
Abstract
Human Herpes Simplex Virus type 1 (HSV-1) infection is suggested to play a role in the development of Alzheimer’s disease (AD). Immunoglobulin G (IgG) neutralize HSV-1 activity, but the virus can evade IgG-mediated immune responses by expressing receptor that efficiently binds the Fc portion of all IgG subclasses with the exception of IgG3. We analyzed HSV-1-specific IgG subclasses and IgG-mediated serum neutralization activity against HSV-1 in individuals with a diagnosis of either AD or mild cognitive impairment (MCI), comparing the results with those obtained in age-matched healthy controls (HC). 186 individuals were enrolled in the study: 67 AD, 58 MCI, and 61 HC. HSV-1 IgG titers and subclasses, neutralizing antibody (NAb) titers, and complement C3 concentration—critical component of antibody-mediated effector activity—were measured in sera by ELISA; IgG neutralizing activity was performed on HSV-1 infected Vero cells. Results showed that, whereas HSV-1-specific IgG1, IgG2, and IgG4 titers as well as complement C3 serum concentration were comparable in all groups of individuals, IgG3 were more frequently detected in MCI (89%) compared to AD (75%; p < 0.05) and HC (68%; p = 0.003), whereas the titer is similar among the three groups (AD: 0.66±0.21 OD; MCI: 0.68±0.24 OD; HC: 0.72±0.28 OD). Notably, HSV-1 specific neutralizing ability of AD sera was reduced even in the presence of high quantity of IgG3. As IgG3 plays a key role in counteracting the ability of HSV-1 to evade immune responses, these data reinforce the hypothesis of a pathogenetic role of HSV-1 in AD.
Keywords
INTRODUCTION
Alzheimer’s disease (AD), the most common form of dementia, is a chronic neurodegenerative disorder characterized by extracellular plaques, intracellular neurofibrillary tangles and neuronal loss [1]. Mild cognitive impairment (MCI) is defined as a subjective and objective decline in cognitive performance that is greater than expected for an individual’s age and education level, but does not meet criteria for the diagnosis of dementia [1–3]. Elderly MCI patients are at high-risk for developing dementia [4], with an estimated annual rate of MCI conversion to AD ranging between 10% and 15% [5]. The etiopathogenesis of AD is still poorly defined, but both genetic and environmental factors are believed to play roles in the pathogenesis of the disease. A number of genes are suspected to be involved in modulating AD susceptibility, but as of today the only known confirmed genetic risk factor is the ɛ4 allele of the Apolipoprotein E gene (APOE4) [6]; regarding environmental, several infectious agents are suspected to be involved in the disease, and Human Herpes Simplex virus type 1 (HSV-1) has long been suspected to play a crucial role [7, 8].
HSV-1 is a DNA virus belonging to the Herpesviridae family, Alphaherpesvirinae subfamily, that commonly infects human, with about the 90% of the population harboring it by the sixth decade of life [9]. HSV-1, after a usually asymptomatic primary infection, establishes latency in the sensory ganglia of the peripheral nervous system. The virus can then reactivate and come back to the site of primary infection, where it causes new lesions, including skin vesicles or mucosal ulcers [10]. Although rarely, HSV-1 reactivation can cause a very severe form of encephalitis that often results in severe brain damage and death. As is the case with most viruses, HSV-1 can be neutralized by humoral immune response; HSV-1 nevertheless has evolved a number of strategies allowing it to evade such response. Thus, the virus is capable of inhibiting activities mediated by complement [11] and can interfere with immunoglobulin G- (IgG) mediated neutralization secondarily to the expression of a receptor that binds the Fc portion of all IgG subclasses with the exception of IgG3 [12, 13].
Recent data have shown that HSV-1 IgG antibody (Ab) titers are higher in AD compared to HC [14]. To further analyze HSV-1-specific humoral immunity in AD we verified whether the distribution and concentration of HSV-1-specific IgG subclasses differ among AD, MCI, or HC subjects and compared HSV-1-specific neutralizing capacity among these groups.
