
Abstract
Background:
Patients with mild cognitive impairment (MCI) show lower decision making and ratio processing abilities as compared to healthy peers.
Objective:
To evaluate whether cognitive training on number processing and/or executive functions improves performance on ratio processing and decision making under risk.
Methods:
In a controlled cross-over study, patients with MCI (n = 23; mean MMSE 26.48, SD 2.43) underwent a week of numerical training followed by a week of executive-functions training (subgroup A), or vice versa (subgroup B). Before training (T1), patients performed experimental tasks of decision making (Game of Dice Task, GDT; Probability-Associated Gambling task, PAG-60 task) and of ratio processing as well as a neuropsychological background assessment. Experimental tasks were also administered after the first (T2) and the second (T3) training week.
Results:
The numerical training and the training of executive functions had a differential effect on experimental tasks of ratio processing. Only the numerical training proved to be effective. The effects of the two training types on decision making under risk were less clear-cut. While no changes over time were observed in the GDT, performance on the PAG-60 task improved in both training subgroups. These improvements were apparent in one subgroup after a period of executive-functions training, in the other subgroup after both training weeks. That means, improvements are not attributable to one specific training type.
Conclusion:
Patients with MCI can profit from a cognitive training on number processing and executive functions. Improvements are reflected in higher ratio processing abilities and more advantageous decisions after training. These results are consistent with assumptions of current cognitive models.
INTRODUCTION
Patients with mild cognitive impairment (MCI) show slight impairments on objective neuropsychological assessment, but criteria for a diagnosis of dementia are not met [1–3]. Patients have to make important decisions with regard to their health status. For example, they have to decide whether to go regularly to medical assessments or to take a prescribed medication. As the prognosis is often unclear, decisions have to be made under high uncertainty. Recent research has shown that patients with MCI perform lower than healthy peers not only in memory, attention, and executive-functions tests but also in decision-making tasks [4–6]. Persons with MCI show difficulties in making advantageous decisions in situations of ambiguity, where important information about options and consequences is missing or misleading, emotional processing is fundamental, and people need to learn from experience which options are the best for them in the long run [4]. Difficulties also emerge in decision making under risk [4, 5]. These are situations where explicit information about options and consequences is offered, and people can rely on reflective processes such as calculation or estimation [7, 8]. Performance of people with MCI on laboratory decision-making tasks resembles to some extent that reported for patients with mild dementia [9, 10]. Recent studies have also described lower performance of patients with MCI relative to healthy controls in a real-life decision-making task [6], as well as in the financial domain [11–13] and a health-related ratio processing task [5, 14]. Lower ability to make advantageous decisions in situations of risk is found to be associated with lower ratio processing abilities and lower executive functions [5]. Interestingly, the way in which health-related information is presented (framing) influences medical judgements of people with MCI more strongly than it happens in healthy people [15].
Recent investigations have attributed an important role to executive functions and numerical processing in decision making under risk [7, 8]. For example, executive functions are needed for categorizing information and options, for developing strategies or retrieving them from long-term memory, for comparing strategies and deciding which one is the most advantageous, for representing, manipulating, and maintaining relevant information in short-term memory, and for generating or initiating an advantageous decision plan [7, 8]. Decision making under risk also requires different numerical abilities, such as understanding numerical information, assessing probabilities, comparing gains and losses, or estimating expected values [7, 8]. Patients with executive deficits choose significantly more high-risk options and therefore make more disadvantageous decisions in decision-making under risk tasks [9, 16–19]. Studies on medical decision making have shown that people with lower numerical abilities are less likely to make advantageous decisions [20]. For example, low numerate people show limited understanding of the risks and benefits associated with a specific medical treatment [21], have less insight into the benefits of a cancer screening [22], or show poor ability in the self-management of chronic diseases [23]. They are also more influenced by the information frame than highly numerate people [24]. As shown by Delazer and colleagues [14, 25], the ability to process and understand ratio concepts such as probabilities, fractions, percentages, and proportions declines with age and is significantly compromised in case of MCI. In healthy people, advantageous decision making is linked to higher executive functions [26, 27] and number processing abilities [28]. It has also been shown that ratio processing acts as a mediator between basic cognitive functions (executive functions, basic mental calculation) and decision making under risk, with higher competence in ratio processing predicting more advantageous decisions [29]. All in all, these findings suggest that increasing numerical understanding and improving executive functions through a targeted cognitive training should facilitate advantageous decision making under risk.
