
Abstract
Background:
Time trends for dementia prevalence and incidence rates have been reported over the past seven decades in different countries and some have reported a decline.
Objective:
To undertake a systematic review to critically appraise and provide an evidence-based summary of the magnitude and direction of the global changes in dementia prevalence and incidence across time.
Methods:
Medline, EMBASE, and PsychINFO were searched for studies focused on secular trends in dementia prevalence and/or incidence until 18 December 2017. In total, 10,992 articles were identified and 43 retained.
Results:
Overall, prevalence rates are largely increasing (evidence primarily from record-based surveys and cohort studies in Japan, Canada, and France) or have remained stable (evidence primarily from cohort studies in Sweden, Spain and China). A significant decline in prevalence has however been reported in more recent studies (i.e., from 2010 onwards) from Europe (e.g., UK and Sweden) and the USA. Incidence rates have generally remained stable or decreased in China, Canada, France, Germany, Denmark, Sweden, the Netherlands, UK, and USA. An increase has only been reported in five countries: Italy, Japan, Wales, Germany, and the Netherlands. Only one study reported findings (stability in incidence) from a low and middle-income country using data from Nigeria.
Conclusions:
The evidence on secular trends in the prevalence and incidence of dementia is mixed including contradictory findings using different (and in some cases the same) datasets in some countries (e.g., the USA, UK, and Sweden). This making it difficult to draw concrete conclusions. However, declining trends recently observed in some high-income Western countries in the most recent two decades including the UK, USA, and Sweden are encouraging. Updated dementia prevalence and incidence estimates will inform public health and financial planning as well as development of prevention strategies.
INTRODUCTION
Dementia is a global health concern. In 2015, it was estimated that there were 47 million people with dementia worldwide, and this number is predicted to increase to 75 million by 2030 [1]. However, recent evidence suggests, at least in some countries, that the risk of dementia is changing and even declining [2–5]. Population-level public health strategies and improved clinical management of key modifiable risk factors such as smoking, low educational attainment and cardiovascular disease are putative drivers of the declining trends.
However, not all studies have reported declining (or stable) trends in dementia prevalence or incidence rates. Heterogeneous findings may be due to differences in study methodology (e.g., time periods investigated, changes in dementia diagnostic criteria over time) as well as economic transitions resulting in changes in population health status (e.g., increasing obesity rates), improved risk factor management (e.g., hypertension), differences in survival (e.g., from stroke and with dementia), improved public health and awareness of dementia, or higher educational attainment (e.g., cognitive reserve). Knowing changes in population risk of dementia has implications for calculating future projections used for anticipating health care needs, estimating costs, and budgeting resources. Current estimates are usually based on the assumption that dementia prevalence and incidence rates are stable over time and, in light of recent findings, calculations using this method may be incorrect [6].
We therefore sought to determine whether rates of dementia have changed over time by conducting a systematic review of studies which have investigated historical or recent secular trends in dementia prevalence or incidence rates.
METHODS
Search strategy
This systematic review was conducted adhering to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses: PRISMA guidelines [7]. Embase, Medline, and PsychINFO were searched with the terms “dementia”, “epidemiology”, “prevalence”, and “incidence” (see Supplementary Material 1). All languages and dementia sub-types were included. The initial search was conducted on the 27 January 2015. Updated searches were run from January 2015 to 22 July 2016 and again from 22 July 2016 to 18 December 2017.
