
Abstract
Background:
Verb fluency (VF) is the less commonly used fluency test, despite several studies suggesting its potential as a neuropsychological assessment tool.
Objective:
To investigate the presence of VF deficits in mild cognitive impairment (MCI) and mild Alzheimer’s disease (AD) dementia; to assess the usefulness of VF in the detection of cognitively healthy (CH) people who will convert to MCI, and from MCI to dementia; and to establish the VF cut-offs useful in the cognitive assessment of Spanish population.
Methods:
568 CH, 885 MCI, and 367 mild AD dementia individuals were administered the VF test and a complete neuropsychological battery. Longitudinal analyses were performed in 231 CH and 667 MCI subjects to search for VF predictors of diagnosis conversion.
Results:
A worsening on VF performance from CH, MCI to AD dementia groups was found. Lower performances on VF were significantly related to conversion from CH to MCI/MCI to dementia. When the effect of time to conversion was analyzed, a significant effect of VF was found on the faster conversion from CH to MCI, but not from MCI to dementia. Moreover, VF cut-off scores and sensitivity/specificity values were calculated for 6 conditions (3 age ranges by 2 educational levels).
Conclusion:
The VF test may be a useful tool for the differential diagnosis of cognitive failure in the elderly. Since VF deficits seem to take place in early stages of the disease, it is a suitable neuropsychological tool for the detection not only of CH people who will convert to MCI, but also from MCI to dementia.
INTRODUCTION
Verbal fluency refers to the ability to generate spoken or written words in a given time, usually one minute [1]. Verbal fluency tests, such as letter and category fluencies, are often included in neuropsychological test batteries as a measure of language and executive functions [2] due to their shortness and ease of administration, without the need for any other instrument than a stopwatch.
In general terms, verbal fluency tasks require preserved language and executive functions to be properly performed [2–5]. These tasks may be particularly useful discriminating between normal and impaired cognitive abilities [6–8]. Therefore, verbal fluency tasks have been incorporated in screening tools designed to detect cognitive deficits such as the Addenbrooke’s Cognitive Assessment [9, 10], the Dementia Rating Scale [11, 12], or the Edinburgh Cognitive Assessment [13]. Verbal fluency tests have been used in a wide range of neurological diseases such as Alzheimer’s disease (AD) [14], neurodegeneration coursing with movement disorders [15, 16], multiple sclerosis [17], and human immunodeficiency virus (HIV) [18].
Interestingly, several studies have reported that each type of verbal fluency may be sensitive to different aspects of cognitive functioning and, consequently, to the functioning of different cerebral structures. Indeed, the results of case studies have demonstrated that verb and noun retrieval are subserved by different anatomical substrates [19–21]. In addition, studies of patients with different neurodegenerative disorders, such as AD [22, 23], Parkinson’s disease [24–27], frontotemporal dementia [28, 29], motor neuron disease [16, 30], and HIV [18], have described qualitatively different performances in each type of these verbal fluency tasks.
Previous research has suggested that verbal fluency tests are useful, not only to differentiate between healthy individuals from those with cognitive impairment or dementia [31–36], but also to discriminate between converters and non-converters to dementia from mild cognitive impairment (MCI) [37–39]. However, most of these studies used category and letter fluency to assess their subjects, not verb fluency. That is, the less common test of verbal fluency is the verb fluency task. Indeed, verb fluency has not been frequently used in neuropsychological assessment, whereas nowadays, due to several studies suggesting the potential of this tool [40], the use of verb fluency is increasing.
The verb fluency refers to the generation of as many verbs (or actions or things that people do) as possible in a given time, allowing the production of verbs denoting concrete actions (i.e., to run) or internal states (i.e., to think) [21]. This type of verbal fluency task assesses language and executive functions. It is sensitive to dysfunctions in fronto-subcortical networks linking primary and secondary motor cortex, frontal lobes, and basal ganglia [19–21, 40–44]. Since the generation of verbs has also been related to neocortical-hippocampal interaction, mainly the perirhinal cortex, which receives reciprocal inputs from associative regions (prefrontal, insular and anterior cingulate cortices) [45], verb fluency has been proposed as a sensitive test detecting early dysfunctions associated with AD.
