
Abstract
Background:
Neurocognitive disorders (NCD) are underdiagnosed in primary care, mainly because of the misunderstanding of benefits associated with timely diagnosis.
Objective:
The aim of this study was to explore the benefits and risks of diagnosis in a population of general practitioners (GPs), specialized physicians (SPs), other healthcare professionals (HPs), and informal caregivers (ICs).
Methods:
A questionnaire was submitted to GPs, SPs, HPs. and ICs. It aimed at evaluating benefits and risks related to NCD diagnosis associated with four prototypical clinical cases at different stages: isolated cognitive complaint/mild NCD, major NCD at mild/moderate stage, moderate stage with behavioral and psychotic symptoms, and severe stage. The concepts of early, timely, and personalized diagnosis were evaluated.
Results:
A total of 719 completed surveys were collected from 183 GPs, 176 SPs, 281 HPs, and 79 ICs. More than 90% of the participants considered initiating a diagnosis as relevant except at the severe stage. Benefits were superior to risks for all groups and all four cases alike (p < 0.001). Benefits were lower according to GPs and higher for SPs than the other groups at the first two stages (p < 0.001). At the moderate stage, there were few differences between groups. At the severe stage, GPs and SPs claimed it was less relevant to carry out a diagnosis than the other groups (p < 0.001). Risks were higher for ICs and lower for SPs (p < 0.001). The best diagnosis concept was the personalized diagnosis.
Conclusion:
Benefits appeared more relevant than risks with differences according to the stage of the disease and type of respondents.
INTRODUCTION
Neurocognitive disorders (NCD) including Alzheimer’s disease and related diseases represent a major and growing health issue with an estimation of approximately 45 to 48 million people affected worldwide [1–3]. An important surge of Alzheimer’s disease cases, up to 80 million by 2030 and 140 million in 2050, is expected to occur in the future because of the increasing life expectancy despite recent incident decrease by age range [4, 5]. In response to this public health challenge, several countries, including France, have developed a national policy for the diagnosis and care of NCD [6]. NCD raise ethical challenges regarding both benefits and risks associated with the diagnosis at each step of the disease for people living with NCD, but also for the informal caregivers, the healthcare providers and society. Consequently, it is estimated that only half of people with dementia is diagnosed, and that the diagnosis is often performed late. Dementia diagnosis thus represents an issue in primary care [3, 8]. Moreover, the diagnosis is often performed late (Mini-Mental State Examination mean score in France at diagnosis: 18.91±5.48) [9, 10], leading to a late management.
Developing a better diagnosis strategy focusing on ethical issues was one aim of the European Joint Action “AlzheimerCooperativeValuation in Europe” (ALCOVE) in 2013 which is currently followed by the European Joint Action “Act on Dementia” [8]. Thanks to these works, the concept of a timely diagnosis arose. It refers to a diagnosis at the stage when patients meet clinicians because of concerns about cognitive, behavioral, or functional changes. These patients may also present with an “at risk” situation without expressing any complaint. They may also still be free of dementia and functionally independent [11]. A timely diagnosis potentially offers the opportunities of early intervention, preservation of quality of life, education of patients and caregivers, advanced directives, implementation of coordinated care, better management of symptoms and at-risk behaviors (medications or other interventions), access to clinical trials, organization of timely counseling and social support as well as access to resource and psycho-educational groups. This term (timely) differs from the term early diagnosis which refers only to the notion of time and is not adapted to individual needs.
Barriers to the timely diagnosis include stigma, denial, anxiety, depression risk, diagnosis uncertainty, shortage of specialized diagnosis services, downplaying of symptoms, fear and anxiety of caregivers, and the reluctance of healthcare providers to make a diagnosis when no effective disease-modifying options are available [11]. However, several studies have reported that almost all the patients as well as family/close relatives would be in favor of receiving an accurate and informed diagnosis in case of “clinically-proven” NCD [12–16].