Inclusion/exclusion criteria
All population-based studies reporting dementia prevalence or incidence rates, across similarpopulations separated by time were eligible for inclusion. No restriction was applied to the setting from which the cohorts were derived (e.g., community, care home, or residential home) provided that comparison was being made between cohorts from similar backgrounds (e.g., location, socio-demographic status). Studies were required to have based their diagnosis of dementia or its subtypes on validated criteria (e.g., Geriatric Mental State Examination, Diagnostic and Statistical Manual of Mental Disorders (DSM), or International Classification of Diseases criteria). Other methods for the diagnostic assessment of dementia such as the use of cognitive test scores (e.g., Clinical Dementia Rating (CDR) Scale or Mini Mental State Examination (MMSE)) or via record review, were also allowed provided the study had evidenced the presence of standardization in their choice. Exclusion criteria included: 1) studies where dementia prevalence and/or incidence were reported in a single cohort only, with no time trends; and 2) studies where the sample was restricted to participants aged ≤60 years in order to focus on late-life rather than early onset dementia which is relatively rare, often has a different presentation, and has, in some cases, been associated with genetic abnormalities [8]. Studies were not excluded if the diagnostic criteria for dementia changed across time; the limitations of such studies will be discussed separately.
Data analysis
Three investigators (EYHT, MS, RB) independently searched publications for inclusion. Titles and abstracts were searched first, followed by the full text of identified articles. Reviews were also retained and the reference lists of these and each included paper interrogated. Where multiple publications using the same study were identified, these were retained for full text review. Disagreements were resolved by consensus or discussion with a third investigator (BCMS or LR). Data were independently abstracted by three investigators (EYHT, RB, TDC) and checked by a third (BCMS). Due to considerable methodological variation, no meta-analysis was performed. Instead, figures were produced to show the time trends in dementia prevalence and incidence reported across the studies based on statistical significance of the results. Also, see Supplementary Material 2 for the reported rates over time and statistical results where trends have been tested.
Role of the funding source
Preparation of the results for publication was completed as part of the NIHR Global Group: DePEC (Grant number: 16/137/62). BCMS has full access to the data and had final responsibility to submit for publication.
RESULTS
As shown in Fig. 1, the electronic search returned 15,126 articles, of which 10,992 were retained after removing duplicates. Following the title/abstract search, 90 articles were selected for full text review. Of these, six presented data from the Rochester Epidemiology Project (Minnesota, USA) [9–14], six presented data from the Japanese Hisayama Study [15–20], three presented data from the National Long-Term Care Survey (NLTCS, USA) [21–23], and two presented data from Daisen-cho (Japan) [24, 25]. Of the six Rochester articles, one presented unique findings on prevalence [9] and the other on incidence [14] and both were retained. Of the six Hisayama Study articles, three reported time trends in prevalence: one [17] over seven years follow-up (1985 versus 1992), one [18] over 20 years follow-up (1985, 1992, 1998, and 2005), and one [19] over 29 years follow-up but only using the neuropathology data. The most recent paper [20] reported time trends in prevalence (1985, 1992, 1998, 2005, and 2012) and incidence (1998 versus 2002 cohorts) and was retained. Two articles utilizing data from the NLTCS were retained as they covered unique time periods [21, 23]. Only one article [25] was retained from the study in Daisen-cho (Japan) as it included data from the previous publication. One article [14] synthesized findings in time trends of incidence and prevalence of cognitive impairment and dementia from different studies across the USA. This was retained as it included unique (incidence) data from the Rochester Study; two other relevant studies reported in this article had been identified in the electronic search and were included separately [26, 27]. From the full text review, a further 28 articles [28–55] presented unique findings on time trends in prevalence and/or incidence and were included. Six articles [56–61] were identified from other sources and were also retained. The full text of one potential article [62], identified from a systematic review [63], could not be located. Therefore, 43 articles are included. Most studies used samples representative of the population of interest (see Tables 1 and 2).

Article selection.
Of the 43 articles, 18 [9, 61] included time trends in prevalence, 17 [14, 64] included time trends in incidence, and 8 [20, 57] included time trends in both prevalence and incidence. Tables 1 and 2 summarize the design, methods, and key findings from the prevalence and incidence studies, respectively. Studies varied in the data resources used (health data/record review versus cohort studies), period of assessment (earliest baseline 1947 [41] versus latest baseline 2011 [52]), length of time between comparison studies (range: 3 to >20 years), outcome (all cause dementia, Alzheimer’s disease (AD), and vascular dementia (VaD)) and sample age (entire age range versus restricted to the older aged population).