MATERIAL AND METHODS
Patients and controls
One-hundred-eighty-six individuals were included in the study: 67 AD patients, 58 MCI individuals and 61 sex- and age-matched healthy controls (HC), the majority of them had been previously included in studies finalized at verifying a possible role for HSV-1 in the pathogenesis of AD [15–17]. All subjects were recruited by the Rehabilitative Neurology Unit of the IRCCS Santa Maria Nascente, Don C. Gnocchi Foundation – ONLUS, in Milan, Italy. Patients were diagnosed with probable AD according to the NINCDS-ADRDA criteria [1] or with MCI according to Petersen criteria [18]. AD patients were in mild-moderate stage of the disease as determined by both Clinical Dementia Rating (CDR) scale (CDR, median: 1; interquartile range, IQR: 0.5-1.5) [19] and mini-mental state examination (MMSE) score (MMSE mean±standard deviation: 20.3±3.0) [20]. MCI individuals were required to meet the Grundman operational criteria [21]: memory complaint, confirmed by an informant; abnormal memory function, documented by previous extensive neuropsychological evaluation; normal general cognitive function, as determined by both CDR scale (CDR with at least a 0.5 in the memory domain and MMSE score≥24); no impairment in functional activities of daily living as determined by clinical interview with the patient and informant; no significant cerebral vascular disease (Hachinski score≤4) [22]; no major psychiatric illnesses with particular attention to exclude subjects with history of depression (Hamilton Depression Rating Scale score≤12 [23]. Healthy controls were selected according to the SENIEUR protocol for immuno-gerontological studies of European Community’s Control Action Program on Aging and were unrelated healthy spouses of AD and MCI patients [24]. The cognitive status of HC was assessed by administration of MMSE (score for inclusion as normal control subjects >28). The study conformed to the ethical principles of the Declaration of Helsinki; all subjects or their care-givers gave informed and written consent according to a protocol approved by the local ethics committee of the Don Carlo Gnocchi Foundation – ONLUS, Milan, Italy. For each subject, whole blood and serum samples were collected.
HSV-1, CMV, and HHV-6 IgG analyses
HSV-1, using commercial enzyme-linked immunoassorbent assay (ELISA) (BEIA HSV-1 IgG Technogenetics, Milan), according to standard protocol. To verify that the relation between disease and viral antibody is specific for HSV-1, also cytomegalovirus (CMV) human herpes virus 6 (HHV-6) serum IgG titers were measured for all the subjects, using commercial enzyme-linked immunoassorbent assay (ELISA) (BEIA CMV IgG Quant, Technogenetics, Milan, Italy, and HHV-6 IgG ELISA kit, Abnova, Taiwan), according to standard protocol.
The optical densities (OD) of wells were determined at 450/620 nm. HSV-1 and HHV-6 Ab titers were expressed as antibody index (AI), calculated by dividing OD measurement generated from the assay by OD cut-off calibrator. Subjects with AI >1.1 were seropositive, whereas subjects with AI <0.9 were seronegative. CMV Ab titers were calculated from a calibration curve derived from calibrators included in the kit, and expressed as arbitrary units/ml (AU/ml); samples have been considered positive if AU/ml>10, negative if <8. If the results were in grey zone (AI between 0.9 and 1.1, and AU/ml between 8 and 10), the tests were repeated in triplicated and, if the results remained in grey zone, the subjects should be excluded from the study.
Quantitation of HSV-1 IgG subclasses
Quantitation of the four different HSV-1 IgG subclasses was carried out by an opportunely modified ELISA assay (HSV-1 IgG ELISA, Sigma-Aldrich, St. Louis, MO, US). In particular, after incubation of diluted (1:21) serum samples, four biotinylated subtype-specific monoclonal antibodies (anti-IgG1, -IgG2, -IgG3 and -IgG4, Sigma-Aldrich) and ExtrAvidin®-Peroxidase (Sigma-Aldrich), were separately used to detect the specific IgG subclass. Results were expressed as the OD (measured at 450/620 nm), using as cut-off the mean value + one deviation standard obtained by 10 sera of seronegative subjects.
