
Abstract
Background:
Clinical practice guidelines for dementia highlight the importance of providing patient-centered care. This can be achieved by improving health professionals’ attitudes and knowledge toward people with dementia.
Objective:
Quantitatively evaluate the impact of a virtual dementia experience on medical and pharmacy students’ knowledge and attitudes toward people with dementia.
Methods:
A non-randomized controlled study from September-October 2016. The intervention group received a 1.5-hour multisensory, virtual simulation of light, sound, color, and visual content to experience the cognitive and perceptual difficulties faced by people with dementia. Controls participated in the standard curriculum only. All students were invited to complete the 20-item Dementia Attitudes Scale (DAS) pre- and post-intervention.
Results:
A total of 278 students (n = 64 medical, n = 214 pharmacy) were analyzed (n = 80 intervention, n = 198 control). The majority of students were female (n = 184, 66.2%), with an average age of 22.5 years. The intervention improved the DAS total score and subdomains of comfort and knowledge (p < 0.001).
Conclusion:
The intervention had a positive impact on medical and pharmacy students’ knowledge and attitudes toward people with dementia.
INTRODUCTION
The World Alzheimer Report 2016 and UK National Institute for Health and Care Excellence (NICE) guidelines highlight the importance of considering the context, values, and preferences of people with dementia [1, 2]. Additionally, the Australian Clinical Practice Guidelines and Principles of Care for People with Dementia recommend that physicians, nurses, allied health and care workers receive training in effective communication with people with dementia, carers, and family members [3]. Despite this, current healthcare systems often provide care perceived as unresponsive to the needs of people with dementia and their families [2].
The quality of dementia education provided to future medical practitioners and pharmacists is an important focus [4]. However, didactic lecture-based education and clinical placements may not effectively promote person-centered healthcare. Tullo et al. found that dementia-specific education provided by 23 UK medical schools primarily focused on knowledge and skills rather than behaviors and attitudes [5]. Additionally, pharmacy education is often focused on medication properties, rather than patient needs and experiences [6], or the skills required to effectively communicate with specific patient groups [7]. There is often limited opportunity during university training for medical and pharmacy students to understand the physical and cognitive impact of dementia, despite evidence to suggest that nonclinical experiential education may improve attitudes towards people with dementia [8].
Few studies have explored the impact of dementia-focused educational interventions on healthcare student attitudes. Participation in a 90-minute group-based creative storytelling program significantly improved attitudes (p < 0.05) of 22 fourth-year medical students across 12 of the 20 Dementia Attitudes Scale (DAS) items [8]. Comfort and knowledge significantly improved (p≤0.01) following 20 preclinical first year medical students participating in a single 90-minute community-based arts program [9]. Finally, of 52 pharmacy students, 40% of students felt an increase in their empathy, and 50% felt an increase in their knowledge regarding suitable behavior, following an educational module involving visual and textual patient and caregiver narratives [10].
Most previous educational initiatives have improved only some attitudinal items, used relatively small samples sizes, and not incorporated a control group. The research team is unaware of published research into healthcare student-focused dementia education with a virtual component. As a result, this study quantitatively evaluated the impact of a virtual dementia experience on medical and pharmacy students’ knowledge and attitudes toward people with dementia.
MATERIALS AND METHODS
Study design
A two-group, non-randomized controlled study for medical and pharmacy students was conducted from September to October 2016.
Participants
The participants were third year (of a five year) Bachelor of Medicine and Bachelor of Surgery (n = 69) and fourth year (of a four year) Bachelor of Pharmacy students (n = 229). The intervention was offered to students in these year levels because it was considered complementary to their clinical placements. Dementia education at the participating university is currently targeted toward understanding how to use cognitive tests and medications for diagnosis, monitoring, and treatment, and there is limited non-clinical education designed to assist students with understanding the physical and cognitive impact of dementia.