Training in old age can be very effective. Recent studies on cognitive training have indeed reported promising results in healthy participants [30] and in patients with MCI [31]. For example, in the ACTIVE study including 3.000 participants, effects of memory training, reasoning training, or speed-of-processing training were assessed over 10 years [32]. Reasoning and speed training resulted in improved targeted cognitive abilities over 10 years, while memory training effects were less long lasting. However, all three training groups showed a smaller decline after 10 years in self-reported instrumental activities of daily living compared with the control group performing no training [32]. Zehnder et al. [33] reported in a meta-analysis of 24 studies significant effects of memory training in healthy older adults and in patients with MCI. It should be noted, however, that training effects were not specific and were comparable to those found in active control conditions.
The main aim of this study was to assess the relative efficacy of cognitive training of number processing in comparison to training of executive functions on ratio processing and decision making under risk. To our knowledge, no study so far has in fact compared the effects of these two training types on ratio processing and decision making. There are some expectations, though, regarding each of the two training types. Regarding the numerical training, we know from a recent study on healthy people [34] that reasoning about the probabilities, gains/losses, and mean expected values associated with the options of the Game of Dice Task (GDT, modified version) [29] leads to significant improvements in decision making under risk. We therefore hypothesized that decision making under risk should improve after the numerical training. We also have reason to hypothesize that understanding and processing of complex numerical concepts such as ratios would improve through the numerical training [29].
Not only the numerical training but also the training of executive functions might lead to improved decision making. Different executive functions are involved in decision making and support advantageous choices. They are essential for the extraction of information, for deliberation, development, and planning of strategies, and for feedback processing [7, 8]. As outlined by Schiebener et al. [26], general control functions seem to have a key role as they are essential for implementing the calculative and cognitively controlled processes involved in advantageous decision making under risk. General control allows allocating attention according to the task’s rules and goals, and inhibiting interfering signals or automatic responses. Summing up, several studies [8, 29] indicate that improving executive functions should lead to better decision making under risk.
In this study, we aimed at assessing whether a targeted cognitive training would improve performance of a group of patients with MCI on ratio processing and decision making under risk. In a controlled cross-over design, patients performed a numerical training followed by a training of executive functions (or vice versa). We predicted that both trainings should lead to significant improvements in decision making and ratio processing. Whether one of the two trainings has better effects is open for investigation.
In this study, we also assessed possible correlations between performance on experimental tasks (ratio processing, decision making) and neuropsychological background measures. Following results of previous research [8, 29], we expected significant correlations between decision making, numerical processing, and executive functions. Specifically, higher performance in decision making and ratio processing tasks should be associated with higher executive functions and numerical abilities. Whether the patients’ benefits from cognitive training are also related to their cognitive status at baseline will be also investigated.
METHODS
We tested patients with MCI with tasks tapping decision making under risk and ratio processing before and after treatment. Patients also performed a comprehensive neuropsychological background assessment before training. Both a numerical treatment and a treatment of executive functions were applied to each patient according to a cross-over design.
Participants
We recruited 23 patients with MCI at San Camillo Hospital IRCSS, Venice, Italy. They had a mean age of 76.70 years (SD 6.12), a mean education of 10.57 years (SD 3.81), and a mean MMSE score of 26.48 (SD 2.43) [35]. They were evaluated prospectively using standard neurological and neuropsychological testing procedures. Diagnosis of MCI was based on the recently suggested criteria [1, 2]. All patients underwent routine neurological examination including MRI and general medical examination to exclude other causes of possible cognitive alterations. Exclusion criteria were history of major neurological disease (e.g., severe head trauma), psychiatric disease (e.g., major depression), or any other major medical disease that may compromise cognition. The study was approved by the Institutional Review Board of the San Camillo Hospital IRCSS, and informed consent was obtained from all individuals before participation. The study was carried out in accordance with the Declaration of Helsinki for experiments involving humans.
Procedure
Patients were in total tested three times (T1 = before training, T2 = after the first training week, T3 = after the second training week). Between T2 and T3 as well as between T1 and T2 patients performed five consecutive days of training. We used a controlled, cross-over design with patients being randomly assigned to training order A (first week: numerical training, second week: executive-functions training; n = 12) and training order B (reverse order; n = 11; see Fig. 1 for a schematization of the experimental procedure). Patients were not given any detailed information about the differences between the interventions or the expected results. At T1, patients underwent a comprehensive neuropsychological background assessment. They were also tested with decision making and ratio processing tasks (see below for a description). Subsequently, they received the training material with written instructions. Training material and procedure were additionally explained by the examiner. Patients performed the training at San Camillo Hospital IRCSS (each training lasted five days, approximately 20–30 min a day). At T2 and T3, patients were tested on a parallel version of the Probability-Associated Gambling (PAG) task and the ratio processing tasks. The same version of the GDT was used at T1, T2, and T3.
