
Abstract
Background:
Neurocognitive disorders (NCD) are a growing health issue and the importance of diagnosis is still debated despite the benefits of making a diagnosis appearing to be greater than the risks.
Objective:
The aim of the present study was to explore the perception of the main benefits and risks to perform a diagnosis workup of NCD in a population of general practitioners (GPs), specialized physicians (SPs), other healthcare professionals (OHPs), and informal caregivers (ICs), and to identify the lowest perceived benefits and the highest perceived risks that could be levers to promote a diagnosis of NCD.
Methods:
A standardized questionnaire was submitted to GPs, SPs, OHPs, and ICs aiming to evaluate the importance of eight benefits and eight risks related to NCD diagnosis (selected from the literature) for four prototypical clinical cases at different stages of the disease: subjective cognitive impairment/mild NCD, major NCD at mild/moderate stage, moderate stage with behavioral and psychotic symptoms, and severe stage.
Results:
The lowest perceived benefits of making an NCD diagnosis were “access to medical research”, “patient’s right to know”, and “initiation of symptomatic drug treatment”. The highest perceived risks of making an NCD diagnosis were “negative psychological impact for the patient”, “absence of disease-modifying treatment”, and “absence of suitable institution”.
Conclusion:
This study highlights the lowest perceived benefits and the highest perceived risks of making an NCD diagnosis. These benefits and risks could be modified to become levers to promote a personalized diagnosis of NCD.
Keywords
INTRODUCTION
Neurocognitive disorders (NCD) are a major and growing health issue [1], but remain under-diagnosed, and when a diagnosis is made, it is late in the course of the disease at a time when cognition and behavior are already deeply altered [2–5]. In France, the mean Mini-Mental State Examination score at the first diagnosis of NCD was estimated at 18.91±5.48 [4], and the mean dementia diagnosis rate was 66% in 2017/18 in the United Kingdom [6, 7].
For the identification of NCD patients, both an early diagnosis, i.e., as early as possible in the course of the disease (corresponding to the Chronos conception of time in ancient Greek [8], i.e., chronological time), and timely diagnosis of NCD has emerged (Kairos conception of time [8], i.e., an opportune moment, or right time) [2, 10]. The first European joint action on Alzheimer’s disease (AD) recommended in 2013 a timely diagnosis, when people first notice changes in cognition or behavior, complain, or present with a situation at risk that should be accessible to all sections of the community at a stage [2]. At the personal level, diagnosis of NCD is not experienced in terms of chronological time, and it has recently been reported that personalized diagnosis is more pertinent. A personalized diagnosis is defined as a diagnosis strategy in accordance with the dyad patient/caregiver’s needs and wills respecting the general principle of autonomy and should lead up to a global and personalized care plan established together with the patient, his or her close caregiver, and all the professionals involved [11, 12].
Diagnosis of NCD is associated with benefits for patients, caregivers, and society, for example future planning, elaboration of a suitable care plan, better informed patients and patient relatives who will better understand the symptoms and the course of the disease, access to medical research, and early interventions to prevent or delay progression [7, 14]. Risks related to an NCD diagnosis are also described, and include stigmatization, isolation, and lack of disease-modifying treatment in particular, and could explain the under-diagnosis of NCD [11, 15]. Many studies report that the general population would like to have the diagnosis if they had NCD [16–21]. We previously reported that perception of benefits of an NCD diagnosis workup was stronger than risks, at each stage of the NCD (from subjective cognitive decline to severe major NCD) among general practitioners (GPs), cognition specialized physicians (SPs; i.e., neurologists, psychiatrists, and geriatricians), other healthcare professionals (OHPs), and informal caregivers (ICs) in a national French survey [11]. Herein we will analyze with the same sample of respondents, the relative importance of each main risk and each main benefit from the point of view of GPs, SPs, ICs, and OHPs, and at each stage of NCD, but also between respondents. We hypothesize that the diagnosis workup of NCD could be further promoted by increasing further the balance in favor of benefits, and for this it is important to identify the benefits and risks that could be targeted.