Few published studies have explored the benefits or risks of a timely diagnosis of NCD. Further investigations are needed to evaluate the benefits and improve the understanding of the barriers that may impede a timely diagnosis [11]. Determining the main barriers and advantages seems to be essential to elaborate the most appropriate national NCD diagnosis policy and decrease the brakes for primary care detection. We hypothesized that general practitioners (GPs) are sensitive to ethical issues regarding the diagnosis of NCD, and this approach considering the benefits/risks ratio would help to decrease the brakes of NCD detection in primary care. This study was conducted to assess the perception of ethical issues and challenges of NCD diagnosis, i.e., benefits and risks, in a French population of informal caregivers (ICs) and health professionals involving GPs, specialized physicians (SPs, i.e., neurologists, geriatricians, and psychiatrists), and other healthcare professionals (HPs) at different stages of the disease from mild NCD to severe stages of the major NCD [17–20]. The aim of the study was to assess the perception of benefits and risks among professional respondents and caregivers throughout the stages of the disease.
METHODS
Study design and setting
This national study was a non-interventional study based on a descriptive survey in France. A standardized questionnaire was sent by email. It was available on GoogleForms® [21]. Self-reported answers were collected from June 30 until November 24 of 2016 on a Microsoft® Excel file. Participants were free to take part in the study, questionnaires were anonymous, and no incentive was given in exchange for participation to this study. Consent from participants was implied by the completion and submission of the online survey.
Study population
There were four groups: ICs (contacted via the internet website of the French national association “France Alzheimer”), GPs (contacted via the Departmental Boards of the College of Physicians and Regional Unions of Liberal Doctors), cognition SPs (neurologists, geriatricians, and psychiatrists contacted via the French Research and Resources Memory Centers, Memory clinics, and liberal neurologists associations), and other HPs (contacted via professional societies of each specialty).
Data collection
The sociodemographic data (gender, age, location, and type of dwelling or work) and a self-assessment of knowledge of diagnosis process and care plan for patients with NCD (with a scale between 0 and 5) were collected.
The survey included four clinical cases at four different stages of NCD, uninvestigated until now: Case 1: isolated memory complaint without autonomy loss (isolated cognitive complaint or complaint with mild NCD); Case 2: memory and language complaint for 18 months associated with difficulties in activities of daily living (major NCD at mild/moderate stage); Case 3: cognitive disorders for 2 years and behavioral and psychotic symptoms of dementia (BPSD) (major NCD at moderate/severe stage with BPSD); Case 4: severe cognitive and BPSD with severe autonomy loss in a nursing home (major NCD at severe stage).
Each case presentation was outlined along with a list of possible benefits and risks of a diagnosis workup of NCD based on the ALCOVE Joint Action [8] (Table 1).
Benefits and risks of initiating a diagnosis workup proposed in the survey
For each case, the participants were first asked about the relevance of the initiation of a diagnosis workup by answering a close-ended question. Furthermore, for case 1, the respondents had to reply to another close-ended question about the relevance of making a diagnosis without patient complaint.
Then, they were asked to evaluate each benefit and risk on a scale from 0 to 5; 0 being the most irrelevant score for the item and 5 being the most relevant score for the item. This scale was chosen to avoid having a neutral answer. Participants could also report by themselves other benefits or risks.
The means of the scores were calculated for each group (GPs, SPs, HPs, and ICs) at each stage. The means of the scores of the 8 benefits as well as the 8 risks (respectively evaluated from 0 to 5) range from 0 to 40. The ratio between the sum of the 8 benefits and the sum of the 8 risks was calculated for each case. As the sum of the 8 risks may equal 0, the sums of benefits and risks were shifted by 1 point to allow performing the division:
A ratio higher than 1 was interpreted as a case for which the benefit was globally considered higher than the risk whereas a ratio lower than 1 was interpreted as a case for which the benefit was lower than the risk. A ratio equal to 1 was considered as a case with equal overall benefit and risk.