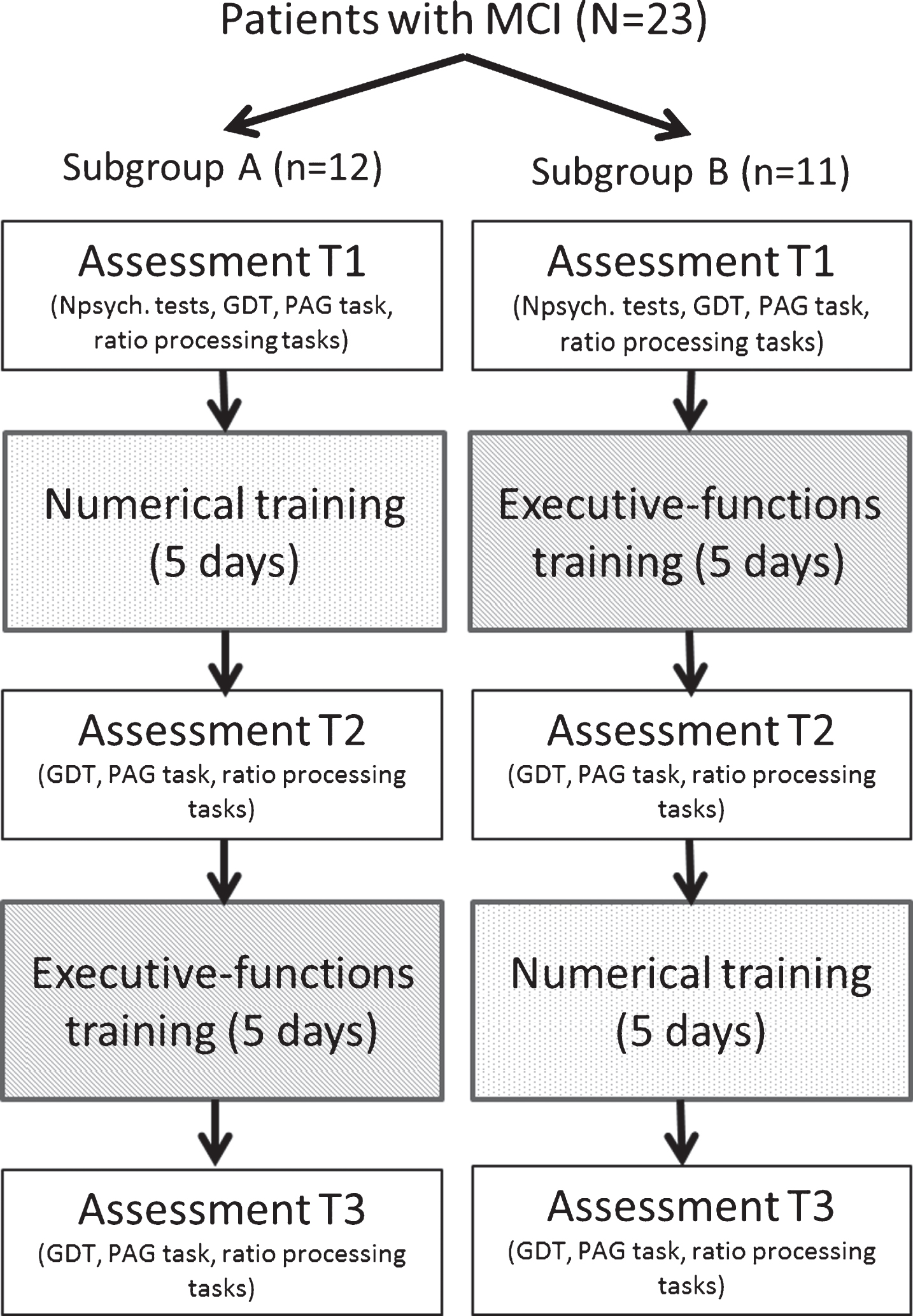
Schematization of experimental procedure.
Neuropsychological background assessment
As part of their clinical evaluation, patients performed a comprehensive neuropsychological background battery including measures of attention, executive functions, reasoning, language, memory, and visuospatial abilities. Additionally, they performed tasks assessing mental complex calculation [25] and number comparison with ratio concepts [6]. They also responded to a self-rated questionnaire on anxiety and depression symptoms [36].
