
Abstract
Background:
Ischemic heart disease (IHD) is associated with cognitive decline and may contribute to an increased risk of dementia.
Objective:
The goal of the present study was to investigate whether cilostazol use is associated with a lower risk of incident dementia in Asian patients with IHD, and whether these effects differed based on sex.
Methods:
This retrospective cohort study was performed using the Korean National Insurance Claim Data of the Health Insurance Review and Assessment Service; the duration of the study was from January 1, 2007 to December 31, 2015. The study group comprised 66,225 patients with IHD, aged >65 years, who had received cilostazol. Age- and sex-matched IHD patients without cilostazol exposure were selected as the control group. The risk of dementia was compared between the cilostazol and control groups.
Results:
Compared to the control group, total cilostazol users had a marginally significant lower risk of incident dementia. After stratification by sex, the reducing effect of cilostazol on incident dementia was significant in female participants, but not in male participants. Female patients who had cilostazol for over 2 years showed a clinically meaningful preventive effect (HR, 0.85; 95% CI, 0.82–0.88).
Conclusions:
This study suggested that cilostazol treatment may reduce the risk of incident dementia in Korean patients with IHD. Its beneficial effect was remarkably significant in female patients who received cilostazol for over a 2-year period.
INTRODUCTION
Ischemic heart disease (IHD) remains the leading cause of mortality [1] and is an increasing healthcare burden in elderly adults worldwide [2]. Similar to IHD, the prevalence of dementia, a disorder characterized by memory and cognitive impairments, also increases with age. In addition to age, dementia and IHD share some background risk factors, such as hypertension and diabetes. It has been reported that IHD is associated with an increased risk of cognitive decline and may contribute to the risk of dementia [3 –5]. The Bronx Aging Study demonstrated that women with a history of IHD had a five-fold increase in the risk of developing dementia [5]. Using the results from the Rotterdam and Rotterdam Scan Study, Ikram et al. [6] demonstrated that IHD in men was associated with an increased risk of dementia. In addition to an increased risk of dementia, the coexistence of IHD and dementia also significantly increases the risk of mortality of patients with ischemic heart failure [7]. Thus, the development of an effective method to reduce the risk of dementia in the IHD population is clinically important.
Cilostazol acts as an antiplatelet agent and has other pleiotropic effects based on phosphodiesterase-3-dependent mechanisms [8]. Cilostazol has been prescribed for the treatment of IHD [9], and is particularly popular in Asian countries, such as Korea, Japan, and China [10]. The recommended dosage cilostazol in Korea is 100 mg twice daily. In addition, cilostazol offers endothelial protection that involves the inhibition of apoptosis in endothelial cells [11], attenuation of the phenotypic modulation of vascular smooth muscle cells [12], and sustained blood flow by endothelium-independent vasodilation [13]. Intriguingly, cilostazol has been reported to decrease amyloid-β (Aβ) accumulation and plays a protective role against Aβ-induced cognitive deficits in experimental models [14, 15]. In a retrospective study, patients with mild dementia showed slowed cognitive decline with cilostazol [16], suggesting for its potential as a therapeutic candidate for improving cognitive impairment [17].
Sex is an important factor to consider in clinical practice as it can influence healthcare, the choice of individual pharmacological treatments, and patient outcomes [18, 19]. In general, disability and morbidity are more prevalent in older women than older men. This may explain why older women are more likely to use more medication [20]. Although many sex differences as well as gender differences have been reported in human health throughout history, most clinical studies have been conducted on male participants, with the consideration that the male sex is the true representative of human beings [21]. In particular, 22% of the reports failed to provide separate efficacy data for women and men, with 17% of reports omitting sex-related safety data for new drug applications [22]. Ultimately, a better understanding of the sex-related factors on drug response would be helpful to improve the efficacy of the drug for different individuals.
In this context, the objective of the present study was to investigate whether cilostazol use was associated with a lower risk of incident dementia in Asian patients with IHD (Korean Health Insurance Review and Assessment Service database), and if so, whether its effects differed between men and women.