In the end, participants were asked to evaluate the relevance of the terms early diagnosis, timely diagnosis, that is matching the patient’s characteristics (stage of the disorder and patient’s or relatives’ expectations), and personalized diagnosis (a timely diagnosis coupled with a specific care plan) (score from 0 to 5; 0 being totally irrelevant and 5 being totally relevant score). Finally, medical doctors were asked whether diagnosis workup would be promoted by the publication of national or international guidelines regarding a diagnosis strategy at each stage. The questionnaire, with the four clinical cases, is available in the Supplementary Material.
Statistical analysis
Socio-demographic characteristics of the participant groups (GPs, SPs, HPs, and ICs) were compared using the Pearson Chi-square test. The relevance of the initiation of diagnosis workup was described by considering the proportion of positive answer. These proportions were compared between groups by using the Pearson Chi-square test. For each case, the score of benefits was compared to the score of risks using the paired t-test. In addition, the scores of benefits as well as the scores of risks of each case were also compared between each other using the Friedman’s test. Comparisons of the scores between groups of participants were performed using a multivariate general linear model (GLM). In this model, the 8 scores of benefits and risks were considered as dependent variables and the group of participants as independent variables. The effect of potential confounders (gender, age, and location) was assessed. The global p value of the Fisher test was reported as well as the p values for pair-wise comparisons (Bonferroni post-hoc test) between the groups of participants if applicable. Throughout the tables and text, results are presented as means±SD (standard deviation). Comparisons of the benefit-risk ratios between groups were performed using a multivariate GLM. As the distribution of the ratios was skewed, they were log-transformed for the analysis. Bonferroni and Scheffé’s post-hoc tests were used for pair-wise comparisons.
A p value <0.05 was considered statistically significant. All statistical tests were two-tailed. Statistical analyses were performed using SPSS (Statistical Package for the Social Sciences) version 19.0 for Windows (SPSS Inc., Chicago, IL, USA).
RESULTS
Demographic data
The study population included 719 subjects: 183 GPs, 176 SPs (114 geriatricians, 52 neurologists, 10 psychiatrists), 281 HPs (234 speech therapists, 47 other professionals), and 79 ICs (Table 2).
Characteristics of the study population (n = 719). *Chi-square test
Relevance of the initiation of diagnosis workup
The initiation of a diagnosis workup was considered as relevant by all the participants in all stages. All the results are summarized in the Table 3. Regarding the case 1 (isolated cognitive complaint or mild NCD), 59.6% of GPs, 74.4% of SPs, 75.9% of ICs, and 61.9% of HPs agreed to its relevance in case of the absence of a patient’s complaint, as requested by an additional question, with significant differences (p = 0.002) between respondents.
Relevance to initiate a diagnosis workup by type of respondents
Perceived benefits and risks according to disease stage
All the results are summarized in the (Fig. 1a).In each clinical case, benefits were significantly higher than the risks (p < 0.001). However, perceived benefits and risks varied significantly between clinical cases (p < 0.001). Cases 2 and 3 had the highest benefits score (respectively, 30.3±6.8 and 29.8±6.8) compared to the other cases (p < 0.001). Case 1 was associated with the highest risks score (18.0±9.2). Case 4 had simultaneously the lowest benefits and risks scores (respectively, 21.8±9.9 and 11.9±9.6) compared to the other cases (Fig. 1a).

Perceived benefits and risks according to disease stage and to group. a) Global means scores of benefits and risks for each case. b) Differences between each group regarding benefits and risks scores. Case 1: isolated cognitive complaint or complaint with mild NCD; Case 2: major NCD at mild/moderate stage; Case 3: major NCD at moderate/severe stage with BPSD; Case 4: major NCD at severe stage with severe BPSD. NCD, neurocognitive disorders; BPSD, behavioral and psychological symptoms of dementia. Paired t test, Error bars represent 95% confidence intervals.
