
Abstract
Background:
Alzheimer’s disease (AD) is the most prevalent cause of dementia with vascular dementia (VaD) being second alongside with mixed AD and VaD, according to some. For some time, it has been proposed that cardiovascular disease (CaVD), hypertension, and diabetes mellitus (DM), which are known risk factors for VaD, also are associated with and contribute to the development of AD.
Objective:
The aim of this study was to investigate the prevalence of these proposed general risk factors, and to document presence of CaVD as evidenced from clinical records or from autopsy findings, further to correlate these with the diagnoses AD, VaD and mixed AD-VaD (MD), respectively.
Methods:
Autopsy reports at the Clinical Department of Pathology in Lund from 1992–2017 were analyzed. All cases with a complete autopsy report and a neuropathologically diagnosed dementia disorder (AD, VaD, or MD) were selected on the condition of a clinical diagnosis of dementia. Clinical data were retrieved through medical records and the Swedish National Diabetes Register (NDR). A total of 268 subjects were included.
Results:
In AD, there was less CaVD as significantly less organ/tissue findings (p < 0.05), significantly less hypertension (p < 0.001), and likewise significantly less DM (p = 0.0014) than in VaD, with the MD group results being set between these two in all aspects studied.
Conclusion:
AD and VaD exhibit such different profiles of organ and vascular damage as well as of hypertension and DM that they clearly point toward different pathogenic origin with low likelihood of shared risk factors.
Keywords
INTRODUCTION
Dementia (or major neurocognitive disorder [1]) is a major health concern worldwide and a growing problem. It is estimated that around 50 million people suffer from dementia and since it is a disease among the elderly, and since this age group is set to almost double in the next 30 years, it is projected that there will be around 82 million people with dementia in 2050 [2]. Among the dementing disorders, Alzheimer’s disease (AD) is the most prevalent of all, contributing to 40–70% of cases [2–8]. AD is neuropathologically defined, besides an atrophy accentuated in the medial temporal lobe, including the amygdala and hippocampus, as a neurodegeneration with neuronal disease and loss and the accumulation of pathological tau protein and amyloid-β in the brain tissue as well as presence of amyloid deposits in the blood vessels [9].
Recently, it has been suggested that apart from the previous risk factors such as age and family history [9], risk factors for developing AD also include cardiovascular disease (CaVD) [10–12], cerebrovascular disease (CeVD) [13–15], diabetes mellitus (DM) [16, 17], and hypertension (HT) [12, 16]. This means that these newly proposed risk factors are the same for AD as for vascular dementia (VaD) [9], which is considered a brain disorder where cerebrovascular pathologies are responsible for the cognitive impairment [18] in the absence of other pathologies [9]. VaD contributes to almost 20% of dementia cases and is claimed to be one of the most prevalent dementing diseases after AD [6, 19].
A third form of dementia, mixed AD-VaD dementia (MD), is defined through a combined pathology with the amyloid plaques, neurofibrillary tangles, and neuronal loss of AD, and ischemic lesions (CeVD) [20]. Hence the diagnosis of MD is made when the findings of both AD and VaD are judged severe enough to have contributed to the cognitive impairment. In MD, it is not all clear how the different pathologies contribute to the cognitive impairment, as studies argue both for a synergistic and/or additive effect of the AD and VaD pathology [18, 20]. Because MD is a disease of two different brain disorders combined, one may anticipate difficulties in clinically diagnosing MD correctly. This is also shown in studies in which an autopsy was performed on clinically diagnosed AD and VaD cases, which were in fact proven to be neuropathologically defined MD [21–23]. There are also reports claiming that MD is the most common form of dementia as most cases of both AD and VaD have mixed pathologies [24].
DM has been associated with increased risk of cognitive impairment [25]. However, the reason for this association is unclear. One study showed that there was an increased risk of developing AD among those with higher insulin levels, with or without DM [26], whereas in one study it was suggested that the vascular damage regularly accompanying DM could be the cause of cognitive impairment or dementia [10].
In the same way as for DM, the correlation between HT and AD is not fully established. In the Honolulu-Asia Aging study (a large epidemiological study without neuropathologic diagnosis verification), there was an increased risk of AD among subjects with untreated HT at mid-life [27], but in another report from the Cardiovascular Health Study, no relation was found between HT and risk of AD [28]. Furthermore, studies of blood pressure in older subjects indicate that both low and high blood pressure affect cognitive performance negatively [10].
