
Abstract
Background:
Amyloid-β (Aβ) commonly coexists and impacts prognosis in subcortical vascular cognitive impairment (SVCI).
Objective:
This study aimed to examine the differences in clinical and neuroimaging variables between Aβ-positive and Aβ-negative SVCI and to propose a prediction model for Aβ positivity in clinically diagnosed SVCI patients.
Methods:
A total of 130 patients with SVCI were included in model development, and a separate cohort of 70 SVCI patients was used in external validation. The variables for the prediction model were selected by comparing the characteristics of the Aβ-negative and Aβ-positive SVCI groups. The final model was determined using a stepwise method. The model performance was evaluated using the receiver operating characteristic (ROC) curve and a calibration curve. A nomogram was used for visualization.
Results:
Among 130 SVCI patients, 70 (53.8%) were Aβ-positive. The Aβ-positive SVCI group was characterized by older age, tendency to be in the dementia stage, a higher prevalence of APOE ɛ4, a lower prevalence of lacune, and more severe medial temporal atrophy (MTA). The final prediction model, which excluded MTA grade following the stepwise method for variable selection, demonstrated good accuracy in distinguishing between Aβ-positive and Aβ-negative SVCI, with an area under the curve (AUC) of 0.80. The external validation demonstrated an AUC of 0.71.
Conclusions:
The findings suggest that older age, dementia stage, APOE ɛ4 carrier, and absence of lacunes may be predictive of Aβ positivity in clinically diagnosed SVCI patients.
Keywords
INTRODUCTION
Subcortical vascular cognitive impairment (SVCI) is one of the most common causes of cognitive impairment in elderly individuals. Although SVCI is characterized by extensive cerebral small vessel disease (CSVD), such as white matter hyperintensities (WMHs) [1], it commonly coexists with Alzheimer’s disease (AD) [2–5]. In fact, our group previously demonstrated that 30–50% of patients with SVCI had substantial amyloid-β (Aβ) burden on Aβ positron emission tomography (PET) [6–8]. More importantly, Aβ is the major contributing factor to cognitive decline and functional disability in patients with SVCI [9, 10]. In this regard, differentiating patients with Aβ-positive SVCI and amyloid-negative SVCI might have important clinical implications; clinicians could predict patient prognosis and make more informed decisions regarding treatment options according to the presence of Aβ, particularly in the era of Aβ-targeted treatment.
Although Aβ PET can detect Aβ deposition with high accuracy, the limited clinical use of Aβ PET due to its high cost has underscored the need to identify potential patients with Aβ positivity in SVCI. In fact, a previous study proposed criteria for distinguishing Aβ negativity on Pittsburgh compound B (PiB) PET (which captures Aβ deposition in the brain) among subcortical vascular dementia (SVaD) based on clinical and magnetic resonance imaging (MRI) variables [11]. This study suggested that a combination of older age, a lower number of lacunes, and increased medial temporal atrophy (MTA) could help differentiate PiB-positive SVaD from PiB-negative SVaD. This finding provided a potential avenue for predicting mixed or pure SVaD without expensive Aβ PET scans in clinical settings. However, there are still some gaps that need to be addressed. For instance, fluorine-based Aβ-PET ligands are now predominantly used. Furthermore, a previous study has focused on SVaD, but in clinical practice, predicting Aβ status at earlier stages of subcortical vascular mild cognitive impairment (svMCI) is also important. This clinical stage could provide additional predictive value for Aβ positivity. Therefore, an update of the prediction model is warranted.
Thus, the main purpose of the current study was to investigate the differences of Aβ positive and negative SVCI patients by addressing gaps in the literature and to propose the prediction model for Aβ positivity in clinically diagnosed SVCI patients using clinical and MRI variables. We hypothesized that a combination of various features could make it possible to predict Aβ positivity in SVCI. To achieve this goal, we utilized a nomogram that could be easily applied in a clinical setting.