METHODS
Data source
The present study used the Korean Health Insurance Review and Assessment Service (HIRA) database. The National Health Insurance (NHI) program was initiated in Korea in 1977 and achieved universal coverage by 1989. The data gathered via this program is available to all health care institutions for medical claim reimbursement. The NHI universal health care program covers the entire national Korean population of approximately 50 million as a social insurance benefits scheme. HIRA data consist of patients’ demographic information, diagnoses, prescription records, medical procedures and services, types of health care institution, medical utilization information, and admission dates. Prescription records include the brand name, generic name, prescription date, duration, dose, and route of administration. Diagnosis is recorded by the Korean Standard Classification of Disease, Six Revision, which reflects the International Classification of Disease, Tenth Revision [ICD-10]. For our analysis, all potential identifiers in the HIRA claims data were removed and the information was linked with a new unidentifiable code representing individual patients. The present study was approved by the Institutional Review Board of Ajou University (No. 201610-hb-EX-001).
Study population
Patients with a diagnosis of IHD, who were identified as outpatients or inpatients from 01 January 2007 to 31 December 2015, were selected for our first cohort. All were 65 years of age and older. Patients with IHD were defined as those with at least one diagnosis of ICD-10 codes I20-I25, of whom, patients prescribed cilostazol at least once from 1 January 2008 to 31 December 2010 (index period) were selected as cilostazol users. The cohort of cilostazol users was matched with a comparison cohort group using propensity score matching. Before propensity score matching, the comparison cohort group was selected by random sampling with adjustment for age and index year. Then they were matched with the cilostazol users based on propensity scores calculated by age, sex, comorbidities, index year, and concurrent medication. The index date was defined as the date when cilostazol was first prescribed and the first date of matched index period. To include only those who were newly treated with the study therapy, we excluded patients who had received cilostazol in the year before the index date and those who used cilostazol for less than 3 months were also excluded [23]. We also excluded patients who had a dementia diagnosis code or were prescribed anti-dementia drugs prior to cohort entry to exclude patients with incident dementia.
Exposure to cilostazol
During the index period, commercially available cilostazol products were used. A cilostazol user was considered ‘continuously exposed’ if a prescription was filled within 1.5 times the prescription days’ supply after the end date of the previous prescription [24]. The cumulative duration of cilostazol exposure was calculated as the sum of supply days to investigate the effect of duration, which was classified into ‘short-term’ (<1 year), ‘mid-term’ (1-2 years), and ‘long-term’ (>2 years) use.
Diagnosis of dementia
The primary outcome was an incident diagnosis of all types of dementia in previously cilostazol-naïve patients with IHD. Follow-up was started from the index date; all patients were tracked until they developed dementia, were censored from the database owing to death, or showed no record of medical claims for more than a year, or since 31 December 2015, whichever came first. We defined new-onset dementia as a record of a diagnosis of dementia with Alzheimer’s disease (ICD-10, F00, G30-31), subcortical ischemic vascular dementia (ICD-10, F01-03), and a prescription of anti-dementia agents.
Covariates of analysis
We considered confounding factors in the analysis to reduce potential bias. These factors were as follows: age, sex, comorbidities including hypertension (ICD-10, I10), diabetes (ICD-10, E11-E14), ischemic stroke (ICD-10, I63-64), depression (ICD-10, F32-33), and Parkinson disease (ICD-10, G20-22, G23.2). These comorbidities are known risk factors for dementia [25 –29]. Diagnoses for comorbidities were considered present if the records were shown at least twice in the year prior to the index date. The Charlson comorbidity score was calculated in the year prior to the index date. During the study period, concomitant medications considered were aspirin, other antiplatelets, angiotensin converting enzyme inhibitors, angiotensin receptor blockers, β-blockers, calcium channel blockers, statins, antidiabetic agents, and proton pump inhibitors. These medications were not included as concomitant medications if prescribed only once for a period of less than 7 days.
Statistical analyses
Cilostazol users and non-users were matched according to propensity score analyses. Propensity scores were obtained by fitting a logistic regression model that included the predictor variables as all baseline covariates. Baseline characteristics were presented as patient numbers along with categorical variables in percentages, and as mean and standard deviation (SD) for continuous variables. Categorical variables and continuous variables were then compared and analyzed using the Mantel-Haenszel Chi-squared test and Student’s t-test, respectively. We performed a Cox proportional hazard analysis to evaluate the effect of cilostazol therapy on the incidence of dementia. Outcomes are presented as hazard ratios (HR) and 95% confidence intervals (CIs). All statistical analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC, USA). Bonferroni correction was used to cater for multiple comparison and p values were compared against α/number of comparisons instead of α=0.05.
