
Abstract
Background:
Delirium is a common geriatric syndrome, with a prevalence of between 15–70% among older long-term care residents. It is associated with adverse outcomes, and its onset may prove imperceptible to health professionals. Few studies in institutionalized older people have analyzed the predictors of delirium.
Objective:
The aim of the present study was to identify delirium predisposing and triggering factors, and develop a predictive model.
Methods:
A cohort trial-nested case-control study covering a period of 12 consecutive months (April 2015 – March 2016) was carried out. Predisposing and triggering episodes of delirium were recorded.
Results:
A total of 443 older persons were recruited, with a mean age of 85.73 (6.72) years and female predominance (78.3%; n = 374). The incidence of older people with delirium was 18.7% (n = 83). Dementia was the predisposing factor with the highest predictive capacity (OR = 2.74 [1.49–5.04]). In the presence of dementia, falls (OR = 2.45 [1.49–3.69]), neuroleptics (OR = 2.39 [1.23–4.65]) and anticholinergic drug use (OR = 1.87 [0.95–3.69]) were identified as triggering factors. The area under the curve (AUC) was 0.72 (95% CI: 0.66–0.78).
Conclusions:
Our findings suggest that interventions targeted to potentially preventable triggering factors could avoid the onset of delirium in older people with dementia. Knowledge of the predictive factors of delirium facilitates the screening of older people at increased risk, thereby allowing mental health service providers to prevent and identify the onset of a delirium episode. The decrease in delirium predictive factors should lead to a direct reduction in the occurrence of delirium and its consequences.
INTRODUCTION
Delirium is a neuropsychiatric syndrome frequently seen in acute disease, surgery, the hospital setting, and in institutionalized older people. It is characterized by an acute onset, fluctuating course, and alterations in consciousness, orientation, memory, thinking, perception, and behavior. The development of delirium is associated with adverse outcomes including a 62% increase in comorbidity and mortality, a 63% probability of developing dementia within 48 months of becoming delirious, and increased patient dependency and institutionalization. Since delirium is a preventable syndrome, these statistics are unacceptable [1–3]. Although there is consistent evidence on the impact of delirium, in daily clinical practice it is difficult to establish a diagnosis and treatment; as a result, delirium remains an underdiagnosed and undertreated neuropsychiatric syndrome [4]. The prevalence of delirium is between 15–70% among older long-term care residents, although the detection of hyperactive delirium is more frequent due to symptoms such as disorientation, irritability, psychomotor agitation, and visual hallucinations [5].
The underlying etiology can be divided into the presence of predisposing and triggering factors. Predisposing factors characterize people with greater vulnerability to delirium, while the presence of triggering factors subsequently establishes the syndrome [6]. Typical predisposing factors of delirium are old age (30.1%), cognitive decline (62.9%), disabilities (81%), sensory impairments (23%), environmental changes (50.1%), and multi-morbidity (48.6%) [7–9].
However, relatively few studies have systematically explored and reported triggering factors of delirium. It has been suggested that the most common triggering factors are acute conditions (e.g., stroke, infections, heart failure and cancer, or metabolic disorders such as hypoglycemia), the use of drugs such as hypnotics, sedatives, and anticholinergics, multiple drug prescription, iatrogenic complications, surgery, trauma, and uncontrolled pain. Older patients may have several triggering factors, and although only one triggering event is needed, several factors usually coexist [2, 9–12].
Delirium may be imperceptible to healthcare professionals. There are two major barriers to the detection of delirium: the lack of visibility of the condition and the misconception that delirium is benign and part of the aging process [13].
Delirium screening needs to be incorporated to daily patient assessment. It is the nursing staff who are able to detect cognitive changes in the patients, as they are the professionals that spend the most time with them. Since delirium is not recorded or identified as such in medical records, standardized documentation is essential to ensure accuracy and to avoid compromising patient care [14].
Predictive models are necessary to identify patients at risk. In this way it is possible to identify individuals who need close monitoring; eliminate or control the factors that predispose them to greater vulnerability; implement prevention strategies for prognostic decision making; and determine clinical trial eligibility. Adequate knowledge allows families to know the risk and to understand the disease process. It also makes it easier for health professionals to improve care. In this regard, the establishment of delirium is considered a benchmark for quality of care [15]
Predictive models in hospitalized older people have been widely studied, though few studies have been made in older people living in nursing homes [8, 17], where the consequences of delirium lead to increased consumption of nursing time and worsened functionality, cognitive status, and mortality.
