
Abstract
Potential participant registries are tools to address the challenge of slow recruitment to clinical research. In particular, registries may aid recruitment to secondary prevention clinical trials for Alzheimer’s disease (AD), which enroll cognitively normal older individuals meeting specific genetic or biomarker criteria. Evidence of registry effectiveness is sparse, as is guidance on optimal designs or methods of conduct. We report our experiences of developing a novel local potential participant registry that implemented online enrollment and data collection. In the first year of operation, 957 individuals submitted email addresses to the registry, of whom 592 self-reported demographic, family history, and medical data. In addition, registrants provided information related to their interest and willingness to be contacted about studies. Local earned media and community education were the most effective methods of recruitment into the registry. Seventy-six (26%) of 298 registrants contacted about studies in the first year enrolled in those studies. One hundred twenty-nine registrants were invited to enroll in a preclinical AD trial, of whom 25 (18%) screened and 6 were randomized. These results indicate that registries can aid recruitment and provide needed guidance for investigators initiating new local registries.
INTRODUCTION
The global imperative to develop improved therapies for Alzheimer’s disease (AD) is hindered by delays in accrual to clinical trials [1, 2]. Few interventions to improve clinical trial recruitment are available and those that exist have limited evidence related to their effectiveness or cost efficiency [3]. Over the last decade, revelations into the long prodromal phase of AD biology, which substantially precedes clinical diagnosis, [4] have led to an evolution in AD trials [5]. Trials increasingly focus on pre-dementia populations, now including those meeting criteria for “preclinical” or “asymptomatic” AD [6, 7]. These clinical trials represent a new model in AD research, enrolling cognitively normal older persons deemed at increased risk for AD based on biomarker and genetic tests. Traditional recruitment through memory clinics will not adequately address the needs of these trials. Furthermore, unique barriers to enrollment are likely to be encountered in preclinical AD trials, [8–10] necessitating novel approaches to complete trial accrual [11].
Potential participant registries are tools to improve recruitment to clinical research, and are increasingly being utilized to facilitate preclinical AD trials [12, 13]. Registries are large collections of individuals who have expressed preliminary interest or granted permission to be contacted about clinical studies for which they may be eligible. Registries vary in their design and scope [12, 13]. Some registries are international or national, [12, 14] some are statewide, [15, 16] and some are local [3, 17]. Registries may include only names and contact information, reducing the logistical, infrastructural, and regulatory burden associated with their construction and initiation. Registries increasingly collect additional data, ranging from demographic and family history information to prospective cognitive testing performance, as a means to identify individuals most likely to be eligible for preclinical AD trials, that is, to demonstrate AD biomarkers [12].
A number of important questions related to the design and effectiveness of recruiting from registries remain unanswered [18]. These questions include what tactics work best to recruit registrants; do particular design elements enhance the effectiveness of registries; and will registrants be willing to participate in preclinical AD trials? We report the development and initial experiences with an online local potential participants registry, which we developed at the University of California, Irvine, Institute for Memory Impairments and Neurological Disorders (UCI MIND) and Institute for Clinical Translational Science (UCI ICTS), named the UCI Consent-to-Contact Registry (C2C).
METHODS
Design overview
The UCI C2C is a local online potential participant registry. The purpose of the C2C is to enhance the efficiency of recruitment to clinical research at UCI. Although the registry was designed with an emphasis on preclinical AD trials, it is a resource to any UCI investigator performing human subjects research with Institutional Review Board (IRB) approval. Permitting additional recruitment beyond preclinical AD trials 1) increases the overall value of the registry to the local research enterprise, 2) improves the risk-benefit ratio for the registry by increasing its scientific value, [19] and 3) increases the likelihood that an individual registrant will be contacted about a study, improving participant engagement [18].
To enroll, visitors to the registry website (https://c2c.uci.edu/) submit their email address. A personalized email then invites full enrollment through a Research Electronic Data Capture (REDCap) survey data collection instrument. After authentication preventing bot infiltration, enrollees sign informed consent electronically (Supplementary Material) and complete an enrollment survey.