Experimental tasks
Game of dice task
A detailed description can be found in [18]. The GDT is a computerized task which measures decision making under risk. In this task, participants have to maximize their fictitious starting capital of 1000€ within 18 throws of a single virtual die by guessing which number will be shown next. Participants can choose among single numbers (e.g., 3), combinations of two numbers (e.g., 1 2), combinations of three numbers (e.g., 1 2 3), or combinations of four numbers (e.g., 1 2 3 4). Each alternative is associated with a specific winning probability and a specific amount of gain/loss. For example, the single-number alternative is associated with a winning probability of 1/6 and a gain/loss of 1000€. By choosing the single-number alternative, the participant can win 1000€ if the selected number turns up head; otherwise, s/he loses 1000€. Alternatives and associated gains/losses remain visible on the computer screen for the whole duration of the task. Before the task begins, participants are explicitly instructed about rules and gains/losses associated with each alternative but not about which alternative is the most advantageous. In the GDT, the single-number alternative is the most disadvantageous, whereas the four-numbers alternative is the most advantageous. After a choice is made, the computer indicates which number has turned up head, whether the participant has won/lost, the residual capital, and the number of remaining throws. For analysis purposes, we computed the net score by subtracting the number of high-risk choices (selection of single numbers and two-numbers combinations) from the number of low-risk choices (selection of three-numbers combinations and four-numbers combinations). A positive net score indicates a low-risk performance (advantageous behavior), whereas a negative net score indicates a high-risk performance (disadvantageous behavior). Furthermore, we computed the expected value of each single decision as “ (gain×winning probability) – (loss×losing probability)” and then computed the mean expected value (MEV). We also analyzed how often participants selected the single-number alternative and the four-numbers alternative. The same task was used in the three assessment sessions.
Probability-associated gambling task – 60 trials (PAG-60)
This is a modified version of the PAG task [4, 37]. In this task, participants have to decide whether to take a fixed sum of±25€ or to gamble 100€. If the participant chooses the fixed sum alternative, s/he will either get 25€ [+] or pay 25€ [– ] according to what is indicated in a box on the left side of the screen. Differently, if the participant chooses the gambling alternative, s/he will either win 100€ when a red ball is drawn or lose 100€ when a blue ball is drawn. Red balls are winning balls. The winning probability associated with the gambling alternative is indicated by the ratio of red balls to blue balls within a box on the right side of the screen (e.g., red:blue = 6:3; winning probability, pW = 0.67; losing probability, pL = 1 – 0.67 = 0.33). The fixed sum alternative and the winning probability associated with the gambling alternative change from trial to trial so that participants have to adapt their decision strategy to the changing contingencies. The difference between the expected value of the gambling alternative and the fixed sum alternative indicates each time which alternative is more advantageous. For example, in a trial where the fixed sum alternative is +25€ and the winning probability associated with the gambling alternative is 0.67, the expected value of the gambling alternative is “[(0.67×100) – (0.33×100)] = 34€ ” which is higher than the fixed sum alternative (+25€). In this case, gambling 100€ is more advantageous than taking a fixed sum of +25€. Winning probabilities range from 0.30 to 0.70. Presented in a pseudo-randomized order, there are 30 trials where the gambling alternative is more advantageous and 30 trials where the fixed sum alternative is more advantageous (total N = 60 trials). In both conditions (gambling advantageous, fixed sum advantageous), there are two difficulty levels. In easy trials (total n = 24), the difference between the expected value of the gambling alternative and the fixed sum alternative is large; here, participants should easily recognize which alternative is more advantageous. By contrast, difficult trials are characterized by a small difference (total n = 36). Difficult trials can be subdivided in congruent (total n = 24) and incongruent trials (total n = 12). In congruent trials, it is advantageous to gamble in case of more red balls than blue balls, while it is advantageous to take the fixed sum in case of more blue balls than red balls. Incongruent trials require exactly the opposite. In incongruent trials, participants cannot rely exclusively on the ratio of red balls to blue balls but have also to take into consideration the fixed sum alternative in order to make advantageous decisions. Perceptual aspects are also controlled for. In half of the difficult (congruent) trials as well as in half of the easy trials, the numerically larger set is smaller in cumulative surface area. On the other half of the trials, the numerically larger set is also larger in cumulative surface area. In this modified version of the PAG task, no feedback is given to participants (i.e., no ball is actually drawn). Participants do not know whether they win or lose after choosing the gambling alternative, nor do they receive any information about their actual capital. In each trial, participants have 8 s to make a decision. In total, task duration is ca. 7 min. We prepared two versions of the task, which differed from each other with respect to the presentation order of the trials. Administration of these two versions was counterbalanced between participants and sessions. For analysis purposes, we evaluated the percentages of advantageous decisions (i.e., correct answers) made in each condition (gambling, fixed sum) without taking into account the difficulty level.
Ratio processing tasks
Patients performed two ratio processing tasks. The first task (health-related ratio processing task) is an adapted and expanded version of the numeracy scale by [38]. A detailed description can be found in [14, 25]. In this task, participants are required to convert percentages, compare proportions, add or subtract a defined percentage, or show understanding of a dosage instruction as given in a short patient information leaflet (n = 12 items). Questions are embedded in a health-related context. Answers are given orally (time limit is set at 45 s per items). Four parallel versions of the task were prepared (version 1 and version 1b: identical items but different item order; version 2 and version 2b: identical items but different item order; different ratios were used in versions 1-1b versus versions 2-2b). Presentation order of the four versions was counterbalanced across participants and sessions.
