
Abstract
Background:
The contrast between memory versus executive function impairments is commonly used to differentiate between neurocognitive disorders (NCDs) due to Alzheimer’s disease (AD) and vascular cognitive impairment (VCI). We reconsidered this question because of the current use of AD biomarkers and the recent revision of the criteria for AD, VCI, and dysexecutive syndrome.
Objective:
To establish and compare the neuropsychological profiles in AD (i.e., with positive CSF biomarkers) and in VCI.
Methods:
We included 62 patients with mild or major NCDs due to pure AD (with positive CSF biomarker assays), and 174 patients (from the GRECogVASC cohort) with pure VCI. The neuropsychological profiles were compared after stratification for disease severity (mild or major NCD). We defined a memory-executive function index (the mean z score for the third free recall and the delayed free recall in the Free and Cued Selective Reminding Test minus the mean z score for category fluency and the completion time in the Trail Making Test part B) and determined its diagnostic accuracy.
Conclusion:
Although the contrast between memory and executive function impairments was supported at the group level it does not reliably discriminate between AD and VCI at the individual level.
INTRODUCTION
Alzheimer’s disease (AD) and vascular cognitive impairment (VCI) are the two most common causes of neurocognitive disorders (NCDs) [1]. The differential diagnosis is important because of the differences in prognosis and management between the two diseases [2, 3]. The neuropsychological pattern is a central feature of the recently published diagnostic criteria for AD [4] and for VCI [5]. Indeed, the profile of neuropsychological impairment is widely used to distinguish between AD and VCI in clinical practice.
Several studies have found that episodic memory impairments are more severe in patients with AD than in patients with VCI, whereas the latter have more severe impairments of executive function [6 –11]. However, other studies did not find a difference between the two neuropsychological profiles [12 –14]. These divergences may have been due to circularity bias; the diagnosis is based on clinical criteria, which in turn are based on a defined neuropsychological profile.
Only three studies examined neuropathological data [15 –17]. In an analysis of 25 patients with NCDs (AD: n = 19; VCI: n = 6), Reed et al. [15] concluded that memory impairment was prominent in AD (observed in 71% of cases) and executive function impairment was prominent in VCI (observed in 67% of cases). Although these findings are important, they are limited by the small number of patients and the choice of the neuropsychological methods used to assess executive functions (backward digit span, verbal fluency, and the initiation-perseveration subscore from the Dementia Rating Scale, which are not appropriate for detecting dysexecutive syndrome in AD and VCI [18 –20]. Yang et al.’s [16] assessment of 440 subjects from the Religious Order Study found that 1) the severity of memory impairment (according to the logical memory story A delayed recall, word list recall and word list recognition subscores from the Wechsler Memory Scale – Third Edition) was associated with AD, and 2) higher response slowing (according to the Number Comparison Test and the Symbol Digit Modalities Test) was associated with cerebral infarction. The main limitation of Yang et al.’s study is that it described inflexions in the cognitive profile as a function of disease severity, rather than defining the profile for each “pure” pathology. Ramirez-Gomez et al. [17] enrolled 69 patients with AD and 20 patients with subcortical VCI. The AD patients performed worse in a delayed recall test (the List Learning Subtest from the Memory Assessment Scale) but there were no differences between the two groups in executive tests (donor scales: the initiation–perseveration subscale of the Mattis Dementia Rating Scale, the F-A-S test, backward digit span, and backward visual memory span [21]). The main limitation of Ramirez-Gomez et al.’s work was the small number of patients with VCI. Lastly, a study comparing cognitive impairment in pure subcortical VCI (with negative Pittsburgh Compound B (PiB) positron emission tomography (PET)) versus AD (with positive PiB PET) [22] found that memory impairment was prominent in AD and that executive disorders were prominent in VCI. However, the latter study selected VCI patients with purely subcortical disease, and did not assess the extent of neurodegeneration in the AD group.
In view of recent data highlighting the elevated frequency of executive disorders in AD [19 , 24], and the ability to avoid circularity bias by measuring amyloid and neurodegeneration biomarkers in vivo, it has now become essential to recharacterize the patterns of cognitive impairment in AD versus VCI.
The main objective of the present study was thus to establish and compare the neuropsychological profiles for mild and major NCD due to “pure” AD (with positive CSF biomarkers) and for “pure” VCI (i.e., participants from GRECogVASC (Groupe de Réflexion pour l’Évaluation COGnitive Vasculaire) cohort [25]) by using a validated framework to interpret the results of a neuropsychological battery [26].