Infrastructure and data security
The C2C uses REDCap [20] as a data infrastructure. The need for a single controlled instance of a dataset with shared access for researchers while allowing registrants to update their information necessitated an electronic, web-based data capture system. The application also needed to enable audits of user access, information sharing, exports, and ad-hoc queries. Standard applications such as Microsoft Excel or Google Spreadsheet do not satisfy online data security restrictions [21]. REDCap fits these restrictions, as well as the requirement for data safety, security, and sharing. When sharing data requests with researchers, either the raw data or labeled data can be exported. The REDCap data dictionary acts as the version control system for any significant changes to registry surveys and the application allows for data exports to the most commonly used statistical packages (e.g., SAS, SPSS, Stata, and R). The application is licensed for non-commercial research purposes; there is no required software to install for the registrant, other than a web browser from their Internet-enabled device [22].
Web site interface/development
Webpages describing the C2C were created using WordPress, an open source content management system. The WordPress system is hosted on a LAMP stack with a purchased theme for designing the registry’s front facing webpages. The website displays relevant study information and frequently asked questions for online browsing.
Links on the C2C website redirect users to the UCI MIND REDCap application. The initial data submission consists of capturing and then confirming the registrant’s email address. A unique secondary survey link, viewable only by the participant or a member of the research team, is sent directly to the registrant’s email address, bypassing the need for a web portal where registrants are required to set up an account or create passwords. Survey links are active until the registrant successfully completes and submits their responses. Similar unique emails invite participants to renew data annually, via a linked REDCap survey.
Hardware and software
All systems are hosted on-site on two purchased Dell PowerEdge 720 server systems running Microsoft Windows 2012 R2 Enterprise Edition (institute enterprise license). Two virtual machines (VM) run the REDCap application. The first VM is a web front end with IIS 7; the second is a MySQL database. A third VM hosts the WordPress application. The decision to run on VM consists of two main factors: the ability to transfer between core OS in case of physical failure and the ease of VM backups and restores. If the host server is downed due to system malfunction or hardware issues, the VMs are easily moved to another server, reducing registry downtime. The only limitation due to internally hosting the registry is if there is a long-term power or network outage.
Data elements
Registry design choices were made with a focus on feasibility, data usability, and participant burden and preferences [23]. We aimed to collect data that instruct study eligibility and recruitment, and identification of individuals at greatest risk for AD biomarkers [24]. All data are self-reported, obviating the need for Health Insurance Portability and Accountability Act approval from participants.
Demographic data include name and contact information, date of birth, sex, height, weight, race, ethnicity, years of education, and spoken languages. We collect data related to maternal and paternal medical history, as well as current medical history, including prescription medications. Medical history includes specific questions regarding cancer, neurological, and psychiatric diseases. We use REDCap’s ability to connect to BioPortal site (RxNORM) to collect medication information and ensure accuracy [25]. For registrants, medications are captured within the survey with a simple text entry search. We inquire as to the availability of another person, such as a spouse, family member, or friend, who could join the registrant at study visits.
To assess physical activity levels, we use an eight-item scale that examines the number of days-per-week, over the last year, the registrant achieved specific levels of exercise [26]. Dietary habits are assessed using the brief food frequency questionnaire [27]. Subjective cognitive performance and research attitudes are examined using the Cognitive Function Inventory (CFI [28]) and the Research Attitude Questionnaire (RAQ [29]), respectively.
Registrants are asked to indicate their preferred methods of contact and their interest in being notified about studies involving approved medications, investigational medications, altering diet or lifestyle, blood draws, cognitive testing, magnetic resonance imaging (MRI), positron emission tomography (PET), lumbar puncture, and autopsy. Although genetic testing is not performed, we survey registrants’ willingness to undergo blood draw at the medical center and to receive a buccal swab kit at-home, both for the purpose of genetic testing.
Recruitment to the UCI C2C
Our goal was to enroll 1000 local participants in the first year. Table 1 outlines recruitment strategies used in the first 12 months, categorized as earned media, community outreach, referrals, email, Internet/social media, and other. Recruitment began with an email invitation to a distribution list maintained by UCI MIND (n = 1,184). Community outreach performed over the reporting period included more than 35 educational presentations at which the registry was consistently advertised and typically included the opportunity for attendees to enter their email addresses using iPads. iPads were also maintained at UCI MIND resource tables at community health fairs and local Alzheimer’s walks (n = 17). The support of a pro bono public relations firm was secured to assist in attaining traditional (newspaper, television, and radio) and Internet (news, blogs, and social media) earned media stories. From December 2016 to September 2017, 53 publicity stories were achieved in trade and local publications, websites, and blogs. In addition, we used social media (15 Facebook posts, 2 paid Facebook advertisements, and 26 Tweets) to promote the registry. The C2C was registered in the Alzheimer’s Association’s TrialMatch [30]. Referrals were made by local dementia support organizations, physicians, and UCI faculty and staff. One email request was made of current registrants to invite 1-2 friends or family members to enroll in the registry. To facilitate this referral, a template email invitation was shared with registrants.