HSV-1 neutralization assay
Neutralization tests were carried out in Vero cells (African Green monkey kidney cells, ATCC CCL81), cultured in growth medium containing Dulbecco’s Modified Eagle Medium (DMEM, Euroclone, Pero, Italy), supplemented with 2% fetal bovine serum (FBS, HyClone, Logan, UT, US). Serial dilution of sera (in growth medium) were mixed with 50 PFU (plaque-forming unit) of HSV-1, incubated for 1 h at 37°C, inoculated (in triplicates) in cells monolayers in flat bottom cell culture plates 96 well and incubated for 48 h in 5% CO2 at 37°C.
The vitality of Vero cells were measured by trypan blue exclusion test (VWR Life Science, Radnor, PA, USA). Neutralization titers were calculated as the reciprocal of highest dilution showing 50% of neutralization of cytopathic effect (or 50% vitality) after 48 h.
Serum complement C3 concentration
Complement component 3 (C3) was measured in serum of each subject by ELISA assay (C3: Abcam, Cambridge, UK). Optical densities were determined at 450/620 nm. Results were reported as μg/mL based on a standard curve.
ApoE genotyping
Genomic DNA was isolated from whole blood from each subject by phenol-chloroform extraction. Customer-design Taqman probes for the 112 and 158 codons were used to determine the genotype of apolipoprotein E gene (APOE) [17].
Statistical analysis
The parametric data are expressed as mean±standard deviation, whereas the non parametric data as median and interquartile range (IQR). AD, MCI and HC were compared on demographic data using Chi-square test and One-way ANOVA with Bonferroni post hoc test for categorical and continuous variables, respectively. Differences in experimental data among groups were tested using Kruskal-Wallis test and, when appropriate, the Mann Whitney U test, and the correlations using Spearman’s correlation coefficient. p-values corresponding to <0.05 are described as statistically significant in the text. The statistical analyses were accomplished using commercial software (MedCalc Statistical Software version 14.10.2, Ostend, Belgium). A priori power analysis was run with the G-power software [25].
RESULTS
Demographical and clinical characteristics of the subjects
Gender, educational level and age were comparable in the three groups examined; global cognitive levels (MMSE) were, as per definition, significantly reduced in AD and MCI compared to HC (p < 0.0001) and in AD compared to MCI (p < 0.0001). As expected, a significant higher frequency of the APOE ɛ4 carriers was detected in AD patients compared to HC (p = 0.004). Demographic and clinical characteristic of the individuals enrolled in the study are summarized in Table 1.
Demographic and clinical characteristics of subjects enrolled in the study
*p < 0.0001 compared to MCI and HC. **p = 0.004 compared to HC. Data are reported as mean±standard deviation. AD, Alzheimer’s disease; MCI, mild cognitive impairment; M, male; F, female; MMSE, Mini-Mental State Evaluation; APOE, Apolipoprotein E.
Viral seroprevalence and antibody titers
No differences were observed between the three groups when HSV-1 seroprevalence was evaluated (AD: 95%; MCI: 95%; HC: 93%). Results confirmed previously published data showing that higher HSV-1 titers were found in AD (median: 9.10; IQR: 7.15–10.12 AI) and MCI individuals (8.50; 7.70–9.76 AI) compared to HC (7.55; 6.91–8.04 AI; AD versus HC: p = 0.004; MCI versus HC: p = 0.04) (Fig. 1) [14].
