
Abstract
Background:
While many studies focus on the prognosis of individual neurological diseases, very few comprehensively compare and analyze real-world data of these diseases.
Objective:
To address this gap in knowledge, in this study, we comprehensively analyzed the real-life data of patients with neurological diseases.
Methods:
We prospectively enrolled patients with neurological diseases at three hospitals from December 1, 2016 to September 30, 2020. Neurological diseases were classified into nine groups: Dementia, Cerebrovascular disease, Parkinson’s and related, Functional, Spinocerebellar degeneration, Neuroimmune, Epilepsy, Muscle dystrophy disease, and Hypertension. Patients were followed up for three years, and their prognosis and evaluation of their cognitive function served as the endpoint.
Results:
A total of 426 patients were finally enrolled. Both mortality and cognitive function differed among the neurological disease categories. After 3 years, mortality was highest in the Dementia (25.5%), Parkinson’s and related (21.6%), and Spinocerebellar degeneration (35.3%) groups while the cognitive function of patients in these three groups was significantly lowest.
Conclusions:
When the neurological diseases were holistically observed, both mortality and cognitive function of the Dementia, Parkinson’s and related, and Spinocerebellar degeneration groups were significantly worse than the remaining diseases.
Keywords
INTRODUCTION
Neurological diseases such as dementia, cerebrovascular disease (CVD), Parkinson’s disease (PD), and others are important medical issues due to their rapid advancement in aging societies, especially in advanced countries [1–3]. Several studies suggest that societies will face challenges due to these neurological diseases in the near future [4, 5], so they should prepare and take measures to overcome a potential crisis. However, comprehensive real-world studies that analyze neurological diseases linked with aging are lacking, even though there are many studies that focus separately on each neurological disease prognosis [6–8]. A comprehensive analysis of the prognosis of neurological diseases is important because it provides actual information and reveals which aspects need to be focused on to prevent future crises in societies related to these diseases.
Here, we report on the Tochigi Neurological Disease Cohort Study in which we comprehensively analyzed the real-life data of patients in Tochigi (a Japanese prefecture) with neurological diseases over a 3-year period.
METHODS
Study design
The Tochigi Neurological Disease Cohort Study was conducted at three hospitals in Tochigi: Jichi Medical University, Kamitsuga General Hospital, and Imai Hospital. Patients with neurological diseases were prospectively enrolled between December 1, 2016 and September 30, 2020. The follow-up period was three years in which patients’ prognosis and cognitive functions were evaluated.
The Ethical Committees of Jichi Medical University, Kamitsuga General Hospital, and Imai Hospital approved this study, which was exempted from institutional review board approval based on our guidelines (approval no.: Rin-A 22-009). All patients or their family members provided informed consent regarding participation in this study.
Patients
Only patients 50 years old or older were enrolled in this study. These were patients who had been admitted to the neurological departments of these three hospitals, and they were classified into one of nine groups of neurological diseases: Dementia, CVD, Parkinson’s and related, Functional, Spinocerebellar degeneration (SCD), Neuroimmune, Epilepsy, Muscle dystrophy disease (MDD), and Hypertension. To analyze the neurological disease results, the Hypertension group was set as the disease control. The Dementia group included Alzheimer’s disease, vascular dementia, dementia with Lewy bodies, and frontotemporal dementia. The CVD group included past ischemic stroke, transient ischemic attack, and intracranial hemorrhage. Past ischemic stroke was further classified into atherosclerosis, cardioembolism, lacunar, other, and unknown based on the trial of ORG 10172 in acute stroke treatment (TOAST) criteria [9]. The Parkinson’s and related group included PD, corticobasal syndrome (CBS), and progressive nuclear palsy (PSP). The Functional group included rapid eye movement sleep behavior disorder, headaches, and essential tremors. The SCD group included multiple systemic atrophy and spinocerebellar ataxia. The Neuroimmune group included myasthenia gravis, multiple sclerosis, neuromyelitis optica, and anti-myelin oligodendrocyte glycoprotein-associated diseases. The Epilepsy group consisted of epilepsy, the MDD group consisted of muscular dystrophy disease, and the Hypertension group consisted of hypertension. In order to classify these diseases into the nine groups, we referred to the pathological policy and characteristics of these neurological disease [10, 11].
The diagnosis of each disease was based on disease diagnostic criteria or related standards, as described in the Supplementary Material. The classification of diseases was based on the disease at the time of enrollment.
