
Abstract
Background:
Identifying patients at high risk of delirium is crucial to facilitate prevention. Although dementia is the most consistent risk factor across populations, it remains under-diagnosed. Hence understanding other markers of delirium vulnerability on admission is important.
Objective:
We aimed to identify predictors of incident delirium development in older medical inpatients that were readily identifiable at presentation to the emergency department.
Methods:
Medical inpatients of ≥70 years were assessed on admission for delirium using the Revised Delirium Rating Scale (DRS-R98) and those with prevalent delirium were excluded. Consenting non-delirious patients were then assessed daily using the DRS-R98. Data pertaining to multiple baseline delirium risk factors were collected, including pre-morbid dementia. Multivariable logistic regression was used to examine which factors predicted the development of incident delirium.
Results:
Of 555 patients approached, 184 (33.1%) had prevalent delirium. Following other exclusions, 191 were included in the study and 61 developed incident delirium. Predictors of incident delirium on multivariable analysis, controlling for confounders, were dementia (OR 2.54, 95% CI 1.01–6.43, p = 0.048); Barthel Index score (OR 1.15 for each unit decrease in score, 95% CI 1.06–1.25, p = 0.001), and Modified Cumulative Illness Rating Scale score (OR 1.13 for each unit increase in score, 95% CI 1.05–1.22, p = 0.001).
Conclusion:
Dementia is a well-known risk factor for delirium; however, it too is under-recognized and on admission can be missed. Conversely, the Barthel Index is a simple and widely used measure of functional ability that may prove useful in stratifying those at risk of in-hospital delirium on admission.
INTRODUCTION
Delirium is highly prevalent, being present in 10–31% of older medical patients on admission and occurring de novo in 3–29% during their hospital stay [1]. It leads to increased mortality [2] and morbidity [3] and more than doubles healthcare costs [4]. Despite this, it remains poorly detected, being missed in up to 76% of cases attending the emergency department (ED) [5] and in approximately two-thirds of older medical inpatients [6]. Proactive multifaceted systematic interventions aimed at modifying delirium risk factors can halve delirium incidence [7], but risk stratification and prognostication of older adults presenting to the ED is challenging [8].
Several delirium risk factor studies have been conducted in multiple settings and patient groups, the most consistently reported predictors being advanced age, premorbid cognitive impairment, and co-morbid illness [9]. A 2014 systematic review conducted by Ahmed et al. [10] found that these three factors were among those most commonly associated with incident delirium in older medical inpatients. In 2010, the United Kingdom’s National Institute for Health and Clinical Excellence (NICE) published guidance on the diagnosis, prevention, and management of delirium [11]. These guidelines include a review of risk factors for delirium in adult patients in both hospital and long-term care settings, concluding that those at highest risk are older patients, those with cognitive impairment, those with a current hip fracture, and/or severe illness. The NICE guidelines recommend that all patients meeting these criteria should undergo daily delirium screening and be placed on a delirium prevention pathway once admitted. This categorization includes most hospital inpatients, and all older patients, and correctly reflects the pervasiveness of delirium across hospital settings. However, in the busy acute sector, targeting those at highest risk of developing delirium at point of presentation to the ED may make the implementation of multicomponent risk factor modification programs more feasible.
In terms of risk stratification, several clinical prediction tools exist [12], however these can include elements not easily assessed at presentation [13], require blood test results [14] or involve complex calculations, unsuited to the demands of busy clinical practice [15]. In this study, we aimed to identify predictors of incident delirium in older medical patients, based on information readily available and easily recordable at the point of hospital admission, and without the need for results of bloodwork, repeated measures (e.g., vital signs), or complex calculations (e.g., illness severity), in an effort to simplify risk stratification in this population.