The verb fluency task seems to be more cognitively demanding than other verbal fluency tasks [40, 44]. Accordingly, healthy adults perform worse on generating verbs than nouns [23, 46]. The reasons for this discrepancy could be partly grammatical. In fact, in many languages the verb morphology tends to be more complex than noun morphology, yet they could also reflect deeper conceptual differences, with action semantics underlying verb production being more complex than that of nouns [47].
Following this line of reasoning, we hypothesized that verb fluency may be a useful tool to assess cognition. Thus, the aims of the present study were: To investigate the presence of verb fluency deficits in patients with MCI and mild AD dementia; to assess the potential usefulness of the verb fluency for the detection of healthy aging people who will convert to MCI, or from MCI to dementia; and to establish the verb fluency cut-off scores of impairment that could be useful in the cognitive assessment of Spanish population.
METHODS
Subjects and study design
This study was divided into two parts: (I) a cross-sectional study including all cognitively healthy (CH) individuals, subjects with MCI, and patients with mild dementia due to AD who fulfilled the inclusion criteria for the present study; and (II) a longitudinal study searching for the verb fluency predictor value of conversion of diagnosis (from CH to MCI and from MCI to dementia), among those CH and MCI subjects who had at least one follow-up assessment.
The study was conducted in Fundació ACE, Institut Català de Neurociè ncies Aplicades (Barcelona, Spain), a non-profit Alzheimer’s center that provides diagnostic, treatment and patient management services to the Catalan Public Health Service (Xarxa Hospitalà ria d’Utilització Pú blica, XHUP) [48]. Subjects are usually referred to the Memory Clinic of Fundació ACE by primary care physicians or medical specialists because the subjects, their families, or their physician felt that they could have a memory loss or cognitive decline in other domains. In the diagnostic procedure, we used cut-off scores for determining the presence or absence of cognitive impairment. These cut-off scores were obtained from a representative sample of our target population older than 44 years. See [7] for more details.
Inclusion and exclusion criteria
The general inclusion criteria for all subjects regardless to the group they belonged were: 1) age older than 44 years old because the authors had normative data for this age group [7]; 2) educational level of at least elementary school (that is, at least 6 years of formal education) to ensure the correct understanding of the verb fluency test; 3) had completed the verb fluency test and had been administered the Neuropsychological Battery from Fundació ACE (NBACE) [7, 49]; 4) had completed the diagnostic procedure with a baseline final diagnosis of CH, MCI or mild dementia due to AD.
For the CH group the following inclusion criteria were considered: 1) being classified as “without objective cognitive impairment”; 2) no neurologic symptoms reported either by the participant or an informant; 3) a Clinical Dementia Rating (CDR) [50] of zero; 4) average or above average scores on the NBACE, score≥12 on the Memory test of the 7 Minute Screen test [51, 52] and score≥24 on the Mini-Mental State Examination (MMSE) [53, 54]; 5) no history of functional impairment due to declining cognition; 6) a score < 4 on the Blessed Dementia Rating Scale [55, 56].
The inclusion criteria for the MCI group were: 1) subjective memory complaints; 2) normal general cognition as measured by the MMSE; 3) preserved performance in activities of daily living; 4) absence of dementia; 5) an objective measurable impairment in memory or another cognitive function with or without impairment in other cognitive domain (MCI amnestic or non amnestic single or multiple domain [57]) with absence (probable MCI) or presence (possible MCI) of comorbidities (i.e., depression, cerebrovascular disease) that could explain observed cognitive deficits [39].
The inclusion criteria for the AD dementia group were: 1) diagnosis of dementia syndrome due to AD [58]; 2) mild severity of dementia determined by a total score of 1 in the CDR; 3) a MMSE score > 19.