METHODS
Population
AD
All patients had been referred to Amiens University Hospital’s memory center between June 2006 and December 2016. The patients met the recent criteria for major or mild NCD due to pure AD (classic form), [4, 27], positive CSF AD biomarkers [28] (abnormal Aβ1-42 plus abnormal t-tau and/or p-tau levels), and MRI and neuropsychological datasets in the AMIENSCOG® registry [29]. All patients with comorbidities that could potentially affect cognition (Parkinson’s disease, Lewy body disease, epilepsy, normal pressure hydrocephalus, alcohol abuse, etc.) [30] were excluded, as were patients with possible vascular contributions to the NCD on the basis of clinical events (e.g., stroke) or imaging results (e.g., white matter abnormalities with a Fazekas score >2 or a cavity suggestive of prior infarct or hemorrhage when MRI datasets were systematically re-examined according to a validated method [31]). Of the 142 eligible patients, 62 were included (Table 1).
Study population
AD, Alzheimer’s disease; VCI, vascular cognitive impairment; NCD, neurocognitive disorder; MMSE, Mini-Mental State Examination.
VCI
The multicenter GRECogVASC study (NCT01339195) assessed cognitive status at 6 months post-stroke [25, 32]. GRECogVASC patients with mild or major NCD (according to VCI criteria [5]) monitored at the coordinating center at Amiens University Hospital were eligible (n = 174 from N = 204) All patients with NCD were invited to undergo a CSF biomarker analysis or to participate in the IDEA3 study (NCT02813434), which assessed brain amyloid deposition using florbetapir PET). Patients with a positive CSF AD-biomarker assay or a positive amyloid PET scan were excluded (n = 9). A total of 174 patients with VCI were included (Table 1). Ethics approval was obtained from the local institutional review board and a written informed consent was obtained from patients. MRI information is in the Table 2.
MRI information in VCI group
The patients with AD were older and were more likely to have major NCD than the patients with VCI. The two groups did not differ with regard to the educational level and the presence of depressive symptoms. Given that the two groups differed in the severity of NCD, all analyses were stratified for this parameter, i.e., mild and major NCD.
Neuropsychological assessment
Testing
Patients were assessed with a standardized neuropsychological battery [25, 33] for 1) general cognitive efficiency with the GRECO version of the Mini-Mental State Examination (MMSE) [34], 2) language with the Boston Naming Test [35] or the DO80 test [36]; 3) visuoconstructive abilities with Albert’s cancellation test [37] and the Rey-Osterrieth Complex Figure Test [38], 4) episodic memory with the French adaptation of the Free and Cued Selective Reminding Test [39] and the Doors and People Test [40], 5) executive function with the Digit Symbol Coding Test [41], the GREFEX versions [18] of verbal fluency (letter and category) tests [42], and the Trail Making Test (TMT) [43], and 6) behavioral executive disorders with the Behavioral Dysexecutive Syndrome Inventory (BDSI) [44]. Depressive symptoms were evaluated using the Montgomery-Åsberg Depression Rating Scale [45] or the Center for Epidemiological Study-Depression Scale [46]. Symptoms of anxiety were evaluated using the French version of the Goldberg Scale [47]. Behavioral Dysexecutive disorder, such as apathy, were retained only if behavioral changes were not accounted for by psychiatric condition such as depression [18]. Activities of daily living were assessed using the modified Instrumental Activities of Daily Living scale [48].
Cut-offs
Domain scores were computed using previously validated methods [26]. Data were collected from 1003 healthy controls (males: 35.9%; mean±SD age: 62±11.3; mean±SD full-time education: 11.4±3.2 years) [49]. Briefly, the transformed cognitive test scores (log transformation for the completion time in the TMT, and Box-Cox transformation for the other scores [50]) were entered into a series of linear regression analyses (one per score) with age, educational level, gender, and an interaction term (age×education level). Significant factors in controls were selected. The regression coefficients computed for controls were used to calculate standardized residuals, i.e., z scores (where poor performance corresponded to a negative z score). Scores for the BDSI were not influenced by demographic factors [18], and so were analyzed as z scores. The average of the 12 behavioral z scores was used as an overall behavioral summary score. The dichotomization of performance (normal versus impaired) was based on the 5th percentile cut-offs determined from the control group’s z scores. The 95% confidence interval (CI) for the frequency of impairment was computed using the equation p±zx√(p×(1–p)/n).