Details of included studies (arranged by baseline year): Prevalence findings
Key: ACT, The Anatomical Therapeutic Chemical Classification System; AD, Alzheimer’s disease; ADL, Activities of Daily Living; AGECAT, Automated Geriatric Examination for Computer Assisted Taxonomy; DSM-III, Diagnostic & Statistical Manual of Mental Disorders, Third Edition; DSM-III-R, Diagnostic & Statistical Manual of Mental Disorders, Third Edition (Revised); DSM-IV, Diagnostic & Statistical Manual of Mental Disorders, Fourth Edition; GLM, General Linear Model; HDS-R, Hasegawa Dementia Rating Scale-Revised; IADL, Instrumental Activities of Daily Living; ICD-9, International Classification of Diseases, Ninth Revision; ICD-9-CM, The International Classification of Diseases, Ninth Revision, Clinical Modification; ICD-10, The International Classification of Diseases, Tenth Revision; ICD-10-CM, The International Classification of Diseases, Tenth Revision, Clinical Modification; IQCODE, Informant Questionnaire for Cognitive Decline; MMSE, Mini-Mental State Examination; NINCDS ADRDA, National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s Disease and Related Disorders Association criteria; NINDS-AIREN, National Institute of Neurological Disorders and Stroke and Association Internationale pour la Recherché criteria; NR, Not reported; sig, Significant; VaD, vascular dementia; WHO, World Health Organization; y, years.
Details of included studies (arranged by baseline year): Incidence findings
Key: ACT, The Anatomical Therapeutic Chemical Classification System; AD, Alzheimer’s disease; ADL, Activities of Daily Living; AGECAT, Automated Geriatric Examination for Computer Assisted Taxonomy; DSM-III, Diagnostic & Statistical Manual of Mental Disorders, Third Edition; DSM-III-R, Diagnostic & Statistical Manual of Mental Disorders, Third Edition (Revised); DSM-IV, Diagnostic & Statistical Manual of Mental Disorders, Fourth Edition; GLM, General Linear Model; GP General Practitioner; HDS-R, Hasegawa Dementia Rating Scale-Revised; IADL, Instrumental Activities of Daily Living; ICD-9, International Classification of Diseases, Ninth Revision; ICD-9-CM, The International Classification of Diseases, Ninth Revision, Clinical Modification; ICD-10, The International Classification of Diseases, Tenth Revision; ICD-10-CM, The International Classification of Diseases, Tenth Revision, Clinical Modification; MMSE, Mini-Mental State Examination; NIA AD, The National Institutes of Health Alzheimer’s disease criteria; NINCDS ADRDA, National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s Disease and Related Disorders Association criteria; NINDS-AIREN, National Institute of Neurological Disorders and Stroke and Association Internationale pour la Recherché criteria; NR, Not reported; sig, Significant; VaD, vascular dementia; WHO, World Health Organization; y, years.
Prevalence studies
Of the 26 studies reporting time trends in prevalence most were conducted in the USA (n = 5 [9, 50]) and Sweden (n = 5 [32, 41]), followed by Canada (n = 4 [40, 58]), France (n = 3 [29, 56]), Japan (n = 3 [20, 61]), China (n = 2 [30, 45]), the UK (n = 2 [43, 55]), and one study each in Germany [54] and Spain [31]. Nine studies [9, 56–58] used data from medical record, health and health care utilization databases and 17 [20, 61] used cohort study data. Two studies [20, 30] did not maintain consistency in diagnostic criteria across time and used updated criteria at the later time point.
