
Abstract
Background:
There is evidence that Alzheimer’s disease (AD) has significant cerebrovascular etiopathogenesis. Understanding potentially modifiable risk factors for vascular disease can help design long-term intervention strategies for controlling or preventing cognitive dysfunction attributable to cerebrovascular disease.
Objective:
To evaluate the presence and severity of markers of cerebrovascular pathology, its relationship to diagnostic categories of dementia, including AD, and association with the metabolic biomarker homocysteine.
Methods:
In a cross-sectional observational study, 340 community-dwelling elders received a clinical evaluation including brain MRI and neuropsychological tests. Dementia and mild cognitive impairment (MCI) were diagnosed by consensus committee. Fasting total plasma homocysteine was measured. Statistical analyses were adjusted for demographics and cerebrovascular risk factors.
Results:
Nearly 25% of those diagnosed with AD had small vessel infarcts (SVI). Periventricular white matter hyperintensity (pvWMHI) was prevalent in participants with AD (61%) or MCI (amnesic 61% and non-amnesic 54%, respectively). Participants with SVI and/or pvWMHI also had greater brain atrophy. Homocysteine concentrations were higher in individuals with cerebrovascular findings than in those without. In individuals with cerebrovascular disease, homocysteine was inversely related to executive function (p = 0.022) and directly related to degree of brain atrophy (p = 0.009).
Conclusions:
We demonstrated a significant prevalence of small vessel markers of cerebrovascular pathology in individuals diagnosed with AD, with a significant concurrence between cerebrovascular disease and brain and ventricular atrophy. While current research on AD has focused on amyloid-βpeptide deposition, tau-pathology, and microglial activation and inflammation, greater attention to the cerebrovascular contribution to this neurodegenerative disease presents an additional target for therapeutic prevention and intervention.
Keywords
INTRODUCTION
When Alzheimer’s disease (AD) was widely adopted as the designation for most of ‘senile dementia’ 70 years after Alois Alzheimer’s 1907 postmortem description, attendant vascular pathology emphasized in other cases [1] were relegated to the designation of vascular dementia. Data from more recent clinical research, however, suggest an overlap between AD and cerebrovascular disease [2 –4], and give evidence that cerebrovascular disease is a determinant of the presence and severity of clinical symptoms in individuals with early AD pathology [5, 6]. There is evidence that small vessel disease is the most common cause of vascular cognitive impairment [7], particularly executive function, the cognitive domain that includes planning and cognitive flexibility [8]. The presence of silent and small vessel brain infarcts on magnetic resonance imaging (MRI) increases the risk of dementia and predicts a steeper decline in cognitive function [9]. White matter hyperintensities (WMHI), which may reflect small vessel disease with/or a disruption of myelin [10], have been shown to be associated with cognitive impairment [7] and gait disturbances [11]. Better understanding of potentially modifiable risk factors for vascular disease can aid in developing long-term intervention strategies for controlling or preventing the cognitive dysfunction attributable to cerebrovascular disease [12].
One potential target, the biomarker plasma homocysteine, reflects the functional status of three B vitamins: B12, B6, and folate. Mild to moderate elevation of plasma homocysteine concentration has been implicated as a risk factor for cardiovascular disease [13], stroke [14, 15], cognitive impairment (particularly executive dysfunction) [16, 17], and dementia [18]. Homocysteine is a sulfur amino acid whose metabolism stands at the intersection of two pathways: remethylation to methionine, which requires folate and vitamin B12 (or betaine in an alternative reaction); and transsulfuration to cystathionine, which requires pyridoxal-5–phosphate (vitamin B6). Elevated plasma homocysteine concentrations, or hyperhomocysteinemia, results with a disruption in either one of these metabolic pathways. Homocysteine lowering has been shown to have a beneficial effect on cognition in community dwelling elders [19], mild cognitive impairment (MCI) [20, 21], kidney transplant [22], and patients with mild, and presumably early, AD, but not in moderately advanced AD [23]. A recent consensus statement supports elevated homocysteine as a risk factor for dementia [24]. When improved cognitive function is observed in response to nutritional interventions and homocysteine lowering, executive function appears to be the most responsive element of multiple measures of cognitive function [22]. These results emphasize the importance of examining the vascular components of cognitive decline and of identifying subsets of the population that may benefit from intervention focused on slowing progression of vascular pathology and clinical symptom severity. The purpose of the present study was to evaluate the presence and severity of cerebrovascular pathology on MRI in older, community-dwelling adults, its relationship to diagnostic categories of dementia, including Alzheimer-type, MCI, and association with the metabolic biomarker homocysteine.
