-out were death of the subject, institutionalization of subject, deterioration of subject health, and caregiver-related reasons (i.e. health, burden, death). The prevalence of specific NPS (classified as present or not present) during the five-year follow up is presented in Table 2. The progression of specific NPS (continuous variable, frequency x severity) in relation to dementia severity (CDR-sb) is shown in Fig. 1.
Baseline characteristics (n = 236) and annual means (standard deviations) of neuropsychiatric symptoms of subjects with very mild (CDR 0.5) or mild (CDR 1) AD baseline
CDR, Clinical Dementia Rating; NPI, Neuropsychiatric Inventory. Mean (standard deviation) presented unless other specified.
Prevalence of neuropsychiatric symptoms of persons with AD during a five-year follow-up. Number of subjects with each symptom and valid percent are shown
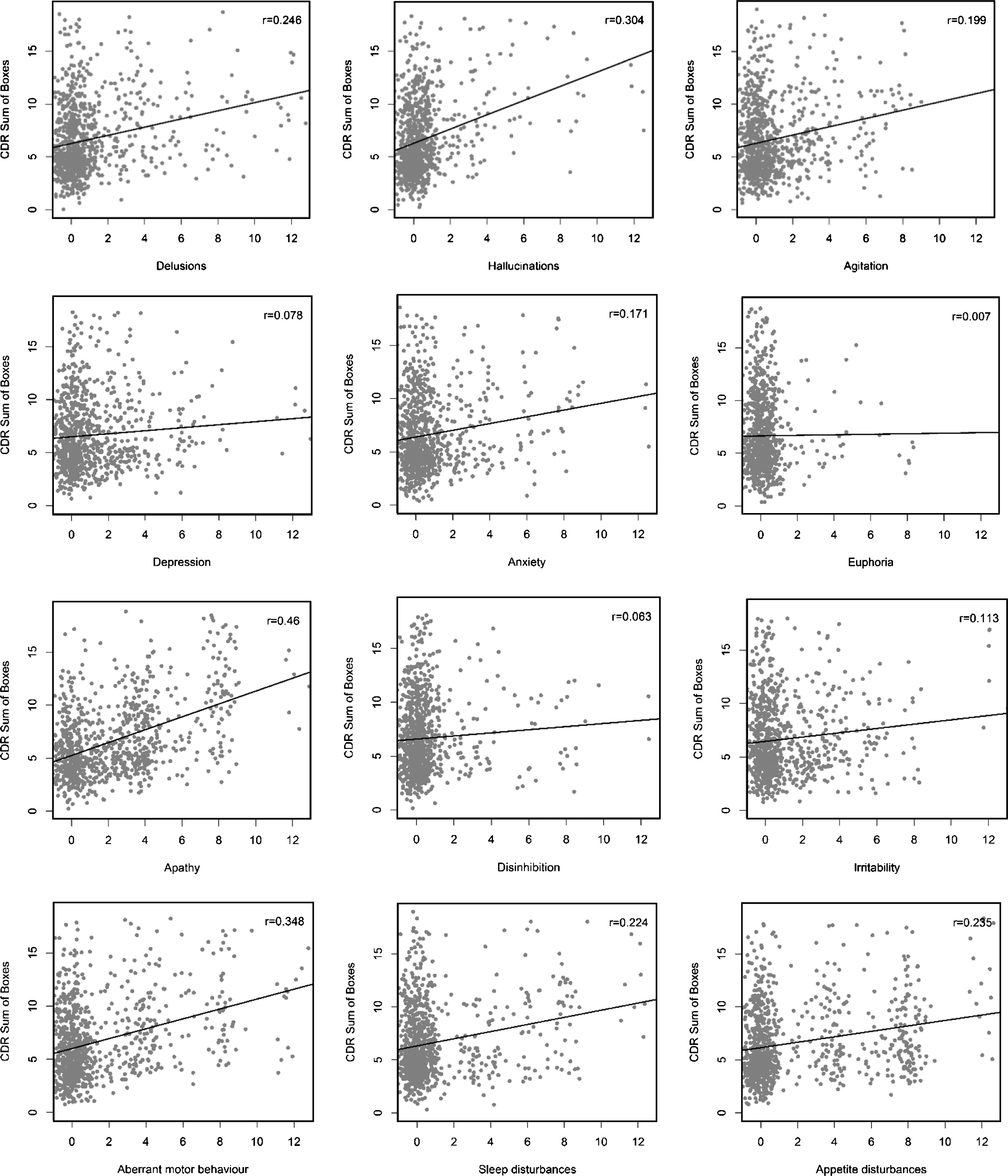
Scatterplot and linear relationship between each neuropsychiatric symptom and Clinical Dementia Rating Sum of Boxes.