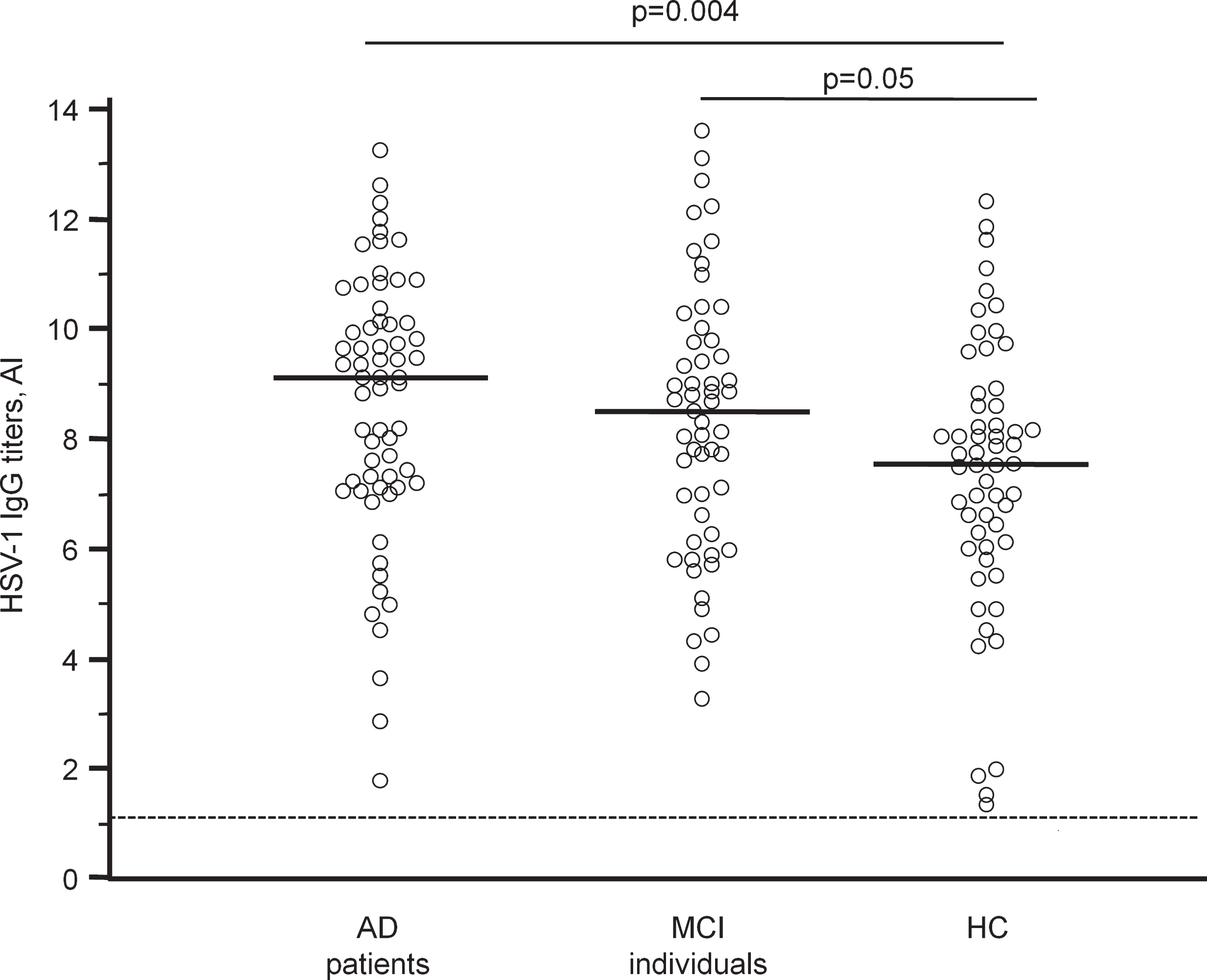
HSV-1-specific antibodies in AD, MCI and HC. Horizontal lines represent the median value. Dotted line represents threshold value of seropositivity.
The prevalence and titers of Ab anti-CMV and -HHV-6, two other ubiquitous viruses that have been suspected to play a role in AD, were analyzed as well in all the individual enrolled in the study; no differences were observed either in seroprevalence or titers among the three groups (data not shown). No grey zone results were observed for HSV-1, CMV, and HHV-6 seropositivity measurement.
As no differences among the three groups were observed for CMV and HHV-6 antibodies, for the next steps we focused on HSV-1, considering only HSV-1 seropositive subjects: 64 AD patients, 55 MCI individuals and 57 HC. All the HSV-1 seronegative subjects were excluded from the following analyses.
HSV-1 IgG subclasses
Four IgG subclasses are known; the frequency of each one of these subclasses was analyzed next among the three groups. Results showed that, whereas the frequency of sera in which HSV-1-specific IgG1, IgG2 and IgG4 were observed, was comparable in AD, MCI and HC individuals, a significantly higher percentage of sera from MCI individuals (50/55 or 89 %) contained HSV-1-specific IgG3 compared to AD patients (48/64, or 75 %) and HC (38/57 or 68 %) (MCI vs. AD p < 0.05; MCI vs. HC p = 0.003) (Table 2).