MATERIALS AND METHODS
Setting and participants
This prospective observational cohort study was conducted in two teaching hospitals in Cork city, Ireland (Cork University Hospital and the Mercy University Hospital) between October 2011 and August 2013. Patients of ≥70 years of age admitted medically through the ED were screened for study eligibility within 36 h of presentation to ED (and usually within 24 h). The number of participants recruited at a time needed to be controlled because this prospective study required daily assessments by a single assessor (NO’R) for the first week of admission. Hence, participant sampling was non-consecutive and recruitment was conducted only on weekdays. To minimize bias, recruitment days were pre-defined and, depending on included numbers, either all or the first ‘n’ of older emergency medical admissions were considered eligible on days of recruitment. Those who refused, who were gravely ill or dying, or who were admitted to the intensive care unit were excluded from screening assessment. Following initial assessment, patients with prevalent delirium on admission (identified by NO’R using the Revised Delirium Rating Scale, DRS-R98, see below); and those in whom formal delirium assessment was impossible due to coma or severe communication difficulties (e.g., severe dysphasia, non-communicative dementia) were excluded from longitudinal assessment. Informed consent was sought from those eligible for inclusion and consenting participants underwent daily assessment for delirium development for the first week of admission or until discharged (including weekend days). Patients discharged early without delirium (within 3 days of admission) were excluded from the study due to inability to confidently outrule incident delirium post-discharge.
Assessments used: Delirium
A trained delirium assessor (NO’R) performed all delirium assessments using the Revised Delirium Rating Scale (DRS-R98), an instrument validated for discriminating delirium from other neuropsychiatric diagnoses, with high inter-rater reliability, sensitivity, and specificity [16, 17]. This 16-item clinician-rated scale comprises 13 severity (symptom) items and 3 diagnostic (contextual) items and is used to rate symptoms and their context over the previous 48-h period. Higher scores indicate a greater severity of delirium. Users are trained to score this instrument using all available sources of information, including assessment of the patient and discussion with nursing staff and family or caregivers. In this study, delirium was diagnosed using a cut-off of ≥15 on the severity scale and/or ≥18 total score, in keeping with guidelines for its use [18].
Potential delirium predictors
Potential predisposing and precipitating factors in medical inpatients were identified by reviewing the existing literature, including the NICE guidelines [11]. We included baseline factors that can be recorded routinely on arrival to the ED. We excluded laboratory tests (as these require processing time) and factors that are measured repeatedly (e.g., vital signs).
Data pertaining to potential delirium predictors were collected by NO’R and JF. Demographic data and social history factors were recorded including age, sex, marital status, place of residence, social support, level of educational attainment, and alcohol and smoking history. Excess alcohol intake was defined as drinking more than 14 units per week for females and more than 21 units per week for males [19]. Comorbidity burden was calculated using the Modified Cumulative Illness Rating Scale for Geriatrics (M-CIRS) and medication use was recorded (see below). Prior history of depression was obtained from the medical chart. The method used to ascertain premorbid cognitive status is described below. The Modified Barthel Index (BI) was used to assess functional status on admission and the Mini-Nutritional Assessment – Short Form (MNA-SF) graded nutritional status. Simple screening assessments of hearing and sight were performed at the bedside. A modified version of the Geriatric Depression Scale, the ABCDS (AB Clinician Depression Screen) [20], was used to screen for current depression.
Medications and polypharmacy
A list of admission medications was compiled, including those taken regularly or on a PRN (as required) basis. The term polypharmacy refers to the use of multiple medications by a patient; however, because there is no international consensus numerical value for polypharmacy, we considered the two cut-offs cited in the NICE guidance: three-or-more (≥3) and five-or-more (≥5) medications [11]. Additionally we collated a list of potentially deliriogenic medications (see Table 1) based on the existing literature [21] and on the NICE guidelines [11]. We separately assessed medication as a binary variable (0 or ≥1 potentially deliriogenic medication) and a continuous variable (total number of potentially deliriogenic medications). This data was collected by NO’R.
List of medications included as potentially deliriogenic *
*Analyses were repeated including antipsychotic medications and NSAIDs respectively as these medication classes have been shown in some studies to be associated with delirium development [21, 42] however there remained no significant association. Given that both antipsychotics and NSAIDs may have a protective effect in relation to delirium development, the analysis reported includes neither of these medications classes (Kalisvaart et al. [41]; Cunningham et al. [43]).