Baseline factors associated with NPS progression
In univariate analyses, we found that baseline disease severity measured with both continuous CDR-sb and CDR stage (very mild or mild dementia) was a significant factor explaining the progression of NPS during the five-year follow-up. In multivariate analyses, we found that the best model explaining the progression of NPS included baseline disease severity and age at baseline, gender, and education were excluded (not statistically significant) (data not shown).
Baseline NPS predicting AD progression during a five-year follow-up
In univariate analyses, delusions (p = 0.001), agitation (p = 0.010), and aberrant motor behavior (p = 0.015) at baseline were statistically significant factors explaining later AD progression. Additionally, baseline euphoria (p < 0.001) was negatively associated with the progression of the disease. In multivariate analyses, the best model based on the information criteria to explain AD progression included education, delusions, euphoria, agitation, and aberrant motor behavior (Table 3).
Baseline neuropsychiatric symptoms predicting AD progression (CDR-sb) during the five-year follow-up: Generalized Estimated Equations
aSet to zero because this parameter is redundant. Data denote B regression coefficients (95% CI) unless other specified.
NPS associated with AD severity during the 5-year follow-up
In univariate analyses, all other NPS (severity x frequency value, p between 0.000 and 0.008) were significantly associated with disease severity except euphoria (p = 0.941) and inhibition (p = 0.56). The correlation coefficients between all NPS and demographic variables were in the acceptable level (<0.70) to be included in the same analysis. In multivariate analyses, the best model associated with AD severity based on that all variables were statistically significant (p < 0.05) included education, and time-dependent NPS including delusions, hallucinations, agitation, apathy, aberrant motor behavior, and sleep and appetite disturbances (Table 4). Also information criteria were evaluated.
The association of neuropsychiatric symptoms and AD severity (CDR-sb) during the five-year follow-up: Linear Mixed Models
aSet to zero because this parameter is redundant. Data denote F coefficients and B regression coefficients (95% CI) unless other specified.
DISCUSSION
We found that persons with advanced age and more severe AD at baseline developed more NPS during the five-year follow-up. Delusions, agitation, and aberrant motor behavior at the time of diagnosis predicted later AD progression. Furthermore, hallucinations, delusions, agitation, apathy, aberrant motor behavior, and sleep and appetite disturbances during the follow-up were associated with AD severity over the five-year period.
Previous studies have focused on the progression of NPS over time, and in some studies baseline NPS have been used to predict AD progression. However, there are fewer studies analyzing which baseline characteristics are associated with NPS progression. In our study, persons with mild AD (CDR 1) at baseline had more severe NPS during the follow-up than persons with very mild baseline AD (CDR 0.5). This result may be explained by the duration of the disease, different disease course in these groups, or the benefit of early diagnosis. We have previously studied, that persons with very mild AD at baseline (CDR 0.5) were more educated, but education did not correlate with NPI total score at baseline [30]. However, we have to take into consideration the possible impact of education on NPS progression. Actually, the education, was the only demographic variable which was included in the prognostic model with specific NPS, even though it was not statistically significant variable to predict AD progression in by itself. Age at the time of the diagnosis explained total NPS progression. As reviewed by Zhao et al. [11] age especially affects the prevalence of delusions, aggression, disinhibition, irritability, euphoria, anxiety, and depression. The possible effect of age to specific NPS has to keep in mind while interpreting our results, even though significant results include both symptoms, those affected and not affected by age in previous studies.
In our study, more severe baseline delusions, agitated behavior, and aberrant motor behavior were associated with later AD progression. Our findings are consistent with previous studies, in which psychotic symptoms at baseline have predicted rapid disease progression [14, 19]. However, Wilson et al. report that hallucinations but not delusions predicted rapid progression [13]. A role of agitation in AD progression has been previously found [18, 20], and aberrant motor behavior has been shown to predict mortality [9]. However, Wilkosz et al. [19] and Wilson et al. [13] include only psychotic symptoms in their analyses, and rapid progression was measured with a cognitive scale (Mini-Mental State Examination).
All NPS except frontal (euphoria and disinhibition), and affective (depression, anxiety, and irritability) symptoms were associated with AD severity during the follow-up. In correspondence with previous reports [11], euphoria and disinhibition were rarely detected, which may explain the lack of their significance. Brodaty et al. [10] and Zhao et al. [11] similarly show an increase in aggression, irritability, aberrant motor behavior, delusions, and apathy associated with AD severity, and Tschanz et al. also found that irritability is a relevant factor [12]. As in studies of Brodaty et al. and Tschanz et al., we found that hallucinations are associated with AD severity, contrary to Zhao et al. [11]. In some previous reports, disinhibition [10–11] and anxiety [10, 12] have been increased over time, but in our study, they do not associate with AD progression. We also found that sleep disturbances were associated with AD severity, unlike Brodaty et al. [10]. In summary, the results of the role of NPS during the course of AD vary between studies.