Perceived benefits and risks according to group
All the results are summarized in (Fig. 1b and Supplementary Table 1). Age, gender, and location did not contribute significantly to the model (respectively: p = 0.11, p = 0.22, and p = 0.93). In the model, the SPs systematically assigned lower risks for all the cases (p≤0.001 for all pair-wise comparisons with SPs). In terms of risks, GPs attributed similar risks compared to HPs, whatever the cases. Conversely, ICs attributed the highest risks, in particular for the cases 1 and 2 compared to other participants. The SPs and HPs attributed the highest benefits in the cases 1, 2, and 3 compared to other participants. Finally, in the case 4, ICs and HPs attributed the highest benefits score (Fig. 1b and Supplementary Table 1).
Benefit-risk ratio of a diagnosis workup
For all the cases and all the participants, the benefit-risk ratios were higher than 1, that is to say, the participants considered there were more benefits than risks for each situation. The benefit-risk ratio was higher for the SPs compared to the other groups with a significant difference (p < 0.001) in all the cases. Regarding the other participants, in the cases 1 and 4, ICs, GPs and HPs had similar benefit-risk ratio (respectively Scheffe’s test p = 0.13 and p = 0.35). In the cases 2 and 3, ICs had the lowest ratio compared to the others (Fig. 2).
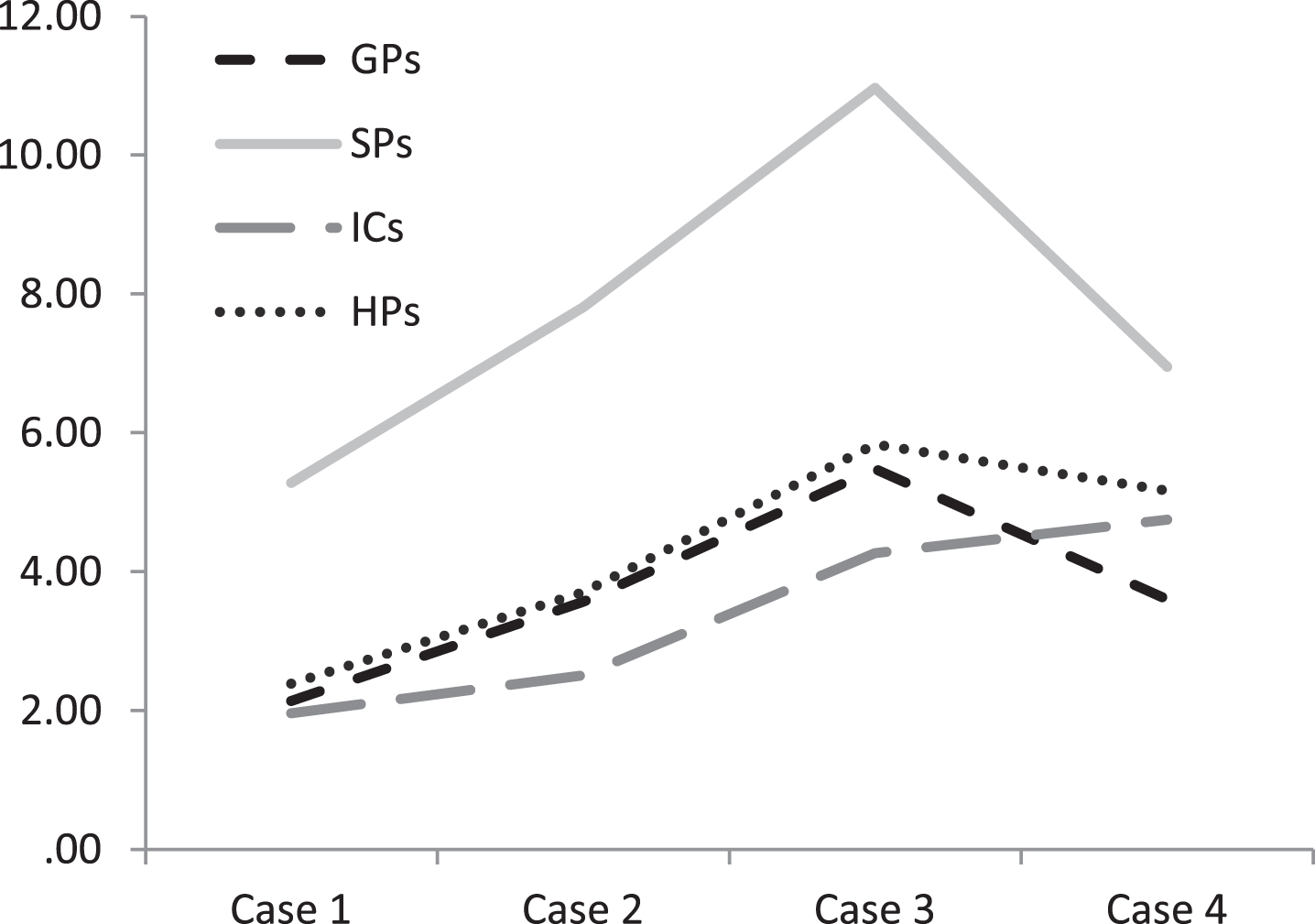
Log-transformed benefit-risk ratios for each case.