METHODS
Study population
This study involved a subset of the Nutrition, Aging, and Memory in Elders (NAME) cohort who had undergone MRI, cognitive testing, and had fasting blood samples (n = 340). The NAME study’s design, subject recruitment, and data collection methodology has been previously described in detail [25]. Briefly, the NAME study was a cross-sectional study designed to identify relationships between micronutrient status, and cognitive capacity and cerebrovascular pathology in older adults. The study cohort consisted of community-based elders living in the greater Boston, Massachusetts area age 60 years and older. Subjects were visited in their homes by trained research staff who administered a neuropsychological testing battery. Fasting blood samples and a range of health and behavior questionnaires and anthropometric and blood pressure measures were obtained in the participants’ homes by trained research staff. MRI was done at Tufts Medical Center in Boston, Massachusetts. The study was approved by the Tufts University Health Sciences Campus Institutional Review Board.
Consensus diagnosis
Clinical diagnoses were made during consensus meetings attended by a psychiatrist, neuropsychologist, neurologist, and neuroradiologist. The NINCDS-ADRDA criteria [26] were used for the diagnosis of possible or probable AD, and the NINDS-AIREN criteria [27] were used for the diagnosis of possible or probable vascular dementia. Amnesic MCI (aMCI) and non-amnesic MCI (naMCI, either multiple domain or single domain, primarily executive function) were diagnosed according criteria described by Petersen et al. [28, 29].
Blood sampling and laboratory methods
A fasting blood sample was obtained during a home visit, immediately aliquoted, centrifuged, and transported to the laboratory on ice. Plasma total homocysteine was measured by high pressure liquid chromatography (Waters Corporation, Milford, MA) using fluorescence detection (Perkin Elmer, Waltham, MA) according to the procedure of Araki et al. [30]. Plasma folate and vitamin B12 concentrations were measured with the use of the Quantaphase II radioassay kit (Bio-Rad Laboratories). Serum creatinine was measured by a kinetic modification of the Jaffe procedure [31] on a clinical chemistry analyzer, Olympus AU400 (Olympus America Inc., Melville, NY), as modified by Cook [32] using Olympus America calibrator and reagent (traceable to isotope dilution mass spectrometry) and according to protocol (calibration method standardized as recommended by the national Kidney Disease Education Program). The genetic status of apolipoprotein E (ApoE) alleles was characterized using polymerase chain reaction, and individuals either heterozygous or homozygous for the 4-allele were defined as a carrier of the ApoE4 allele.
Cardiovascular risk factors
Classification of diabetes was made according to the guidelines from the American Diabetes Association (fasting plasma glucose of >126 mg/dl, or are using prescribed oral medication for diabetes or insulin). Hypertension (based on the average of two blood pressure measurements) was defined as ≥140 or 90 mmHG for systolic or diastolic blood pressure, respectively.
Magnetic resonance imaging
Images were obtained on a 1.5T Symphony Siemens’ scanner. Series included intermediate and T1-weighted axial images, T2-weighted conventional spin-echo axial images, Fluid Attenuation Inversion Recovery Turbo SE axial images, and T1-weighted Magnetization Prepared Rapid Acquisition Gradient Echo coronal images. A board-certified neuroradiologist, blinded to other data, assessed the images for small and large vessel infarcts, WMHI severity and location, and oversaw brain, ventricular, and intra-cranial volume measurements [33, 34].