Serum quantitation of HSV-1-specific IgG subclasses were analyzed next; no significant differences emerged (Table 2). Finally a positive correlation was found between IgG1 and total IgG in AD (p = 0.0001) and HC (p < 0.05), but not in MCI. In MCI alone, though, a positive correlation was detected between IgG3 and total IgG (p < 0.05). No correlation was observed with MMSE score or APOE ɛ4 status.
HSV-1 neutralization assay
HSV-1 neutralizing antibody titer was measured next using sera of individuals in whom either high (>75th percentile: 0.841 OD) or low (<25th percentile: 0.478 OD) serum concentrations of IgG3 were present; notably, the concentration of the other IgG subclasses was comparable in these sera. The neutralization assay was performed with sera of 9 subjects with high IgG3 concentration (3 AD, 3 MCI, 3 HC) and 9 individuals with low IgG3 concentration (3 AD, 3 MCI, 3 HC).
Low neutralizing ability (neutralizing antibody – NAb – titers <100) characterized AD, MCI, and HC sera in whom low IgG3 concentrations were observed. Neutralizing ability of MCI and HC sera in whom high IgG3 concentration were detected was, as expected, high (NAb = 150), notably, though, the neutralizing ability of AD sera with high IgG3 titers was low (NAb < 100). Thus, these data suggest that the neutralizing activity of AD patients serum is reduced indipendenlty of its IgG3 content.
No correlation was observed between NAb and IgG subclasses, MMSE score or APOE ɛ4 status.
Complement C3 fraction concentration in serum
As the complement system, and in particular complement fragment 3 (C3), plays a critical role in mediating Ab-mediated immune effector mechanisms, C3 concentration was evaluated in sera of all the individuals enrolled in the study. C3 serum concentration was not significantly different in the three groups analyzed (AD: 952.42; 858.44–1016.50μg/mL; MCI: 940.70; 781.03–1029.23μg/mL; HC: 992.04; 864.50–1050.25μg/mL), but, interestingly, C3 serum concentration was negatively correlated with total HSV-1-specific Ab titers in MCI (p = 0.02). No correlations were observed between complement C3 and IgG subclasses, NAb, MMSE score or APOE ɛ-4 status.
DISCUSSION
HSV-1, a ubiquitous virus, has long been suspected to have a role in the development of AD [7]; this hypothesis has been reinforced by new immunologic and virologic evidences [8]. In particular, we have recently shown in AD patients that HSV-1 titers are positively correlated with grey matter volume in the brain area typically affected by the disease [14]. Additionally, in MCI, a condition that can predispose to the development of AD, we observed that the avidity of HSV-1-specific IgG is inversely correlated with the likelihood of AD conversion [16], suggesting that HSV-1 IgG specific antibodies may play a protective role against AD.
Herein we analyzed the distribution of the four different subclasses of HSV-1-specific IgG antibodies in AD and MCI subjects as well as in age-and sex-matched healthy controls. Results showed that the frequency of HSV-1 IgG3 was significantly higher in MCI compared to AD and HC. Importantly, whereas a positive correlation between total IgG and IgG1 in serum was observed in AD and HC, in MCI total IgG positively correlated with IgG3 and not with IgG1. This result is unexpected as IgG1, commonly elicited by viral infections [26], is the IgG subclass mainly present in human serum.
HSV-1-specific IgG subclasses
#considering only HSV-1 seropositive subjects. *p = 0.04 versus MCI. **p = 0.003 versus MCI. Data are reported as percentages. AD, Alzheimer’s disease; MCI, mild cognitive impairment.