In the second ratio processing task (calculation with ratios task), participants are required to compute percentages (e.g., how much is 1% of 200?) and proportions (e.g., how much is 3/4 of 32 m2?) as well as to convert proportions in percentages (e.g., 100 out of 1000 corresponds to ___%) and vice versa (13% corresponds to ___ out of 1000). Participants are given 10 min time to complete the task (n = 14 items) and can use paper and pencil to compute solutions. Three parallel versions of the task were prepared; presentation order was counterbalanced across participants and sessions. The percentage of correct answers obtained in both ratio processing tasks was submitted to analysis.
Cognitive training
Numerical training
In the first two sessions, participants had to link percentages and frequencies to pictographs, and to convert frequencies to percentages and vice versa (e.g., 75 out of 1000 = ___%). In the third session, they performed comparison tasks with symbolic (frequencies, percentages) and non-symbolic (pictographs) representations, where they had to specify which of two frequencies, percentages, or pictographs indicated the larger value (e.g., what is larger: 75% or 84% ?). In the fourth session, tasks regarded the comparison of decimals and fractions, and the conversion of decimals into fractions and vice versa. In the last session, participants had to compute discounted prices knowing the full price and the percentage of discount. Each training session contained two levels of difficulty (easy items, difficult items). All participants performed the easy items; difficult items were optional (however, the majority of participants also trained on difficult items).
Executive-functions training
In each of five sessions, participants received five different tasks: phonological verbal fluency, semantic verbal fluency, set-shifting, word scramble, and figural fluency. In the phonological verbal fluency task, they had to write down as many words starting with a specific letter (e.g., B) as possible. In the semantic verbal fluency task, they needed to write down as many exemplars within a specific category (e.g., food) as possible. In the set-shifting task, participants had to alternate between words starting with different letters (for example, they had to write down first a word starting with L, then a word starting with S, then again a word with L …). Time limit to perform the first three tasks was set at 6 min. In the word scramble task, participants were presented with two different words (e.g., “girasole”, “piattaforma”) and were required to form new words by using only the letters of the given word (time limit: 4 min). In the figural fluency task, participants received squares containing five points and were required to connect them by means of straight lines by creating as many different patterns as possible (time limit: 2 min). In all tasks, repetitions were not allowed. In the phonological verbal fluency tasks, proper names had to be avoided.
Statistical analysis
Statistical analysis was performed by using SPSS 24.0 for Windows. Subgroup A and B were compared to each other by means of Mann-Whitney U-test or Chi2-test where appropriate. Performance changes over time were analyzed by means of Friedman tests and, in case of significant results, by means of Wilcoxon tests. A Spearman rank-order correlation analysis was carried out to investigate the relation of performance on experimental tasks (GDT, PAG-60, ratio processing) at T1 with neuropsychological measures of executive functions, abstract reasoning, and numerical processing. A further correlation analysis was performed for the two subgroups separately to investigate the relation of performance changes over time (T2 minus T1) and neuropsychological variables. Significance was set at α= 0.05.
RESULTS
Demographical characteristics
Mann-Whitney U-tests showed that subgroups A and B had comparable age and education (see Table 1 for medians, interquartile ranges, and p-values). A Chi2-test indicated that the two subgroups had also a comparable gender distribution.
Demographical information about subgroup A (training order: number processing – executive functions) and subgroup B (executive functions – number processing)
IQR, interquartile range; aMann-Whitney U-test; bChi2-test.
Neuropsychological background assessment
Subgroups A and B were compared to each other by means of Mann-Whitney U-tests. We found no significant differences between them in any neuropsychological tests (see Table 2 for medians, interquartile ranges, and p-values). Importantly, at T1, subgroups did not differ from each other in any decision making and ratio processing tasks, all p > 0.1.
Performance on neuropsychological background tests of subgroup A (training order: number processing – executive functions) and subgroup B (executive functions – number processing)
IQR, interquartile range. Group comparisons were carried out by means of Mann-Whitney U-tests.
Game of dice task
Descriptive statistics are reported in Table 3. Friedman tests were performed for the two subgroups separately to investigate changes in performance over time. Results indicated no significant changes between sessions for either subgroup in any GDT measures, all p > 0.1. We also found no significant results when we carried out Friedman tests on the whole patient sample to examine whether, independently of the training type, performing a cognitive training could lead to any changes in the GDT over time.