In this study, we compared the neuropathological dementia diagnoses and autopsy findings of CaVD and CeVD along with the prevalence of clinically diagnosed DM and HT in AD, VaD, and MD. There is to our knowledge no other study in which autopsy-observed findings of atherosclerosis in the coronary arteries and aorta have been compared in detail in neuropathologically confirmed subtypes of dementia.
The aim of the study was to investigate the correlation of the alleged shared dementia risk factors CaVD, DM, and HT and their prevalence in AD, VaD, and MD, respectively. This is essential for the assessment of risk calculations, treatment and prevention strategies for the prevalent specific subtypes of dementia.
MATERIAL AND METHODS
Study design
In this retrospective observational study on individuals with dementia, deceased, and subject to autopsy in Lund, Sweden between 1992 and 2017, we analyzed findings of CaVD and CaVD risk factors, as reported in: 1) the autopsy reports from the Department of Pathology in Lund, using the database system SymPathy, in which the referrals and all macro-and microscopical autopsy findings are assembled and stored; 2) the clinical records, as available at time of autopsy and afterwards, through the local medical records, which were attained through the net-based clinical record system Melior (for years from 1997) and through the Regional Archive of stored records in Lund (for the time before 1997); and 3) the Swedish National Diabetes Register (Gothenburg Sweden).
An approval from the Regional ethical review board, Lund University was obtained for this study, dnr 944–2017.
Subjects
All known cases of dementia neuropathologically diagnosed in Lund between 1992 and 2017 were searched (n > 1,200 individuals, averaging 50 / year). All diagnoses except “clean” AD, VaD, and MD were excluded (e.g., frontotemporal dementia, Lewy body disease, and cases with admixture of other brain pathology than the dominating/named disease), as were cases with irretrievable or insufficient clinical data. A clinically diagnosed dementing disease (by a specialist in cognitive disorders or by a general practitioner) was a prerequisite for inclusion, as well as a performed comprehensive neuropathological examination. We thus excluded individuals with clinically unknown (not established diagnostically) dementing disorder and we excluded cases for which the neuropathological examination had been limited to a minor investigation of only a few brain regions.
The primary neuropathological investigations had resulted in confirmation, partial confirmation, or refutal of the subtype diagnoses and were performed by one pathologist, whereas the general autopsy had been performed by many different pathologists from the department. The procedures of brain investigation have been thoroughly described in a previous publication [23] and is in brief an extensive examination of the entire brain, covering not only specified small sampling areas but entire lobar regions on small and whole-brain coronal sections. The stainings used are similarly described earlier [23], include hematoxylin-eosin and myelin stains, Congo red for amyloid, Silver stains Campbell, and modified Gallyas for neurofibrillary degenerative components and plaques, as well as immunostainings against phosphorylated tau, amyloid-β and further against alpha-synuclein pathology, in order to exclude admixture of Lewy body disease in these cases.
Pathology definitions of dementia subtypes
The AD diagnosis was primarily established in adherence with internationally accepted criteria [29, 30] and later ascertained to adhere to the later appearing, more comprehensive criteria of the National Institute on Aging /Reagan Institute from 1997 [31]. AD pathology as reflecting clinical dementia disease was defined by brain tau neurofibrillary tangle pathology of Braak stage III or more [32], without any traits of VaD or other disease. Braak stage of III is generally considered as associated with cognitive impairment, whereas lower stages are not consistently associated with cognitive impairment [9]. The neuropathological difference between stages II and III is recognized as a progression of pathology from the hippocampus and entorhinal cortex (stage II) to the limbic allocortex and adjoining neocortex [32]. It is acknowledged that amyloid-β plaque pathology in general accompany that of the tau pathology [33] as well as with amount of neuronal degeneration and cell loss [34].
VaD patients were defined as having clear signs of vascular-ischemic pathology (several focal infarcts, ischemic white matter rarefaction, vasculopathy of arteriosclerotic or hypertensive type, or neurons regionally reduced in number and pycnotic, while having minimal and regionally restricted AD changes (at most Braak stage II) [35], or, as often: none.
The MD group was defined as having a significant vascular component as well as a significant component of AD pathology (Braak stage of III or more), this because of the considerations that both pathologies should be severe enough to contribute to the clinical disease [21, 36]. Cases with substantial vascular component and complete absence of AD components or at most a Braak stage of I or II (i.e., minimal neurodegenerative changes) were defined as VaD [32].