METHODS
Study design and setting
This study was a national multicenter descriptive survey conducted in France. A standardized self-administrative questionnaire was sent by email in June 2016 and replies received up to the end of November 2016 were included, as previously described [11]. Participants were free to take part in the study, questionnaires were anonymous, and no incentive was given in exchange for participation to this study. Consent from participants was implied by completion and submission of the questionnaire.
Study population
There were four groups: ICs (contacted via the national patient and caregiver association France Alzheimer), GPs (contacted via departmental councils of the college of physicians and regional unions of private practitioner physicians), cognition SPs (neurologists, geriatricians and psychiatrists contacted via the French federation of memory centers, and private practice neurologist associations), and other OHPs (contacted via professional societies of each specialty).
Data collection
The survey contained four short clinical cases at four different stages of NCD, uninvestigated until now. Case 1 corresponded to a person with isolated memory impairment without autonomy loss (if an investigation was done, the stage would probably be subjective cognitive impairment or mild NCD) [22–24]. Case 2 corresponded to a person with memory and language impairment for the previous 18 months, associated with difficulties in activities of daily living (if an investigation was done, the stage would probably be major NCD at mild/moderate stage) [22, 25]. Case 3 corresponded to a person with cognitive disorders over the 2 previous years and behavioral and psychotic symptoms of dementia (if an investigation was done, the stage would probably be major NCD at moderate/severe stage with behavioral and psychotic symptoms of dementia) [22, 25]. Case 4 corresponded to a person with severe cognitive impairment and behavioral and psychotic symptoms of dementia with severe loss of autonomy (if an investigation was done, the stage would probably be major NCD at severe stage) [22, 25] (see details in Supplementary Table 1).
Each case presentation was accompanied by a list of possible benefits and risks of a diagnosis investigation of NCD [2].
The eight benefits were: patient’s right to know, future planning through decision-making (advanced healthcare directives, trusted person), initiation of symptomatic drug treatment, initiation of non-drug treatment, elaboration of a suitable care plan, inform the patient and his/her relatives to better understand the disease and its course, relatives’ adaptation to the changes, and access to medical research (clinical trials).
The eight risks were: to identify memory disorders related to aging as abnormal, absence of diagnosis certainty, negative psychological impact for the patient, negative psychological impact for the relative, absence of disease-modifying treatment, difficult access to a diagnosis platform, absence of suitable institution at a specific stage of the disease, and stigmatization, rejection, isolation.
Participants were asked to evaluate benefits and risks to initiate a diagnostic work-up of NCD. The pertinence of benefits and risks were evaluated on a 6-point Likert scale from 0 to 5; 0 being the least pertinent and 5 the most [26]. This was chosen to avoid having a neutral answer. The mean scores of each benefit and risk were calculated for each group (GPs, SPs, OHPs, ICs) at each stage of disease.
Statistical analysis
The following analyses were conducted separately for each of the four cases. For the evaluation of the relative importance of risks and benefits among respondents, the Likert scale scores (dependent variables) for the eight types of benefit (independent variable) were compared using a non-parametric Kruskal-Wallis analysis of variance; as were the eight types of risk (independent variable). Results were summarized in figures as the mean score for each benefit and risk for each case and their 95% confidence intervals [95% CI]. The p value of the Kruskal-Wallis test was reported, as well as the p values for Wilcoxon pair-wise comparisons (corrected using the Holm method) between the type of benefits or risks as appropriate. For the secondary objective, the scores between groups of participants were compared using the Kruskal-Wallis analysis of variance. In this model, the eight scores of benefits and risks were considered as dependent variables, and the group of participants as the independent variable. The p value of the Kruskal-Wallis test was reported. A p value < 0.05 was considered significant and statistical tests were two-tailed. Statistical analyses were performed using R software version 3.5.2 (R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
Population
Data were collected from 719 subjects: 183 GPs, 176 SPs (114 geriatricians, 52 neurologists, and 10 psychiatrists), 281 OHPs (234 speech therapists, 47 various), and 79 ICs.