The aim of the present study was to identify delirium predisposing and triggering factors in nursing home residents, and to develop a predictive model based on such factors.
METHODS
Study design and participants
A cohort trial-nested case-control study was carried out to establish a predictive model of delirium predisposing and triggering in older people (≥65 years of age) living in nursing homes. The study was conducted in 6 nursing homes in the province of Valencia (Spain).
The inclusion criteria were older people (≥65 years of age) living in the nursing home during the 12 months of follow-up of the study. The exclusion criteria were older people with only temporary residence (those who spent less than a year in the nursing home), end-of-life status (to avoid possible bias of the delirium episode in a state of agony), or individuals who spent more than two months out of the nursing home (due to hospital admission or temporary leave).
Data were collected from April 2015 to March 2016 by 5 nurses external to the nursing homes.
Sample size
The study comprised a total of 703 older people living in the nursing homes and with a prevalence of delirium of 60.1% in previous studies [16]. The sample size was calculated for an estimated relative risk of 2 with a 95% confidence level and a statistical power of 80%. To compensate for potential dropouts, an oversample of 5% was considered, bringing the final minimum sample to 438 subjects for follow-up.
Data collection
A comprehensive geriatric assessment was conducted to collect sociodemographic (age and sex), clinical (comorbidity), functional, psychological, and emotional variables from all the subjects meeting the inclusion criteria. The functional assessment tool used was the Barthel Index of activities of daily living (BI) [18]. Regarding psychological assessment, the Mini-Mental State Examination (MMSE) of Folstein [19] was used, while emotional evaluation was based on both the Yesavage Geriatric Depression Scale (GDS) [20] and the Cornell Scale [21]. The Mini-Nutritional Assessment (MNA) scale assessed nutrition. The screening phase consists of 6 items: a food intake item, two anthropometric parameters (recent weight loss and body mass index), and three general parameters (physical and emotional stress). The assessment phase had 12 items: anthropometric (calf and upper arm circumference), general lifestyle, medication, and mobility, dietary, and subjective assessment [22]. Based on the consulted literature, the following delirium predisposing factors were considered: age ≥89 years at the start of the data collection period, male sex, BI <60 points, MMSE <24 points, Cornell scale >8 points, Yesavage >5 points, and MNA ≤17 points. In addition, the diagnoses (previous or during the period of study) referred to dementia, depression, Parkinson’s disease, dysphagia, diabetes mellitus, visual impairment, hearing impairment, previous stroke, epilepsy, and comorbidity (presence of ≥4 chronic diseases) were recorded. Insufficient hydration assessed using a liquid consumption cut-off point of ≤550 ml over a period of 7 hours was documented from the medical records. Finally, a history of previous delirium was evaluated.
The following triggering factors were documented: the presence and intensity of pain as assessed by a visual analogue scale (VAS) and the Pain Assessment in Advanced Dementia (PAINAD) scale for patients with dementia (score ≥3) [23], anemia (hemoglobin <12 g/dl in males and <11.5 g/dl in females), renal failure and insufficient glomerular filtration (creatinine clearance <60 ml/min), autoimmune diseases, and incontinence (urinary or fecal). Data were also collected referred to pneumonia, hypoglycemia, urinary infection, and systemic (non-urinary) infections in the month preceding the delirium episode. The most common definition of polypharmacy is a numerical definition of 5 or more daily drugs, but ranges from two or more to 11 or more drugs [24]. More than 50% of the elderly people living in nursing homes take more than 9 drugs a day [25]; accordingly, following consensus by the research group, polypharmacy was defined as at least 7 drugs a day. Also, the prescription of anxiolytics, anticholinergic agents, antidepressants, and neuroleptic drugs during the data collection period were included. In addition, the presence of falls, the placement of a bladder catheter, and visits to the emergency department and hospital admissions were recorded. The number of predisposing and triggering factors was counted, as an increased number of risk factors elevated patient vulnerability [6].
Other triggering factors such as physical restrictions, mild stimulation, or an inadequate environment were not taken into account, given the personal care program implemented in the nursing homes. All information was collected from the electronic medical history of the patient.