Pathological data
The severity of atherosclerosis in the coronary arteries and the aorta was assembled from the autopsy reports. It is general routine to dissect these blood vessels and to observe the presence and degree of atherosclerosis, as by a sum impression of number of plaques, degree of calcifications in these plaques, degree of vascular stenosis, or aneurysmal changes. The pathologists all used similar terms for reporting the severity degree of sclerosis and therefore each subject’s atherosclerosis degree was converted in to a scale between 0 and 3 (based on the described severity of the findings). The carotid arteries and the circle of Willis were not assessed with the same consistency in the primary reports and were hence not being subject to grading and specific comparisons.
We used the following grading system for atherosclerosis in the coronary arteries: 0 - No atherosclerosis; 1 - Mild atherosclerosis; 2 - Moderate atherosclerosis; 3 - Severe atherosclerosis, or mentioning of stenosis.
We used a similar grading system for atherosclerosis in the aorta: 0 - No atherosclerosis; 1 - Mild atherosclerosis; 2 - Moderate atherosclerosis; 3 - Severe atherosclerosis, or mentioning of aneurysm.
In addition, information about presence of myocardial infarction, myocardial hypertrophy on autopsy, organ weights of the brain and heart, nephrosclerosis and the presence of atherosclerosis in the brain vessels were also collected from the autopsy reports. Of these parameters, the myocardial hypertrophy, an increased heart weight (≥500 g) and nephrosclerosis more or less as a rule connote HT [37–41]. These factors were thus noted but did not count alone, without notion of clinical HT. Because of the wide range of what is considered normal heart weight among the general population [42–44], and to prevent over analysis, we decided that a weight≥500 g would be interpreted as pathological.
Intracerebral hypertensive angiopathy (HTA) was noted, if present in the autopsy reports. HTA is highly associated with HT [45] and exhibits specific microstructural details.
Clinical data
The information regarding presence of DM was assembled through 1) the database clinical records and 2) the Swedish National Diabetes Register (NDR) for subjects which were autopsied between 1997 and 2017 and through archival medical records for subjects autopsied between 1992 and 2017. Only presence or absence of DM diagnosis were taken into account and not type of DM nor choice of treatment or age at onset. The subjects were assumed to be free of DM disease if no documentation regarding DM was found through the NDR or in the medical records.
Concerning the presence of HT, information regarding individuals autopsied before 1997 was accessed through medical records and for those autopsied after 1997 information was collected from medical journals and the NDR. A cut off for HT was decided at a blood pressure≥140/90, which is the general limit according to recent guidelines [46]. All subjects with either reported HT or anti-hypertensive treatment were defined as having at least a blood pressure of≥140/90. Choice of anti-hypertensive treatment was not considered. The subjects were considered to have had HT if HTA was reported in the autopsy reports, even if the diagnosis was not mentioned in the medical records or in the NDR. If no documentation of HT was found nor presence of HTA on autopsy was described, the subjects were assumed to be free of this diagnosis.
Additionally, a history of myocardial infarction and CeVD through the NDR and medical records were also considered/noted.
Data analysis
The statistical analyses were done using IBM SPSS Statistics 25. Concerning HT, DM, myocardial hypertrophy, prevalence of myocardial infarction, heart weight, and nephrosclerosis, the three groups were compared using crosstabs and Pearson Chi-Square test was used to test for significance and to investigate the variance in prevalence between the groups. A p-value of 0.05 was considered statistically significant. If a difference was found to be significant when testing the three groups, the same analysis was made to compare each dementia group; AD with MD, AD with VaD, and MD with VaD. Because several statistical tests were being performed simultaneously, adjustment of the level of significance was done using the Bonferroni correction. As three consecutive tests were performed the level of significance (0.05) was divided by 3 (0.005/3 = 0.017). No statistical analysis was made regarding atherosclerosis of either the aorta or the coronary arteries as these findings were based on subjective interpretations from different pathologists, converted to a scale. A statistical test concerning these findings would mean a risk of a spurious conclusion of these results.
RESULTS
Subjects
The resulting sum of cases suitable for analysis was 268 individuals, including 81 cases of AD, 106 cases of VaD, and 81 cases of MD. For demographic data on the three groups, collected from the autopsy reports, see Table 1.
Demographics for all subjects and the three subgroups AD, MD, and VaD
AD, Alzheimer’s disease; MD, mixed dementia; VaD, vascular dementia.
Presented in median years, interquartile range within brackets.
CaVD parameters from autopsy: aortic sclerosis, coronary sclerosis, myocardial pathology, heart weight, nephrosclerosis, and intracerebral hypertensive angiopathy
Data on the CaVD parameters from autopsy were obtained in most of the cases (Table 2), with singular exceptions regarding both heart and vessel pathology, while reports on renal macroscopic appearance, for potential nephrosclerosis, was lacking in 32% of the AD group, in 22% of the MD group, and in 8% of the VaD group.