Responses about the diagnosis concepts and guidelines
Regarding the diagnosis concepts, there was a clear consensus in all groups about the term personalized diagnosis, i.e., a timely diagnosis with tailored diagnosis strategy including a specific care plan. Its global mean score of 4.2 (from 0 to 5) was significantly higher than the mean scores of early diagnosis (p = 0.001) and timely diagnosis (p < 0.001). No significant difference was observed between respondents (p = 0.246). The concept of early diagnosis was more debated. Its global mean score was significantly lower than the mean score of personalized diagnosis (p = 0.001) and it was significantly lower for the GPs when compared to the scores of SPs, HPs, and ICs (Fig. 3). The majority of respondents claimed that diagnosis workup would be encouraged with a systematic personalized diagnosis: 90.2% of GPs, 83.5% of SPs, 93.7% of ICs, and 90.4% of HPs. Finally, 80.3% of GPs and 77.8% of SPs stated that diagnosis workup should be encouraged with national or international guidelines of diagnosis strategy at each stage.
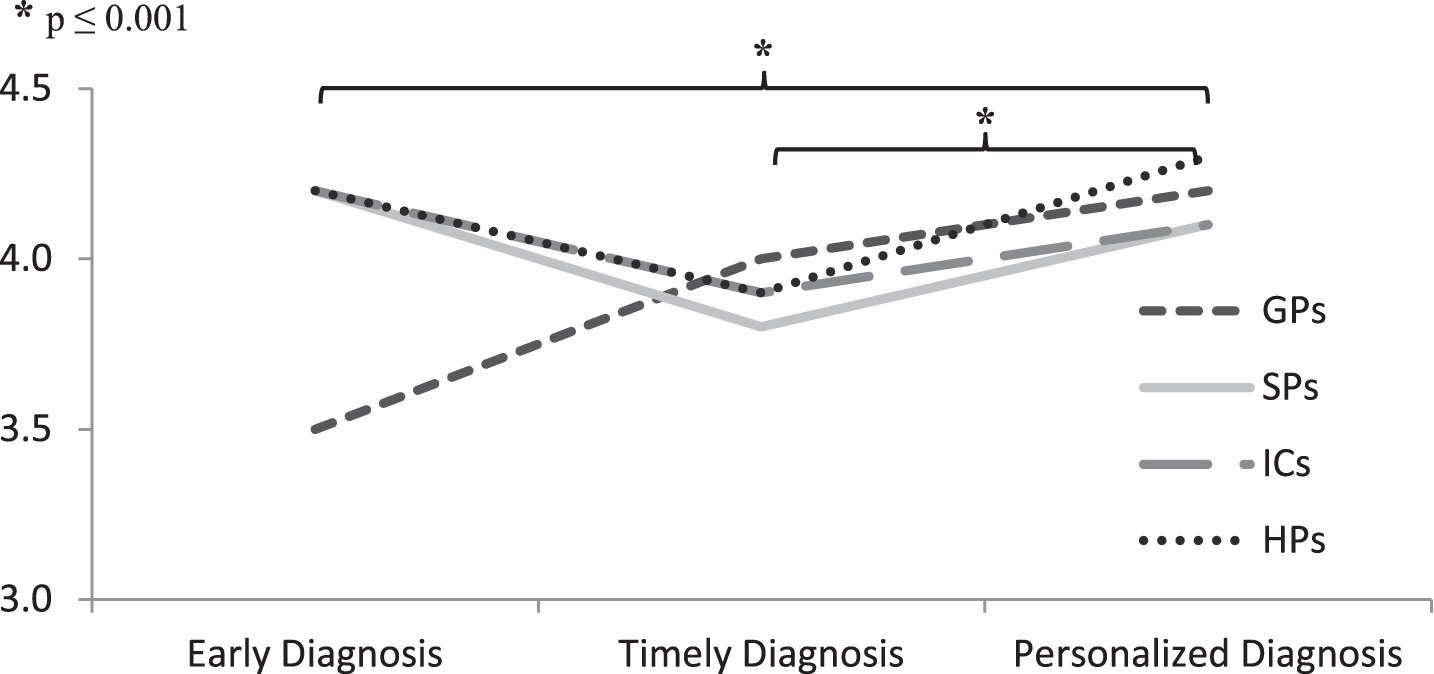
Relevance for the concepts of diagnosis workup.
DISCUSSION
After compiling all the putative risks and benefits of the diagnostic workup of dementia, this study shows that most participants perceived more benefits than risks, whatever the disease stage. These results seem highlight a strong agreement about NCD diagnosis even at the stage of isolated cognitive complaint/mild NCD despite the underdiagnosis of NCD found in the literature [3, 8]. The high relevance of a diagnosis workup found in this study is in line with the high percentage of the French population who would like to know the diagnosis if they had Alzheimer’s disease (91%) [22].
This study shows differences in the perception of ethical issues and challenges of NCD diagnosis between respondents at each stage of NCD. Benefits associated with the diagnosis decreased with the evolution of the disease. According to the respondents, and especially for the SPs and GPs, benefits of the diagnosis are lesser at the late stage of the disease when the patient is suffering from severe NCD with behavioral disorders. In the late stage, ICs and HPs are the ones perceiving more benefits. Unlike physicians, ICs and HPs provide help and care to people affected by NCD on a daily or weekly basis. That may explain