Assessment of previous cognitive status
The Informant Questionnaire on Cognitive Decline in the Elderly Short-Form (IQCODE-SF) [22] was used to screen for pre-morbid dementia. This 16-item scale, scored by a caregiver or near relative, examines degree of cognitive change over a 10-year period. In this study, a mean item cut-off score of ≥3.5 was used as a cutoff for pre-morbid dementia in keeping with similar study cohorts reported prior to this study’s inception. [23]. Patients were also assessed using the Standardized Mini-Mental State Examination (SMMSE) [24], an operationalized version of the Mini-Mental State Examination (MMSE) [25]. In borderline cases, diagnosis was reached by consensus discussion (with ST and DM). In the absence of an IQCODE-SF or previous diagnosis of dementia made by an appropriately trained physician, ascertaining premorbid cognitive status was challenging. Because dementia prevalence has been found to be 2% in patients with MMSE scores of ≥27/30 [26], we considered those with similar scores on the SMMSE not to have dementia. Premorbid cognition was recorded as “unknown” in participants with SMMSE scores <27/30 without IQCODE-SF (n = 2).
Statistical analysis
Demographic data were expressed as means±standard deviation (SD) or medians and interquartile ranges (IQR), depending on the distribution of the data. Intergroup comparisons (delirium, no delirium) were made using a χ2 or Fisher Exact test for differences in proportions, a t-test for differences in means or non-parametric tests for rank differences. Univariate logistic regression was used to assess if clinically relevant baseline predictor variables were associated with incident delirium. Variables with p < 0.1 were included in a multivariable logistic regression model, using a simple “enter” method, where all significant variables were entered in the model together, as well as age and sex. The final model was assessed using the Hosmer-Lemeshow (CHL) test for goodness of fit, and fitted the data well (p > 0.05). Multicollinearity with the independent variables was investigated using the variance inflation factor (VIF) and tolerance statistic and where there was collinearity between variables, the most clinically relevant variable was included in the model, so that all the remaining variables had a VIF less than 10 and a tolerance statistic more than 0.1. Analyses were conducted using SPSS version 20.
RESULTS
During the study period, 555 patients were approached and 529 were assessed (Fig. 1). Prevalent delirium on admission was detected in 184 patients (34.8%), while 23 patients were not amenable to full delirium assessment on day 1 due to coma, stupor, or communication problems. Thus, 322 patients were initially included. Of these, 88 were discharged within three days without incident delirium, 36 withdrew, five underwent surgical procedures and two became too unwell to participate, all of whom were excluded from the analysis. Hence, 191 patients were included in the final analysis, of whom 61 (31.9%) developed incident delirium. Of these, the majority (n = 139, 72.8%) were admitted for one week or more (median length of stay 9 days, IQR 6), see Table 2. The median age of the included patients was 80 (IQR 10), 52.9% (n = 101) were male and 16.9% (n = 32) had premorbid dementia. We identified a priori, from the existing literature and using clinical judgement, factors that had the potential to increase delirium risk. Table 3 reports the odds ratios of important variables in relation to incident delirium development. Those who developed delirium were slightly older and more likely to have pre-morbid dementia, depression, and hearing impairment. They also had higher comorbidity and functional dependence and were more undernourished. Patients with incident delirium were also more likely to have either family support or formal social support. This was considered a surrogate marker for functional dependence, and not in itself likely to be a delirium risk factor so we did not include this factor in multivariable analysis. Clinically relevant variables with p < 0.1 on univariate analysis were entered in a multivariable logistic regression model (Table 4). The final model identified that M-CIRS, BI, and premorbid dementia were independently predictive of incident delirium in this cohort with adjusted Odds Ratios (OR) of 1.15 (95% CI 1.06–1.25, per 1 unit M-CIRS increase); 1.13 (95% CI 1.06–1.25, per 1 unit BI decrease); and 2.54 (95% CI 1.01–6.43), respectively.