The delirium indicator variable was established following the criteria of the Statistical Manual of Mental Disorders Fourth Edition (DMS-IV) and/or the Confusion Assessment Method (CAM) positive scores. The geriatrician makes the diagnosis following the DSM-IV: disturbance of consciousness (i.e., reduced clarity of awareness of the environment) with reduced ability to focus, sustain, or shift attention; a change in cognition (such as memory deficit, disorientation, language disturbance); or the development of a perceptual disturbance not better accounted for by a pre-existing, established, or evolving dementia. The disturbance develops over a short period of time (usually hours to days) and tends to fluctuate during the course of the day [26, 27]. The criteria are fluctuations in consciousness (changes in the perception of the environment. Different tools have been developed for the assessment of delirium by healthcare professionals other than psychiatrists or geriatricians [28]. So, the Confusion Assessment Method (CAM) scores were also the delirium indicator variable. The CAM scale is widely used as an instrument for the detection of delirium. Its sensitivity (94% to 100%) and specificity (90% to 95%) have been demonstrated compared to the diagnosis of the geriatrician [27]. The CAM evaluates four cognitive elements in the short form of the instrument: 1) acute onset and fluctuating course; 2) inattention; 3) disorganized thinking; and 4) altered level of consciousness [27]. To be diagnosed with delirium, a patient must demonstrate elements 1 and 2 as well as either element 3 or 4 [27].
Ethical considerations and data confidentiality
The study was approved by the Nursing Homes Medical Management and Ethics Committee of the Universidad Católica de Valencia “San Vicente Martir” (reference number: UCV/2015-2016/65).
The data obtained were kept confidential, in line with Spanish legislation on the protection of personal information (LOPD 15/1999 of 13 December 1999 and Law 14/2002 of 14 November 2002), with the designation of a sponsor code (2016/SLOPD/04) by the Universidad Católica de Valencia “San Vicente Martir”. The study was carried out in accordance with the principles of the Declaration of Helsinki.
Statistical analysis
The variables were reported as proportions and means and standard deviations. The Kolmogorov-Smirnov test was used to assess normality, and Levene’s test was applied to explore homogeneity of variances for continuous variables (age, BI, Tinetti scale, MMSE, Cornell scale, number of falls, daily prescribed drugs, emergency visits, and hospital admissions). There were no significant outliers. Parametric testing (Student t-test for unrelated samples) was used for the comparison of means, and nonparametric tests (chi-squared test) were used for the comparison of proportions.
We analyzed the association between delirium and the different risk factors (predisposing and triggering) based on the odds ratio (OR). A binary logistic backward stepwise regression model was developed to explore predisposing and triggering factors. We first considered the complete model with all predisposing and triggering factors found in the bivariate analysis to be significantly associated to the presence of delirium. We base this on the Wald test from logistic regression analysis and a p-value cut-off point of 0.25. More traditional levels such as 0.05 can fail in identifying variables known to be important [29, 30]. While in a second step, we eliminated from the model all those variables failing to produce an important change (defined as the absence of an adjusted effect of >10%), or which did not result in an improved standard error of the estimate on adjusting the model without such variables. Consensus was sought among the investigators in those cases where two or more subsets of variables with the same degree of fit were obtained. For more details on the selection process, see Hosmer and Lemeshow [31].
The study data were entered in MS Excel spreadsheets, followed by analysis using the SPSS® version 23.0 statistical package (IBM SPSS statistics).
We reported the study based on the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) statement [32].
RESULTS
Out of a total of 703 older people living in the nursing homes, 443 were included in the present study (Fig. 1). A female predominance was observed (78.3%). Comprehensive geriatric assessment showed the older subjects to present functional dependence (BI), cognitive impairment (MMSE), and depression (Yesavage and Cornell Scale) (Table 1).