The present study investigates the progression of NPS in relation to AD severity, while previous reports have studied the progression of NPS over time [10, 12] or disease duration [11]. We know that there is individual variability in the course of the disease, and our study design enables us to analyze NPS in relation to disease severity with longitudinal data. Many of the symptoms that associated with AD progression in our study (aggression, aberrant motor behavior, delusions, and apathy) have also been shown to consistently worsen over time in other studies [10–11].
Zhao et al. [11] review both cross-sectional and longitudinal studies, but the results referred to above were analyzed in relation to disease duration, and the follow-up time in Tchanz et al. [12] varied between 0.07 and 12.9 years, with a mean follow-up time of 3.8 years. However, in these studies either only a small proportion of subjects used AD medication, or there was no reference to medication use. Both of those studies included persons with AD exclusively, but Brodaty et al. [10] also included persons with other types of dementia. These differences in study design may help explain the differing results. Tchanz et al. and Brodaty et al. evaluated NPS with NPI as in our study, and Zhao et al. used those 12 NPS included in NPI.
Based on our results, we recommend the detection of all specific NPS in future studies. The range of these symptoms is wide, and there are more individual differences in behavioral than in cognitive symptoms. It is also important to remember that there are NPS which may not significantly increase but are still present and may be remarkable over the course of AD. Tchanz et al. note that the diminishing occurrence of some NPS during the follow-up may reflect the fluctuating nature of NPS or the varying survival of those without NPS.
Our results suggest that subjects with delusions, agitation, and aberrant motor behavior may have more advanced AD at the time of the diagnosis, or they may have a more rapidly progressing disease even with early AD targeted medication. We may speculate whether delusions, agitation, aberrant motor behavior, and progression of cognitive and functional deterioration in AD are related to the dysfunction of the same brain regions. Several neurobiological changes have been connected with agitation and delusions depending on the type or content of these symptoms [31]. In addition, the presence of disruptive delusions could cause aggressive behavior or aberrant motor behavior. However, typically these three symptoms have been classified to different symptoms groups [31]. Some components of agitation can be defined as behavioral dysfunction as aberrant motor behavior [4, Appendix D]. Furthermore, the presence of these difficult symptoms could cause difficulties in everyday life and produce the more severe scores in CDR-sb. Importantly, in two recent meta-analyses, these three symptoms were found to be the most distressing NPS to caregivers, along with depression, apathy, and irritability [32, 33]. We suggest to the systematic evaluation of NPS at the time of the diagnosis in order to offer special support for persons with AD with delusions, agitation and aberrant motor behavior and their caregivers.
This study has some limitations. All subjects had very mild or mild AD at baseline. At the end of the 5-year follow-up AD had progressed to severe AD (CDR 3) stage in only a few subjects. This may reflect both the progression rate of AD and the drop-out bias of the study, as subjects with more severe disease or their caregivers may have felt it too difficult to participate study visits. Furthermore, institutionalization was one of the end-points of this study and Zhao et al. [11] point out that some specific symptoms lead to institutionalization more easily than others. Consequently, symptom pattern during the latest years of the disease may be different than that reported in this study, and results of this study cannot be generalized to persons with severe dementia or persons living in nursing home settings. Inclusion criteria of the study was age ≥65 and the average age at baseline was 75 years. Our results cannot be generalized to persons with early onset AD. The drop-out rate was quite high in our study, although it is comparable to other studies of this population [34]. Approximately half of subjects participated the third follow-up visit, but only 73 were able to participate in the fifth follow-up visit. To avoid the bias followed from this, LMM and GEE models were used in statistical analyses. Furthermore, prevalence of some NPS were low, which may affect the significance of these symptoms.
The main strengths of our study were the long follow-up period of community-dwelling persons and the use of well-known validated measures. Also used statistical methods (LMM and GEE) suits well in this kind of longitudinal study made in aged study population: they allow the use of all available longitudinal data, including the data of dropouts to minimize the bias. Also, all subjects, who participated the follow-ups, used AD-targeted medication started in the mild stages of the disease.
In conclusion, almost all neuropsychiatric symptoms increase in relation to AD progression and during follow-up, and the best predictors of AD progression were baseline delusions, agitated behavior, or aberrant motor behavior.
Footnotes
ACKNOWLEDGMENTS
The authors wish to thank study nurse Helena Mäkelä for her efforts to coordinate and carry out participant follow-ups and for collecting the data, research assistant Markku Kalinen and project researcher Lotta Salo for assisting in extracting the data from the original files to create the analysis data, and administrative assistant Mari Tikkanen for her invaluable help. The authors also wish thank MCs Tuomas Selander for consultation regarding analyses and statistics. This study was supported by Kuopio University Hospital (VTR grant 1V255/5772728), Päivikki and Sakari Sohlberg Foundation, and Finnish Cultural Foundation (IH).