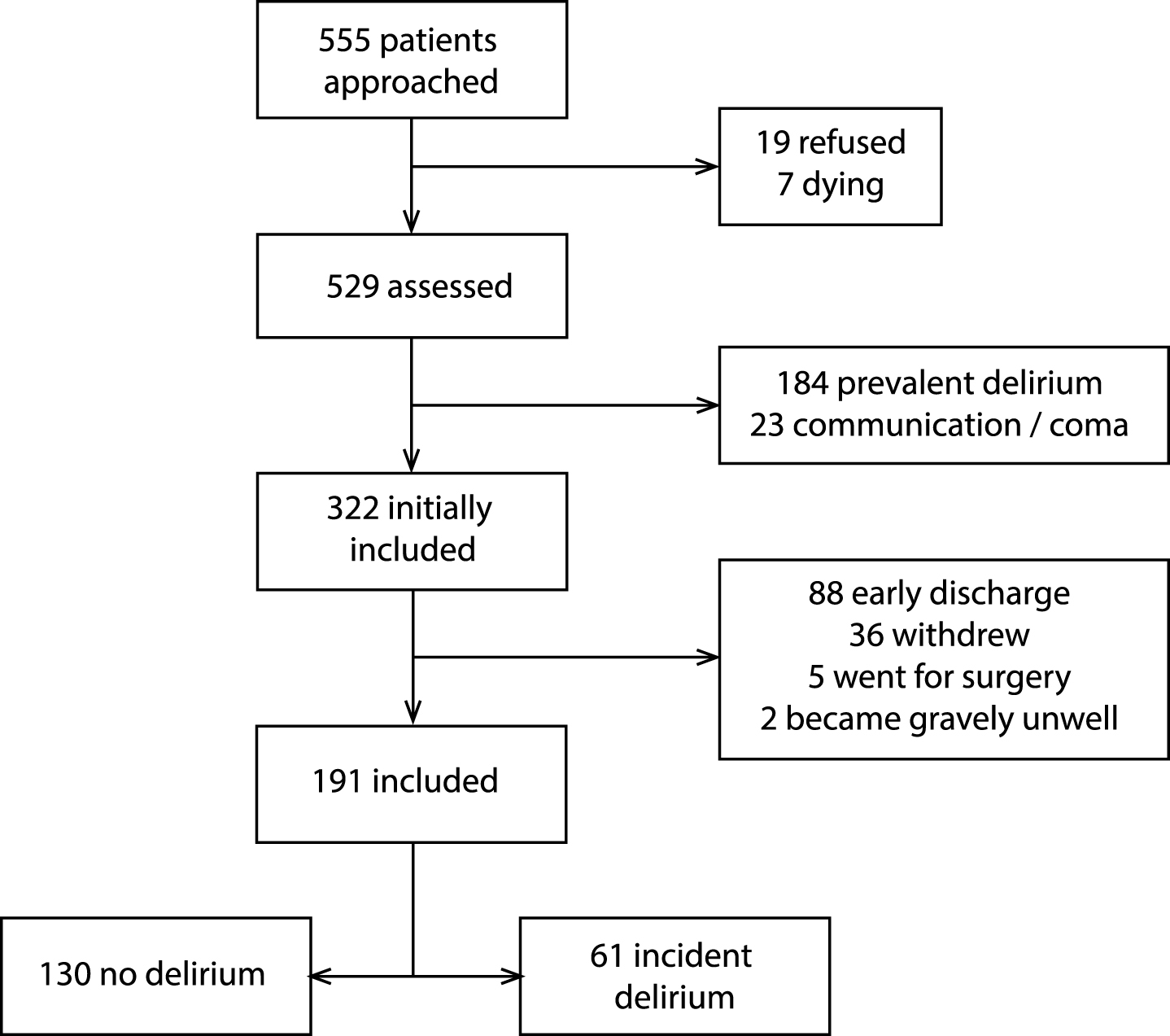
Flow of patients through the study.
Characteristics of the cohort *
*t-test for continuous data and Chi-squared test for categorical data unless ¶Mann-Whitney U-Test +Fisher’s exact test.