Perception of benefits in the total population for each case
The eight benefits were perceived significantly differently in the total population of respondents in each case (p < 0.001; Fig. 1). For case 1, the benefits “access to medical research” and “initiation of symptomatic drug treatment” were significantly lower than the other benefits. For cases 2, 3, and 4, the benefits “access to medical research”, “initiation of symptomatic drug treatment”, and “patient’s right to know” were significantly lower than the other benefits (Fig. 1).

Relative importance of different benefits in the decision to carry out an NCD diagnosis. Means and 95% confidence interval of each benefit and each stage in the total population of respondents are presented.
Perception of different risks in the total population for each case
The eight risks were perceived significantly differently in the total population of respondents in each case (p < 0.01; Fig. 2). For cases 1 and 2, the risk “negative psychological impact for the patient” was significantly higher than the other risks. For case 3, the highest perceived risk was the “absence of suitable institution at a specific stage of the disease”, whereas for case 4 the highest perceived risk was the “absence of disease-modifying treatment” (Fig. 2).
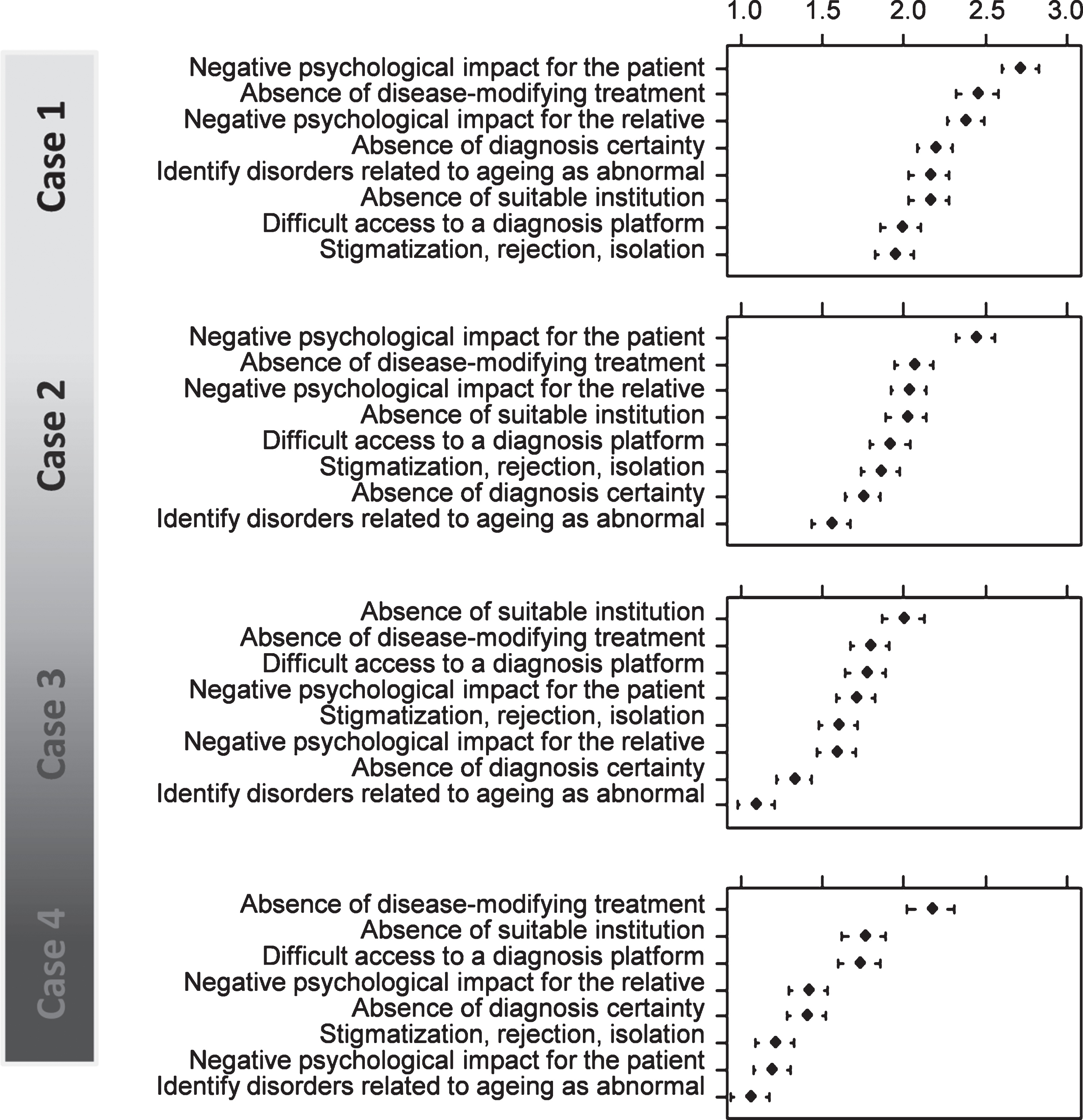
Relative importance of different risks in the decision to carry out an NCD diagnosis. Means and 95% confidence interval of each risk and each stage in the total population of respondents are presented.