Obtainable data for each variable in the dementia groups. Micro- and macroscopical findings (white background) and clinical data (grey background)
AD, Alzheimer’s disease; MD, mixed dementia; VaD, vascular dementia. Percentage within brackets.
For the severity of coronary sclerosis, there was a marked numeric difference between the AD and the VaD group as well as between the AD and the MD group (Table 3). Most patients with a severity grade of 0 and 1 was found in the AD group while severity of grade 2 was most prevalent in the MD group and patients with severity grade of 3 was most common among those with VaD.
Prevalence of the studied cardiovascular pathologies and risk factors among the different dementia diagnoses. Confirmed data* compared to obtainable data**. Micro- and microscopical findings (white background) and clinical data (grey background)
Count (percentage within each dementia group).
Chi-square value between each compared dementia group adjusted with Bonferroni correction: p = 0.05/03 = 0.017.
Significant results. X – No statistical analysis was made.
Confirmed cases among the obtainable data.
Obtainable data.
The same results applied for atherosclerosis of the aorta, where there was also a clear numeric difference in prevalence between all three dementia groups. The cases with no atherosclerosis (severity degree 0) were highest among the AD group, severity degree 1 was highest among the MD group, slightly more prevalent than in the AD group, and severity degrees 2 and 3 were most frequently seen in the VaD group (Table 3).
Myocardial infarctions, including acute and subacute myocardial infarctions as well as older ischemic myocardial lesions, were most prevalent in the VaD group, 73% of cases, whereas AD had the lowest prevalence of infarction, 27% of cases. The results were significant between these two groups even after Bonferroni correction (p < 0.001). The MD group had the second highest prevalence, 41% of cases (Table 3), with a significant difference with the VaD group (p < 0.001) but not with the AD group (p = 0.14). Regarding cardiac and myocardial hypertrophy, it was found in 52% of the VaD cases, 33% of the MD cases, and 25% of the AD cases. These results were significant between the AD and the VaD groups (p < 0.001); however, the results were not significant between the MD and the AD groups (p = 0.42) and not between the MD and the VaD groups after Bonferroni correction (p = 0.030). Nephrosclerosis was seen in 68% of the VaD cases, 60% of the MD cases, and 45% of the AD cases (Table 3). Only the findings between the AD and the VaD group attained significant results regarding this parameter even after Bonferroni correction (p = 0.006) (Table 3). The median heart weight in the VaD group was 433 g (interquartile range (IQR) = 278–588), 29 (29%) cases with a weight above 500 g. Median heart weights in the MD and the AD group were 348 g (IQR = 209–487) and 337 g (IQR = 212–462) with 8 (11%) and 5 (6%) cases above 500 g, respectively (Table 3). When comparing the groups regarding number of cases with a pathological heart weight (≥500 g), there was a significant difference only between the AD and the VaD groups (p < 0.001).
HTA was found in a total of 34 subjects, with the highest prevalence in the VaD group (n = 21), and the lowest in the AD group (n = 2). 25 of these cases had reported HT in the medical records, whereas 9 cases had no accessible medical records or information registered in the NDR. Among these 9 cases with HTA as sole evidence of HT, 7 had VaD, 1 had MD, and 1 had AD.
CaVD associated diseases: Hypertension and diabetes
Data on HT in AD, MD and VaD were obtained in 70%, 73%, and 76%, respectively, while data on DM in AD, MD, and VaD were obtained in 62%, 70%, and 63%, respectively (Table 2).
Regarding HT and DM, both diseases were most prevalent in the VaD group, 74% and 31%, respectively, and the least prevalent in the AD group, 37% and 12%, respectively, (p < 0.001 and p = 0.014, respectively). The prevalence of HT and DM in the MD group was in between that of the other groups, 44% and 19%, respectively (Table 3, Fig. 1). There was a significant difference between the MD group and the VaD group concerning HT (p < 0.001). However, the other parameters in the MD group did not attain a significant p-value when compared with the AD and VaD groups.