Record-based studies
As shown in Fig. 2, the earliest record-based study captured the time period 1975 to 1985 (USA) and reported mixed findings; stability in prevalence 1975 to 1980 and a significant increase 1980 to 1985 [9]. Five further studies also reported significant increases in dementia prevalence including studies in: The USA (1984–1990 to 1991–2001: With the increase more marked for AD than VaD and senile dementia [not AD or VaD]) [23], France (2004–2010) [56], and three studies in Canada (Alberta: 1998–2009 [40], Saskatchewan: 2005–2006 to 2012–2013 [48], and Ontario: 2004–2005 and 2010–2011 [57]). One study in Canada (British Columbia: 2001–2002 to 2007–2008) reported an increase in dementia prevalence but the time trend was not tested statistically [58]. The remaining two studies reported significant decline in prevalence including one study based in the USA (1994–1999) [21] and the other in Germany (2007–2009: Women only with little change in the total sample) [54].
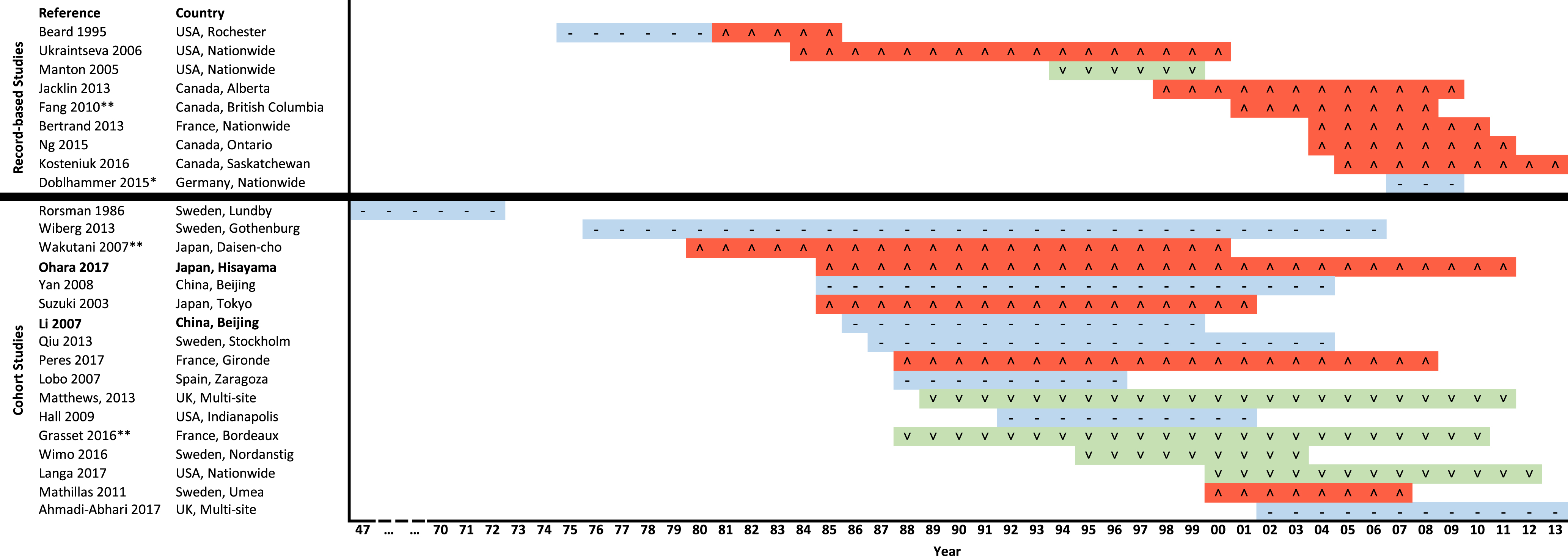
Prevalence trends (based on statistical significance testing, unless otherwise stated) across studies stratified by study design and ordered by earliest baseline. *Significant decline only observed for women (little change over time in the total sample as shown in the figure), stable trend for men. **No statistical test of time trend completed. Bold: Indicates a lack of consistency in diagnostic criteria for dementia across time. Color Key: Blue, Stable rate over time; Green, Decrease in rate over time; Red, Increase in rate over time. Symbol Key: - Stable rate over time; ∧ Increase in rate over time; ∨ Decrease in rate over time.