the fact that they consider the diagnosis as well as post-diagnostic support helpful at this stage. The benefit-risk ratio of a diagnosis workup in this study is not significantly different between the case 1 and the case 4 for each group of respondents. This suggests that all patients benefit from a diagnosis workup tailored to their complaint, their general condition and the evolution of their disease. Initiating a diagnosis workup is the only way to make the differential diagnosis and in particular the curable cause of NCD. It is crucial to consider all NCD etiologies associated to specific and sometimes curable therapeutic approaches such as depression or subdural hematoma.
In this study, there are some differences between respondents. Indeed, SPs consider carrying out the diagnosis more beneficial than GPs. This is possibly explained because GPs are generally more sensitive about the risks for the patients and the caregivers since they are closer to families than SPs. However, many studies show that future GPs are enthusiastic and are willing to fulfill their key role in NCD care [23]. They are well positioned to notice the possible cognitive decline of individuals thanks to the continuity of care and existing inter-personal relationships [24]. The fact that it is at the first stage of NCD that the difference between GPs and SPs in the perceived risks is the highest, and that the GPs are the ones less in favor of early diagnosis, emphasizing the need for continuing medical education programs focusing on the this stage of NCD. They express a wish for further education ideally through small group workshops [25]. GPs also highlight the importance of better collaboration with specialists and adequate guidelines to improve the efficiency of referrals. Strategies for the involvement of primary care in the management of patients with presumed or diagnosed NCD are heterogeneous across Europe [26]. The caregivers experience in everyday life the negative psychological impact of the disclosure. Besides, they feel the stigma or the isolation and face the difficulties to start a diagnosis workup [27–31]. The main barrier to diagnosis may be the familial environment, emphasizing the need for caregiver-directed campaigns. However, in this study, they are the most willing to benefit from a diagnosis, including in the situation of a subjective cognitive decline or mild NCD.