Assessment
For each patient, we recorded their age, sex, presence or past history of atrial fibrillation, heart failure, diabetes mellitus, coronary artery disease, malignant tumor, mortality, and transfer or treatment withdrawal, except due to death, during the follow-up period. Furthermore, we examined their cognitive function, using the Mini-Mental State Examination (MMSE), the Revised Hasegawa’s Dementia Scale (HDS-R), and frontal assessment battery (FAB), at baseline, 1-, 2-, and 3-year follow-ups.
Statistical analyses
All statistical analyses were performed using statistical software (JMP 17; SAS Institute Inc., Cary, NC, USA). The baseline and clinical data of the nine groups are expressed as the mean±standard deviation (Tables) or as the mean±standard error (Figures). Cumulative survival data were estimated and plotted by a Kaplan–Meier analysis. The cognitive function of each group compared to the Hypertension group was analyzed by the Steel-Dwass test. A p-value < 0.05 was considered statistically significant.
RESULTS
Participant characteristics
A total of 426 patients were finally enrolled in this study. Details of the patients, including their number, age, gender, presence or past history of atrial fibrillation, heart failure, diabetes mellitus, coronary artery disease, and malignant tumor, as well as neurological disease group, are shown in Table 1. All members of the MDD group displayed myotonic dystrophy.
Patient characteristics
AF, atrial fibrillation; DM, diabetes mellitus; HF, heart failure; MOG, myelin oligodendrocyte glycoprotein; MT, malignant tumor; OMI, old myocardial infarction; SD, standard deviation.
Mortality separated with neurological disease group
Mortality, and the transfer or treatment withdrawal rate of each neurological disease group are shown in Fig. 1. The Kaplan–Meier plots indicate a significant difference among the nine groups (Fig. 1A, p < 0.001). Following the 3-year follow-up period, compared to 4.6% mortality in the Hypertension group, mortality was 25.5% in Dementia, 7.5% in CVD, 21.6% in Parkinson’s and related, 6.1% in Functional, 35.3% in SCD, and 0% in Neuroimmune, Epilepsy, and MDD groups (Fig. 1B).

Prognosis separated the nine neurological disease groups. A) Kaplan–Meier plots of each neurological disease. B) The proportion of mortality, transfer or withdraw, and survival (with continued hospital visits) for each neurological disease.
Cognitive function separated by neurological disease group
The cognitive function of MMSE, HDS-R, and FAB scores of each neurological disease group is shown in Fig. 2 and Table 2. The MMSE scores of patients in the Dementia group at baseline, 1-, 2-, and 3-year follow-ups were significantly lower than those of patients in the Hypertension group (Fig. 2A). The HDS-R scores of patients in the SCD group at baseline, of patients in the Parkinson’s and related group after 3 years, and of patients in the Dementia group at baseline, and after 1-, 2-, and 3-year follow-ups, were significantly lower than the HDS-R scores of patients in the Hypertension group (Fig. 2B). The FAB scores of patients in the Parkinson’s and related as well as Dementia groups at baseline, and after 1-, 2-, and 3-year follow-ups, were significantly lower than those of patients in the Hypertension group (Fig. 2C).

Cognitive function separated based on neurological disease group. (A) MMSE, (B) HDS-R, and (C) FAB of each neurological disease.
Patient cognitive function
FAB, Frontal Assessment Battery; HDS-R, Revised Hasegawa’s dementia scale; MMSE, Mini-Mental State Examination; SD, Standard deviation.
Cognitive function separated based on each neurological subgroup
We also analyzed cognitive function, which was separated based on each neurological subgroup. These results are shown in Figs. 3 and 4. The MMSE, HDS-R, and FAB scores were not significantly different between the baseline, 1-, 2-, or 3-year follow-ups in Dementia, CVD, Functional, SCD, and Neuroimmune subgroups (Fig. 3A, B, and Fig. 4A–C). In contrast, according to the sub-group analysis of the Parkinson’s and related group, compared to the MMSE score of PD, the scores of CBS after 2- and 3-year follow-ups, and those of PSP at baseline and after the 1-year follow-up, were significantly lower (Fig. 3C, left). Compared to the HDS-R score of PD, the scores of CBS after the 1- and 3-year follow-ups, and those of PSP at baseline and after the 1-year follow-up, were significantly lower (Fig. 3C, middle). Compared to the FAB score of PD, the scores of CBS after the 2- and 3-year follow-ups, and those of PSP at baseline and after the 1-year follow-up, were significantly lower (Fig. 3C, right).