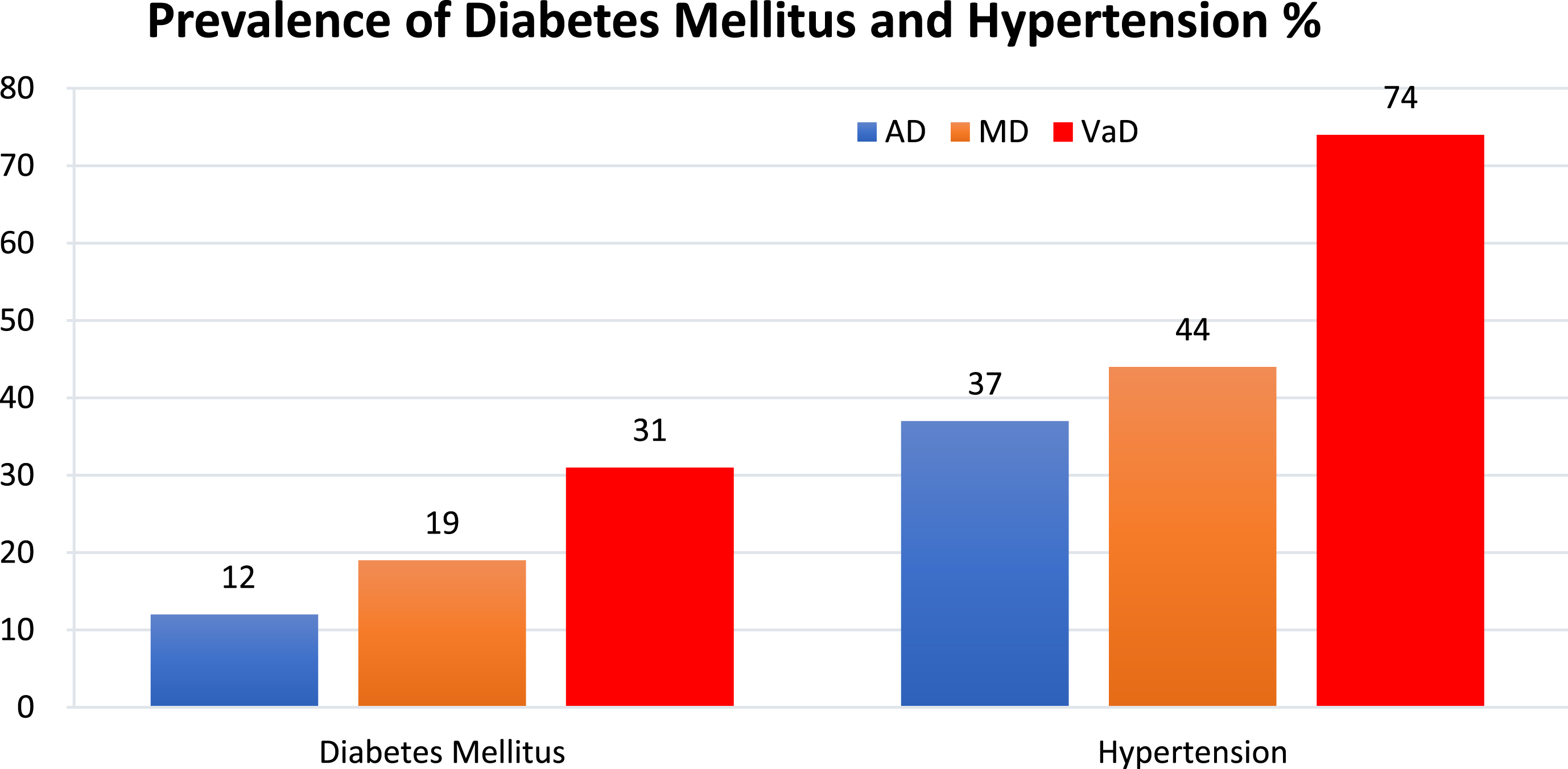
Prevalence of diabetes mellitus and hypertension among the different study groups (%). AD, Alzheimer’s disease; MD, mixed dementia; VaD, vascular dementia.
DISCUSSION
We presented the autopsy findings of CaVD and the clinical and national register data on HT and DM for association with the different neuropathologically diagnosed diseases AD, VaD, and MD. Since these diseases have markedly dissimilar pathology profiles, it seemed possible to assume, as our results also indicate that the presence of above mentioned CaVD, HT, and DM would be likewise dissimilar. It is also our experience that in numerous studies the term “Alzheimer’s disease” is expressed as seemingly equal to dementia in general and not as one of many specific disease types. Therefore, alleged risk factors for AD could in fact be risk factors for non-AD dementias as well as for dementia in general.