The exclusion criteria were: 1) age younger than 45 years old because the authors had no normative data for this age group; 2) educational level below Elementary School to correctly understand the instruction of the verb fluency test; 3) MMSE score below 20 to ensure that patients with moderate dementia were not included in the study; 4) Global Deterioration Scale [59] score > 4 or a dementia of the non-AD type.
In the diagnosis procedure, all participants received an extensive clinical evaluation including a complete neuropsychological assessment (for details, see below), a neurological history and examination, and a semi-structured psychosocial interview conducted by a social worker. Moreover, patients’ functionality was assessed by the Blessed Dementia Rating Scale [55, 56].
Prior to the evaluation a written informed consent was obtained from all participants and in those cases of patients with dementia, also by their caregivers. The study was conducted in accordance with the Declaration of Helsinki and with Spanish biomedical laws (Law 14/2007, July 3rd, about biomedical research; Royal Decree 1716/2011, November 18th). The study was approved by the Fundació ACE Research Ethics Committee.
Neuropsychological assessment
The NBACE was administered in the diagnostic procedure. It assesses cognitive functions relevant to the diagnosis of neurodegenerative disorders. Its administration takes approximately 45 minutes and includes the following tests: Temporal, Spatial, and Personal Orientation; Digit Span (forward and backwards), Block Design (abbreviated in 4 items), and Similarities (abbreviated to the first 10 items) subtests extracted and adapted from the Wechsler Adult Intelligence Scale-Third Edition; The Word List Learning test from the Wechsler Memory Scale-Third Edition (WMS-III) (without using the interference list); Repetition (2 words and 2 sentences); Verbal comprehension (to correctly execute 2 simple, 2 semi-complex, and 2 complex commands); an abbreviated 15-item Boston Naming Test (15-BNT); the Poppelreuter test; Luria’s Clock test; the Automatic Inhibition subtest of the Syndrome Kurz Test; Letter Fluency (to name as many words as possible beginning with the letter “p” in one minute); Category Fluency (to name as many words belonging to the semantic category “animals” as possible in one minute); 4 item Imitation praxis; 4 item Ideomotor commands; and the 15-Objects Test (15-OT). Normative data and cut-off scores of NBACE subtests have been reported elsewhere [7, 49].
The verb fluency task was added for the purpose of the present study and its scores were not taken into account when diagnosing the participant. Note that when the authors devised the early version of the NBACE (2006), the assessment of verb fluency was not popular among general test batteries of cognitive decline. Participants were asked to name as many verbs in infinitive or actions as possible in one minute. They had to say the verbs in infinitive, but if they named any inflection or repetition of a verb, only the first one was considered as correct. When the participant needed an example to understand the task, they were told the following sentence: “Something that we can do such as to sing” [60]. All types of verbs were allowed even abstract verbs. The total score consisted of the number of correct answers. Errors were not registered.
Statistical analysis
Statistical analysis was carried out using SPSS 20.0 (SPSS Inc., Chicago, IL). Normal distribution of data was verified before conducting the statistical analyses. In the Cross-sectional study, One factor Analysis of Variance (ANOVA), with contrasts, was carried out to compare demographic and cognitive scores (verb fluency, NBACE and MMSE) between CH, MCI, and AD dementia groups; and χ2 for sex comparisons.
In the whole sample, Pearson’s correlation analyses were performed between verb fluency scores, age, and years of education. Data of subjects with cognitive impairment (MCI and mild dementia) and CH were used to calculate cut-off scores and sensitivity/specificity values for six conditions after combining 3 age ranges (44 to 64; 65 to 74; and older than 74 years) by 2 educational levels (elementary school (6–8 years) and more than elementary school (>8 years). Receiver operating characteristic (ROC) analysis was used to establish the optimal cut-off values between cognitive impairment and CH groups, by calculating the sensitivity and specificity of verb fluency test cut-off values for the 6 (age by education) conditions.
In the longitudinal study, t-tests were used to compare verb fluency performances between converters and non-converters from CH to MCI, and from MCI to dementia. Logistic Regression analyses were performed to describe the predictive value of verb fluency test in the conversion from CH to MCI, and from MCI to dementia. Moreover, Cox Proportional Hazard models were carried out to measure the association between the verb fluency performance and time to convert from CH to MCI and from MCI to dementia diagnosis.