Performance on the Game of Dice Task of subgroup A (training order: number processing – executive functions) and subgroup B (executive functions – number processing)
MEV, mean expected value; IQR, interquartile range; T1, before training; T2, after the first training week; T3, after the second training week. Group comparisons were performed by means of Mann-Whitney U-tests.
PAG-60 task
Friedman tests indicated significant differences between sessions for both subgroups in the fixed sum condition, both p < 0.05 (Fig. 2a). Results were not significant in the gambling condition, both p > 0.1 (Fig. 2b) 1 . Post-hoc comparisons were performed by means of Wilcoxon tests. There was a significant improvement for subgroup A from T1 to T3, Z = – 2.94, p < 0.01. Other contrasts (T1 versus T2, T2 versus T3) were not significant, both p > 0.1. For subgroup B, there was a significant improvement from T1 to T2, Z = – 2.19, p < 0.05. The contrast T1 versus T3 was also significant, Z = – 2.09, p < 0.05, while the contrast T2 versus T3 was not, p > 0.1.

PAG-60 task. Percentage of correct answers as a function of session and subgroup: a) fixed sum condition; b) gambling condition. T1, before training; T2, after the first training week; T3, after the second training week; subgroup A, first week: numerical training – second week: executive-functions training; subgroup B, first week: executive-functions training – second week: numerical training.
Ratio processing tasks
Friedman tests were performed on the percentage of correct answers given at T1, T2, and T3 in both ratio processing tasks (Fig. 3). For both subgroups, we found significant results, both p < 0.05. Wilcoxon tests indicated a significant improvement for subgroup A from T1 to T2, Z = – 2.48, p < 0.05. The contrast T1 versus T3 was also significant, Z = – 2.04, p < 0.05, while the contrast T2 versus T3 was not, p < 0.1. For subgroup B, we found no difference from T1 to T2, p > 0.1, but a significant improvement from T2 to T3, Z = – 1.96, p = 0.05. The contrast T1 versus T3 was also significant, Z = – 2.58, p < 0.05.

Ratio processing tasks. Percentage of correct answers as a function of session and subgroup. T1, before training; T2, after the first training week; T3, after the second training week; subgroup A, first week: numerical training – second week: executive-functions training; subgroup B, first week: executive-functions training – second week: numerical training.
Healthy controls without training
In order to assess possible effects of repeated testing, 25 healthy adults (mean age 41.68/SD 21.21 years, mean education 13.80/SD 2.25 years) performed a modified version of the GDT [29] and both ratio processing tasks in total three times. As for the patients with MCI, the second evaluation took place a week after the first one, the third evaluation a week after the second one. Healthy participants did not perform any training between testing sessions. Friedman tests showed no performance improvement over time in any decision making or ratio processing measures (Table 4), all p > 0.1. We found no significant results even when individuals performing at ceiling during the first assessment (GDT-D: n = 7; ratio processing: n = 9) were excluded fromanalyses.
Performance on a modified version of the Game of Dice Task and on Ratio Processing Tasks of a group of healthy adults who did not perform any trainings
MEV, mean expected value; IQR, interquartile range; T1, first assessment; T2, second assessment after a week; T3, third assessment after an additional week.
Correlation analysis
In a first step, we computed a Spearman rank-order correlation analysis between performance at T1 of the whole patient group on experimental tasks and neuropsychological measures. As measures of decision making, we entered the mean percentage of advantageous decisions in the fixed sum condition of the PAG-60 task and the number of four-numbers selections in the GDT. As measure of ratio processing, we used the percentage of correct answers given in both ratio processing tasks. Table 5 reports results of this correlation analysis. We found that better decision making in the PAG-60 task was associated with better selective attention. Also, higher ability in ratio processing was associated with higher number processing abilities and better attention and executive functions. Other correlations were notsignificant.
Coefficients of a Spearman rank-order correlation analysis computed for performance of the whole patient sample at T1
*p < 0.05, **p < 0.01, ***p < 0.001. (1) PAG-60 task (fix sum condition, advantageous decisions), (2) GDT (four-numbers selections), (3) Ratio processing tasks (correct answers), (4) Phonemic verbal fluency, (5) Stroop task (interference inhibition, s), (6) Attentive matrices, (7) Digit span backward, (8) Raven Progressive Matrices, (9) Mental complex calculation, (10) Number comparison with ratios.
In a second step, we computed a Spearman rank-order correlation analysis for the two subgroups separately between neuropsychological measures and performance changes over time (T2 minus T1) in the PAG-60 task (advantageous decisions in the fixed sum condition) and ratio processing tasks (percentage of correct answers). We did not enter any measures of performance changes in the GDT as for this task we did not find significant differences between subgroups. Results are reported in Table 6. We found no significant correlations for subgroup A. For subgroup B, we found that improvements in ratio processing tasks were higher for people with lower calculation abilities at T1. When we excluded the patients who performed at ceiling in calculation at T1 (n = 2), this correlation was not significant anymore, p = 0.150. Other correlations were notsignificant.