Regarding the diagnosis concepts, there seems to exist a clear consensus about the conditions of this diagnosis workup. The most relevant concept highlighted by this work is a personalized diagnosis. First, this concept refers to a timely diagnosis, i.e., a tailored diagnosis strategy in accordance with the couple patient/close caregiver’s needs and wills respecting the general principle of autonomy [11, 33]. Also, a personalized diagnosis should lead up to a global and personalized care plan established altogether with the patient, his or her close caregiver and all the professionals involved. This is the best way to initiate a diagnosis process. Ideally, the diagnosis process must start as early as possible in the course of the disease evolution to allow the patient and his or her informal caregiver to organize and anticipate the future, participate in medical decisions, and access research and clinical trials [11, 32].
In this survey, 80.3% of GPs and 77.8% of SPs stated that NCD diagnosis would be encouraged if there were guidelines about diagnosis workup at each stage. This diagnosis workup depends on the cognitive, behavioral and functional stage of the patient and should be graduated along the evolution of the disease. Therefore, recently in France, the representatives of the National College of General Practitioners, the French Federation of Memory Centers, the French Federation of Gerontology and Geriatrics, the French Federation of Neurology, the French Society of Psychogeriatrics, and the national plan on neurodegenerative diseases proposed a graduated and tailored diagnosis strategy involving primary care and specialists of NCD [34]. This collaborative strategy aims at harmonizing the different points of view.
Several strengths of the study should be highlighted. This study is a national survey concerning large and different populations as opposed to the studies addressing one or two specific groups such as GPs [35–37], SPs [37], and the general population [22, 38]. The choice of prototypical clinical cases representing each stage of the disease according to the international classification of NCD and understandable by both the medical and non-medical community constitute the originality and the strength of this study design. To our knowledge, the present study is the first to explore the perceived ethical issues of NCD in a population of medical doctors (GPs and SPs) compared to other HPs and ICs.
Some limitations must be taken into account when interpreting our results. We do not know how many people received and did not answer the questionnaire but participants who answered the online questionnaire may be those who are naturally interested in NCD. People, especially GPs who are not interested in NCD, may have not completed the questionnaire. This constitutes a selection bias which did not allow to know their arguments against diagnosis. The ICs sample size was smaller than the sample sizes of the other groups. Even if a representative sample of GPs may have been more reluctant to the diagnosis workup, differences between clinical cases and differences between groups recruited in the same fashion are still interesting.
In conclusion, this study states for the first time that French GPs, SPs, other HPs, and ICs respondents assert that benefits of carrying out a diagnosis of NCD are more relevant than their risks. ICs insist more on the risks while SPs insist more on the benefits at each stage of NCD. Further analyses are needed to determine which benefits and risks are the most relevant during the evolution of the disease and the best lever to motivate people to initiate a diagnosis workup. It would be useful to elaborate guidelines for diagnosis strategy at each stage to help all the community making a better personalized diagnosis.
Footnotes
ACKNOWLEDGMENTS
France Alzheimer association, National Union of Healthcare Professionals, French Federation of Memory Centers, Departmental Councils of the College of Physicians and Regional Unions of Liberal Doctors which have collaborated. This work is the end-of-study dissertation for the DIU MA2 course of A. Garnier-Crussard, J. Vernaudon, and N. Auguste. The DIU MA2 course (Diplôme Inter Universitaire de diagnostic et de prise en charge des Maladies d’Alzheimer et Apparentées) is the French transdisciplinary course on diagnosis and care of Alzheimer’s Disease and related disorders (![]() ) The course is supported by the Fondation Alzheimer and the Fondation Vaincre Alzheimer.
) The course is supported by the Fondation Alzheimer and the Fondation Vaincre Alzheimer.