RESULTS
Cross-sectional study
A total of 1.820 subjects had been administered the verb fluency test and assessed by the neuropsychological battery NBACE. They completed the diagnostic procedure with a final diagnosis of CH (n = 568, 31.2%), MCI (n = 885, 48.6%, 535 amnestic and 350 non amnestic), or mild dementia due to AD (n = 367, 20.2%). Demographic data are detailed in Table 1. Adjusted mean scores, standard deviation (SD), and Analysis of Covariance values of the verb fluency task and NBACE subtests are detailed in Table 2.
Demographic characteristics of participants
CH, cognitively healthy; MCI, mild cognitive impairment; AD, mild AD dementia; SD, standard deviation; 1: χ2; 2: F. ***p < 0.001.
Neuropsychological performance of the study subjects
CH, cognitively healthy; MCI, mild cognitive impairment; AD dementia, mild Alzheimer’s disease dementia. The results of Analysis of Covariance, corrected for age and education, are shown as adjusted Mean (Standard Deviation). ***p < 0.001; All scores significantly differed between CH, MCI, and mild AD dementia groups.
As shown in Table 2 and Fig. 1, verb fluency test provided a statistically significant worsening on performance from CH to MCI and mild AD dementia groups; and in Fig. 2, it is shown including amnestic and non amnestic MCI groups.
Data from 1.252 patients with cognitive impairment (MCI and mild AD dementia) and 568 CH subjects were taken to calculate verb fluency cut-off scores in relation to age and education (see Table 3).
In the whole sample, lower verb fluency scores were significantly correlated with older age (r = –0.44, p < 0.001) and lower education (r = 0.50, p < 0.001), but not with sex (t = –1.04, p = 0.300). Interaction between age and education was statistically significant (F = 5.78, p = 0.003). For this reason, cut-offs were reported after combining three age ranges (45–64, 65–74, and >74) by two educational levels (elementary school and >elementary school) (see Table 3 for details).
Longitudinal study
From the 568 CH subjects and 885 patients with MCI, 231 and 667 were followed up (that is, they were reassessed at least 6 months after baseline), respectively. Mean time follow-up was 19.3 months (SD = 12.2) in CH subjects and 16.6 months (SD = 9.5) in the MCI group. With regard to CH group, the 18.2% of subjects (n = 42) had converted to MCI at the time of follow-up. The mean annual conversion rate for this group was 12.1%. The conversion rate of patients with MCI (n = 144) to dementia (106 patients or 71.1% AD dementia, 25 patients or 16.8% vascular dementia, 9 patients or 6% frontotemporal dementia, 9 patients or 6% with parkinsonism) at the time of the follow-up was 21.6%. The annual conversion rate for this group was 15.6%.
With regard to CH group, converters to MCI had worse baseline performances on verb fluency test than those who maintained a stable performance (converters to MCI: mean = 13.9, SD = 4.9, non-converters: mean = 18.7, SD = 6.3; t = 4.63, p < 0.001). Those MCI patients who converted to dementia performed significantly worse on verb fluency (converters to dementia: mean = 9.4, SD = 5.6, non-converters: mean = 10.9, SD = 5.7; t = 2.933, p = 0.003) than those who did not convert. A Logistic Regression analysis introducing the verb fluency test, adjusting for age, showed that this test was significantly related to conversion from CH to MCI (Wald = 15.186, OR = 0.87, p < 0.001); and also significantly related to conversion from MCI to dementia (Wald = 4.503, OR = 0.96, p < 0.034).
A Cox Proportional Hazard model was carried out to measure the association between the verb fluency variable and time to convert from CH to MCI, controlling for age, showed that verb fluency had a statistically significant effect (Wald = 7.922, p = 0.005, HR = 0.90; CI 95 0.842–0.970). Another Cox Proportional Hazard model, controlling for age, was performed to measure the association between the verb fluency variable and time to develop dementia from MCI. It showed that verb fluency had not any statistically significant effect.