Coefficients of a Spearman rank-order correlation analysis computed for the two subgroups separately between performance changes in experimental tasks (T2 minus T1) and neuropsychological measures
*p < 0.05. (1) Performance changes in the PAG-60 task (fix sum condition, advantageous decisions), (2) Performance changes in ratio processing tasks (correct answers), (3) Phonemic verbal fluency, (4) Stroop task (interference inhibition, s), (5) Attentive matrices, (6) Digit span backward, (7) Raven Progressive Matrices, (8) Mental complex calculation, (9) Number comparison with ratios.
DISCUSSION
In this study, we found that the two training types (“numerical training”, “executive-functions training”) had a differential effect on experimental tasks of ratio processing. Only the numerical training proved to be effective. The effects of the two training types on decision making under risk were less clear. While no changes over time were observed in the GDT, performance on the PAG-60 task improved in both training subgroups. These improvements were apparent in one subgroup after a week of executive-functions training, in the other subgroup after both training weeks. That means, improvements are not attributable to one specific training type. In sum, patients with MCI could profit from cognitive training. Likely, numerical abilities and executive functions improved through training which in turn had a positive effect on performance in untrained tasks of ratio processing and (partly) on decision making. Following cognitive training, patients likely could understand ratio concepts in a health-related context better, could solve problems with ratios more correctly, could estimate winning probabilities better and make more advantageous choices.
Results of this investigation show that the numerical training had a positive and specific effect on performance in untrained ratio processing tasks. This finding is of importance as ratio concepts are essential in dealing with every-day situations, such as estimating price reductions, mortgage rates, or – in the health context – the risk of side effects or the probability of recovery. We assume that the numerical training leads to better and more accurate processing of numbers and calculation. However, the effects of numerical training may go beyond this aspect. As reported by Peters and colleagues [39, 40], people with higher numeracy pay more attention to numbers, accept numbers as a useful source of information, and rely on numerical information more than on other information. Thus, the effects of numerical training may be manifold. It may improve the ability to process numbers and to calculate. Moreover, it may enhance attention to numerical information. Paying more attention to numerical concepts may also result in improved performance in ratio processing tasks.
There are reasons to believe that the performance improvements of patients with MCI in untrained tasks of ratio processing and (partly) on decision making were related to cognitive training and not to effects of repeated testing. A group of healthy participants was tested three times with a modified version of the GDT [29] and both ratio processing tasks but received no training in-between. For them, we found no significant performance differences over time in any tasks. Future studies might further investigate the beneficial effects of training on decision making and ratio processing by, for example, comparing the effects of cognitive training with the effects of a non-cognitive training (e.g., physical activity or meditation).
In line with previous studies [8, 29], in this investigation we found that better decision making under risk correlated with better selective attention. Also, higher ratio processing abilities correlated with higher numerical abilities and better attention and executive functions. A correlation analysis carried out for the two patient subgroups separately between training-related performance improvements in experimental tasks and neuropsychological measures showed no relevant results, possibly due to the small sample size.
Decision making under risk can be based on reflective processing such as calculating probabilities, comparing options, or planning consecutive choices. However, intuitions and emotions as well as the use of heuristics, strategies, and metacognition can also guide decision making under risk. Some authors suggest that reflective processing and intuitive processing interact and inform each other, and that advantageous decision making relies on both, intuitions and reflections [8, 42]. For example, the model by Schiebener and Brand [8], which is mostly based on evidence collected through the GDT, proposes that a reflective mode and an impulsive mode are activated in parallel during decision making. One mode is triggered as the leading one, and individual predispositions as well as situational conditions influence which processing mode is leading (this choice can be modified at any stage of the decision process). The reflective mode includes processes such as cognitive control, deliberation, planning, and ratio processing. The impulsive mode regards intuitions, impulses, emotions, and feelings. These modes can interact with each other, and both can lead to evaluation of options and eventually to a decision. After a decision is made, the feedback is processed influencing which mode is triggered as the leading one in the next decision process.