Brain infarcts
Brain infarcts were identified and measured by a neuroradiologist to quantify subclinical and clinical cerebrovascular disease. Large vessel infarcts (LVI) were defined as cortical infarcts of any size and subcortical infarcts >1.5 cm in maximum dimension, whereas small vessel infarcts (SVI) were defined as subcortical infarcts 3 mm to 1.5 cm. To qualify for an infarct, the lesion had increased signal on T2 and FLAIR images. For subcortical infarcts in white matter, additional low signal on T1-weighted images was required to be considered as infarct [35].
WMHI
Grading of WMHI was done on a scale of 0 to 9 (higher numbers indicating greater severity) [33], and were identified as periventricular (pvWMHI, within 1 cm adjacent to the lateral ventricular margin) and/or subcortical (scWMHI, lesions not adjacent to the lateral ventrical).
Brain, ventricular, and intra-cranial volume measurements
Analyze image analysis software (Biomedical Imaging Resource, 1986–2006) was used for region of interest analysis and brain segmentation. Quantitative segmentation of CSF from brain was performed using the method described by deCarli et al. [34]. Brain and ventricular volumes were corrected for intracranial volume. Brain atrophy was also graded on a scale of 0 to 9 (higher numbers indicating a greater degree of atrophy) [36].
Cognitive testing
The Mini-Mental State Examination (MMSE) [37] and the North American Adult Reading Test (NAART) [38] were administered as screening tools, and as estimates of global cognitive function and premorbid verbal intelligence. Participants with a MMSE score ≤10, or NAART derived estimated verbal IQ <75, were excluded from participation to prevent floor effects. The neuropsychological test battery, which has been previously described in detail [25], was administered at home by trained research assistants. It was designed to assess multiple cognitive domains and included WMS-III Word List Learning and Logical Memory subtests [39], WAIS-III Digit Span, Digit Symbol Coding, Block Design and Matrix Reasoning subtests [40], Mental Alternations [41], Trail Making Tests A and B [42], and Controlled Oral Word Association [43]. Principal components analysis of the cognitive tests was used to derive composite scores for use in subsequent data analyses. The analysis of cognitive factors was completed with an orthogonal rotational procedure (varimax). The adequacy of the correlation was assessed with Bartlett’s test and Kaiser – Meyer – Olkin measure. Factors with eigenvalues >1.0 were selected, and factor loadings were defined by items with factor loading scores> |0.4|. PCA revealed three distinct factors related to memory, executive function, and attention/processing speed (Supplementary Table 1). The resulting composite scores for these three cognitive domains were used in statistical analyses, with means = 0 and standard deviations (SD) = 1.
Description of total study participants
s.d., standard deviation.
Statistical analysis
All data were analyzed using SPSS version 22.0 (IBM SPSS Inc, Chicago, IL). Prevalence of neuroimaging markers of cerebrovascular disease was established and the relationship between LVI, SVI, and WMHI was tested using Pearson chi-square and logistic regression. Demographics and cardiovascular risk factors were compared between participants who had radiological evidence of infarct or WMHI and those without cerebrovascular disease findings using Pearson chi-square for nominal data and analysis of variance (ANOVA) for continuous variables. Pearson chi-square was used to evaluate the relationship of cerebrovascular variables and ApoE4 allele status with dementia diagnosis. Analysis of covariance (ANCOVA) was used to assess the relationship between cerebrovascular variables and brain atrophy, neuroimaging markers and cognition. ANCOVA was also used to assess the relationship between homocysteine, folate and vitamin B12 concentration quintiles, ApoE4 allele status, and cognitive function. Analyses involving cognition utilized the cognitive composite scores described above.
Covariates
Unless otherwise indicated, all parametric analyses were adjusted for age, sex, education level, race (black/not black), diabetes, hypertension, and serum creatinine level.