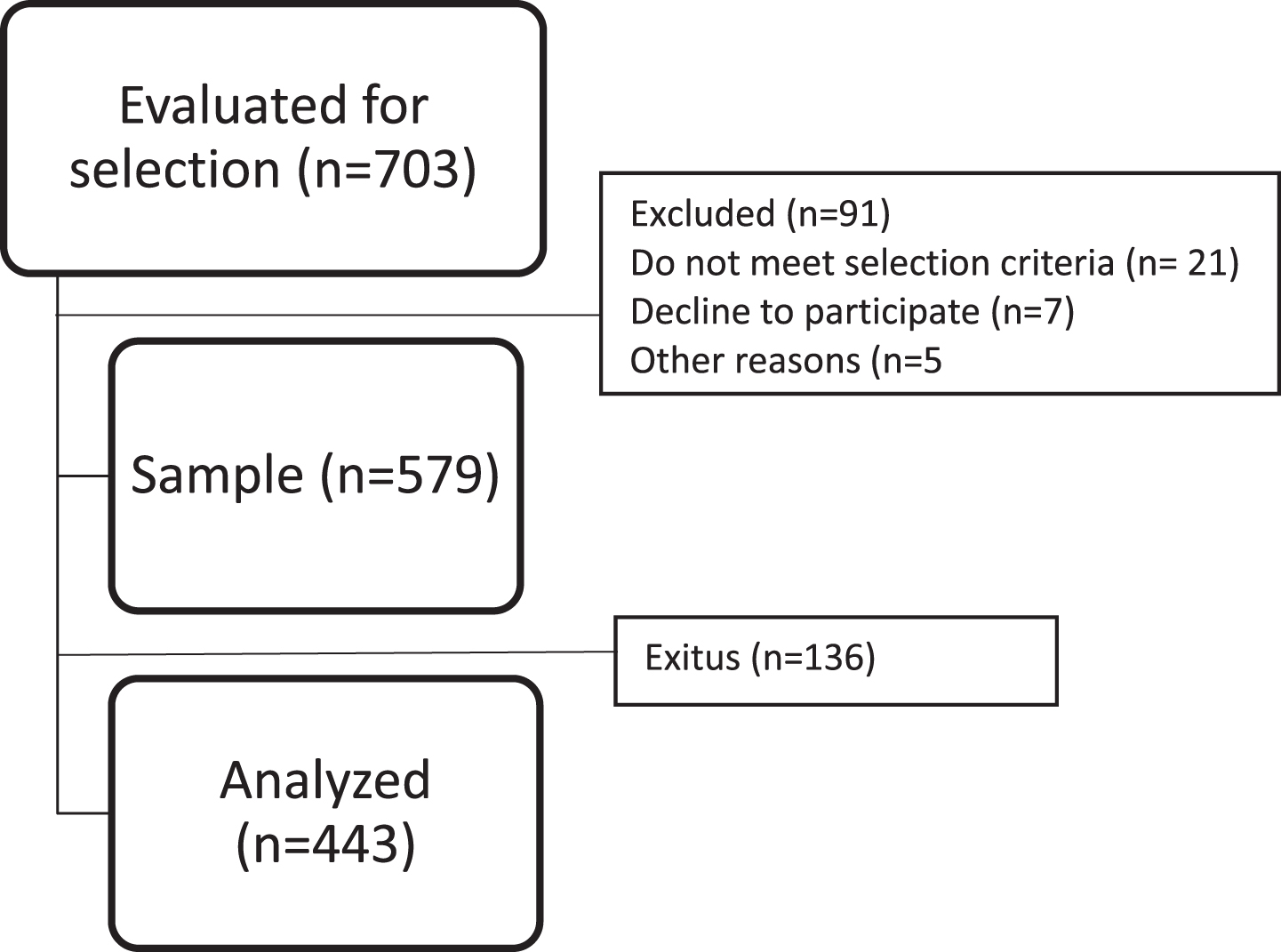
Study flow chart.
Characteristics of the study sample
Barthel Index, a basic activities of daily living rating scale, with scores between 0–100 (a score <60 indicating dependency); MNA, Mini-Nutritional Assessment scale, with scores from 0–30 (a score <17 points indicating malnutrition); MMSE, Mini-Mental State Examination, a cognitive impairment rating scale with scores between 0–30 (a score <24 indicating cognitive impairment); Cornell Scale, a depression rating scale in older people with dementia, with depressive symptoms being suggested by a total score of ≥8.
Eighty-three subjects (18.7%) presented delirium and of these, 22 (26.5%) suffered two or more episodes during the study period. A total of 121 episodes of delirium were recorded.
Of the 19 predisposing factors analyzed, only a Barthel score <60 points, dementia and dysphagia were seen to significantly increase the risk of delirium (Table 2). In turn, of the 19 triggering factors analyzed, anticholinergic drug use, neuroleptics, falls and incontinence were entered in the regression model (Table 3).
Delirium predisposing factors (odds ratios)
MMSE, Mini-Mental State Examination.
Delirium triggering factors (odds ratios)
Pain measured by a visual analogue scale (VAS) and the PAINAD scale for patients with dementia (a score ≥3 on both scales indicating pain). Anemia (hemoglobin <12 g/dl in males and <11.5 g/dl in females), insufficient glomerular filtration (creatinine clearance <60 ml/min).