Cohort studies
As shown in Fig. 2, of the 17 cohort studies, four reported a significant increase in prevalence including studies in: Japan (1985–2001 in dementia [61] and 1985–2012 in dementia and AD only, not VaD or other/unclassified dementia [20]), France (1988–1990 versus 2007–2009) [53], and Sweden (Umea [70- and 75-year-olds only]: 2000–2002 versus 2005–2007, no significant difference in the proportion of AD to VaD between time periods) [32]. A further study, based in Japan (rural area), reported a trend of an increase in the prevalence of dementia and AD (mainly in mild versus moderate/severe cases and a J-shape trend in VaD prevalence: 1980, 1990, and 2000) [25]. However, in this study changes in rates over time were not statistically tested. In contrast, three studies reported a significant decline in prevalence including studies in Rural Sweden (Nordanstig: 1995–1998 versus 2001–2003, total sample and men only) [39], the UK (1989–1994 versus 2008–2011) [55], and the USA (2000–2012) [50]. One study from France (Bordeaux: 1990s versus 2000s) also reported a decline, but the rate of change was not statistically tested [29]. Eight studies reported no significant changes across time including studies in: Sweden (Gothenburg: 1976–1977, 2000–2001, and 2005–2006 [38]; Lundby (senile and multi-infarct dementia): 1947–1957 versus 1957–1972 [41] and Stockholm: 1987–1994 versus 2001–2004 [34]), China (Beijing: 1986–1989 versus 1997–1999 [30] and 1986–2004 [45]), Spain (1988–1989 versus 1994–1996; significant reduction in men only) [31], the USA (1992 to 2001, African Americans only and including all cause, AD, and other dementia disorders) [26] and the UK (2002–2003 to 2012–2013) [43].
Incidence studies
Of the 25 studies reporting time trends in incidence, most were conducted in the USA (n = 7 [14, 60]), followed by Canada (n = 3 [47, 57]), France (n = 2 [29, 56]), the Netherlands (n = 2 [37, 49]), Sweden (n = 2 [35, 41]), UK (n = 2 [33, 43]), Germany (n = 2 [44, 52]), and one study each in Nigeria [28], Denmark [64], Wales [59], Italy [42], Japan [20], and China [30]. Twelve studies [14, 64] used data frommedical record, health and health care utilization databases and thirteen studies [20, 60] used cohort data. Four studies [14, 35] did not maintain consistency in diagnostic criteria across time.
Record-based studies
As shown in Fig. 3, four studies reported an increase in incidence of dementia including studies from: Italy [42] (1998–2000: but, the trend was not statistically tested), the Netherlands [49] (1992–2014: the increase while statistically significant was small, i.e., 2.1%), Wales [59] (relatively stable 1999–2003 and significant increase 2004–2010), and Germany [52] (2011–2015 based on General Practitioner data; relatively stable 2011–2012 and significant increase 2013–2015, mainly driven by increases in VaD and non-specific dementia with a relatively stable trend in AD). In contrast, three studies reported a significant decrease in incidence including two in Canada (Ontario: 2002–2013 [47] and Saskatchewan: 2005–2013 [48]) and one study in Germany (2006–2007 to 2009–2010 [44]). Four studies including one each from France [56] (2004–2010), Germany [52] (2011–2015: Using data from Neuropsychiatric Specialist Practices), the USA [46] (1970 versus 1980), and Canada [57] (Ontario: 2004–2005 to 2010–2011) reported stability in rates.