RESULTS
Population characteristics
Demographics and other cohort characteristics of the participants included in our analyses are presented in Table 1. The mean age was 73 (±8.3) years, and the participants were predominantly female (73%). Attained level of education was moderate, with 30% high school graduates and 44% having attended at least some college. The mean BMI was in the obese range (30.8 + 7.9 kg/m2) with a high prevalence of hypertension (84%) and diabetes (31%). Mean plasma homocysteine concentration was 11.9μmoles/L. Cut-offs for plasma homocysteine quintiles were 8.0, 9.9, 11.9, and 14.9μmoles/L. Approximately 48% had elevated homocysteine concentrations, as defined as ≥10μmoles/L in women, and ≥11μmoles/L in men.
Prevalence of cerebrovascular disease on MRI
Table 2 compares the demographic and cardiovascular risk factors for individuals with and without neuroimaging evidence of cerebrovascular pathology. In general, those with any cerebrovascular disease were older and more likely to be male than those without. Individuals with SVI were more likely than those without to have concomitant pvWMHI (OR 3.22, 95% CI 1.69–6.13). There was no statistically significant association between pvWMHI and LVI (OR 1.46, 95% CI 0.66–3.24). There was no association between scWMHI and SVI or LVI.
Cerebrovascular MRI findings and participant characteristics
Subgroups include all participants with the stated cerebrovascular finding; subgroups are not mutually exclusive. Comparison between those participants with no cerebrovascular findings versus cerebrovascular subgroups, ∧ p < 0.10; * p < 0.05; ** p < 0.01; *** p < 0.001; Race is presented as Black versus not Black; Estimated Verbal IQ, North American Adult Reading Test [38]; MMSE, Mini-Mental State Exam [37]; BMI, body mass index; all reported values are either percentage (%) or mean (standard deviation).
Cerebrovascular disease, dementia diagnosis, and brain atrophy
Table 3 shows the proportion of study participants who have cerebrovascular pathology, stratified by consensus diagnoses of AD, vascular dementia, aMCI, naMCI, or none. Close to 25% of those with the consensus diagnosis of possible or probable AD had SVI, while 0% of those with aMCI did. PvWMHI were common in those participants diagnosed with AD (61%), or with either a- or naMCI (61% and 54%, respectively). By definition, those with clinically diagnosed possible or probable vascular dementia commonly had SVI (54%), LVI (33%), and pvWMHI (83%) as compared to those without a diagnosis of dementia or cognitive impairment.
The proportion of study participants with cerebrovascular pathology, stratified by consensus diagnosis
Each subscript letter denotes consensus diagnoses with cerebrovascular pathology subtype proportions not significantly different from each other at the p < 0.05 level (e.g., within a row, all “a” subscripts are not statistically different, and all “b” subscripts are not significantly different). WMHI, white matter hyperintensity.
An ANCOVA indicated that those individuals with SVI and/or pvWMHI had larger ventricle/ ICV ratios (p < 0.01 and p < 0.10, respectively), and a smaller brain/ICV ratios (p < 0.05 and p < 0.10, respectively) than did those individuals without cerebrovascular findings. Individuals with LVI also had smaller brain/ICF ratios than did those without cerebrovascular findings (p < 0.01). The brain/ICV or ventricle/ICV ratios in individuals with scWMHI did not significantly differ from those individuals without cerebrovascular MRI findings (Table 4).
Ratios of brain and ventricular volumes to ICV, by MRI cerebrovascular finding category
Data are presented as unadjusted means with standard deviations. Statistical significance was determined using ANCOVA, adjusted for age, sex, education level, race (black/not black), diabetes, hypertension and serum creatinine concentration. ICV, intracranial volume. All reported values are mean (standard deviation); ∧ p < 0.10, * p < 0.05, ** p < 0.01 compared to those with no cerebrovascular findings.
Cerebrovascular pathology and cognition
Presence of pvWMHI was associated with lower executive function scores (mean difference = 0.285 SD, SE±0.105; P = 0.007); scWMHI was not associated with cognitive function in this study population. These relationships with cognition did not change after further adjustment for brain volume or for presence of LVI or SVI. The presence of SVI was significantly associated with lower memory scores (mean difference = 0.268 SD, SE±0.132; p = 0.042), and with trends for lower executive function and attention (mean differences of 0.239 and 0.256 SD, respectively, p < 0.10). The presence of LVI on MRI was associated with lower executive function (mean difference = 0.531 SD, SE±0.168; p = 0.002) and better memory (mean difference = 0.350 SD, SE±0.169; p = 0.040) scores.