Based on criteria described the Methods section, the following 6 variables were entered in the predisposing factors regression model: MMSE <24 points, BI <60 points, dysphagia, diabetes mellitus, insufficient hydration, and dementia. The triggering factors were taken into account following the same premises and included falls, urinary incontinence, anticholinergic agents and neuroleptic drugs, and emergency visits over 12 months.
A predisposing and triggering factors predictive model was generated. Dementia as a predisposing factor and anticholinergic and neuroleptic drugs and falls as predisposing factors were included in the final model (Table 4). The area under the curve (AUC) was 0.72 (95% CI: 0.66–0.78; p < 0.001) (Fig. 2). The model correctly classified 72.4% of the subjects.
Variables of the binary logistic regression analysis in older subjects
Nagelkerke R2 = 0.192; Specificity = 93.2%; Sensitivity = 25.7% (95% CI).
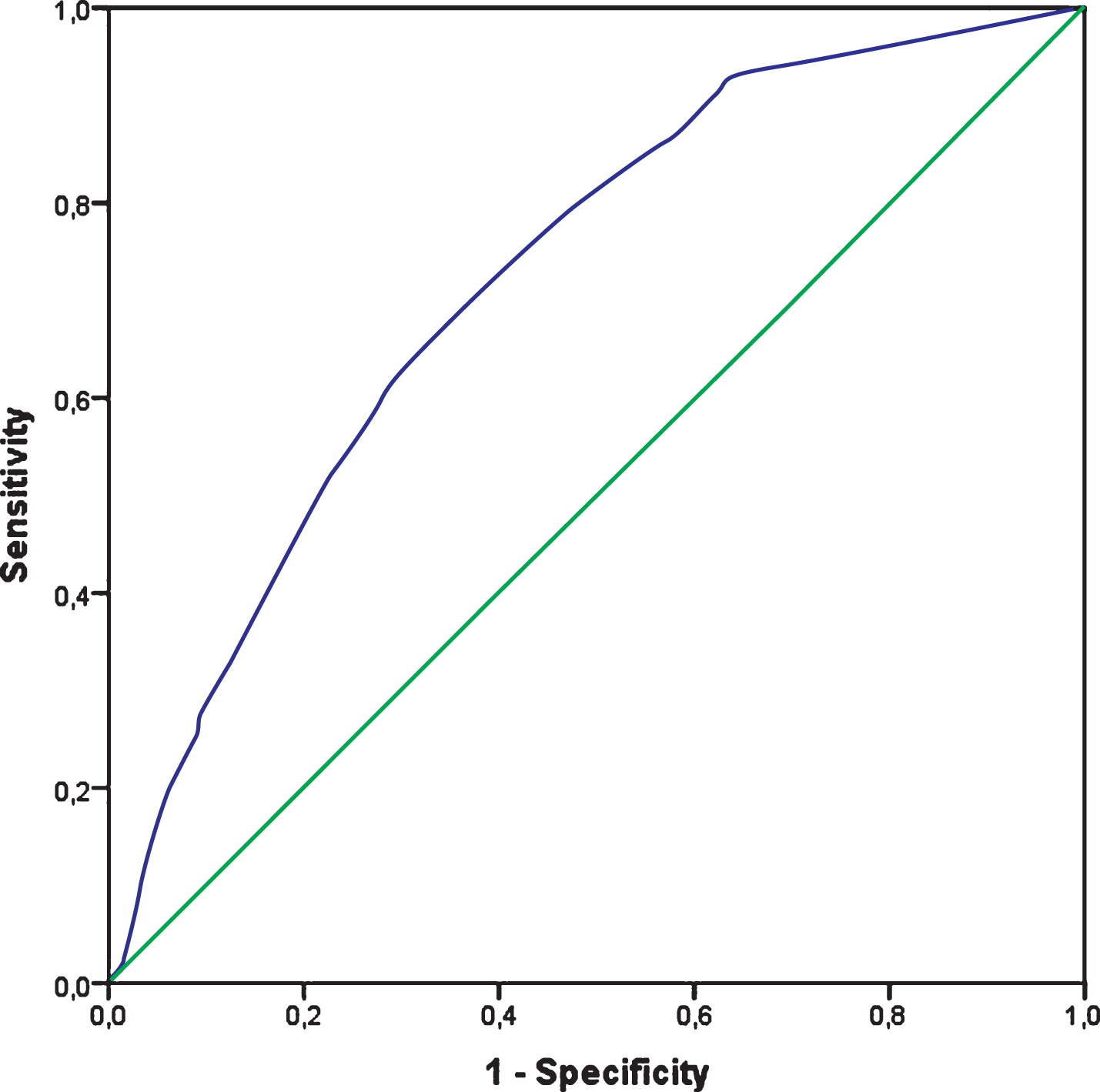
Receiver operating characteristic curve. Area under the curve = 0.72 (95% CI: 0.66–0.78; p < 0.001).