RESULTS
Baseline characteristics of patients
The study population with IHD from 2008 to 2010 consisted of 2,262,748 patients, who were aged 65 years or older. Of those, 132,450 patients who were initially dementia-free were captured after 1:1 matching based on propensity scores. Overall, 64,687 (48.8%) male patients and 67,763 (51.2%) female patients were included. Table 1 summarizes the clinical characteristics of the study cohort.
Characteristics of study patients
CCI, Charlson comorbidity indes; ACEI, angiotensin-converting-enzyme inhibitor; ARB, angiotensin II receptor blocker; CCB, calcium channel blockers; PPI, proton pump inhibitors.
The cumulative duration of cilostazol use and the effects of sex difference on risk of dementia
Figure 1 shows that, Over the follow-up period (mean 5.1 years, median 5.7 years; range 3.3–7.0 years), 15,252 of the 64,687 male participants developed dementia, which included 6,963 (22.4%) of the 31,118 cilostazol users and 8,289 (24.7%) of the 33,569 non-users. Of the 67,763 female participants, 20,490 participants experienced dementia during the follow-up (mean 5.1 years, median 5.8 years; range 3.4–6.9 years), which included 10,390 (29.6%) of the 35,107 cilostazol users and 10,100 (30.9%) of the 32,656 non-users. As shown in Table 2, total cilostazol users had a marginally significant lower risk of dementia compared to the control group (HR, 0.98; 95% CI, 0.96–0.98). After stratification by sex, the reducing effect of cilostazol on incident dementia was significant in female participants (HR 0.95, 95% CI 0.92–0.98), but not in male participants (HR 0.97, 95% CI 0.94–1.00). The risk assessment for developing dementia according to the duration of cilostazol therapy is shown