Cerebrovascular pathology and homocysteine
Homocysteine concentrations were higher in those individuals with SVI (13.7μmoles/L, SD±7.3; p = 0.007), LVI (12.8μmoles/L, SD±5.4; p = 0.043), and pvWMHI (12.8μmoles/L, SD±7.4; p = 0.040) than in those without cerebrovascular findings (10.6μmoles/L, SD±4.4) (Table 2). No differences in mean homocysteine concentrations were found between people with scWMHI and those without cerebrovascular findings (11.37μmoles/L, SD±4.98; p = 0.315). The relationships between SVI, pvWMHI, and homocysteine remained significant after adjusting for demographics and cardiovascular risk (p = 0.024 and p = 0.021, respectively). Severity of brain atrophy was related to plasma homocysteine concentration (by quintiles) in individuals with cerebrovascular disease (presence of SVI, LVI, or pvWMHI) after adjustment for demographic and cerebrovascular risk factors (trend p = 0.009). This relationship was not found in those individuals without cerebrovascular disease (Fig. 1). Homocysteine was not related to hippocampal atrophy in either the whole study population or other subgroups. Plasma homocysteine quintiles had the following concentration ranges: quintile 1 = 3.60–8.00μmoles/L; quintile 2 = 8.10–9.90μmoles/L; quintile 3 = 10.00–11.90μmoles/L; quintile 4 = 12.00–14.90μmoles/L; quintile 5 = 15.00–71.20. Additional adjustment for vitamin B12, folate, or ApoE4 allele status did not attenuate the relationship between homocysteine and brain atrophy, WMHI, SVI, or LVI. There were no differences in folate, vitamin B12 concentrations, or ApoE4 allele status in those with and without cerebrovascular findings, and no relationship between folate, vitamin B12, or ApoE4 allele status and brain atrophy (data not shown).
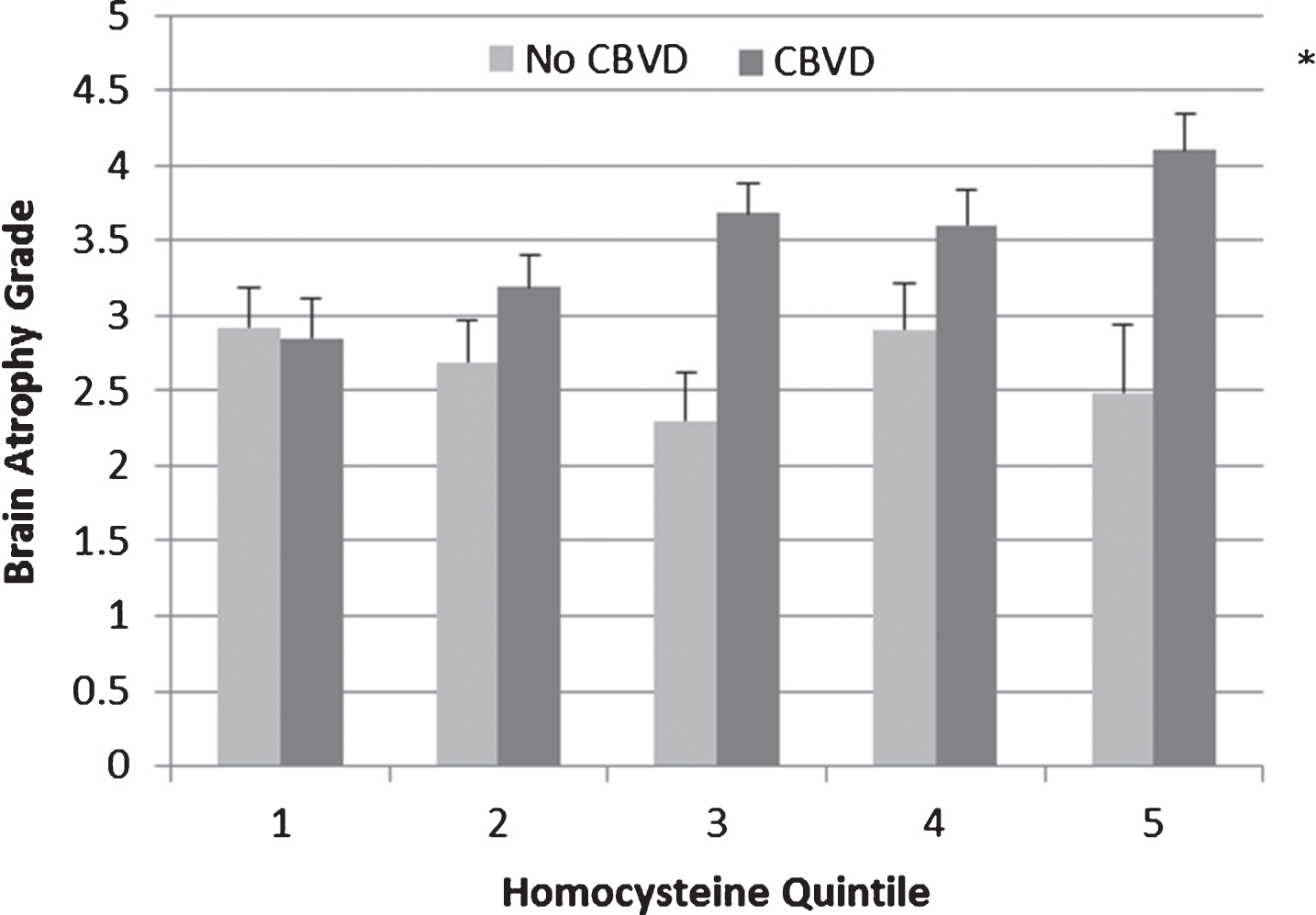