MATERIALS AND METHODS
Ethics approval and consent to participate
The study procedures were approved by the Institutional Review Board of Samsung Medical Center (No. 2017-05-062, 2020-01-024-022), and informed consent was obtained from all participants undergoing amyloid PET scans. All procedures were conducted in accordance with approved guidelines.
Participants
We retrospectively enrolled 131 patients with clinically diagnosed SVCI (85 with SVaD and 46 with svMCI) who underwent Aβ PET at the Samsung Medical Center memory clinic in Seoul, Korea between August 2015 and November 2018. For external validation, we additionally included 70 patients (27 with SVaD and 43 with svMCI) who underwent Aβ PET between January 2019 and January 2023. In this memory clinic, patients with severe WMH were recommended to undergo Aβ PET scans for clinical or research purposes, regardless of cognitive status. It contributed to establishing a well-characterized cohort of SVCI and allowed extensive research on SVCI. The following criteria were used for the diagnosis of SVCI: 1) subjective cognitive complaints by the patient or caregiver; 2) objective cognitive impairment below –1 standard deviation (SD) from the age-, sex-, and education-adjusted norms in any cognitive domain, including language, visuospatial, memory, or frontal function on neuropsychological tests [12, 13]; and 3) severe ischemia on brain MRI, defined as the width of periventricular WMH from the lateral ventricular wall≥10 mm and the longest diameter of deep WMH≥25 mm, as modified from the Fazekas ischemia criteria [8]. The distinction between svMCI and SVaD was based on the activities of daily living.
All participants underwent clinical interviews and neurological examinations, and a clinical diagnosis was established by consensus among a multidisciplinary team. Blood tests included complete blood count, blood chemistry, vitamin B12/folate level measurement, syphilis serologic test, thyroid function test, and APOE genotyping. The APOE ɛ4 carrier was defined as carrying at least one copy of the APOE ɛ4 allele, and the APOE ɛ2 carrier was defined likewise. Patients were excluded when they had territorial cortical infarctions, brain tumors, or vascular malformations on MRI. Patients with WMH due to radiation injury, multiple sclerosis, vasculitis, or leukodystrophy were also excluded.
Aβ PET and definition of Aβ positivity
18F-florbetaben PET (n = 161) and 18F-flutemetamol PET (n = 40) were performed using a Discovery STe PET/CT scanner (GE Medical Systems, Milwaukee, WI, USA). A 20-min emission PET scan in dynamic mode (consisting of 4×5-min frames) was performed 90 min after injection of a mean dose of 311.5 MBq 18F-florbetaben and 197.7 MBq 18F-flutemetamol, respectively. Three-dimensional PET images were reconstructed in a 128×128×48 matrix with a 2×2×3.27-mm voxel size using the ordered-subset expectation maximization algorithm (18F-florbetaben, iteration = 4 and subset = 20; 18F-flutemetamol, iteration = 4 and subset = 20). To quantify Aβ burden on FBB and FMM PET, we replicated the image processing steps described in the previously published Centiloid Project [14]. We defined Aβ positivity using a Centiloid cutoff value of 20.0 [15].
Brain MRI acquisition and analyses
We acquired standardized three-dimensional T2-weighted T1 turbo field echo images, three-dimensional FLAIR images, and T2*-weighted gradient echo (GRE) images at Samsung Medical Center using a 3.0T MRI scanner (Philips 3.0T Achieva; Philips Healthcare, Andover, MA, USA), as previously described. The mean time interval between Aβ PET and brain MRI was 0.23±0.43 years. The images were processed using the CIVET anatomical pipeline (version 2.1.0) [16]. Native MRI images were registered to the MNI-152 template by linear transformation [17] and corrected for intensity nonuniformity using the N3 algorithm [18]. The detailed methods for cortical thickness and hippocampal volume measurements are described in a previous study [19].