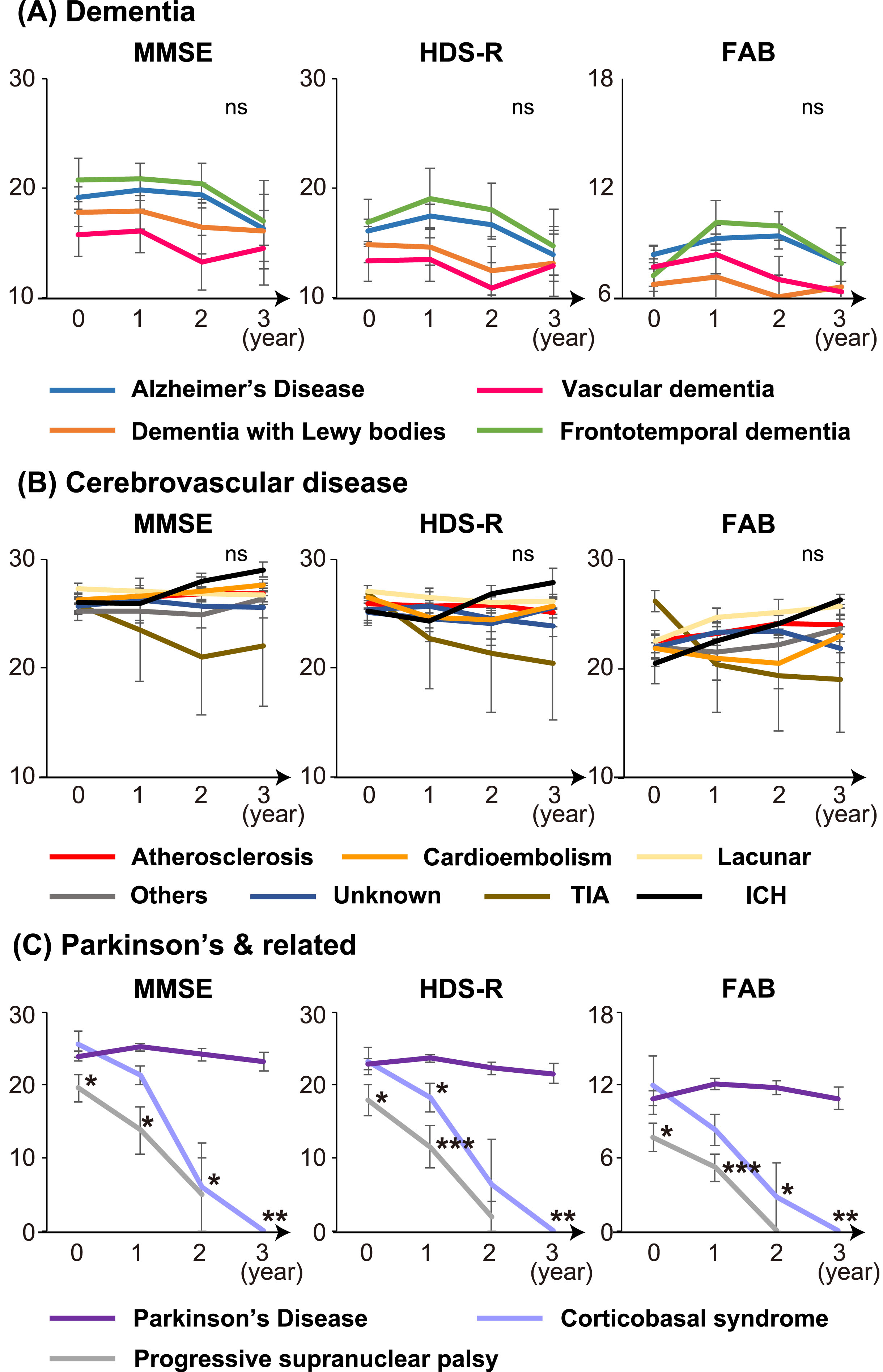
Cognitive function separated based on the subgroup of each group. (A) Dementia, (B) CVD, and (C) Parkinson’s and related. ICH, intracranial hemorrhage; TIA, transient ischemic attack.