The memory-executive function index
The executive function score was the mean value of the z scores for category fluency and for the completion time in the TMT part B [51]. The memory score was the mean value of the z scores for the third free recall and the delayed free recall in the Free and Cued Selective Reminding Test, since these scores had been found to provide optimal discrimination between controls and both the AD and VCI groups (results not shown). To better evaluate the contrast between the memory and executive function impairments, a differential memory-executive function index (the memory score minus the executive function score) was computed.
Statistics
The AD and VCI groups’ respective neuropsychological profiles (z scores) were compared using an analysis of variance with each domain score (language, visuoconstructive abilities, memory, cognitive executive function, and behavioral executive function) as within-subject factors and the disease stage (mild or major NCD) and disease group (AD or VCI) as between-subject factors. Intergroup comparisons for depression, disease stage (mild or major), education level and gender were performed using Fisher’s test. Intergroup comparisons for age and the MMSE score were performed using a T-test.
To distinguish between patients with a prominent dysexecutive syndrome and those with a prominent amnesic syndrome, we determined the differential memory-executive function index: the lower the value of the index, the greater the memory impairment (relative to the executive disorder). A receiver operating characteristic (ROC) curve was plotted, and the area under the curve (AUC) [95% CI] was computed. Optimal cut-off points were determined using the maximum value of the Youden index (calculated as sensitivity-specificity-1). Unless otherwise indicated, the threshold for statistical significance was set to p≤0.05. Statistical analyses were performed using SAS software (version 4.3, SAS Institute Inc., Cary, NC).
RESULTS
Neuropsychological profiles
As expected, all domain cognitive scores were lower for patients with major NCD than for patients with mild NCD (p≤0.003). Comparisons stratified for the NCD stage showed that memory impairments (p = 0.001) and behavioral dysexecutive changes (p = 0.001) were more severe in AD, whereas language impairments were greater in VCI (p = 0.003). The two disease groups did not differ with regard to cognitive executive impairments (p = 0.11) or visuoconstructive impairments (p = 0.18) (Fig. 1).

Neuropsychological profiles (z scores) of VCI and AD patients with mild and major NCDs. AD, Alzheimer’s disease; VCI, vascular cognitive impairment; NCD, neurocognitive disorder. * p < 0.005.
The memory-executive function index
The two AD and VCI groups differed significantly with regard to the memory-executive function index (p < 0.001), due to the greater memory impairment in the AD patients (Fig. 2). The index was not influenced by the NCD stage (p = 0.2) (interaction group x stage: p = 0.9).