Perception of benefits and risks according to type of respondent
For case 1, the perception of benefits and risks was significantly different between respondents, i.e., between GPs, SPs, ICs, and OHPs, except for the benefit “elaboration of a suitable care plan” (p = 0.11). For case 2, the perception of benefits and risks was significantly different between respondents, except for the benefit “future planning” (p = 0.64). For case 3, the perception of benefits and risks was significantly different between respondents, except for the benefit “Initiation of non-drug treatment” (p = 0.41). For case 4, the perception of benefits and risks was significantly different between respondents. Overall all the benefits and risks decreased from the case 1 to the case 4 (Figs. 3 and 4).

Perception of the 8 benefits of NCD diagnosis, for each respondent and each case. ***p < 0.001, **p < 0.01, *p < 0.05, ns: non-significant: differences between respondent for each case (Kruskal-Wallis test).
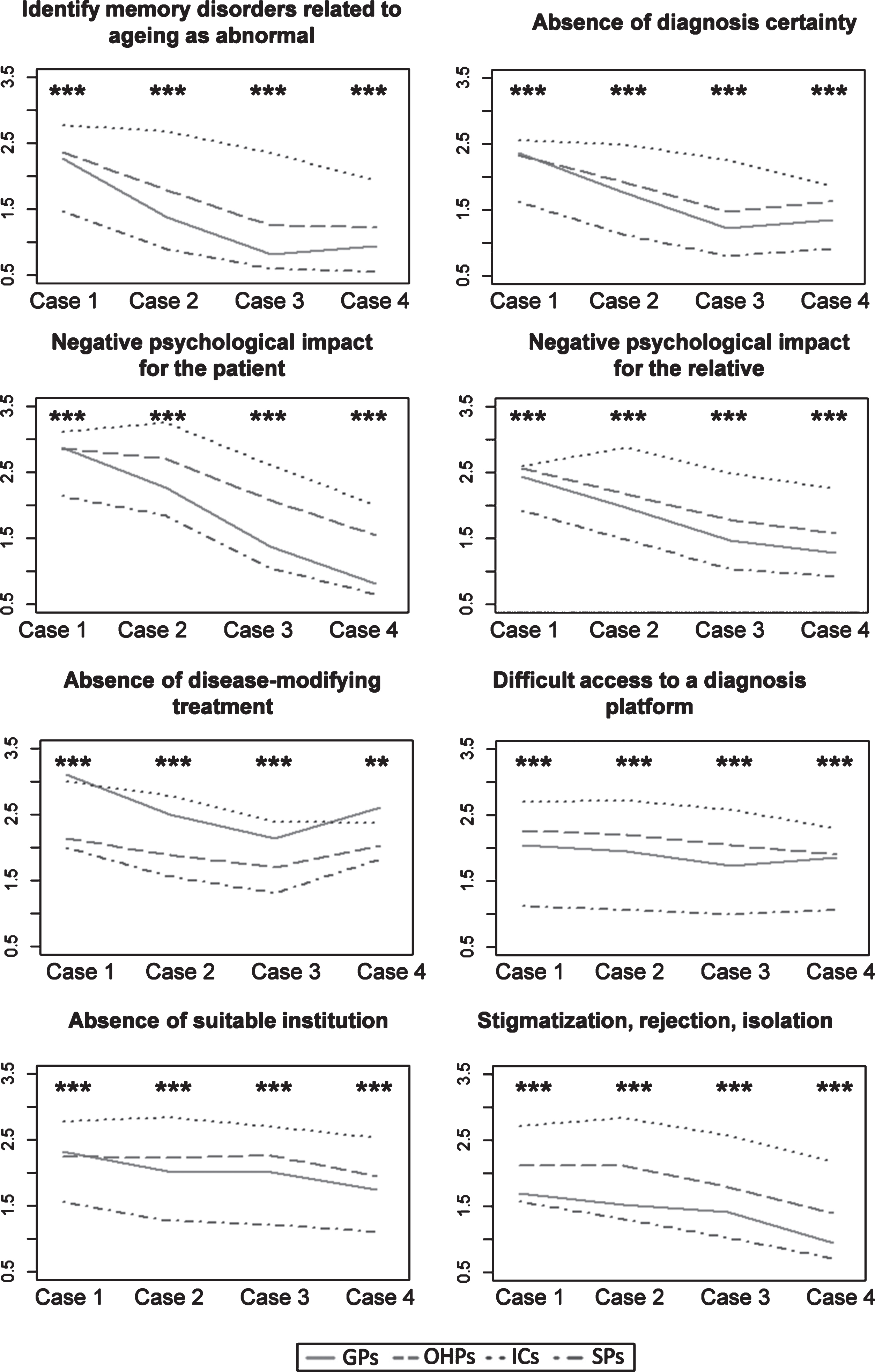
Perception of the eight risks of NCD diagnosis, for each respondent and each case. ***p < 0.001, **p < 0.01, *p < 0.05, ns: non-significant: differences between respondents for each case (Kruskal-Wallis test).
DISCUSSION
The present study found that “patient’s right to know”, “access to medical research”, and “initiation of symptomatic drug treatment” are the lowest perceived benefits; the “negative psychological impact for the patient”, mostly at the earlier stage, the “absence of suitable institution at a specific stage of the disease” and the “absence of disease-modifying treatment” were the highest perceived risks to make an NCD diagnosis.
The “patient’s right to know” was one of the lowest perceived benefits, although this is the general principle of autonomy [27]. The perception of this benefit decreases linearly from case 1 to case 4, similarly between the four groups of respondents. However, from a clinical point of view, respecting the patient’s right to know, whatever the stage of the NCD is