Recruitment
In September 2016, medical and pharmacy students received a face-to-face presentation by the principal investigator outlining the study prior to a single lecture (medical students) or multiple tutorials (pharmacy students). Students were provided with a copy of the study explanatory statement via their online learning platform and were asked to read it prior to attending the above presentation. Implied consent to participate in the study, which involved evaluating the intervention, was received upon submission of an anonymous questionnaire. Consent was not required to undertake the intervention.
Intervention and control group allocation
Medical students were allocated to either the intervention group (i.e., undertook the intervention during the course of the study) or the control group (i.e., undertook the intervention after the study had concluded) based on their tutorial group. Tutorial groups were randomly allocated at the start of the academic year; however, the allocation of each tutorial group to the intervention or control group was based on availability according to the existing clinical placement timetable.
All pharmacy students were asked to express their interest in participating in the study. Pharmacy students who expressed an interest in and were able to attend one of the scheduled intervention sessions comprised the intervention group. The pharmacy students who were not able to attend one of the scheduled sessions or did not express an interest in participating in the study comprised the control group.
Intervention
The 1.5-hour intervention was delivered from September to October 2016 as part of the Alzheimer’s Australia Vic Virtual Dementia ExperienceTM (https://vic.fightdementia.org.au/vic/about-us/virtual-dementia-experience), provided at the Perc Walkley Dementia Learning Centre in Melbourne, Australia, and developed in consultation with people with dementia and their carers. The intervention involved a multisensory, virtual simulation of light, sound, color, and visual content that allowed participants to experience the cognitive and perceptual difficulties faced by people with dementia, as well as facilitator-guided personal reflection and follow-up group discussion. The intervention allowed students to consider improved approaches to caring for people with dementia, environmental issues facing a person with dementia, and work environment modifications to address these.
Evaluation
The impact of the intervention was evaluated using the 20-item Dementia Attitudes Scale (DAS) [11]. The DAS is a widely used scale that was originally developed via structured interviews, exploratory factor analysis, convergent validity testing and confirmatory factor analysis [9, 12]. It reflects the affective and cognitive components of attitude and has been used previously in research involving medical and nursing students [9, 12]. The 20 DAS items includes six reverse scored items. Responses are recorded using a 7 point Likert-type scale from 1 (strongly disagree) to 7 (strongly agree). Questions 1, 2, 4, 5, 6, 8, 9, 13, 16, 17 comprise the DAS subdomain of ‘comfort’ (i.e., comfort associated with interacting with people with dementia) and questions 3, 7, 10, 11, 12, 14, 15, 18, 19, 20 comprise the ‘knowledge’ subdomain [11]. A minor amendment to the DAS was made, where the acronym ‘ADRD’ (corresponding to ‘Alzheimer’s disease and related dementias’) was replaced with ‘dementia’ to facilitate ease of reading. The research team and 11 research pharmacists assessed questionnaires for face and content validity. Following this assessment, additional explanatory information was included in the questionnaire, instructing students to consider questions in the context of working as a healthcare professional, and to respond to questions based on their current perception/understanding/opinion, regardless of the amount of prior experience working with people with dementia.
The DAS was administered via an anonymous, hard copy questionnaire. Hardcopy questionnaires were used, to combat lower response rates observed with internet-based [13] or emailed questionnaires [14]. The baseline and follow-up questionnaires were exactly the same and both medical and pharmacy students received the same questionnaire. Questionnaires comprised three initial questions to facilitate linkage of baseline and follow-up questionnaires, seven demographic questions, and the 20-item DAS [11]. The follow-up questionnaire also included one question asking students whether they had undertaken the intervention.
During recruitment (September 2016), students were provided with a baseline questionnaire and invited to complete it upon receipt. In October 2016, follow-up questionnaires were provided to students prior to the commencement of a single lecture (medical students) or multiple tutorials (pharmacy students).
Statistical analyses
Mean changes from baseline to follow-up were compared between intervention and control groups using analysis of covariance with adjustment for its baseline value yielding a difference of differences that can be interpreted as a comparison of changes. Additional adjustments were made for demographic data including gender, age, birthplace of student (born in Australia with at least one parent born in Australia, born in Australia but both parents born overseas, born overseas), had a family member/relative/friend with dementia, and worked in a professional practice environment. In keeping with findings of a previous study [8], mean Likert scale responses were reported as opposed to medians [15]. Questionnaire data were included in analyses if both a baseline and corresponding follow-up questionnaire were present and could be matched. A significance level of p < 0.05 was used for all analyses.