Verb fluency performances of healthy controls (HC), mild cognitive impairment (MCI), and mild Alzheimer’s disease (AD) dementia groups.
Verb fluency cut-off scores for age and education
SE, sensitivity; SP, specificity.
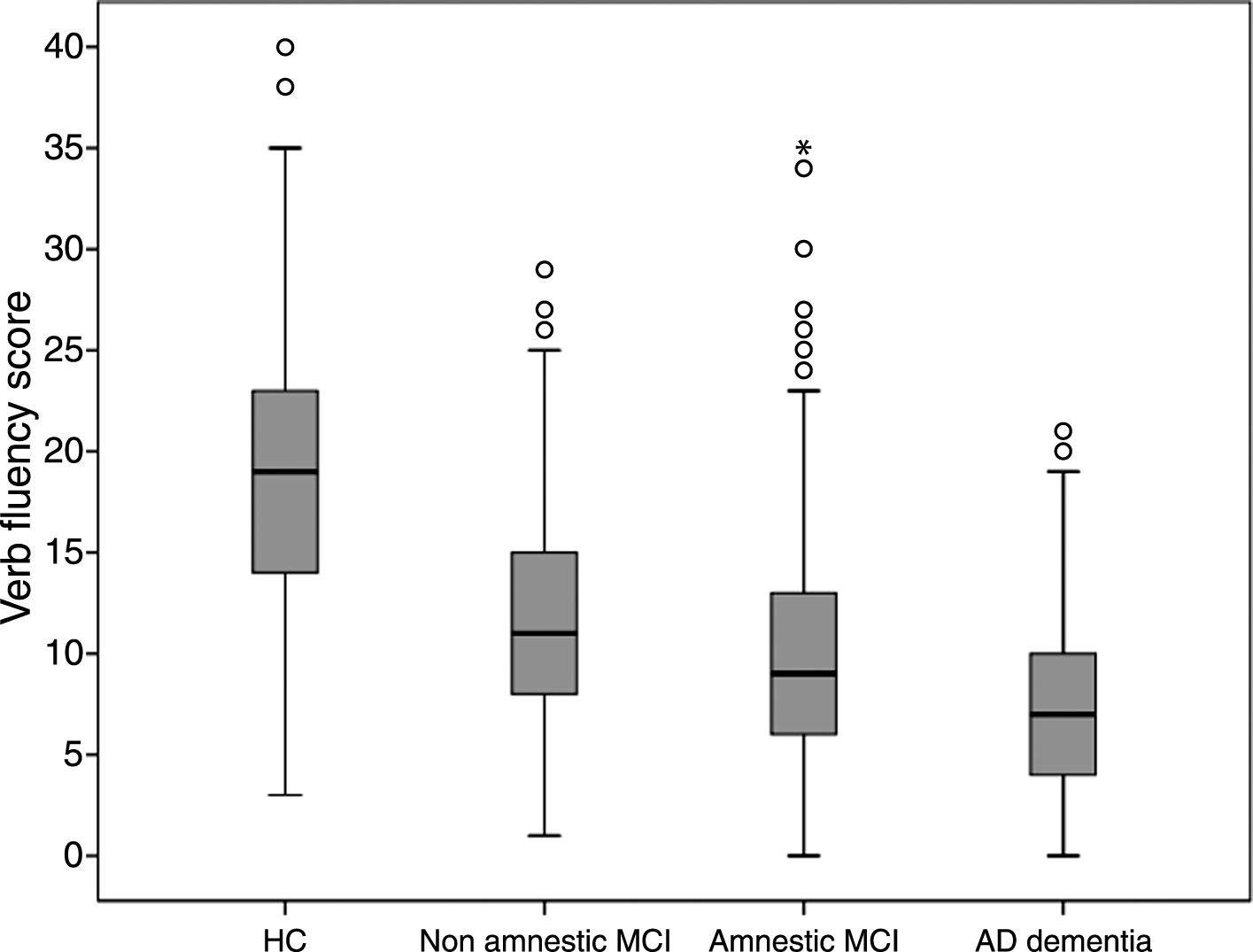
Verb fluency performances of healthy controls (HC), non amnestic mild cognitive impairment (MCI), amnestic MCI, and mild Alzheimer’s disease (AD) dementia groups.