in Table 3. Based on the duration of cilostazol therapy among the study patients (mean 2.1 years), we divided the duration into ‘short-term therapy’ (<1 year), ‘mid-term therapy’ (1–2 years), and ‘long-term therapy’ (>2 years). Long-term cilostazol therapy was associated with a relatively lower risk of developing dementia in both groups; (HR 0.94, 95% CI 0.89–0.97 for men; HR 0.85, 95% CI 0.82–0.88 for women; Table 3).
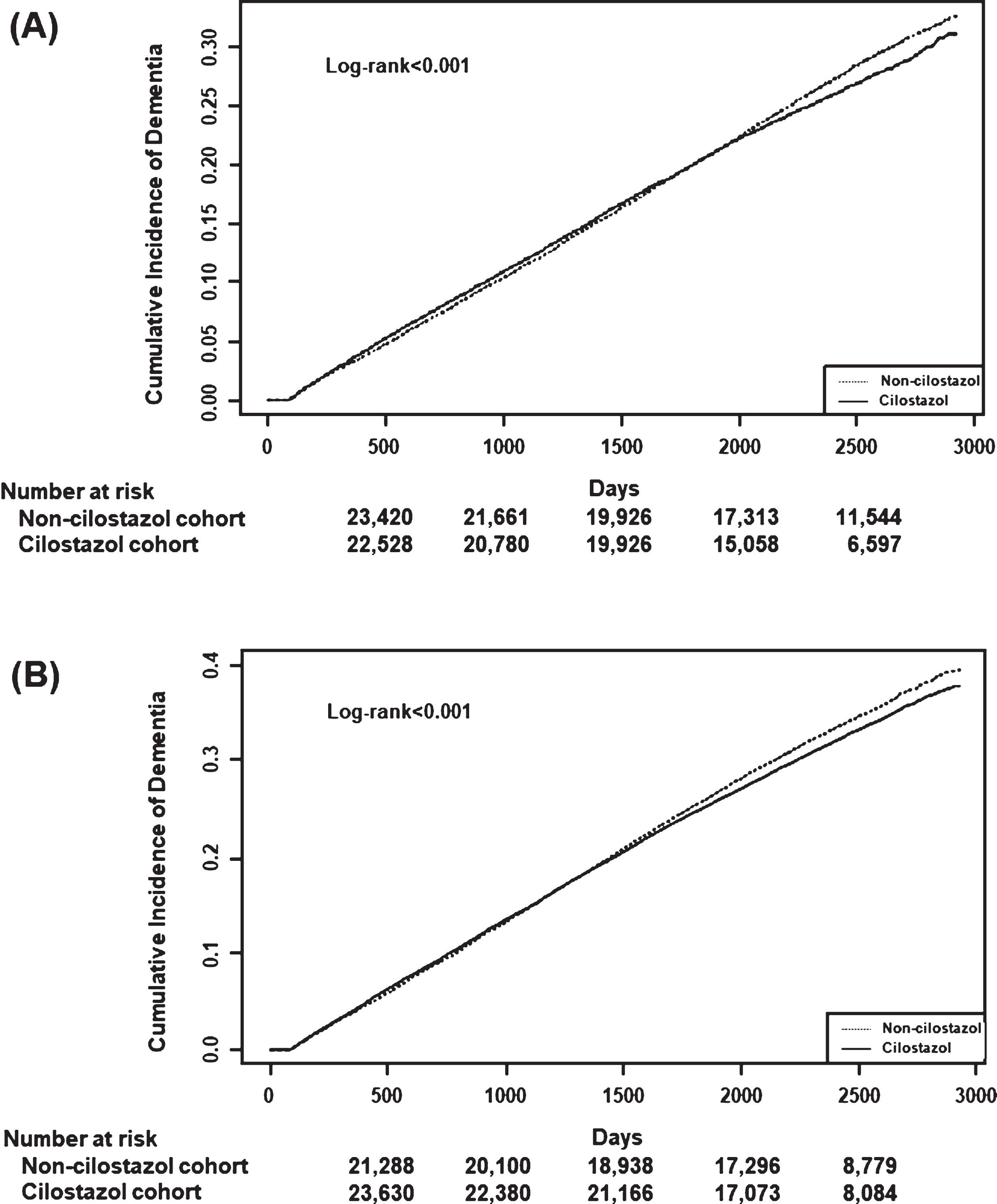
Cumulative incidence of all-cause dementia between cilostazol users and non-cilostazol users during the follow-up period. A) Male cilostazol versus non-cilostazol users. B) Female cilostazol versus non-cilostazol users.
The risk of dementia associated with cilostazol use
Notes: Hazard ratios (HR) were calculated using Cox proportional hazard model; CI, confidence interval.
The risk of dementia associated with cilostazol use by duration
Notes: Hazard ratios (HR) were calculated using Cox proportional hazard model; CI, confidence interval.
Cilostazol use and the risk of dementia in different groups of patients
Subgroup analysis revealed that male and female cilostazol users with hypertension and diabetes mellitus were less likely to develop dementia. The adjusted HR of dementia in male cilostazol users with hypertension and diabetes mellitus was 0.95 (95% CI, 0.91–0.98) and 0.94 (95% CI, 0.90–0.99), respectively. Similar results were found in female cilostazol users with hypertension and diabetes mellitus (HR 0.92, 95% CI, 0.90–0.94 and HR 0.94, 95% CI, 0.91–0.98 respectively). In contrast, no protective effects were observed in cilostazol users with ischemic stroke, depression, and Parkinson’s disease, compared with non-users (all p > 0.05; Fig. 2).