Ethical approval
This study was approved by the Monash University Human Research Ethics Committee (CF16/2157 – 2016001061). The explanatory statement outlined that participation was voluntary and would not contribute to university grades, students who chose not to participate in the study would not be disadvantaged in any way, and students could withdraw from further study participation at any stage.
RESULTS
In September 2016, 68 medical students (68/69 = 98.6% response rate, Fig. 1) and 223 pharmacy students completed a baseline questionnaire (223/229 = 97.4% response rate) respectively. Of these, four medical and nine pharmacy student questionnaires did not have a matching follow-up questionnaire. Forty-one medical and 42 pharmacy students (from 92 who had expressed an interest) attended one of the nine intervention sessions scheduled from September to October 2016. Reasons why pharmacy students did not undertake the intervention, despite expressing an interest, included: not being available when the intervention session was scheduled, no longer interested in undertaking the intervention, being unwell, not responding to email contact, and incorrect contact details provided to the research team.
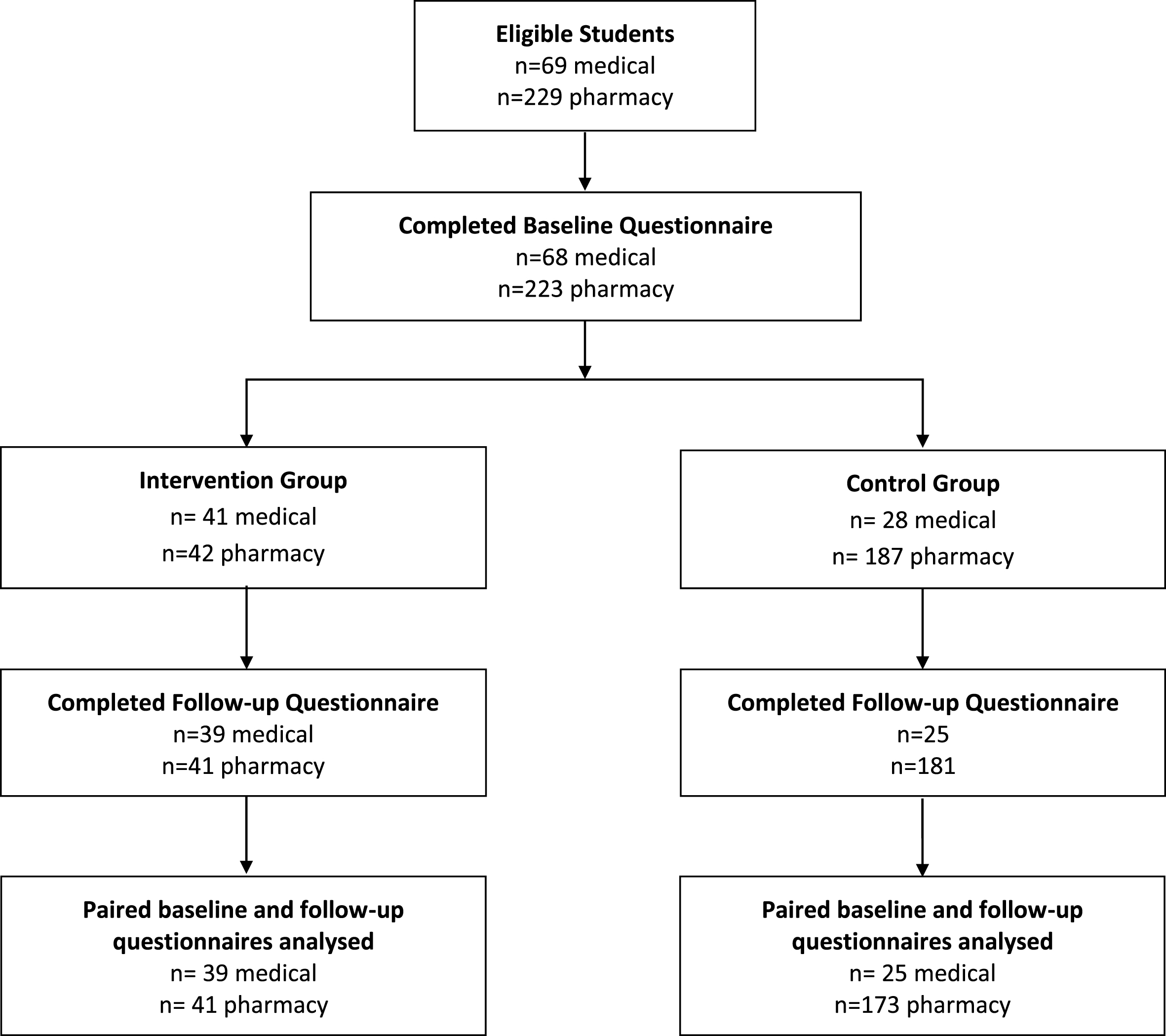
Study overview.