In decision making under explicit risk conditions, people principally can make decisions based on the available information about options and consequences without needing a feedback. However, studies have shown that the presence of immediate feedback considerably influences the decision-making behavior. Some authors have observed increasing risk taking behavior after negative feedback [43]. Others have reported more frequent high-risk decisions in a version of the GDT without feedback in comparison to the standard version of the GDT [44]. This was in particular evident in individuals with lower logical thinking abilities, whereas persons with excellent logical thinking abilities showed to be not affected by the presence or absence of the feedback [45]. Importantly, the feedback is not only processed cognitively but also emotionally. For example, Figner and colleagues [46] described higher risk taking and higher skin conductance responses, which are a marker of bodily emotional reactions, in the “hot” version of the Columbia Card Task (participants turn cards themselves and receive immediate feedback) as compared to its “cold” version (participants only indicate how many cards they would like to turn but do not receive any feedback). Figner and colleagues [46] argued for a competition between affective processes and deliberative processes, with the affective system tending to override the cognitive system in situations where positive feelings about risk taking can develop. It has also been suggested that individual differences in cognitive abilities may influence not only whether feedback impacts performance [45] but also which strategies people may prefer to apply in decision making [47]. While individuals with good cognitive functions seem to prefer more rationally guided decision-making strategies, individuals with poorer cognitive functions tend to rely more on intuitions and to profit from the presence of feedback [47].
In this study, patients showed significant performance improvements following training in the PAG-60 task, while changes in the GDT did not reach significance. Both these tasks assess decision making under risk. They offer explicit information about the decision situation and require abilities such as evaluation of options, probability estimation, comparison of benefits and costs, and selection of an option. In the PAG-60 task, two options are presented, the decision situation changes from trial to trial, and no feedback is given. Differently, the GTD offers several answer alternatives associated with specific winning probabilities and gains/losses, stable rules, and feedback. Thus, task differences, in particular the presence or absence of feedback, might have influenced on which processes people relied during decision making and the extent to which cognitive training on numbers and executive functions was effective. As the PAG-60 task does not offer any feedback, people may rely exclusively on reflective processing, such as ratio processing, to make advantageous decisions. It is therefore plausible that improvements in number processing and executive functions result in significant performance changes in this task. Differently, in the GDT, people may learn from feedback whether an option is advantageous and may adjust their decision strategy consequently. Here, both reflective processing and intuitive processing can be engaged in decision making. As in this task people do not necessarily and exclusively rely on reflective processing, improvements in decision-making performance following a cognitive training targeted to enhance reflective processes might be less evident.
It is also possible that, to improve performance of patients with MCI on the GDT, a tailored intervention program is needed. A recent study has shown that, in healthy participants, explicit advice about the advantageous alternatives of the GDT results in higher performance [48]. A further study with healthy people that used a modified version of the GDT [29] has reported higher performance for participants who are forced to reason about the task’s contingences relative to participants who receive usual instructions [34]. Patients with MCI might show more evident improvements of performance in the GDT when explicit advice about the advantageous options is given or when they are explicitly instructed to reason about the task’s options and consequences. Future studies should investigate the effects of explicit advice and reasoning on decision making under risk in patients with MCI.
Although results of this study seem promising, the transfer to real-life situations has yet to be evaluated. As shown in previous studies, executive functions predict performance on everyday life activities [49], and effects of executive training seem to have a high relevance for instrumental activities of daily living [32, 50]. Since patients with MCI are repeatedly confronted with medical information (as in the tasks used here), an improvement in ratio processing should have an immediate positive effect. Whether the effect also extends to every-day decision making has to be assessed in future studies. Furthermore, in this study, we assessed short-term effects of cognitive training. Other studies have revealed significant long-term effects of cognitive training over ten years in healthy participants [32]. Whether such a long-term effect can also be achieved in patients with MCI depends, among other factors, on the development of the underlying disease, some patients being stable over several years, others developing dementia.
We indicate two possible limitations of our study. First, our sample size for both subgroups was small and this might have underpowered the specific effects of training type on decision-making tasks. Second, we had no “active” control group performing, for example, a non-cognitive assignment between assessment sessions (e.g., a progressive muscle relaxation exercise). This condition might help investigating possible additional positive effects of being aware to undergo a (presumably effective) treatment. We firmly believe that our results about the specific effects of training type in ratio processing tasks cannot be simply reduced to such effects. A new more comprehensive study might wipe out even the most resilient skepticism on this regard.
Our study shows for the first time positive effects of cognitive training on decision making and ratio processing in patients with MCI. In conclusion, we suggest that a targeted cognitive training on numbers and/or executive functions may be beneficial for patients with MCI. It may enhance their understanding of and performance with complex numerical information as well as their ability to make advantageous decisions under risk. This type of intervention could be relevant for improving the patients’ informed and advantageous decision making in the health context.
Footnotes
ACKNOWLEDGMENTS
We thank all patients for their participation in the study. We also thank Roberta Toffano and Roberta De Mitri for their help with the data collection.
This work was supported by San Camillo Hospital IRCCS, Venice, Italy, and by Medical University of Innsbruck, Austria (MUI-Start 2014-05-001).
Results regarding the gambling condition were not significant even when the analysis was performed on the whole patient sample.