Registry recruitment strategies and effectiveness. (Multiple sources were reported for 26 cases)
*Based on self-report at full enrollment.
We report estimated effectiveness for recruitment activities, based on the relationship in time between those activities and email enrollments. At full enrollment, registrants self-report the means by which they learned about the registry. We also report these data and compare them to our overall recruitment efforts.
Engagement
Annual retention rates for some national registries are below 50% [12]. Retention is critical, given that most registrants will not be invited to participate in a study in a given year, [18] and many registrants expect to be contacted relatively soon after signing up. Thus, considerable effort went toward optimizing registrant retention. At enrollment, registrants are given the opportunity to opt-in to regular electronic newsletters from UCI MIND and to register for Health Tweets from UC Irvine Health. The C2C maintains a blog for the community of registrants, which includes compiled blog postings from three UCI sources (http://www.mind.uci.edu/blog/, https://www.ucirvinehealth.org/blog, https://ucistemcellresearchcenter.wordpress.com). Immediately after enrollment, a “thank you” email demonstrates appreciation and explains that not all registrants are invited to enroll in a study within the first year. A similar email is sent at six months to those enrollees who have not yet been contacted about a study. An appreciation gift, a C2C refrigerator magnet, was sent to each enrollee approximately nine months after initiating the registry, along with a thank you letter from the principal investigators and a second magnet to share with a friend who might enroll.
Registrants are invited to renew their enrollment annually. Beginning three months prior to the one-year anniversary of enrollment, monthly invitations to renew are sent. At renewal, demographic and medication data are prepopulated and registrants are requested to confirm accuracy. Some data elements are collected longitudinally, including the exercise and diet questionnaires, CFI, and RAQ.
Regulations
Any UCI investigator with a protocol approved by the UCI IRB is eligible to recruit from the registry. Investigators are instructed to list the C2C as a recruitment source in their IRB protocol. IRB-approved flyers and brochures can be email “blasted” to registrants. Investigators can utilize registry data to increase recruitment efficiency. Once IRB approval is in place, registry staff work closely with investigators to design a query that minimizes identification of ineligible or unwilling registrants. Queries automatically prioritize registrants not previously contacted about a study. Query results (typically limited to n = 50 potential registrants) are shared with the study team for active recruitment by email, mail, or phone. Query results include potential participant contact information, but may also include registry data to facilitate prioritized recruitment (e.g., of those with the highest RAQ scores). There is no limit to the number of queries that can be performed for a given study, but additional query results are provided only to investigators providing recruitment data. The investigative team is expected to carefully document the outcomes of each query (i.e., number of registrants reached, number of registrants deemed ineligible prior to in-person visit, number of registrants declining enrollment, number of registrants screened, number of registrants enrolled). To facilitate this, an excel file containing the registrant names and categories of potential outcomes of recruitment are sent to each team. The files are collected and maintained by the registry team. Data for linking query and recruitment outcomes are stored within the same REDCap infrastructure instance, but data are kept in separate projects with different user access.
Effectiveness of the UCI C2C
We report the activity of recruiting from the C2C registry, including the total number of queries, the total number of potentially eligible registrants identified, and the outcomes of their recruitment by independent study teams. We provide additional details for queries recruiting to a preclinical AD trial, the Anti-Amyloid treatment in Asymptomatic AD (A4) study [31]. The A4 study is exemplary of the type of studies that the registry was built to support.
Ethics
The UCI C2C is approved by the UCI IRB. Individuals submitting only their email address to the registry are not considered to have enrolled in a research protocol. Prior to submitting personal data, registrants sign informed consent electronically. This is completed by using a finger or stylus when enrolling via phone or tablet and with a mouse when enrolling by computer.