Incidence trends (based on statistical significance testing, unless otherwise stated) across studies stratified by study design and ordered by earliest baseline. *Total sample and women only (Algorithmic NOT clinical diagnosis). **Total sample and when stratified by ethnicity (greatest decrease in Non-Hispanic Whites or African Americans; lowest in Hispanics). ***Only data for Alzheimer’s disease (AD) is reported. +Significant increase in all-cause dementia and AD. # No statistical test of time trend completed. $Significant reduction in men only. ±Increase mainly due to vascular dementia (VaD) and non-specific dementia (AD stable). Bold: Indicates a lack of consistency in diagnostic criteria across time. Key: Blue, Stable rate over time; Green, Decrease in rate over time; Red, Increase in rate over time. Symbol Key: - Stable rate over time; ∧ Increase in rate over time; ∨ Decrease in rate over time.
Two studies reported mixed results. One study, based in Rochester (USA), reported stability in incidence from 1975 to 1985 and a small but significant decrease from 1985 to 1994 [14]. The other study, based in Demark, reported significant increases in AD from 2000 to 2002–2003 followed by stagnation until 2009 [64].
Cohort studies
Of the 13 cohort studies only one [20] (Japan: 1988 versus 2002; dementia and AD, not VaD or other/unclassified dementia) reported an increase in incidence over time. In contrast, six studies reported significant decreases in dementia incidence including studies in the USA (Framingham, with the risk reduction observed only in persons with high education, 1977–2008 [36]; Indianapolis, African Americas, AD and dementia, 1992–2000 [28]; Washington Heights-Inwood Columbia Aging Project, total sample, Hispanic and African Americans, 1992–2013 [60]; and Bronx County [51], 1993–2015), France (1988–2010: Bordeaux, overall and women [29]), and the UK (2002–2013: mulit-site [43]). The remaining seven studies reported stability in trends including studies based in: Sweden (1947–1957 versus 1957–1972: Lundby, senile and multi-infarct dementia [41] and 1971–1972 versus 2000–2001: Gothenburg [35]), China (1986–1989 versus 1997–1999: Beijing [30]), the Netherlands (1990–2005: Rotterdam [37]), Nigeria (1992–2001: Ibadan [28]), the USA (1997–2008: Chicago, only AD reported [27]), and UK (1989–2011: multi-site, significant decline in men only [33]).
DISCUSSION
This systematic review, the first to our knowledge to incorporate both historical and current secular trends in dementia prevalence and incidence, builds on previous (non-systematic [3, 4]) reviews, to reveal mixed findings, including stability, increases, and decreases in dementia rates worldwide over time across the last seven decades. The lack of consistent findings, including between- and within-country variability, raises questions regarding comparability and quality of studies, and whether there is enough evidence to suggest that worldwide estimates of an increase in dementia currently reported are incorrect and need adjustment.
Prevalence
Differences in the pattern of secular trends in prevalence across different data resources and world regions were observed. Most record based studies report significant increases in prevalence over time from 1980 to 2013 including studies undertaken in the USA [9, 23], Canada [40, 58], and France [56]. What is driving these increases is unclear. The results may reflect true increases in prevalence or, may reflect changes in perceptions of disease and increasing trends in diagnosis, changes in legal cut-points for treatment/insurance, and increases in knowledge and expertise around dementia in the last three decades. In contrast to findings of increasing prevalence, only one record-based study [21] (USA) reported a significant decrease (total sample and males). The contradictory results from the USA are surprising as both studies used the same data resource and their observation period overlapped. However, their definition of dementia varied; with significant decline observed when dementia was more narrowly defined and the assessment period shorter (1994–1999 versus 1984–2001). Lastly, only one study reported stability (Germany from 2007 to 2009); although a significant decline in prevalence was reported in women [54].
In contrast to the results from record-based studies, cohort studies generally reported stable prevalence rates of dementia (and AD) including studies from Sweden, Spain, China (Beijing), and the USA. Decreasing prevalence rates have, however, been reported in studies from the USA, UK, and Sweden. The trends in decreasing prevalence in high-income Western countries generally appear in the most recent decades, suggesting occurrence possibly because of improved health and risk factor management, lifestyle changes, better education, and improved social welfare all of which could be implicit in changing dementia trends.