Assessment of WMH, lacunes, and microbleeds
Clinical Research Center for Dementia of South Korea WMH visual rating scale was used to investigate WMH in the deep subcortical and periventricular region in FLAIR images as reported in the literature [20]. Briefly, deep WMH was classified as D1 (<10 mm), D2 (10 mm–25 mm), or D3 (≥25 mm) based on the longest diameter of the lesions. Periventricular WMH were classified as P1 (cap and band < 5 mm), P2 (5 mm–10 mm), or P3 (cap or band≥10 mm) based on the maximum length measured perpendicular (cap) and horizontal (band) to the ventricle. The combination of these D and P ratings yielded nine cells, and the overall WMH severity (minimal, moderate, and severe) was defined based on the following combination of D and P ratings: minimal (D1P1, D1P2), moderate (D1P3, D2P1, D2P2, D2P3, D3P1, D3P2), and severe (D3P3). To test the inter-rater reliability of our WMH visual rating, two experienced neurologists performed a visual rating of the WMH severity. Inter-rater agreement was excellent for the overall WMH severity (Fleiss k = 0.86). Lacunes and cerebral microbleeds (CMBs) were identified and counted in accordance with STandards for ReportIng Vascular changes on nEuroimaging (STRIVE) [21]. Lobar CMBs were defined as homogenous and round lesions with signal loss (≤10 mm in diameter) on T2*-weighted GRE images, with a lobar location (cortex, gray-white matter junction, and subcortical white matter) [22]. Deep CMBs were defined as CMBs in the basal ganglia, internal/external capsules, and thalamus [22]. CMBs in the brainstem were also classified as deep CMBs [23]. Two experienced neurologists (H.J. and H.K.) rated the lacunes and microbleeds for the training set, and three experienced neurologists (J.Y., E.H.L., and D.S.) blinded to this study rated all imaging markers for the validation dataset. The kappa measures for inter-rater agreement were 0.87, 0.86, and 0.56 (all p < 0.001) for lobar CMBs, deep CMBs, and lacunes, respectively, and the discordant cases were discussed and reconciled through consensus.
Visual rating of MTA on MRI
The degree of MTA was rated from 0 (no atrophy) to 4 (severe atrophy) for each side, and the more severe degree of MTA was selected if the degree of MTA was asymmetric. The inter-rater reliability for MTA was 0.67 (p < 0.001), and a consensus was reached in any case of discrepancy.
Neuropsychological tests
All patients underwent standardized neuropsychological tests at baseline using the Seoul Neuropsychological Screening Battery 2nd edition [24], which contains tests for attention, language, visuospatial function, verbal memory, visual memory, and frontal-executive function; the Korean Mini-Mental State Examination (K-MMSE) [25]; and the Clinical Dementia Rating-Sum of Boxes (CDR-SB) [26].
Statistical analyses
The demographic and neuropsychological characteristics of the participants were compared between the Aβ-negative and Aβ-positive SVCI, using appropriate statistical methods, including the t-test, Mann–Whitney U test, chi-square test, and Fisher’s exact test. Based on descriptive statistics, the clinical and MRI variables, which indicated the difference between Aβ positivity at a significance level of p < 0.10, were selected for developing the prediction model using multiple logistic regression analysis. The final prediction model was determined by the both-direction stepwise method. To assess the performance of the final model, discrimination and calibration were evaluated using the receiver operating characteristic (ROC) curve and a calibration curve, respectively. To test the final model, the external validation was performed in a separate cohort of SVCI patients who underwent Aβ PET during a different period. Finally, a nomogram was employed as a visualization tool to help interpret the effect of variables on the probability of Aβ positivity. Lacunes, lobar CMBs, and deep CMBs were categorized based on their data characteristics of being positively skewed and the interpretability of the results. The statistical analyses were conducted using SPSS version 21.0 and R.