RESULTS
Construction
Registry development involved approximately one year of planning, design, and construction. The REDCap infrastructure facilitated the rapid development of the data collection instrument. Website development was achieved through part-time freelance web designers, who spent a total of 236 hours on web design. Open source programs were used wherever possible and for several instances institutional licenses were leveraged, reducing costs. In total, the estimated cost of launching the C2C website, including freelance support, hardware and software, printing and mailing, and miscellaneous supplies, but not accounting for full-time faculty and staff effort was $19,970.
Enrollment in the UCI C2C registry
The registry was launched on August 16, 2016. In the first year of existence, 957 individuals registered their email addresses, of whom 592 (62%) enrolled in full, providing demographic, medical, and other data. Although enrollment was consistent over time, it was largely related in time to recruitment activities (Fig. 1). Sixteen recruitment activities resulted in 23 24-hour periods in which more than ten individuals enrolled. These periods accounted for 543 (57%) of the total initial email enrollments. Eleven of these 23 peak days were attributed to community outreach events, six to earned media appearances, two to Internet news stories and social media postings, two to referrals, and two to email solicitations. As seen in Table 1, earned media produced more full enrollees (37%) than any other recruitment strategy. One local newspaper article about the registry resulted in at least 104 full enrollments. Referrals (25%) and community outreach (22%) were the next most effective recruitment strategies.

UCI C2C enrollment over time. Cumulative email (dotted line) and full (hashed line) enrollment are plotted over the first 12 months of the C2C registry. The solid line displays 24-hour email enrollments. Twenty-three specific occurrences of greater than 10 enrollments within a single 24-hour period are coded based on the recruitment strategies that elicited these peaks (A, earned media; B, community outreach; C, referrals; D, email; E, Internet), with some activities resulting in more than one 24-hour period of high activity.
Table 2 describes the population fully enrolled in the first year. The mean age is 63 years. Two-thirds of registrants are female and most are Caucasian and non-Latino. Asian American and Latino registrants each make up 7% of the enrollment population. The most frequently reported medical conditions are hypertension (26%) and hypercholesterolemia (24%). Twenty-two percent of registrants have been diagnosed with a cancer, of whom 45% report basal or squamous cell carcinoma. On average, registrants are taking three prescription medications; 78% of participants are taking at least one prescription medication. The most common prescription medications taken by registrants are anti-hypertensives (27%), cholesterol-lowering drugs (22%), and thyroid medications (11%). Two percent of participants self-report a diagnosis of mild cognitive impairment (MCI); 1% report a diagnosis of AD.