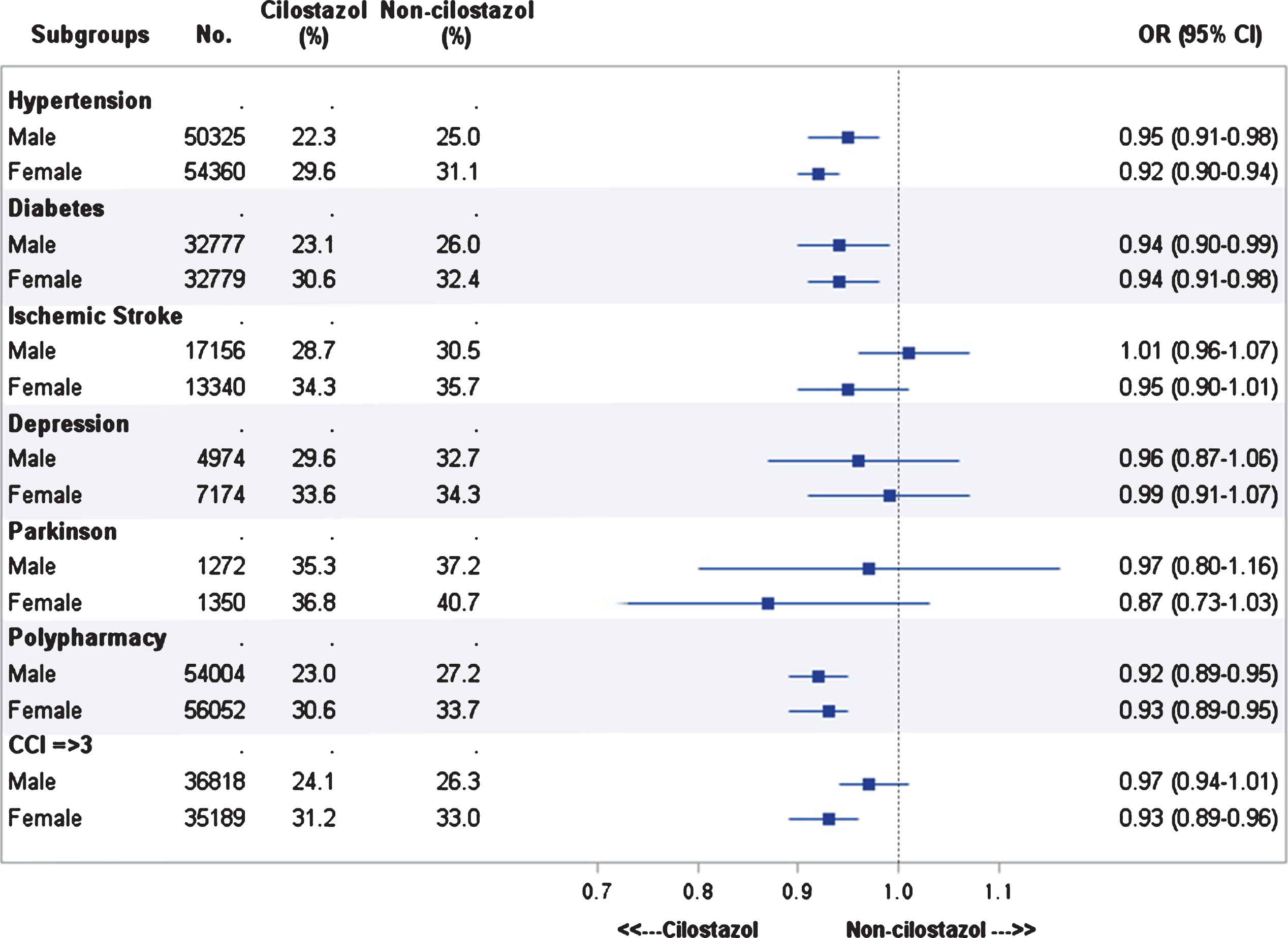
The risk of incident all-cause dementia stratified by sex. Hazard ratios (HR) were calculated using Cox proportional hazard model; CI = confidence interval.
DISCUSSION
Dementia is characterized by the cumulative cognitive decline and progressive inability to live independently. It is a major public health problem with approximately 36 million dementia patients worldwide, which is projected to double every 20 years [30]. In 2010, the estimated worldwide cost of dementia therapy was US$ 604 billion [31]. Thus, the appropriate treatment and care for dementia has a socioeconomic impact on reducing the burden of the disease. The incidence of dementia could be effectively reduced by primary prevention strategies, such as ameliorating its risk factors [32]. Since IHD, as well as ischemic stroke, is a well-known risk factor for dementia, anti-platelet/anti-thrombotic therapy has been suggested to reduce the risk of dementia. In fact, aspirin has been reported to have the potential for preventing dementia [33, 34]. However, there are controversial data reporting no effect of aspirin use on incident dementia. A recent study reported that the use of another anti-platelet/anti-thrombotic agent, cilostazol, reduced the risk of incident dementia, and suggested a possible difference of its effect between patients with and without comorbidities [23]. To the best of our knowledge, the present study is the first population-based propensity-matched cohort study of an Asian population, exploring the role of sex in the relationship between the use of cilostazol and the risk of incident dementia in patients with IHD. Our study yielded several important findings. First, cilostazol use was associated with a reduced risk of incident dementia in patients with IHD. Second, the cumulative duration (>2 years) of cilostazol use was influential in the protective effect of incident dementia. Third, sex was an effect-modifying factor in the relationship between the utilization pattern of cilostazol and the risk of incident dementia.