Brain atrophy grade by homocysteine quintile in the presence and absence of cerebrovascular disease. Brain atrophy grade 0–9 (higher grade indicates more severe atrophy), reported are adjusted estimated marginal means with standard error; CBVD, cerebrovascular disease (the presence of small vessel infarcts, large vessel infarcts, or periventricular white matter hyperintensities); trend for brain atrophy grade by homocysteine quintile in cerebrovascular disease present group, p = 0.009; adjusted for age, sex, education, race (black/not black), diabetes and hypertension diagnosis, and serum creatinine concentration. Plasma homocysteine quintiles had the following concentration ranges: quintile 1 = 3.60 – 8.00μmoles/L; quintile 2 = 8.10–9.90μmoles/L; quintile 3 = 10.00–11.90μmoles/L; quintile 4 = 12.00–14.90μmoles/L; quintile 5 = 15.00–71.20; * p < 0.05, compared to first quintile.
Homocysteine and cognition
The relationship between plasma homocysteine concentration and cognitive function was different in participants with and without cerebrovascular disease. In those individuals with cerebrovascular disease (presence of SVI, LVI, or pvWMHI), plasma homocysteine quintile was inversely related to executive function after adjustment for demographic and cerebrovascular risk factors (trend p = 0.022, Fig. 2). This relationship was not seen in those individuals without cerebrovascular disease. Plasma homocysteine concentration was not related to either memory or attention composite scores in participants either with or without cerebrovascular disease. Adjustment for vitamin B12, folate, or ApoE4 allele status did not attenuate the relationship between homocysteine and executive function. Neither vitamin B12, folate, nor ApoE4 allele status were associated with measures of cognitive function or dementia diagnosis (data not shown).