Description of registrants
Figure 2 illustrates the proportion of registrants willing to engage in studies involving specific research procedures. Greater than 90% of registrants are willing to be contacted about studies involving cognitive testing, magnetic resonance imaging, blood draws, and lifestyle or diet interventions. Similarly, 94% of registrants are willing to donate blood and 95% are willing to receive saliva kits at home for the purpose of genetic testing to be better matched to appropriate studies. In contrast, 40% of those registering are willing to be contacted about studies involving lumbar puncture. Eighty-six percent of participants are willing to be contacted about studies of approved medications; 78% are willing to be contacted about studies of investigational medications.
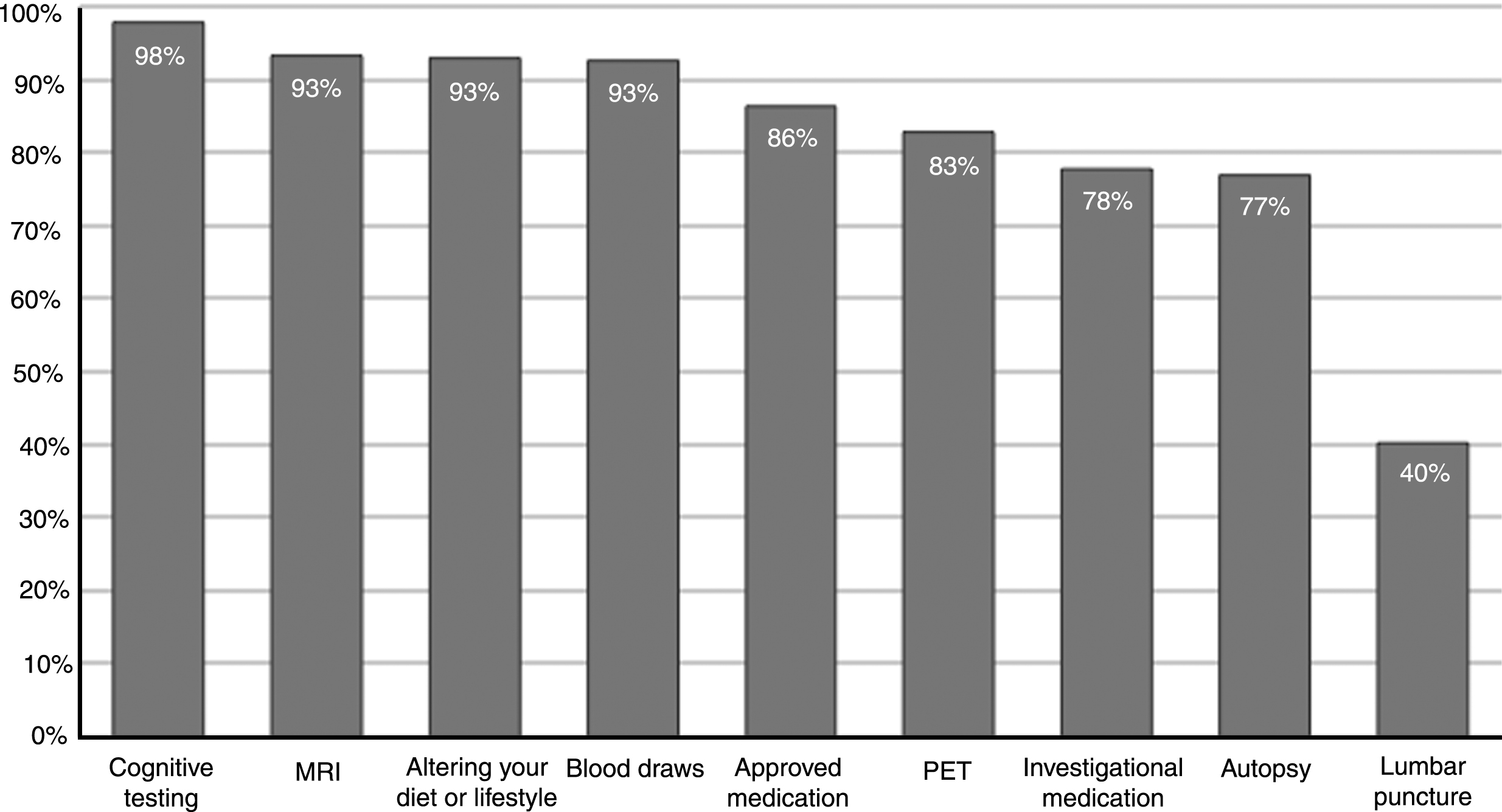
Registrant willingness to be contacted about studies. The proportion of registrants who indicated willingness to be contacted about studies involving specific interventions or research procedures is illustrated. MRI, magnetic resonance imaging; PET, positron emission tomography.
Efficiency of recruiting from the registry
In the first year, 291 registrants were identified in queries seeking to recruit to studies. Outcomes data were unavailable for 20 participants. Thirty-seven percent were not reached; 19% declined; 9% were ineligible based on phone screen. Eighty-two (28%) individuals were enrolled in nine studies. Of these, 26 were deemed ineligible at screen; the remaining 56 (19%) were enrolled.
In the first year, 129 registrants were identified as potentially eligible for the A4 trial. Of these, 26% were not reached, 37% declined participation, 17% were deemed ineligible via telephone screen. Twenty-five individuals enrolled, of whom 22 underwent amyloid imaging. Six were eligible and randomized.
DISCUSSION
We report the experiences of developing, launching, and preliminarily using a local potential participant registry to enhance clinical research recruitment at an academic research institution, including recruitment to preclinical AD trials. A recent review of registries as tools to improve recruitment concludes that a variety of factors are critical to consider when designing and building a research registry [13]. These include purpose, infrastructure, governance, targeted population, informed consent, data collection and data security methods, and operations. We provide details for our rationale and methods of addressing several of these factors, as well as our initial experiences in recruiting clinical research participants from the C2C registry.
Our experiences may offer guidance to other investigators wishing to initiate registries to support research recruitment. We used an electronic consent form and treated enrollment in our registry as enrollment in a unique study. Indeed, an added goal of our registry is to engage in the science of recruitment, to test optimal means to recruit to and enroll from these important but still new tools.