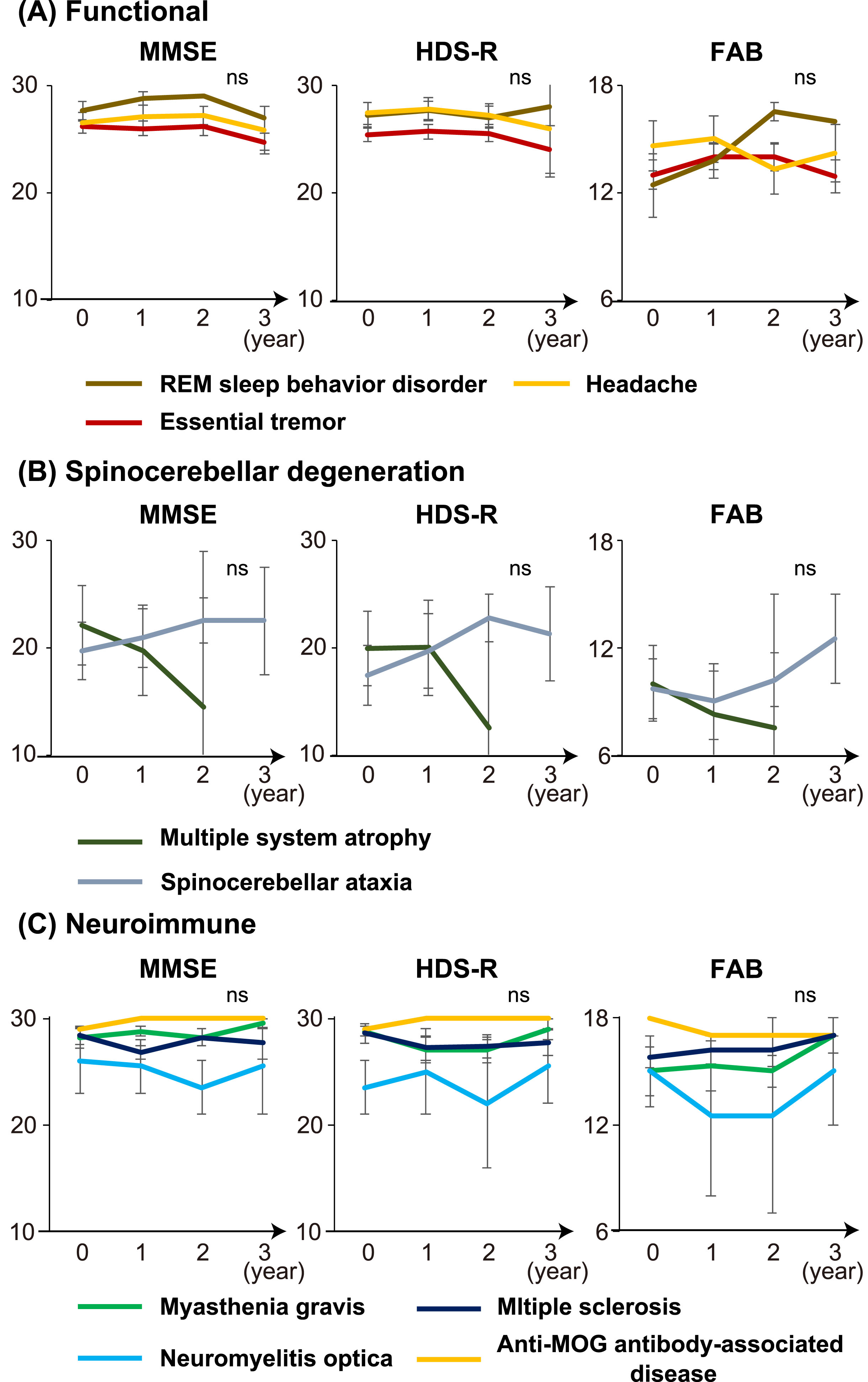
Cognitive function separated based on the subgroup of each group. (A) Functional, (B) Spinocerebellar degeneration, and (C) Neuroimmune.
DISCUSSION
Our study shows that: 1) both mortality and cognitive function differed among the nine neurological disease categories; 2) mortality of the Dementia (25.5%), Parkinson’s and related (21.6%), and SCD (35.3%) groups was highest among all nine groups; 3) all scores of MMSE, HDS-R, and FAB of the Dementia group, part of HDS-R and all scores of FAB of the Parkinson’s and related group, and part of HDS-R of the SCD group were significantly lower than the scores of the hypertension group; 4) unlike other groups, the cognitive functions among Parkinson’s and related subgroups, namely Parkinson’s disease, CBS, and PSP, were significantly different while those of CBS and PSP were significantly lower than those of the PD group.