**Excess alcohol intake was defined as drinking more than 14 units per week for females and more than 21 units per week for males [19].
***Premorbid dementia was based on IQCODE-SF scores, SMMSE scores, and consensus discussion as outlined in text.
Odds Ratios for clinically relevant variables in relation to incident delirium development
β, coefficient; OR, odds ratio; CI, confidence interval; BI, Modified Barthel Index; M-CIRS, Modified Cumulative Illness Rating Scale; MNA-SF, Mini Nutritional Assessment – Short Form. Residence was recoded as the binary variable ‘nursing home resident yes / no’; Alcohol excess was recoded as ‘current alcohol excess yes / no,.
Association (multivariable logistic regression) between independent variables and incident delirium
β, coefficient; OR, odds ratio; CI, confidence interval; BI, Modified Barthel Index; M-CIRS, Modified Cumulative Illness Rating Scale; MNA-SF, Mini Nutritional Assessment Short Form.
We found that patients with incident delirium have respectively significantly lower BI scores and higher M-CIRS scores (Table 2) on admission than those who remain non-delirious throughout. Our data cannot provide a cut-off score that accurately predicts incident delirium for either of these variables, given that the boxplots overlap (Fig. 2). Nonetheless, we examined BI as a predictor variable in more detail (as this is the more practical instrument to use in the ED). Again, using multivariable logistic regression, we examined the predictive ability of BI using several cut-off scores and found that BI with a cut-off of 16 / 17 as a predictor variable had an adjusted odds ratio of 7.08 (95% CI 2.5–20.04, p < 0.001) in the prediction of incident delirium. The most parsimonious model included also premorbid dementia status and M-CIRS score (–2 log likelihood 181.96, Hosmer-Lemeshow test p = 0.974) and correctly predicted delirium status in 76.1% of cases.

Boxplots for the distribution of (a) Barthel Index and (b) M-CIRS Based on Groups defined by Incident Delirium Status.
DISCUSSION
Delirium is known to be a multifactorial condition, with more than one causative factor evident in most episodes [27]. Identifying high risk patients on admission is important so that delirium prevention strategies can be targeted most effectively. Multiple risk factor studies have shown a diverse range of predisposing and precipitating factors; however, many studies do not differentiate between incident and prevalent delirium, which is crucial in order to ascertain which factors predated delirium development [10, 28]. Additionally, some risk factor studies report factors that involve excessive complexity in delirium risk stratification, for example delirium predictors that require laboratory sample analysis, such as serum urea [14, 30] and serum albumin [31, 32], or predictive models that involve a mathematical calculation [15]. Our aim was to examine factors present on arrival to ED that may identify those at significantly higher risk of developing in-hospital delirium. We found three independent risk factors for incident delirium: pre-morbid dementia; high comorbidity; and high functional dependence. These risk factors have been identified in other studies, pre-existing cognitive impairment being one of the most consistently recognized delirium predisposing factors across clinical settings [10, 34].
Co-morbid illness has also been shown in several studies to be independently predictive of delirium development. A study of 667 older hospitalized patients in Mexico, using the Cumulative Illness Rating Scale (CIRS) to evaluate comorbidity burden, found an adjusted OR for delirium development of 1.16 for each unit CIRS increase (95% CI 1.04–1.3, p = 0.006), independent of other factors, findings very similar to ours [32]. Inouye and colleagues found that high comorbidity indicated by a Charlson Comorbidity Index (CCI) score of >4 was independently predictive of delirium diagnosis at discharge from hospital (OR 1.7; 95% CI 1.1–2.6) in older medical patients. This effect of comorbidity has also been shown in surgical patients, again using either CIRS [35] or CCI [36].