RESULTS
Demographic and neuropsychological characteristics of Aβ-positive and Aβ-negative SVCI
The demographic characteristics of the participants are presented in Table 1. As one participant was excluded due to an error in imaging analysis, a total of 130 SVCI patients were finally included in the training set. In the training set, the mean age and education level of the patients were 78.3 years (SD = 6.9) and 9.1 years (SD = 5.6), respectively. The number of females and dementia were 91 (70.0%) and 85 (65.4%), respectively. Among the 130 patients, 70 (53.8%) were categorized as Aβ-positive SVCI.
Comparison of the demographic, clinical, and MRI variables between the patients with Aβ-negative and Aβ-positive SVCI
T-test, Mann-Whitney test, Chi-square test, or Fisher’s exact test were conducted, as appropriate. Values are presented as means±standard deviations, medians (interquartile ranges), or numbers (%), as appropriate. Aβ, amyloid-β; SVCI, subcortical vascular cognitive impairment; MRI, magnetic resonance imaging; CMB, cerebral microbleed; MTA, medial temporal atrophy.
In the training set, individuals with Aβ-positive SVCI were older than those with Aβ-negative SVCI (80.3±5.6 versus 76.0±7.5 years, p < 0.001) and tended to have a higher percentage of being in the dementia stage compared to those with Aβ-negative SVCI (p = 0.053), although the two groups did not significantly differ in sex, years of education, and vascular risk factors. The proportion of APOE ɛ4 carriers was higher in individuals with Aβ-positive SVCI (p < 0.001), although the proportion of APOE ɛ2 was not different between the two groups. Regarding the MRI variables, the two groups differed in the number and presence of lacunes and MTA. Specifically, individuals with Aβ-positive SVCI tended to have fewer lacunes (p = 0.067), had a lower prevalence of lacune (p = 0.034), and exhibited higher MTA (p = 0.008), while there were no differences in lobar CMBs and deep CMBs between the two groups.
The neuropsychological characteristics of the participants are presented in Table 2. Although there were no significant differences in general cognition between the two groups (p = 0.108), the patients with Aβ-positive SVCI slightly differed in several cognitive tests compared to those with Aβ-negative SVCI. Specifically, individuals with Aβ-positive SVCI tended to show poorer performance in the memory domain, specifically visual recognition (–1.35±1.30 versus –0.91±1.30, p = 0.068), while individuals with Aβ-negative SVCI tended to perform worse in the frontal function domain, especially COWAT phonemic (–1.45±1.03 versus –1.07±1.07, p = 0.073). However, they did not significantly differ in attention and language domains.
Comparison of the neuropsychological characteristics between the patients with Aβ-negative and Aβ-positive SVCI
Aβ, amyloid-β; SVCI, subcortical vascular cognitive impairment; K-MMSE, Korean Mini-Mental State Examination; CDR, Clinical Dementia Rating; CDR-SB, Clinical Dementia Rating-Sum of Boxes; SVLT, Seoul Verbal Learning Test; RCFT, Rey–Osterrieth Complex Figure Test; COWAT, Controlled Oral Word Association Test.
Development of the model predicting Aβ positivity in patients with SVCI in the training set
The two groups tended to differ in age, being in the dementia stage (SVaD versus svMCI), the presence of APOE ɛ4, the absence of lacune, and MTA. Thus, these five variables were incorporated into the multiple logistic regression model. Based on the both-direction stepwise method, the final model consisted of age, being in the dementia stage, the presence of ɛ4, and the absence of lacune, and MTA was subsequently excluded. The result of this final model is presented in Table 3. Older age (OR = 1.12, 95% CI [1.05, 1.20]), being in the dementia stage (OR = 2.29, 95% CI [0.95, 5.50], the presence of ɛ4 (OR = 6.05, 95% CI [2.26, 16.19]), and the absence of lacune (OR = 0.36, 95% CI [0.15, 0.84] for the presence of lacune) were associated with an elevated probability of Aβ positivity in patients with SVCI.
Multiple logistic regression predicting Aβ positivity in SVCI in the training set (both-direction stepwise)
Aβ, amyloid-β; SVCI, subcortical vascular cognitive impairment.