Significant increases in prevalence rates in cohort studies were, however, observed in France [53], Japan [20, 61] (in rates of all-cause dementia and AD with VaD generally showing a J-shaped trend), and one study from Sweden [32]. In France, the sample were rural (farmers) and while rates increased sharply over the 20 years follow-up in the later born cohort, dementia tended to be milder and participants showed less deterioration and lower mortality over time [53]. This suggests that possibly in the later born cohort diagnosis was being made at a milder stage. In Japan, increases in prevalence of dementia (and AD) have been postulated to be linked to increases in the prevalence of metabolic risk factors, reduced mortality (e.g., from cardiovascular disease and stroke) and therapeutic advances in managing aging-related diseases. Regarding VaD, a decline in dementia prevalence from 1985 to 1998 was suggested to be linked to improvement in the management of hypertension, whereas the steep increase in metabolic disorders and partly insufficient control of hypertension were linked to increased dementia prevalence in 2005 [25]. The results from Japan are in line with other high-income Asian countries. A recent meta-analysis of prevalence studies by birth cohort in mainland China, Hong Kong, and Taiwan (1980 to 2012) showed that the unadjusted prevalence of dementia in these three regions increased monotonically (2.1% to 5.7%) from the earliest to the latest study periods [65]. The meta-analysis also reported a pattern of increasing prevalence, from less recent to most recent birth cohorts (see also [66]). A systematic review and meta-analysis of different prevalence studies from across Korea, found that in the past two decades, the prevalence of dementia (including trends for all dementia, AD, and VaD; pooled across 11 prevalence studies) has decreased until 2000–2005 and then increased thereafter (up to 2013) [67]. However, the trend was not statistically significant. When looking at the five [32, 41] prevalence studies in Sweden, only one [32] reported an increasing trend over time (2000 to 2007). In contrast to the other Swedish studies, the sample was restricted to the very old, defined as people aged ≥70 years. Further, the method of dementia diagnosis included direct assessment in addition to medical record review (e.g., records from General Practitioners, hospitals, and institutions) and this could partly explain the increasing trend observed.
Incidence
Just under half (i.e., 40%) of the included studies reported a decline in incidence rates over time including studies from the USA [14, 60], Canada [47, 48], Germany [44], the UK [43], and France [29]. Declining incidence findings are observed against a background of a rapidly aging population, increasing longevity and increased survival with chronic disease (including dementia [20, 34]) all of which would be expected to lead to an increase in incidence of dementia across subsequent cohorts. Similar to the prevalence findings, declining incidence may be due to better cardiovascular disease control, increased educational attainment [14], compression of cognitive morbidity, and improved care and social welfare. However, as the pattern of disease related comorbidity changes in current generations, particularly increased prevalence of diabetes worldwide [68], the gains seen in current generations may not necessarily be replicated in future generations.
In contrast, five studies reported an increase in incidence including four record based studies from sites in Italy [42], the Netherlands [49], Wales [59], and Germany [52] and one cohort study based in Japan [20]. The remaining studies report stability in trends including studies from France (record based study) [56], Sweden (cohort studies) [35, 41], China (cohort study) [30], the Netherlands (cohort study) [37], Nigeria (cohort study) [28], Germany (record based study and findings observed in neuropsychiatric specialist practices only) [52], the UK (cohort study - total sample and women; significant decrease in men) [33], Denmark (record based study) [4], Canada (record based study) [57], and the USA (record based study as well as a cohort study focused only on AD) [27, 46].