the basis of a personalized diagnosis. The low perception of a benefit related to “initiation of symptomatic drug treatment”, particularly in GPs, is, however, understandable in the context of a study conducted in France, as, although symptomatic treatments of AD are still recommended by French scientific and medical societies specialized in NCD, they are no longer reimbursed [28]. Moreover, in France, symptomatic drug treatments are first prescribed by SPs and not by GPs. An interesting point highlighted in the present study was that, while, the “absence of disease-modifying treatment” was one of most important barriers of making a diagnosis, particularly in GPs and ICs, “access to medical research” was among the least important benefits. This seems to be a paradox, in particular as promoting medical research in primary care seems to be one of the main priorities in NCD [29, 30] but barriers to GP’s participation in research are complex and multifactorial [31]. Another point of note is that “negative psychological impact for the patient” was the leading perceived risk of an NCD diagnosis early-on during the course of the disease. This is in accordance with previous studies showing that NCD diagnosis could be accompanied by anxiety, worry, uncertainty, or shock, and sometimes with positive coping responses such as optimism [13, 32–34]. However there is little evidence to support an increase in negative reactions or suicidal risk after disclosure of NCD diagnosis [13, 33–35]. However, after diagnosis, it is reported that patients often feel without support to manage their uncertainties and emotions, and do not know where to turn for support; furthermore, caregivers also report that they do not receive adequate information [16, 33]. Later-on during the course of the disease, the “absence of suitable institution” became a prominent risk. This is in accordance with previous studies and a review previously pointed to the lack of accessible services for patients with NCD, accompanied by financial barriers for family [14].