The evaluation of the final prediction model
The ROC curve was used to evaluate the overall performance of the final prediction model in distinguishing Aβ-positive SVCI from Aβ-negative SVCI (Fig. 1A). The area under the curve (AUC) value for the ROC curve was 0.80 (95% CI [0.72,0.88]) in the training set, which indicated good discrimination of Aβ positivity in patients with SVCI. In addition, the final model demonstrated a sensitivity of 67.1, specificity of 81.7, positive predictive value (PPV) of 81.0, and negative predictive value (NPV) of 68.1 in the training set.
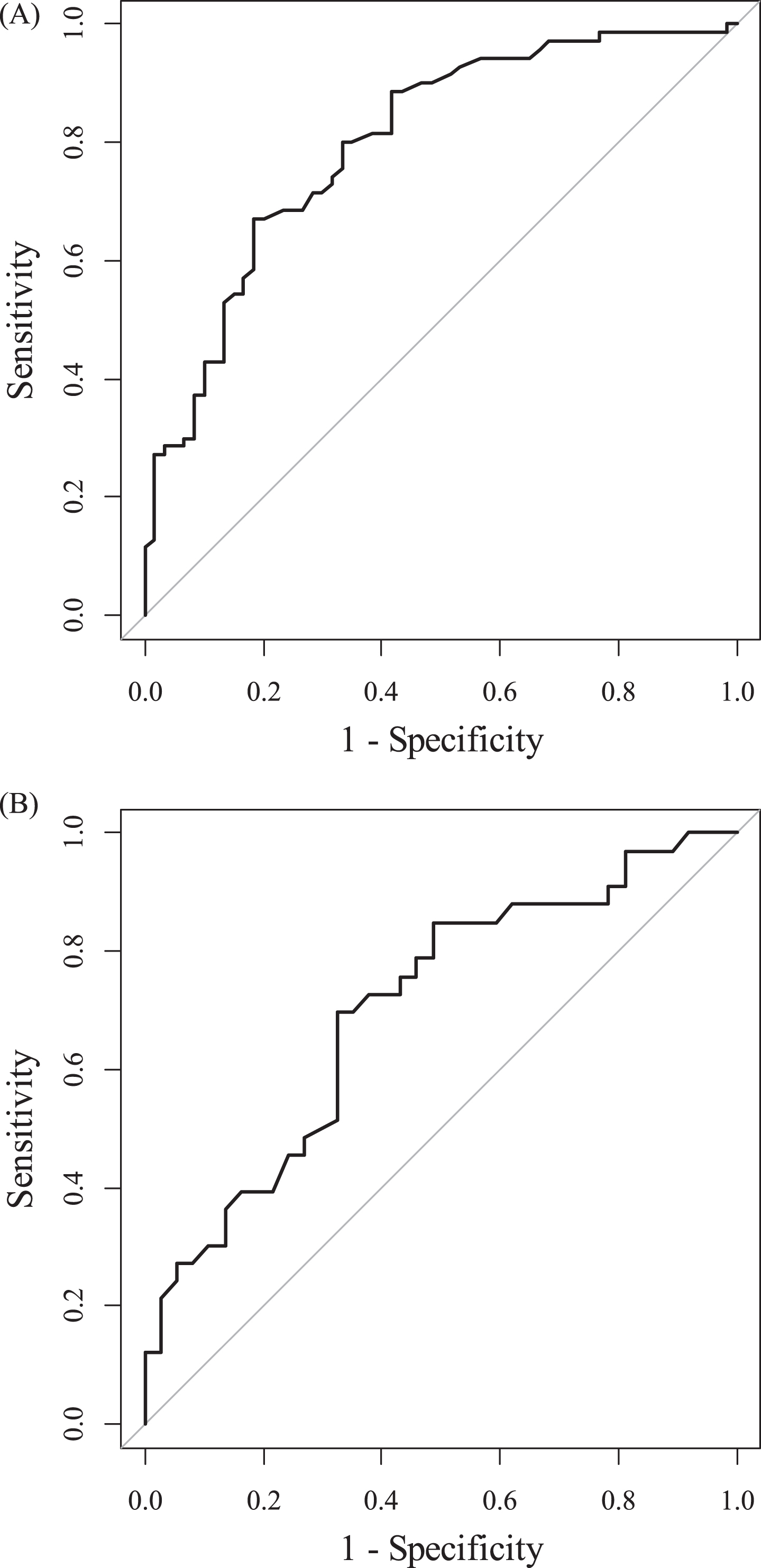
ROC curve for Aβ positivity prediction model in SVCI in the training set (A) and the validation set (B).