However, it is important to note that for some incidence studies while trends were not significant relatively large changes in risk over time were observed (see Supplementary Table 1). For example, a study from the UK [33] reported a 20% non-significant decline in risk over 20 years from 1989–1994 to 2008–2011 and a study from the Netherlands [37] reported a 25% lower risk in a later born (2000–2005) compared to the earlier born cohort (1990–1995) and again the result was not statistically significant. This is in contrast to studies with smaller changes in risk over time where results are significant (i.e., Canada, Ontario 7.4% significant decline from 2002 to 2013 [47]). While we have chosen to focus on statistical significance, these results highlight that it is also important to look at the actual rates and size of change. Further studies, with increased numbers and longer follow-up times to confirm results, particularly small but significant changes, are needed.
Strengths and limitations
Due to the broad topic under review, the search was purposefully kept general, without time restrictions, to minimize the chances of missing relevant studies. This may represent an important bias given that diagnostic criteria and the sensitivity of physicians, has improved in the last decade and a more precise definition of dementia is possible nowadays than in the past. However, this allowed the opportunity for historical as well as current secular trends to be explored. There was large heterogeneity across studies in how dementia was defined, and data collected. Therefore, it was not possible to synthesis the findings in a meta-analysis. Instead, the review gives a comprehensive overview of time trends in dementia across different world regions. Figures showing the pattern of time-trends (based on statistical significance) and the reported percentage change in rates over time (Supplementary Material 2) are provided to allow for cross-study comparison. Further, not all studies have tested changes in trends over time statistically. Lastly, four studies, including two incidence [14, 35] and two combined prevalence/incidence studies [20, 30], did not maintain consistency in diagnostic criteria across time which could have affected the observed rates. However, a sensitivity analysis removing these studies from the results does not change the conclusions of mixed secular trend findings in dementia prevalence and incidence rates.
We included both record-based and cohort studies in the review. Discrepancies in findings between the two study designs may be attributable to several methodological factors. Cohort studies largely ascertain dementia diagnoses based on consistent study protocols over time, including case finding, diagnostic work-up and adjudication of cases according to (in the majority of studies) constant dementia criteria. In contrast, changes in the criteria used to establish dementia, or changes in perceptions of disease among individuals or their treating physicians in record-based studies introduces instability of diagnostic sensitivity. Similarly, in many countries a dementia diagnosis is required to arrange additional healthcare, e.g., admission to a nursing home, which may give rise to conflicting incentives to properly diagnose an individual. Additionally, case ascertainment based on classification systems in record-based studies may erroneously classify individuals, in part attributable to proceedings such as the aforementioned. On the other hand, beyond their study protocols, many cohort studies make substantial efforts to keep their participants in the study in order to minimize loss to follow-up thus reducing potential bias due to attrition. Moreover, some cohort studies further improve coverage of interval cases by linking their study data with medical records from general practitioners, by assessing hospital discharge letters, and by using pharmacy data.
CONCLUSIONS
There is conflicting evidence on the secular changes in prevalence and incidence of dementia worldwide. Some studies have found an increase in prevalence and incidence while others have shown a decline or stability in trends. Results vary across the different data sources (i.e., record based versus cohort study), sample demographics (i.e., population age and gender), and even regionally (i.e., some studies from the same country have reported contradictory findings). There is a clear gap in data from low and middle-income countries. Knowing the number of people at risk of future dementia will be important for service commissioning, planning and distribution of health and welfare resources with the aim to decrease future case numbers and the global burden of disease associated with dementia.
Footnotes
ACKNOWLEDGMENTS
The authors would like to thank Dr Kazutaka Yoshida, Dr Kanke Satoshi and Dr Long Xie for assisting with translation and data extraction of the non-English articles.
The work was supported by the National Institutes of Health (NIHR) [NIHR Global Group: DePEC 16/137/62]. Tang is supported by an NIHR Doctoral Research Fellowship (DRF-2015-08-006). Robinson is supported by an NIHR professorship (NIHR-RP-011-043) and an NIHR Senior Investigator award (NF-SI-0616-10054). Siervo is supported by a Medical Research Council Grant (MR/N007921/1).