DISCUSSION
The results of the present study reveal that verb fluency test can be a useful tool for the differential diagnosis of cognitive failure in the elderly. Verb fluency test provide a useful gradation of impairment from normal aging to MCI and mild AD as reported in previous studies with verbal fluency tests [6, 61].
Consistent with a previous study in healthy Spanish subjects [62], higher levels of schooling were found related to better verb fluency performances. Moreover, in contrast to CH subjects, patients with cognitive impairment (MCI and mild AD dementia groups) obtained lower performances on verb fluency. Thus, verb fluency might be a suitable tool to detect subtle performance deficits in patients with MCI and mild dementia who otherwise perform normally on other verbal fluency tests. This is consistent with the results of a cross-sectional study [63] in which verb fluency, compared to letter and category fluencies, was found disproportionately impaired in MCI and was suggested as a possible linguistic marker for the progression from the subjective memory impairment to MCI diagnosis. From the standpoint of cognitive neuroscience, in contrast to the semantic representation of nouns in the brain that seems to be organized in a systematic, taxonomical way, which may imply an overlap among related semantic neuronal sets [64, 65], in the case of verbs such taxonomies might play a less pronounced role, with less overlapping word meanings, making the verb fluency task more difficult [44, 63]. From a linguistic point of view, verbs are often more complex than nouns, displaying features such as argument structure and, in many languages, more complex morphology [47].
Since most of the decrease in verb fluency seems to take place already in the early stages of AD, decreased performance on this task may herald the conversion from CH to MCI, but is less sensitive to detect the further progression of the disease. In support of this argument, when the time of conversion was taken into account in the Cox Regression analyses, the verb fluency only showed a significant effect on the faster conversion from CH to MCI, but not from MCI to dementia, findings that concur with results of previous studies using category [37, 66] and letter verbal fluencies [38, 66].
Similar to another study in Spanish speakers [62], having fewer years of schooling and older age were significantly related to worse performances on verb fluency, but sex did not affect performance. Since we found that verb fluency is useful to detect cognitive impairment and it is related to age and education, we decided to detail cut-off scores segregated by age and education. That is, those subjects with scores lower than their corresponding cut-off (taking their age and educational level) would be probably cognitively impaired (MCI or AD dementia), and those with scores higher than their cut-off could be taken as cognitively preserved. Thus, data reported here are complementary with the results of our own previous studies [7, 49] in setting the relevant cut-off scores for impaired function and decision making algorithms for use in identifying adult individuals with cognitive impairment.
A limitation of the present study was that cerebrospinal fluid biomarkers were not available, but we considered that it was not a critical matter for the purpose of the present study. Lumbar puncture is not a mandatory technique in Spain for MCI and AD diagnosis in the clinical practice in our country.
Further research will be needed to analyze the ability of verb fluency to discriminate between converters and non-converters to AD among cognitively healthy individuals with subjective cognitive decline.
In conclusion, verb fluency test may be a useful tool in the detection of the different stages of cognitive decline associated with AD. Since the verb fluency seems to take place in the early stages of the disease, it is a suitable neuropsychological tool for the detection of healthy aging people at risk of converting to MCI. Nevertheless, it should be taken into account that the findings of the present study support the usefulness of verb fluency test in the context of a complete neuropsychological assessment, but not when it is used in isolation.
ACKNOWLEDGMENTS
We acknowledge the patients and control subjects who participated in this study. We are indebted to Trinitat Port-Carbó and her family for their support to Fundació ACE research programs. This work did not receive any specific grant from funding agencies in the public, commercial or not-for-profit areas. It was funded by Fundació ACE, Institut Català de Neurociències Aplicades, own research funds.
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/17-0826r1).