Both intervention and control group students completed follow-up questionnaires in October 2016. Of the 41 medical students in the intervention group, 39 completed a follow-up questionnaire (95.1%) and of the 42 pharmacy students, 41 completed a follow-up questionnaire (97.6%). Twenty-five medical students (25/28 = 89.3%) and 181 pharmacy students in the control group completed a follow-up questionnaire (181/187 = 96.8%). Of these, zero medical and eight pharmacy student questionnaires did not have a matching baseline questionnaire. The students who were excluded due to not having a follow-up questionnaire available for analyses had similar baseline characteristics to students included in analyses.
A total of 278 students (n = 64 medical, n = 214 pharmacy) were analyzed (Table 1). Eighty students comprised the intervention group and 198 comprised the control group. Participants were mostly female (n = 184, 66.2%), with an average age of 22.5 years.
Demographic characteristics
For the combined group of both medical and pharmacy students, the intervention group showed a significantly greater change in DAS scores compared to the control group with p < 0.05 for all DAS items (Table 2). A significant improvement was also identified in the DAS subdomains of comfort and knowledge, and in the total score with p < 0.01.
Combined medical and pharmacy students’ Likert scale responses
C, Comfort subdomain; K, Knowledge subdomain; O, Overall score from all 20 DAS items; sd, standard deviation; CI, confidence interval.
For medical students, the intervention group showed a significantly greater change in DAS scores compared to the control group with p < 0.05 for all DAS items except item 3, 14, 19, and 20 (Table 3). A significant improvement was also identified in the DAS subdomains of comfort and knowledge, and in the total score (p < 0.01).
Medical students’ Likert scale responses
C, Comfort subdomain; K, Knowledge subdomain; O, Overall score from all 20 DAS items; sd, standard deviation; CI, confidence interval.
For pharmacy students, the intervention group showed a significantly greater change in DAS scores compared to the control group with p < 0.05 for all DAS items except item 6 (Table 4). A significant improvement was also identified in the DAS subdomains of comfort and knowledge, and in the total score (p < 0.01).
Pharmacy students’ Likert scale responses
C, Comfort subdomain; K, Knowledge subdomain; O, Overall score from all 20 DAS items; sd, standard deviation; CI, confidence interval.
DISCUSSION
A virtual dementia experience positively impacted medical and pharmacy students’ knowledge and attitudes toward people with dementia. All 20 DAS items in the combined group (p < 0.05) and the majority of the 20 DAS items for medical or pharmacy students alone significantly improved [11]. A significant improvement was identified in both the DAS subdomains of comfort and knowledge and in the total score (p < 0.01) for all three groups. No other published study has explored the impact of an educational intervention with a virtual component on the attitudes of a large sample of medical and pharmacy students (n = 298). However, similarities between the current study and Wijma et al.’s evaluation of virtual dementia education for informal caregivers or people with dementia were identified, including greater understanding and insight into the experience of people with dementia [16]. Knowledge gained from this study can provide an evidence base to incorporate educational interventions with a virtual component into the curriculum of medical and pharmacy university students.