Functional dependence [14, 37–40] has also been found in previous studies to be associated with delirium. Martinez and colleagues identified high level of dependency as one of three predictive factors in a model developed to classify delirium risk in patients on internal medicine wards [40]. Another study conducted by Carrasco and co-workers found that older patients with good functional status who are not dehydrated on admission are highly unlikely to develop incident delirium, independent of increasing age [15]. This predictive model requires laboratory measurement of serum urea and creatinine, along with BI measurement of function, with a subsequent calculation to infer delirium risk. Markers of dehydration, for example increased urea, or urea / creatinine ratio have been shown to be a risk factor in other studies [14, 29], however we did not include laboratory values in our analysis, given that our aim was to investigate risk factors that can be ascertained either by the referring doctor or immediately on presentation to the ED.
As well as functional dependency, the predictive model developed by Martinez and colleagues included two other risk factors: age >85 years old and being on centrally acting drugs, including antipsychotics [40]. We chose to assess medication burden in a variety of ways. We assessed polypharmacy using cut-offs of both ≥3 or ≥5 medications, as outlined in the NICE guidance [11]. We created a list of potentially deliriogenic medications on admission (see Table 1) and analyzed this variable in two ways. Firstly, using a binary approach we identified if a patient was or was not on one or more potentially deliriogenic medication, and secondly, we calculated the number of potentially deliriogenic medications each patient was in receipt of and entered this variable as a scale. We compiled this list to include medications identified in a systematic review by Clegg et al. [21] as associated with higher risk of incident delirium, as well as those for which there is uncertainty regarding the risk of delirium. We also included additional medications outlined in the NICE guidance as being potentially deliriogenic [11]. Martinez and colleagues included antipsychotics as a culprit medication, however the evidence regarding this drug class is mixed, with one RCT in hip fracture patients showing that haloperidol was not associated with increased delirium risk [41] and other studies finding an independent association between antipsychotic use and delirium development [33, 42]. Nonetheless, we repeated the analysis including antipsychotics as a potentially deliriogenic medication and our results did not differ. Non-steroidal anti-inflammatory drugs (NSAIDs) are another medication group in which there remains uncertainty in relation to delirium risk [21]; however, given that cyclo-oxygenase inhibition may have a protective effect in mouse models [43], we excluded NSAIDs from our list of potentially deliriogenic medications. We did also repeat the analysis including NSAIDs and there remained no significant association with incident delirium. It is unclear why medication burden was not predictive of delirium development in this cohort, when the literature suggests increased risk with many medications. It is possible that our study was underpowered to detect a significant effect of medications.
Older age was not an independent predictor of incident delirium in our cohort, despite being one of the most consistent risk factors throughout the literature [11], however as in a study conducted by Inouye and colleagues [14], using an age cut-off of >70 years for study inclusion may mean that we had a priori adjusted for age. The systematic review by Ahmed et al. of risk factors for incident delirium in older medical inpatients found on pooled analysis that dementia, illness severity, visual impairment, polypharmacy, low albumin, urinary catheterization, and length of hospital stay were statistically significantly associated with delirium development [10], the first four of which are readily identifiable at presentation. Of these factors, our study similarly identified dementia and comorbidity burden as predictors of incident delirium; however, no significant association was found between delirium development and the presence of visual impairment or polypharmacy.
The strengths of our study include the prospective design; the performance of daily assessments throughout the first week of hospitalization; as well as the use of a highly sensitive and standardized delirium diagnostic instrument performed by a trained and experienced assessor. There were few exclusion criteria and hence our cohort is likely to be representative of real world older medical inpatient populations. The patients were carefully assessed for pre-morbid dementia; functional dependence; comorbidity; medication burden; and for other risk factors, focusing on clinically relevant and easily identifiable risk factors. We found that functional impairment, premorbid dementia, as well as comorbidity burden were independently predictive of delirium development within the first week of admission, emphasizing that delirium occurrence is a marker of general vulnerability, sharing risk factors with other geriatric syndromes, such as falls.