DISCUSSION
The aim of this study was to examine the triggering factors for delirium in institutionalized older individuals in the presence of predisposing factors. The results indicate that dementia is the predisposing factor with the greatest predictive capacity, while falls and neuroleptic drugs are the factors that predict a high probability of onset of a delirium episode.
The incidence of delirium in our study was lower than published elsewhere for institutionalized older people (20–40%) [4, 33–36]. The literature describes disparate incidences for delirium, and this may be due to the use of different assessment and screening scales, differences in the type of residence (nursing homes, long-term facilities, etc.), the prevalence of dementia, and differences in the applied inclusion and exclusion criteria, such as end-of-life status [9].
The analysis of the predisposing factors showed functional dependence to increase the risk of delirium in institutionalized older people, in coincidence with the observations of other authors [8]. Similarly, the presence of dysphagia was also identified as a risk factor, though few studies are available in this regard. Both functional dependence and dysphagia are severely debilitating for older adults [37].
Dementia was the predisposing factor with the highest predictive capacity for delirium, with higher figures than in other studies [38], where prevalences of 59–70% have been observed in long-term facilities. Most studies carried out in both hospitalized older and institutionalized older people have shown a strong association between dementia and delirium, and the higher the degree of dementia, the stronger the association [35]—the probability of delirium increasing by 45% in moderate dementias and 58% in severe dementias [39].
Although depression was a highly prevalent condition, it was not identified as a significant risk factor for delirium in our series, in contrast to the findings of other studies [40, 41]. Similarly, high prevalences of vision defects, comorbidity, and advanced age were not related to delirium. Older residents are assisted 24 hours a day by nursing staff, assistants, and a team of occupational therapists, physiotherapists, and psychologists. In addition, music therapy as well as relaxing or stimulating activities are provided by external staff, and this could reduce the impact of the aforementioned risk factors in comparison with the data found in the literature [3].
A relevant aspect in our study is that diabetes mellitus did not increase the risk of delirium, despite the fact that a number of authors [38, 42] indicate that glucose-related metabolic alterations are directly related to delirium. This could be due to the fact that the older people with diabetes are subjected to individual blood glucose monitoring during the day, and the resulting closer contact with the nursing staff could facilitate the avoidance of delirium before it becomes established [43].
No increased risk of delirium was noted in the presence of a greater number of risk factors [7, 44]. This could be explained by the protected environment of the nursing homes in which the study was carried out, where the integral care afforded may minimize the impact of different risk factors on the older subjects [36, 38].
The most significant triggering factors were urinary incontinence, emergency department visits, neuroleptics, anticholinergic drug use, and falls. The relationship between incontinence and delirium has been widely studied [8, 45]. Polypharmacy can cause delirium and consequently lead to incontinence. Urinary incontinence and bladder catheterization are also related to loss of function, increased risk of urinary tract infections, and the administration of a larger number of drugs—all of which poses an increased risk of delirium [45]. However, in contrast to previous studies [16], incontinence was not included in our predictive model. This is consistent with the need for prospective studies due to the lack of evidence to clarify what the risk factors and consequences are [46].
Similarly, emergency care visits modify the environment in which the patient lives on a daily basis. Transfer to the emergency room, stay, assessment, diagnostic tests, and acute disease conditions are clearly factors that contribute to disorientation and therefore to delirium [26].
Although several psychoactive drugs were analyzed, only anticholinergic agents and neuroleptics were seen to pose a greater risk than anxiolytics and antidepressants [47–50]; use of such drugs may be due to the fact that dementia was more prevalent in the cases than in the controls. Anticholinergic agents and neuroleptics may have been prescribed for the treatment of dementia and for the management of hyperactive or mixed delirium. There is currently no established causal relationship between the use of neuroleptics and delirium, but this is an aspect that should be considered in these patients, due to the mortality associated with the use of these drugs [4, 49].