The calibration of the final model was evaluated with the calibration curve, specifically assessing the fit between the actual and predicted probability. The apparent and bias-corrected line was close to the 45-degree ideal line in the training set (Supplementary Figure 1A), indicating that the model was overall well calibrated (training set; mean absolute error of 2.3%, mean squared error of 0.071%).
Lastly, the nomogram was constructed using the final model (Fig. 2). Specific points at the top were matched to the values of each variable, based on the beta coefficient from the final model. The total points were calculated by adding the points assigned to each variable, and finally, the total points indicated the probability of Aβ positivity in patients with SVCI.

Nomogram predicting Aβ positivity in SVCI.
External validation of the final prediction model
The demographic, clinical, and neuropsychological characteristics between the training and validation sets are presented in Supplementary Tables 1 and 2. Participants in the validation set were younger (75.0±6.1 versus 78.3±6.9 years, p < 0.001), had a lower prevalence of dementia (38.6% veresus 65.4%, p < 0.001), and had a higher prevalence of hyperlipidemia (47.1% versus 26.2%, p = 0.003) compared to those in the training set. In addition, individuals in the validation set had a lower prevalence of both lacune and lobar CMB (38.6% /41.4% versus 58.5% /63.1%, p = 0.007/0.003, respectively). Lastly, the validation set showed better neuropsychological profiles, with better performance in all neuropsychological tests. There were no differences between the sets in other variables.
In the validation set (Fig. 1B), the AUC value for the ROC curve was 0.71 (95% CI [0.58,0.83]), indicating acceptable discrimination of Aβ positivity in patients with SVCI from the separate cohort. It demonstrated a sensitivity of 69.7%, specificity of 67.6%, PPV of 65.7%, and NPV of 71.4% in the validation set. Furthermore, the apparent and bias-corrected line was close to the 45-degree ideal line in the validation set (Supplementary Figure 1B), indicating that the model was overall well calibrated (validation set; mean absolute error of 2.5%, mean squared error of 0.102%).
DISCUSSION
The current study aimed to compare the clinical and neuroimaging variables between patients with Aβ-positive and Aβ-negative SVCIs and subsequently, to develop and externally validate a prediction model for identifying Aβ-positive SVCI. This result suggested that older age, being in the dementia stage (i.e., SVaD), APOE ɛ4 carrier, and absence of lacune could serve as predictive factors for considering confirmatory Aβ biomarker testing such as Aβ PET scans or cerebrospinal fluid testing in patients clinically diagnosed with SVCI. It might help clinicians predict Aβ-positive SVCI when patients present with cognitive impairment and severe WMH in clinical settings, which is important for planning future management and predicting prognosis.