A previous study regarding the effect of cilostazol in incidence dementia acknowledged some limitations, such as the short observation period and small population size [23]. The present study overcomes these limitation, given the large-scale nationwide cohort with a follow-up period of up to 8 years. In particular, this is the first study to evaluate the differences between sexes regarding the therapeutic effects of cilostazol treatment in patients with IHD. As shown in Table 2, total cilostazol users had a marginally significant lower risk of dementia compared to the control group (HR, 0.98; 95% CI, 0.96–0.98, p < 0.018). After stratification by sex, the protective effect of cilostazol on incident dementia was significant in females but not in males. In particular, female patients treated with cilostazol for >2 years had a remarkably lower risk of incident dementia (HR, 0.85; 95% CI, 0.82–0.88, Table 3), which seems to be clinically meaningful. The sex-related difference in the protective effect of cilostazol could be attributed to sex-related pathophysiological differences and/or hormone-modulated pharmacologic or metabolic differences. In fact, current hormonal treatment in postmenopausal women has been postulated to involve improved blood flow [35 –37]. However, the relationship between hormonal treatment and memory decline or dementia is still largely unknown [38 –40].
Despite the beneficial effects of cilostazol, there are also some concerning reports regarding its use. According to the prescribing information from the US Food and Drug Administration, the patient’s heart rate can increase by approximately 5–7 bpm due to cilostazol. Since patients with a history of IHD may be at risk for exacerbations of angina pectoris or myocardial infarction finally leading to death, several studies including ours have addressed the effect of cilostazol on mortality of patient with IHD and found no significant difference compared with the placebo group [43, 44]. In other randomized clinical trials that included patients who have undergone percutaneous coronary intervention, 0.5–2% of mortality rates have been reported in cilostazol users [41 –44]. These results suggest that the potential risk of cilostazol use should be considered before initiating therapy.
Some limitations in our study have to be noted. First, residual confounding in claims data is a concern that cannot be exclusively ruled out. To minimize this inherent bias and increase the comparability between study groups in the current observational study, we identified drug exposure, age, comorbidities, and polypharmacy of the patients before the index date, and matched cilostazol users and non-users based on propensity scores. Second, this study did not differentiate between the various etiologies of dementia. However, our study might have some meaning because, worldwide, there is much higher rate of diagnoses for unspecified or mixed types of dementia than pure dementia [45, 46]. Third, our study did not include an investigation of the effect of cilostazol against ischemic stroke. Since dementia may be caused by ischemic stroke [47, 48], our results may reflect the stroke-prevention effect of cilostazol. Therefore, further study is needed to investigate the stroke-preventing effects of cilostazol, stratified by sex. Finally, our results were derived from an observational database, and therefore we were not able to conclude whether cilostazol directly protects against dementia. A further prospective randomized trial is needed to demonstrate causality.
In conclusion, the present findings will be valuable in clarifying whether patients with IHD are at lower risk of dementia after cilostazol administration. Our results suggest that the beneficial effect of cilostazol administration, for a period of over 2 years, may be remarkably significant for women with IHD. Given the cardiac benefits of using cilostazol and increase in the increase in its prescription rates, quantifying potential benefits/risks for long-term use of cilostazol is critical in enabling physicians and patients to make informed choices.
Footnotes
ACKNOWLEDGMENTS
This research was supported by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number: HI16C0992, HI18C0920). This research was supported by Support Program for Women in Science, Engineering and Technology through the National Research Foundation of Korea (NRF) funded by the Ministry of Science and ICT (No. 2016H1C3A1903202).