The presence of falls was also a predictor of delirium, in coincidence with the data found in the literature [7]. The prevalence of falls in the institutionalized population is high, and its consequences are not only medical, but also functional and psychological. Functional dependence, possible fractures, pain, and fear after a fall are intimately related to the risk of delirium [17].
The presence of polypharmacy likewise did not increase the risk of delirium, and this could be a result of the drug suitability programs (STOPP/START criteria) run by geriatricians for more than 5 years [51, 52].
While risk factors for delirium in hospitalized older patients have been widely investigated [53], few predictive models are available in older people in nursing homes [16]. Most of the studies found in the literature refer to an increase in the number of risk factors and the consequent increase in the probability of delirium [17, 54].
Obtaining a predictive model in older people living in nursing homes makes it possible to detect those individuals at greatest risk, and therefore to adopt preventive actions [15]. The predisposing factor with the greatest predictive capacity was dementia. Dementia has a high prevalence in nursing homes. It leads to cognitive and behavioral disorders, and consequently there may be an underdiagnosis of delirium in patients with dementia. As a result, there is an increased risk of delirium onset, late diagnosis, and hence a poorer prognosis [55, 56]. The assessment scale chosen for delirium screening should be applied two or three times a day, and should be adapted to the characteristics of the target population. In this regard, in institutionalized older people, scales allowing the detection of delirium in older people with and without dementia are indicated [4]. In the presence of dementia, anticholinergic and neuroleptic drugs and falls were seen to be the predisposing factors. The use of antipsychotics for the prevention and treatment of delirium is the drug treatment of choice, but should always be combined with non-pharmacological treatment [57] in an attempt to avoid prolonged and unnecessary use of drug therapies that may have delirium-enhancing effects. Furthermore, there is literature questioning the evidence on the use of these drugs for the prevention and treatment of delirium [58].
Falls are also highly prevalent in the geriatric population, and even more so in institutionalized older people [59]. Falls generate increased dependence resulting from pain and fractures. Both of the latter are risk factors for delirium. Systematic screening of the risk of falls should be carried out in the older in order to minimize them [60] and thus lessen the risk of delirium in the presence of other non-modifiable risk factors (e.g., age, drug use, functional dependence).
In the context of nursing homes and long-term care facilities, nurses are the professionals that spend the most time with the older patients. Adequate communication between them and the interdisciplinary team providing comprehensive care is therefore essential. The identification of predisposing and triggering factors is crucial for the correct assessment of delirium [33].
Limitations
The main limitation of our study is the bias caused by possible failure to detect hypoactive or mixed delirium in patients with dementia. In addition, the study has been conducted in a group of nursing homes with similar operating protocols, and studies therefore should be conducted in different nursing homes in order to evaluate diverse environments that can minimize the risk of certain factors related to delirium.
Dementia and delirium are two associated geriatric syndromes, but it is difficult to correctly screen for delirium in these older people, due to the possible overlap of symptoms in mixed and hypoactive cases [55]. Older people with dementia sometimes retain basic care tasks as well as consciousness up until the advanced stages of the disorder [56, 60]. However, the literature that has shown that disorientation is more common in patients with delirium or delirium superimposed upon dementia than in those with dementia without delirium [61].
The clinical implications of our study are relevant, since the control of potentially preventable delirium-triggering factors could contribute to avoid the establishment of delirium in older people with dementia. Paying more attention to the existence of risk factors for falls and assessing the need for prescription of neuroleptics are the main elements in a prevention strategy. Patient monitoring by the health professionals would contribute to reduce the incidence of delirium and thus minimize the derived risks.
Conclusions
Knowledge of the principal predisposing and triggering factors for delirium would allow us to reduce or minimize them, and if this were not possible, systematic evaluation of the older individuals at increased risk would contribute to detect delirium in its early stages. The prevention or early treatment of delirium makes it possible to avoid the health and quality of life consequences of the disorder among nursing home residents.
Footnotes
ACKNOWLEDGMENTS
The authors wish to thank all the nursing homes group and PREMORE members for their contribution to making this study possible.
This study has received no financial support. The Government authorities, the Universidad Católica de Valencia “San Vicente Martir”, University of Valencia, Nursing homes group and Hospital Universitario de la Ribera had no role in the conduction of this study. None of the signing authors received specific funding for this study.