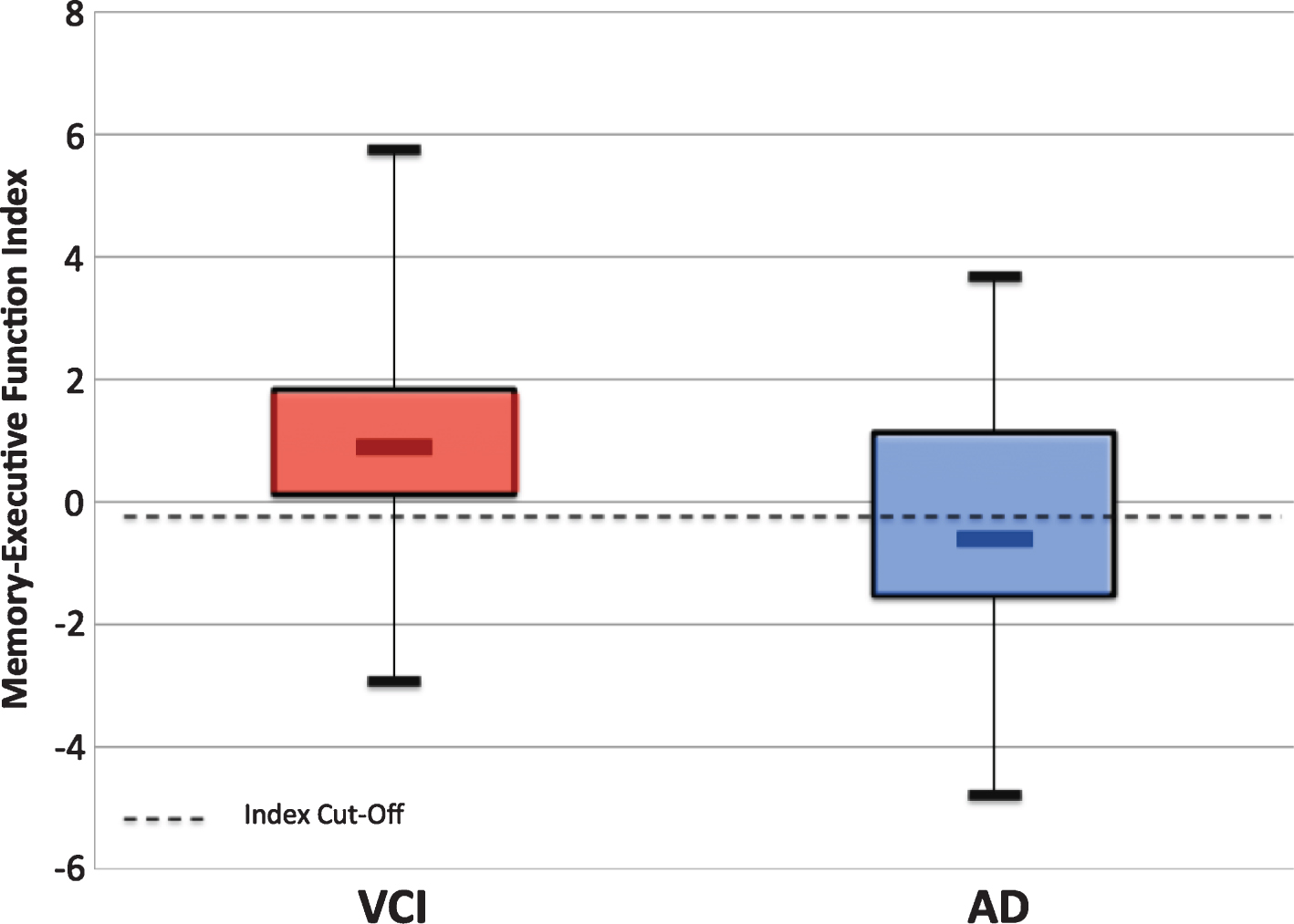
The memory-executive function index in the VCI and AD NCD groups. AD, Alzheimer’s disease; VCI, vascular cognitive impairment.
However, the two group’s individual indices overlapped considerably (Fig. 2). Accordingly, the AUC [95% CI] for the ROC curve was 0.714 [0.608–0.821]. Using the Youden index, the cut-off value was –0.376 (i.e., a memory impairment 0.376 SDs greater than the executive impairment). Application of this cut-off value detected AD with moderate sensitivity (63%) and good specificity (87%).
DISCUSSION
This study compared cognitive profiles for pure VCI versus pure AD in a large cohort of NCD patients. The etiology of AD was confirmed by CSF biomarker assays, and validated neuropsychological methods were used to evaluate and interpret cognitive data. Memory and behavioral executive impairments were prominent in the AD but the VCI and AD had similar levels of cognitive executive impairments. Furthermore, we demonstrated that a memory-executive function index (a contrast between memory impairment and executive function impairment) discriminated poorly between VCI and AD NCDs.
The prominence of language impairment in VCI has not been previously reported, and is probably due to the inclusion of amnestic forms of AD at a relatively early stage in the disease (at which naming abilities are relatively unaffected [2]. Impairment of instrumental abilities may complicate the interpretation of executive performance [18]. This was not the case in the present study where cognitive executive impairment was more severe in the group with language impairment, i.e., AD patients.
In contrast to several literature reports, our results do not indicate that cognitive executive disorders are more prominent in pure VCI than in pure AD [7–10 , 22]. This difference is probably due to the methods used to assess executive disorders. We used the current diagnostic criteria for dysexecutive syndrome [18], which are based on validated neuropsychological tests and cut-offs [26]; this is not the case for the studies of autopsy-defined cohorts by Reed et al. [15] and Ramirez-Gomez et al. [17]. Furthermore, the tests used in the present study (categorical fluency and completion time in the TMT part B) are the most sensitive for detecting executive disorders in AD [51] – again in contrast to the studies by Reed et al., Yoon et al., and Ramirez-Gomez et al. [15 , 22]. Our present results are in line with the high reported frequency of dysexecutive syndrome in AD [23]. Several studies have shown that white matter presence was associated with executive dysfunction [52, 53], in this work we excluded patients with significant white matter hyperintesities, actually two previuos studies proved that executive dysfunction could be independently associated with medio-temporal atrophy [54, 55] which is related to AD neuropathology [2].