The first major finding of this study was that patients with Aβ-positive SVCI were characterized by older age, a higher prevalence of APOE ɛ4 carrier, the absence of lacune, more severe MTA, and a tendency to be in the dementia stage, compared to those with Aβ-negative SVCI. In terms of age, clinically diagnosed SVCI patients (mean age 78.3) tend to be older compared to both AD spectrum patients and the average population visiting memory clinics (mean age 70) [8, 27]. This age difference may serve as a distinctive characteristic distinguishing SVCI from AD. It can be attributed to a more direct relationship between increasing age and severe WMH. However, our results emphasize that advanced age remains a risk factor for concurrent AD pathology in SVCI patients with pre-existing severe WMH. Other factors distinguishing Aβ positivity in SVCI also align with previous knowledge. APOE ɛ4 carrier has been identified as a prominent risk factor for Aβ deposition [28, 29]. Although MTA is not specific to AD, it is still one of the most sensitive markers of neurodegeneration, a hallmark feature of AD [30, 31]. In addition, as previous studies already demonstrated that Aβ positivity is one of the major factors affecting disease progression in SVCI, a more advanced disease stage may have a higher chance of having concomitant AD pathology. Therefore, the dementia stage itself could provide valuable insights to predict Aβ positivity in SVCI individuals. Previous studies have shown that a higher number of lacunes are associated with the disruption of white matter networks and poorer cognitive performance [32]. Therefore, given that lacunes, indicative of focal vascular injury, can impair cognitive function by themselves, we consider that SVCI patients with lacunes may experience cognitive decline without the additive effect of AD pathology. This suggests that lacunes could serve as a biomarker for pure SVCI, which aligns with previous research findings [11, 34].
On the other hand, the number or presence of lobar CMBs and the presence of the APOE ɛ2 genotype were not predictive of the need for diagnostic Aβ biomarker testing in patients with SVCI. In this study, we considered lobar and deep CMBs as separate variables, considering that their topographic locations might indicate different underlying etiologies, cerebral amyloid angiopathy (CAA) and hypertensive arteriopathy, respectively [35]. CAA is characterized by strictly lobar CMBs without deep CMBs and frequently co-occurs with AD, sharing pathogenic mechanisms of impaired Aβ clearance [36]. However, in this study, lobar CMBs did not show significant differences between Aβ-positive and Aβ-negative SVCI. This topographical locations of CMBs might not be critical for discriminating Aβ positivity in SVCI.
In this study, only APOE ɛ4, not APOE ɛ2, genotype was important for predicting the need for diagnostic Aβ biomarker testing, which is partially inconsistent with earlier studies. In fact, compared with APOE ɛ3 homozygotes, APOE ɛ4 is known as a risk factor, while APOE ɛ2 is a protective factor for Aβ deposition in patients with AD [28], which is explained by differential Aβ clearance via low-density lipoprotein receptor-related proteins on the blood–brain barrier. However, a previous study from our group demonstrated that APOE ɛ2 is distinctly associated with Aβ deposition in patients with SVCI [37], suggesting a possible relation between APOE ɛ2 and the coexistence of CAA, or the possible change in the function of APOE ɛ2 protein in severe CSVD. Thus, the role of APOE ɛ2 in the risk for AD in the presence of CSVD and its underlying mechanism needs to be elucidated with further studies.
We found that age, the disease stage, APOE ɛ4 carrier, and the absence of lacune were included in the final model for predicting Aβ positivity in SVCI, with the exclusion of MTA grade. The finding that MTA became nonsignificant in final multiple models was inconsistent with a previous study [11], which developed the Seoul criteria for pure SVaD. One possible explanation is that aside from being explained by age and the disease stage, the predictive value of neurodegeneration for Aβ-positive SVCI might become less critical. We consider that MTA is a neuroimaging maker indicative of neurodegeneration, but not specific to AD [38], and severe vascular burden might also contribute to medial temporal neurodegeneration.
In this study, we included the external validation dataset collected during a different period from the training dataset. Although neuropsychological profiles did not differ between Aβ+versus Aβ- groups in the training dataset and were not included in the prediction model, in the validation set, Aβ-positive SVCI group performed worse in both immediate and delayed recall of verbal and visual stimuli compared to the Aβ-negative SVCI group. Given that the validation set included younger patients and a lower prevalence of dementia, cognitive impairment might be important in predicting Aβ positivity particularly when SVCI participants are young and in the aMCI stage, which warrants to be confirmed in the future study. Furthermore, we performed the external validation of the prediction model developed using the training dataset. As a result of the external validation, our prediction model showed reasonable discrimination and calibration, suggesting that this model could be applicable.