Despite the methodological strengths, this study does have some important limitations. Firstly, the sample was non-consecutive, as with a single delirium assessor, it would not have been feasible to assess consecutive patients in the longitudinal fashion required for the study’s robustness. Secondly, we did not collect data on all potential delirium risk factors that have been cited in the existing literature, for example illness severity score and serum urea level [10], hence we may have missed important delirium predictors in this cohort. Furthermore, there is potential for selection bias given that the researcher who conducted the delirium assessments also conducted the majority of the risk factor profiling (NO’R). Patients were recruited only from Monday to Friday, which may also introduce bias into the sample. Many (n = 131) originally included patients were excluded from the final analysis for several reasons (see Fig. 1). These 131 excluded patients did not differ significantly from the 191 included patients in terms of age (median age 79, IQR 10 compared to median age 80, IQR 9 in included patients, p = 0.532, Independent Samples Mann-Whitney U-Test) and sex (55% of excluded patients were female compared to 47.1% of the included patients, p = 0.167, Pearson χ2 Test), although data pertaining to the other baseline characteristics was not available on the majority of these excluded patients, so we cannot say for certain if they were significantly different overall. The 88 non-delirious patients discharged within 3 days were excluded from the analysis as we could not ascertain if they went on to develop delirium or not post-discharge. We did include non-delirious patients admitted for the greater portion of a week (≥4 days), each with at least four detailed serial delirium assessments (n = 42/130, 32.3%), as we considered this group to be less likely to go on to develop delirium post-discharge, although we cannot be completely certain that this is the case. Because only older medical inpatients were considered, our findings cannot be generalized to surgical or intensive care patients, or to other groups. Furthermore, we explored only the predictors of incident in-hospital delirium, excluding prevalent delirium on admission, and hence we cannot deduce factors that are associated with prevalent delirium on admission. Nonetheless, the existing literature suggests that similar factors predict both prevalent and incident delirium [44]. One study found that prevalent delirium on admission to an acute medicine ward was independently predicted by premorbid cognitive impairment, functional impairment and a high urea nitrogen level [30], not dissimilar to our findings.
The small sample size is another important limitation of our study. Of the 191 patients included in the analysis, 61 (31.9%) developed incident delirium. This is not reflective of a true incidence rate; however, as many initially included patients were excluded from analysis for various reasons as aforementioned, including discharge within 3 days (n = 88) and withdrawal (often with up to five assessments already performed, n = 36). If the denominator includes these patients (n = 315), the incidence of delirium in this cohort is approximately 19.4%, which concurs with the existing literature on the subject (although we cannot confirm the post-discharge delirium status of those patients discharged within one week). A systematic review of delirium epidemiology in medical inpatients [1] describes incidence rates varying between 3% and 29%, depending on the frequency of assessment. In studies reporting lower incidence rates (i.e., 3% to 11%), the frequency of assessment is either unclear or prompted by clinical need, or in one study performed every 48 h, whereas the majority of studies reporting higher incidence rates (12% – 29%) utilized at least daily delirium assessment. We did not investigate any of the in-hospital risk factors, as we were focusing on variables that are readily available at presentation to the ED; however, we appreciate that these additional factors play an important role in precipitating delirium. Our view is that those who are stratified as high risk at the hospital front door, should all then be commenced on a delirium care pathway aiming to minimize the in-hospital precipitants, especially older patients with pre-existing dementia, multiple comorbidities and/or functional impairment.
Incident delirium is a common problem in older medical inpatients. Our study indicates that those most at risk are those with premorbid dementia, baseline functional impairment and high levels of comorbidity. Dementia is a well-known risk factor for delirium, however patients often present to hospital without a prior known diagnosis of dementia [45]. Although a patient’s list of comorbidities is routinely recorded on admission, scoring co-morbidity burden using the M-CIRS may be too cumbersome for routine use in the ED. Baseline functional ability is also an important parameter to record in older patients on admission. The Barthel Index, a simple, commonly used measure of function, may be a useful tool to help identify those patients who are most vulnerable to the development of in-hospital delirium. Although this requires further study, considering patients with a BI of 16 or less as being at increased risk of developing in-hospital delirium, may assist with risk stratification. In busy and often under-resourced health services, risk stratifying older patients in this way may assist in targeting delirium screening and preventative strategies to those who are most at risk, making this important process more feasible for routine application in every day practice.