Cognitive executive function component score by homocysteine quintile in the presence and absence of cerebrovascular disease. Executive function composite score (adjusted estimated marginal mean with standard error); CBVD, cerebrovascular disease (the presence of small vessel infarcts, large vessel infarcts, or periventricular white matter hyperintensities); trend for executive score by homocysteine quintile in CBVD present group, p = 0.022; adjusted for age, sex, education, race (black/not black), diabetes and hypertension diagnosis, and serum creatinine concentration. Plasma homocysteine quintiles had the following concentration ranges: quintile 1 = 3.60–8.00μmoles/L; quintile 2 = 8.10–9.90μmoles/L; quintile 3 = 10.00–11.90μmoles/L; quintile 4 = 12.00–14.90μmoles/L; quintile 5 = 15.00–71.20; * p < 0.05, ** p = 0.003 compared to the first quintile.
DISCUSSION
Elders at high risk for cognitive decline also carry risk factors for vascular and cerebrovascular disease [44, 45]. Since cerebral hypoperfusion and microvascular abnormalities precede cognitive and neurodegenerative changes, we and others [3] have argued that cerebrovascular pathology is important in the etiopathogenesis of age-related cognitive decline, dementia, and perhaps AD. In this analysis of community dwelling elders in the Boston NAME study, we found a high prevalence of neuroimaging markers of cerebrovascular disease in study subjects with brain atrophy, cognitive impairment and dementia diagnosis. Our results are consistent with findings from the Rotterdam Scan Study, that showed a relationship between pvWMHI and risk of dementia, including AD, and brain atrophy [46].
Studies have found that elevated homocysteine is a risk factor for AD [18]; in this context, it is instructive that we found that homocysteine was related to cognitive function and brain atrophy only in those individuals with neuroimaging markers of cerebrovascular disease. This finding supports the hypothesis that homocysteine is a biomarker for cognitive impairment related to cerebrovascular disease, especially SVI, although others have also found a direct relationship with neurofibrillary tangles [47] and an additional mechanism of neurodegeneration may be through direct neurotoxic effects [48]. That homocysteine was associated with executive dysfunction, but not memory impairment, provides further evidence for the vascular interpretation. The difference in executive function between the 1st and 5th quartiles of this group was functionally meaningful with over 0.80 of a standard deviation difference in executive composite scores. These results are similar to our previous finding that microalbuminuria, an early indicator of endothelial damage, was associated with executive cognitive impairment and increased WMHI in NAME study participants [49]. Unlike de Lau et al. [50], we did not find a relationship between vitamin B12 and WMHI, although this may be because we used plasma vitamin B12 to assess status rather than a more sensitive measure such as holotranscobalamin.
Our study is limited by its cross-sectional design and the number of participants with cerebral infarcts. However, the results of our study complement and affirm previous findings that cerebrovascular and neurodegenerative pathology highly coexist in dementia, even in Alzheimer-type dementia [3]. The relative contribution of SVD to cognitive impairment in AD, however, may depend on the severity and stage of AD pathology. Neuropathological examination of decedents from the OPTIMA cohort who had cognitive evaluations within two-years of death found that greater SVD was related to mild to moderate cognitive impairment in those individuals without AD [51] and in those with early stage AD [6], but had no association with the degree of cognitive impairment in those with later stages of AD [6, 52].
While current research on AD has focused on amyloid-β peptide deposition, tau-pathology, cell death of cholinergic neurons, and microglial activation and inflammation, attention to small vessel cerebrovascular contribution to the etiopathogenesis of AD may present an additional target for therapeutic intervention and potentially slow associated cognitive decline in early stages of the disease.
Footnotes
ACKNOWLEDGMENTS
Supported by the USDA (agreement 58-1950-0-014), the National Institute on Aging (R01AG21790-01), and General Clinical Research Center funded by the National Center for Research Resources of the NIH, MO1-RR00054. The sponsors had no role in the design and conduct of the study; in the collection, analysis, and interpretation of data; in the preparation of the manuscript; or in the review or approval of the manuscript. We thank Gayle Petty and the Nutrition Evaluation laboratory at the Jean Mayer USDA Human Nutrition Research Center on Aging at Tufts University for analytical contributions.