Taken together, these risks and benefits could be the most interesting to act upon in order to increase the diagnosis of NCD, and we hypothesize that they could be modified. For instance, recognition of the importance of the “patient’s right to know” could be promoted by greater of knowledge about NCD in the general population and in healthcare professionals, particularly by explaining that patients who suffer from NCD are still able to participate in discussions until the advanced stages of the disease, and that the principle of medical ethics, e.g., the “patient’s right to know” are also valid in the context of NCD. To decrease the negative psychological impact for patients and caregivers, intervention strategies could be implemented, such as post-diagnosis psychological support, to create a more caring social context for people with dementia [16, 36]. Promoting medical research in primary care, perhaps with mobile research teams, could also increase the perceived utility of diagnosis of NCD, providing patients with potentially new therapeutic options [29, 30]. In addition, a policy to increase the availability of suitable institutions and support for patients and their relatives could be another lever to promote the diagnosis of NCD. Improve the diagnosis of NCD was an objective of the French national plan on dementia and of the European Joint Action, and a graduated diagnosis strategy tailored to the patient’s needs, clarifying the role of primary and specialty care has been recently proposed [12].
When assessing the differences in the importance of each benefit and risk among the different groups of respondents we found that GPs appeared less sensitive to the “patient’s right to know”, “access to medical research”, and “initiation of symptomatic drug-treatment”; GPs could thereby be the main target of the previously described recommendation. However, although in some reports GPs are portrayed as barriers to diagnosis, and accused of fatalism regarding NCD, with a “deficit model of GPs behavior and attitudes” [8], a growing body of evidence indicates that the attitude of the majority of GPs is not characterized by diagnostic and therapeutic nihilism and GPs are very positive about their key role in NCD care [37, 38]. For many patients, consultations with GPs where they discuss for the first time a cognitive complaint are positive experiences, with feelings of support, familiarity, and confidence. However, secondary care and memory clinics appear unfamiliar, frightening and sometimes depersonalizing, which could increase the negative psychological impact [32]. More attention should be paid to support GPs in the management of complexity and uncertainty of NCD cases, and specifically the dilemmas involved in meeting relatives’ needs for support over long periods [8]. Moreover, an incentive and research assistance could be offered to GPs that are motivated.
Strengths of the present study should be highlighted. This national survey included a large and diverse population. The prototypical clinical cases representing different stages of NCD [22–25] understandable by both medical and non-medical participants, constitutes one originality of this study design. Some limitations must, however, be taken into account when interpreting the results of this survey. Particularly we could not quantify how many received and did not answer the questionnaire because it was sent by many different associations. This could constitute a selection bias.
In conclusion, this study highlights the lowest perceived benefits and the highest perceived risks to make an NCD diagnosis that could be used as potential levers to promote NCD diagnosis. In particular, better knowledge about NCD, availability of suitable institutions, promotion of medical research, as well as implementation of pre-diagnosis and post-diagnosis interventions such as psychological support, could lead to a better personalized diagnosis of NCD, at the right time defined in terms of Kairos and not Chronos.
Footnotes
ACKNOWLEDGMENTS
France Alzheimer Association, National Union of Healthcare Professionals, French Federation of Memory Centers, Departmental Councils of the College of Physicians and Regional Unions of Liberal Doctors which have collaborated. Data of this work are from a survey which was initially made for the end-of-study dissertation for the DIU MA2 course of A. Garnier-Crussard, J. Vernaudon, and N. Auguste. The DIU MA2 course (laquoDiplôme Inter Universitaire de diagnostic et de prise en charge des Maladies d’Alzheimer et Apparentéesraquo) is the French transdisciplinary course on diagnosis and care of Alzheimer’s Disease and related disorders (![]() ) The course is supported by the Fondation Alzheimer and the Fondation Vaincre Alzheimer.
) The course is supported by the Fondation Alzheimer and the Fondation Vaincre Alzheimer.
We thank Philip Robinson (DRCI, Hospices Civils de Lyon, Lyon, France) for help in manuscript preparation.