IgG3 antibodies have a molecular mass of 170 KDa [27] and are characterized by a hinge region that is longer than the one seen in other IgG subclasses. This allows IgG3 to form a poly-proline helix with much more flexibility compared to the other subclasses [28, 29]. IgG3 antibodies are functionally characterized by having the shortest half-life of all the IgG subclasses; because these antibodies are very effective in inducing effector responses, their short half life could be a mechanism that limits excessive inflammatory responses [27]. Functionally, IgG3 are endowed with the strongest capacity to activate the complement cascade through the classical pathway and, together with IgG1, can ligate and activate phagocytosis by macrophages via the ability of their Fc to bind to a specific receptor on the surface of these cells. On the other hand, IgG3 poorly stimulate basophils and mast cells. Viral infections commonly lead to the generation of IgG antibodies of the IgG1 and IgG3 subclasses, with IgG3 antibodies appearing first in the course of infection [30]. HSV-1, in particular, expresses in the virion envelope a receptor that binds the Fc portion of IgG [31]; this interaction hampers IgG ability to neutralize the virus, allowing the virus to evade host immune response [32]. Importantly, the Fc-specific HSV-1 receptor can interact with all the IgG subclasses with the exception of IgG3 [12, 13]. Several works support the hypothesis that the frequency and the intensity of HSV-1 reactivation may play a key role in the development of AD [33–37]; as a consequence, the ability to impede HSV-1 reactivation may be an important factor in preventing MCI conversion into AD. The finding that HSV-1 IgG3 are significantly more common in MCI may reflect the attempt of these individuals to suppress HSV-1 reactivation by augmenting the expression of the only one IgG subclass that is not blocked by the viral Fc protein receptor.
IgG3, together with IgG4, are endowed with the highest neutralizing capacity against HSV-1 infection, even in comparison with the more abundant IgG1 [38, 39]. The neutralization activity of sera, i.e., the ability of antibodies to block HSV-1 infection, was tested next by comparing the neutralizing activity of sera with high or low IgG3 titers. As expected, low IgG3 serum quantity corresponded with low neutralizing capacity in all the three groups of individuals analyzed, without any differences being observed. Surprisingly, though, in serum of AD patients alone neutralizing activity remained low even when high IgG3 quantity sera were analyzed. These findings, although needing confirmation by independent studies in larger cohorts of patients, seem to suggest that in AD the ability of IgG3 to neutralize HSV-1 is impaired. This is in contrast with what is observed in MCI: in these individuals the immune response against HSV-1 is still robust and efficient, or at least is very similar to that observed in age-matched healthy controls. Notably a limitation of the study is that IgG subclasses were not purified, as the available amount of serum was not sufficient for the purification process. Nevertheless, the observation that the sera selected to analyze neutralization ability differed only for IgG3, with a similar concentration for all the other 3 subclasses, seems to lend support to our interpretation of the results. However, other experiments based on functional study of IgG3 are necessary to better understand the significance of our results.
The complement system functions as an immune surveillance system that rapidly responds to viral infection. As an important arm of the humoral immune response, the complement system quickly targets and eliminates virus particles and interacts with the surface of virus-infected cells to mark them for destruction by other effector mechanisms of the immune response [40]. Viruses have developed several strategies to evade the complement system. In particular HSV-1 encodes several surface glycoproteins that block the activation of complement cascade, among which glycoprotein C (gC) that, by binding complement C3 fragment, [41] protects HSV-infected cells from complement-mediated lysis [42] and cell-free virus complement-mediated neutralization [43, 44]. For this reason, C3 serum concentration was measured next to verify the possibility that reduced complement concentrations could be responsible for the low neutralizing activity of sera of AD subjects with high IgG3 titers. This was not the case, as C3 serum titers were comparable in the three groups of individuals. Notably, C3 serum concentration negatively correlated with total HSV-1 Ab titers in MCI individuals alone. The potential significance of this observation is being investigated.
In conclusion, these results indicate that HSV-1-specific IgG subclasses are differently distributed when AD and MCI individuals are compared to HC. Although the IgG1 subclass response is the predominant type against HSV-1 in all the group analyzed, IgG3 response is significantly more frequent in MCI individuals compared the other groups. These findings are interesting, because the structural and functional properties of the IgG subclasses vary, and, in the case of HSV-1 infection, HSV-1 is not able to interfere with IgG3 function in its immune evasion strategy. The decreased ability of sera from AD to neutralize HSV-1 independently of either IgG3 or C3 titers is surprising: further studies are in progress to understand the potential biological importance of these results.
Footnotes
ACKNOWLEDGMENTS
The authors thank Laura Granata MD and Gioconda Carabellese, MD for taking care of the patients who participated in the study, as well as Dr. Enrico Ripamonti for statistical support.
This work was supported by 2016-2017 Ricerca Corrente (Italian Ministry of Health).