Our registry capitalizes on a variety of open source software programs and a free academic data infrastructure backbone. Costs of building and initiating our registry included needed hardware and freelance support to facilitate public website development for its enrollment site. In total, this cost was lower than that for large national registries, which have been estimated at several hundreds of thousands of dollars [13]. Not factored into our cost estimates, however, are faculty and staff effort. Substantial time went into planning, designing, and constructing the registry. This included time for a full-time staff data manager with expertise in the needed hardware and software. Since launched, faculty and staff have committed considerable effort to recruitment, monitoring registry enrollment and adjusting recruitment strategies, engaging registrants, and maintaining IRB approval.
We also benefited from pro bono support from a local public relations agency, which greatly increased earned media appearances and kept costs low. Earned media produced the highest number of recruited registrants, though some forms of earned media were more effective than others [15]. In particular, one article in a local newspaper was the single most effective recruitment activity. Postings in local blogs, as well as television and radio appearances, were less effective.
Beside earned media, our recruitment strategies were largely community-based. Two primary modes of community outreach were used; traditional public education programs focused on AD research, and vendor tables at health fairs and large events such as walks to raise awareness and funds for AD supportive services and research. Public talks featuring faculty members or other investigators, which had an average audience size of 121 attendees, produced substantially more registry enrollments than did vendor opportunities at local walks, which had an estimated mean attendance of 392 people. Though effective, our community outreach was not exhaustive. For example, others have used direct mailings to recruit to registries [12] and AD prevention trials [32]. Still others have successfully recruited to registries through clinical services [33].
We chose an online model for C2C to facilitate high enrollment. While this may result in a selection bias toward technological savvy volunteers, some investigators have postulated that online targeted advertising is likely to generate more registry enrollment than would community outreach [12]. For us, social media, including a small number of Facebook advertisements, were minimally effective in enhancing recruitment. In fact, more individuals indicated that they discovered our registry through general Internet searches than enrolled after learning about the C2C through social media. Referrals, however, including referrals from friends who had joined the registry, were an effective recruitment source. This may suggest that with coordinated and sophisticated social media campaigns, registry enrollment may have the possibility of ‘going viral.’
The population we recruited to the C2C had high scores on the RAQ and was largely willing to consider studies involving a variety of research procedures, though willingness to consider autopsy and lumbar puncture were lower (Fig. 2). Compared to some other registries, [15] we observed a higher rate of willingness to undergo genetic testing. This may be a function of time and the increasing use of direct-to-consumer advertising for genetic tests [34]. Genetic testing may provide a critical first step to identifying biomarker positive preclinical AD trial candidates and at least two preclinical AD trials implement genetic enrollment criteria exclusively [35]. These results may suggest registrants are comfortable with researchers using genetic information to identify ideal trial candidates. Indeed, the opportunity to learn genetic risk information may incentivize some registrants to enroll in interventional research [9].
In total, the registry resulted in 25 additional screens for an ongoing preclinical AD trial. Of these, 6 participants were ultimately determined to have elevated levels of brain amyloid and randomized. The impact on enrollment to this trial was limited by the fact that construction of the registry was not completed until the late stages of trial recruitment and the fact that prioritized recruitment of those most likely to be eligible based on AD biomarker testing (e.g., older, family history of AD, presence of subjective complaints) was not attempted. Despite these limitations, the number of screens and randomizations were meaningful boosts to recruitment, representing approximately 20% of the site activity, overall.
Conclusions
These results suggest that local registries may enable improved research recruitment, especially in preclinical AD trials. Local registries may offer unique strengths, complementing larger national or regional registries. Local media referrals, and local community talks were effective in increasing enrollment. And compared to some previous registries, we observed greater willingness among registrants to undergo genetic testing and other procedures, perhaps indicating a higher level of trust. Though the cost of initiating our registry was reduced, compared to larger national registry estimates, substantial faculty and staff time went into planning, launching, and maintaining the registry. Preliminary data indicate that this cost ultimately will yield increased study recruitment, though future efforts will need to focus on increasing recruitment efficiency.
Footnotes
ACKNOWLEDGMENTS
This work was made possible by a donation from HCP, Inc. JDG, DH, DLG, CGC, KK, MW, and AP were supported by NIA AG016573. JDG and DG were supported by NIA 1R21AG056931. JDG and AG were supported by UL1 TR000153. We wish to thank The Brower Group, an Orange County, CA, public relations agency, for their pro bono support.