The results of mortality showed a similar tendency to those of cognitive function. The mortality values of the Dementia, Parkinson’s and related, and SCD groups exceeded 20% within 3 years from enrollment, and were the three worst groups. Prior to this study, we expected that mortality of the CVD group would be among the worst groups because stroke can recur more in this group [12], with previous reports showing that more than 25% of cardioembolic ischemic survivors died within a few years [7, 14]. Contrary to our expectation, mortality of the CVD group in the Tochigi Neurological Disease Cohort Study remained at 7.5%, and was ranked fifth among the nine groups, suggesting that the holistic CVD prognosis was not very high. Our study shows that the prognoses of the Dementia, Parkinson’s and related, and SCD groups were worse than the prognosis of the CVD group. The result of the Neuroimmune group was also encouraging, and the common factor between the CVD and Neuroimmune groups was an innovative treatment of those two groups. The use of four kinds of direct oral anticoagulants to treat non-valvar atrial fibrillation [14, 15], several kinds of anti-platelet drugs and combination therapy [16, 17], maintenance of a stroke care unit and a primary stroke center [18, 19], as well as other treatment options, became popular over this past decade in the field of CVD, allowing the development of glucocorticoids and several molecular immunological target therapies for neuroimmune diseases [20–23]. Unlike the CVD and Neuroimmune groups, treatments for Dementia, Parkinson’s and related, and SCD groups have been limited thus far. The development of treatment options for the Dementia, Parkinson’s and related, and SCD groups will be a future focus over the coming years and decades in the neurological sciences as a way to prolong prognosis. In addition, the Dementia, Parkinson’s and related, and SCD groups have a common characteristic of continuous progression disease, both clinically and pathologically. A pathology in these groups involves the abnormal propagation of protein, known as prion-like propagation [24–26]. Our study’s results suggest that prion-like propagation worsened these patients’ prognoses. We emphasize that the establishment of a treatment that not only reveals the cause but also treats the prion-like propagation pathology, would be an effective strategy for improving the prognoses of the Dementia, Parkinson’s and related, and SCD groups.
Based exclusively on cognitive function, significant impairment in the Dementia, Parkinson’s and related, and SCD groups was observed. The low cognitive function of the Dementia group is likely because of the definition and characteristics of this disease [27]. On the other hand, our study revealed that the memory of patients in the Parkinson’s and related and SCD groups, as well as the frontal lobe function of patients in the Parkinson’s and related group, were impaired. Analysis of our study’s subgroups reveals worsening of the cognitive functions of CBS, PSP, and SCD patients. We suspect that no fundamental treatment or treatment that would delay disease progression would influence the results of cognitive function and mortality. We emphasize that cognitive decline in neurological diseases corresponds to high mortality, suggesting that the preservation of neurocognitive function is an important factor for prognosis.
There are several limitations of our study. First, there were only three study institutions, and these lacked multi-facilities. As a result, patient number was not very large. In contrast, in order to gain a holistic view of neurology, we classified the patients into nine groups. Since the limited number of patients were separated into nine groups, further reducing sample size in each, statistical power was somewhat weak in our study. Second, since enrollment was performed in only Japanese institutions, the results might differ from other cultural groups. Third, although real-life clinic data are precious, there may be several confounding factors that may have affected our findings, and removing them is a likely difficult task. Fourth, all the patients in this study were visiting patients while hospitalized patients did not participate in enrollment. Therefore, severe patients who were incapacitated following cardioembolinic ischemic stroke were not included at enrollment, and this may have biased some disease results.
In conclusion, both the mortality and cognitive function of patients in the Dementia, Parkinson’s and related, and SCD groups were significantly worse among the nine neurological diseases. In the forthcoming decade, focus should be placed on the development of treatments for neurologically-related neurodegenerative diseases.
AUTHOR CONTRIBUTIONS
Kosuke Matsuzono (Conceptualization; Formal analysis; Writing – original draft); Takafumi Mashiko (Data curation); Reiji Koide (Data curation); Hiroaki Yoshizumi (Project administration; Writing – review & editing); Shigeru Fujimoto (Supervision; Writing – review & editing).
Footnotes
ACKNOWLEDGMENTS
We would like to extend our appreciation to the participants who cooperated for the study and the medical staff involved in the study.
FUNDING
The authors have no funding to report.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
All data according to this study are available from the corresponding authors on request.