Four of the 20 DAS items that were related to dementia knowledge (people with dementia can be creative, and can enjoy life, we can do a lot now to improve the lives of people with dementia, and difficult behaviors may be a form of communication), did not significantly improve in medical students (p > 0.05). By comparison, only one of the 20 DAS items that was related to comfort (I feel uncomfortable being around people with dementia) did not significantly improve in pharmacy students (p > 0.05). These findings suggest that the virtual experience may complement rather than replace knowledge-based university education.
Limited previous research evaluating the impact of educational interventions on healthcare student attitude toward people with dementia have shown significant improvements in some DAS items; however, smaller sample sizes have been used with varying success. George et al.’s 22 fourth-year medical students showed a significant improvement in attitudes across only 12 of the 20 DAS items (p < 0.05) [8], despite significant improvements in the knowledge (p = 0.001) and comfort (p < 0.001) subdomains and in the overall DAS scale score (p < 0.001) [8]. While Roberts et al.’s study of 20 preclinical first year medical students did not present attitude changes by individual DAS item, despite showing a significant improvement in subdomain DAS scores (p≤0.01) [9]. Finally, Zimmermann did not use the DAS score when evaluating the impact on pharmacy student empathy and knowledge regarding suitable behavior toward people with dementia and their caregivers [10]. Limitations of previously conducted educational studies have been addressed in this study, via incorporating a control group and a large student sample size (n = 278) [8, 9]. Additionally, previous studies did not evaluate the impact of an educational intervention with a virtual component [17], but instead, evaluated the impact of a creative storytelling program [8], a community-based arts program [9] and an educational module involving visual and textual patient and caregiver narratives [10].
Strengths and limitations
The study evaluated an engaging and reproducible intervention that improved attributes of healthcare professionals valued by people with dementia. It is a strength that this study evaluated an intervention that was developed in consultation with people with dementia and their carers, and that high questionnaire response rates were achieved. It is also a strength that this study used a larger sample size than in previous research, and that the 95% CIs were sufficiently narrow to be able to make strong conclusions about the existence of an intervention effect, including the overall DAS score (12.6, 17.3) and the scores for the comfort (7.6, 10.7) and knowledge (4.5, 7.5) domains, in the combined group.
Similarly to other studies exploring the impact of educational interventions on students, it was not possible to randomly allocate students to intervention or control groups due to curricula and recruitment restrictions. Medical students were purposively allocated to the intervention or control group within the constraints of their existing class timetables and pharmacy students were self-selected. There is the possibility that pharmacy students who expressed an interest in undertaking the intervention were more receptive to attitudinal change. However, demographic characteristics were not significantly different between the intervention and control group, apart from age. Additionally, analyses only included students who had completed both a baseline and matching follow-up questionnaire as it is not justified to assume that analysis methods can compensate for missing data [18]. Lastly, future research should explore whether the impact of the intervention on student attitudes is sustained over time and the impact of attitudes on future practice.
A virtual dementia experience had a positive impact on medical and pharmacy students’ knowledge and attitudes toward people with dementia. A significant difference was identified in the DAS subdomains of comfort and knowledge, and in the total score for all three study groups (p < 0.01). Future research should explore the sustained impact of the intervention and impact on future healthcare practice.
Footnotes
ACKNOWLEDGMENTS
Dr. Gilmartin-Thomas is a National Health and Medical Research Council (NHMRC) – Australian Research Council (ARC) Dementia Research Development Fellow. A/Prof Bell is a NHMRC Dementia Leadership Fellow. The authors would like to acknowledge the assistance provided by Liana Moore (Clinical Site Administrator, Monash University Central Clinical School) and the support provided by Alzheimer’s Australia Vic (Parkville, Melbourne). Please note, Alzheimer’s Australia Victoria is now known as Dementia Australia.
This work was supported by a Monash Education Academy Small Grant, co-author JS Bell and the Medical Student Programs (CCS).