We found that the severity of cognitive executive disorders was similar in the AD and VCI groups but that behavioral executive disorders were more severe in the AD group; to the best of our knowledge, the present study is the first to have made this observation. The severity of behavioral executive disorders was not due to advanced disease in the AD group, since the latter’s mean MMSE score was 21.9. Furthermore, we stratified our statistical analysis for the NCD stage (major or mild). This is likely to be accounted by the present assessment optimizing diagnosis of behavioral dysexecutive syndrome in AD, (especially for hypoactivity with apathy) that was previously found to detect behavioral dysexecutive syndrome in 86% of AD patients [23]. Our finding is in good agreement with the observation of behavioral dysexecutive syndrome in very early AD [56], where apathy is the most frequent behavioral disorder [57, 58]. The validity of our neuropsychological profile for the VCI group is supported by a frequency of executive disorders similar to that previously reported (Barbay et al., unpublished results).
In the present study, memory impairment was more prominent in the AD group that in the VCI group. This observation agrees closely with studies based on 1) clinical criteria [6 , 11], 2) clinical criteria with PiB confirmation [22], and 3) autopsy results [15 –17]. We selected patients with “pure” AD, i.e., the classical form characterized by medial temporal lobe atrophy. The latter is characterized by predominant memory impairments [2]3/4a feature pattern attributed to the development of neurofibrillary tangles in the medial temporal lobe [59]. In stroke patients, impairment of episodic memory is related to lesions in the medial temporal, thalamic, frontopolar and (to a lesser extent) deep hemispheric regions [60]. A low prevalence of memory impairment in VCI is probably due to the relative sparing of mesial structures [32], although this feature warrants specific investigation.
Our study also showed that the contrast between memory and executive function impairment is no longer relevant for discriminating between AD and VCI. Its predictive ability at the individual level was found to be moderate (sensitivity: 63%; specificity: 87%). Our results were similar to those reported by Ramirez-Gomez et al. [17], i.e., a sensitivity of 85% and a specificity of 67% using category fluency versus letter fluency (in the F-A-S test) and the first recall from the word learning test (which might be similar to our memory-executive function index). The index was useful in a small subgroup of patients with severe memory impairments.
In fact, our results go beyond the differential diagnosis of AD versus VCI and even challenge the currently accepted cognitive profile in AD. The neuropsychological profile of “typical” AD has been characterized by impairments in memory, visuoconstructive abilities, and language [2, 61]. Our present results emphasized the high frequency of cognitive and behavioral dysexecutive syndromes in “typical” AD, confirming previous results [19 , 24, 62]. Consequently, impairments in both cognitive and behavioral executive functions are conventional features of AD; this complicates the differential diagnosis with regard to other neurodegenerative diseases, such as behavioral variant frontotemporal degeneration (bvFTD). In fact, the neuropsychological profile in bvFTD is characterized by a behavioral dysexecutive syndrome and relatively unaffected memory and visuoconstructive abilities [63]. When compared with AD, patients with bvFTD have a predominant behavioral dysexecutive syndrome than is more than simply hypoactivity with apathy [64, 65]. The behavioral executive disorders in AD and bvFTD will need to be characterized in detail. As well, these results have shown the need to redefine the cognitive profile of mixed NCD (AD and vascular).
The main limitations of the present study were the retrospective inclusion of AD patients and the lack of systematic neuropathological verification. However, all AD patients were assessed using the same standardized work-up [33]. Although neuropathological verification constitutes the gold standard, it has the disadvantage to exclude a significant proportion of patients and it is not relevant for studies of MCI. Conversely patients more frequently agree to the CSF assay. Furthermore, we used a criterion for positive CSF markers of AD (i.e., abnormal Aβ1-42 levels plus abnormal t-tau and/or p-tau levels) which has a diagnostic accuracy of 95% [66]. Moreover, the best way of avoiding bias is to adopt a classification method based on an external criterion (i.e., one that does not include a cognitive profile), which was conveniently provided here by the CSF assay. Another study limitation related to the lack of systematic biomarker screening in patients with VCI. However, we excluded all VCI patients with 1) cognitive worsening that could not be explained by new vascular lesions, 2) CSF biomarkers for AD, or 3) positive PiB PET results. It should be noted that any inclusion of undiagnosed mixed dementia in the VCI group would have resulted in greater executive and memory impairments.
In conclusion, our present results confirmed the prominence of memory impairment in AD NCDs but did not evidence a prominent dysexecutive syndrome in VCI. In clinical practice, although the contrast between memory and executive function impairments was supported at the group level it does not reliably discriminate between AD and VCI at the individual level.
DISCLOSURE STATEMENT
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/17-1097r1).