Several limitations should be noted for this study. First, there may be a bias in the selection of participants, since some patients may have received Aβ PET scans due to clinical suspicions of AD, or because of the study’s retrospective design. Conducting a future study with a prospective design for external validation could improve its generalizability. Second, pathological confirmation was not obtained. Therefore, clinically diagnosed SVCI might have other pathologies, such as argyrophilic grain disease or hippocampal sclerosis, which could be the contributing etiologies of cognitive impairment. Third, our study was conducted on Koreans with clinically diagnosed SVCI, and thus may not be generalizable to other populations or other ethnicities. Fourth, we employed a stepwise method to select variables for our final model. Since this stepwise method is used to identify a model with a lower AIC (i.e., better fit), it might include a variable with a higher borderline p value, namely the dementia stage in our model. Thus, we need to take caution in integrating borderline variables with significant ones, despite the external validation of our final model. Fifth, while we aimed to develop a simple and practical clinical prediction model using only neuroimaging and clinical biomarkers, the rapid advancement and validation of plasma biomarkers have simplified the prediction of Aβ positivity. However, considering that the clinical utility of plasma biomarkers in SVCI cohorts has not been as extensively validated as in Alzheimer’s clinical syndrome, our study may retain its significance by assisting clinicians in predicting Aβ positivity in clinical settings until plasma biomarkers are adequately validated for use in SVCI cohorts.
In conclusion, this study contributes to the literature by addressing the gap in discriminating SVCI with AD pathology and pure SVCI. Specifically, our study included individuals with a whole spectrum of cognitively impaired (MCI and dementia). Currently, as the elderly increasingly visit memory clinics in the early stages of cognitive decline and at younger ages, the diagnosis of concomitant Aβ in their preclinical or prodromal stages would be beneficial to plan further treatment and determine prognosis. Specifically, this study proposed an updated prediction model with utilizing the 18F-ligand PET, as PiB-PET scans are no longer routinely conducted in clinical practice. The findings suggest that patients clinically diagnosed with SVCI, who are older, in the dementia stage, APOE ɛ4 carrier, but do not have lacune, are more likely to have comorbid AD pathology. Thus, our prediction model may warrant confirmatory Aβ biomarker testing for these individuals and guide clinicians on future treatment. Particularly, we consider that our prediction model is not only simple and easy to implement in a clinical setting, but also distinctively advantageous in its comprehensive integration of various predictors, as opposed to evaluating them individually.
AUTHOR CONTRIBUTIONS
Hasom Moon (Conceptualization; Formal analysis; Methodology; Writing – original draft; Writing – review & editing); Hongki Ham (Conceptualization; Data curation; Writing – Review & editing); Jihwan Yun (Conceptualization; Data curation; Writing – review & editing); Daeun Shin (Conceptualization; Data curation; Writing – review & editing); Eun Hye Lee (Conceptualization; Data curation; Writing – review & editing); Hee Jin Kim (Conceptualization; Resources; Writing – review & editing); Sang Won Seo (Conceptualization; Resources; Writing – review & editing); Duk L. Na (Conceptualization; Resources; Writing – review & editing); Hyemin Jang (Conceptualization; Funding acquisition; Methodology; Supervision; Writing – review & editing).
Footnotes
ACKNOWLEDGMENTS
The authors have no acknowledgments to report.
FUNDING
This research was supported by the National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT) (NRF-2020R1A2C1009778) and the Korea Health Technology R& D Project through the Korea Health Industry Development Institute (KHIDI) and Korea Dementia Research Center (KDRC), funded by the Ministry of Health & Welfare and Ministry of Science and ICT, Republic of Korea (HU20C0414).
CONFLICT OF INTEREST
SWS is an Editorial Board Member of this journal but was not involved in the peer-review process of this article nor had access to any information regarding its peer-review.
DATA AVAILABILITY
The anonymized data presented in this study are available upon request from the corresponding author.