Atherosclerosis of the aorta and coronary arteries
Among our studied population, a difference was found between the prevalence of atherosclerosis, both in the aorta and the coronary arteries, between the AD and the VaD group. MD presented with severity of atherosclerosis less than the VaD group but more than the AD group. This is interesting since the only difference in definition of MD and VaD in our study is that there is more AD pathology in the subjects with MD: Braak stage III or more, compared to Braak stage II or less in the subjects with VaD; however the vascular-ischemic pathology should be similar. Therefore, one may speculate that the atherosclerosis in the MD group should at least be equal to or even more severe than in the VaD group. Perhaps AD pathology has a protecting and or inhibitory effect on the severity and progress of atherosclerosis?
What is the explanation for the different prevalence of atherosclerosis between the cases with AD and the ones with VaD? Several studies express the similar view that atherosclerosis and CeVD contribute to cognitive impairment and dementia [10, 47–49]. However, studies are not in agreement whether these conditions are risk factors for AD or not [12, 50]. The famous Nun-study reported an 11% higher prevalence of AD among women with stroke on autopsy than in those without stroke [13]. Newman et al. reported in the Cardiovascular Health study that carotid wall thickness measured with MRI and ankle-brachial index was associated with a higher risk of AD [12]; this study, however, was limited to the use of clinically diagnosed AD, cases that may have had AD and other morphologic counterparts, including MD [21, 23].
As more and more studies have implied that vascular disease is a risk factor for AD, questions have been raised as to what mechanism lies behind it. Stampfer et al. discusses whether AD and vascular disease share risk factors and that these risk factors independently increases both AD and vascular disease or simply that the vascular disease influences the pathological process which causes AD [10]. While some studies suggest that CeVD results in an acceleration of amyloid-β production or affects the clearance of it and thus contributes to AD pathology [51, 52], others claim that the amount of tangles and plaques do not increase by vascular risk factors [53].
The prevalence of atherosclerosis both in the coronary arteries and the aorta in our study groups was corroborated by the findings of myocardial infarction on autopsy, which we interpret as a marker for a general vascular pathology condition and which followed a similar pattern of prevalence as atherosclerosis within our dementia groups.
Diabetes mellitus
DM is a well-established risk factor for cognitive impairment and increased risk for cognitive decline, such as presented in numerous reviews [25, 54]. The mechanism of this process, however, is not fully recognized as studies argue the reason to be either the effect of insulin on the brain, or the vascular damage accompanying DM [10]. The vascular damage is caused by the higher incidence of HT and both CaVD and CeVD in patients with DM [55], whereas the effect of insulin acting directly on the brain is thought to increase the deposition and reduce the degradation of amyloid-β protein [56], which is claimed to be a major pathophysiological mechanism in AD pathology [9]. Interestingly, Okereke et al. showed that women without clinically overt DM but with higher levels of C-peptide, representing insulin secretion, had increased risk of cognitive impairment [57], indicating that it is the direct effect of insulin that matters. Furthermore, Luchsinger et al. showed that individuals with higher levels of fasting insulin, with or without clinical DM, exhibited a 70% higher risk of developing AD [26] and of memory decline [26]. However, as this study used clinically diagnosed dementia cases only, not neuropathological confirmation, it is not excluded that the claimed higher risk for developing AD is in fact an increased risk for cognitive impairment in general.
In 2013, the prevalence of DM was reported to be 15.6% among the normal Swedish population in individuals >65 years [58], which is an age group in proximity to our study group (81 years, SD 9). Comparing that percentage with our results shows that the prevalence of DM in our AD group is found to be within the same interval or even lower than that of the general population in Sweden. This finding is in congruence with previous studies describing a lower frequency of DM among patients with AD [58, 59] and individuals with Down’s syndrome [60], a disease destined to be hampered by AD at a certain age [61–63]. In contrast, the prevalence of DM is higher in the MD group and twice as high in the VaD group, compared to AD and the Swedish population. Hence, these findings indicate a strong association between VaD and DM but do not lend support to the hypothesis that DM contributes to AD pathology.
Hypertension
The question if HT affects cognitive function is accessed in several studies [27, 64–67], whereas they all argue that there is a relation. However, in the East Boston study with over 2,000 subjects, an SBP of <130 and >160 were linked with similar test results on the short Portable Mental Status Questionnaire [66]. The connection between HT and cognitive function is perhaps not that surprising since HT is a well-established risk factor for CaVD and CeVD [68, 69], which both are connected to the development of dementia and mostly with VaD [9]. This is further strengthened by the fact that anti-hypertensive treatment is known to reduce the risk of both cardiovascular and cerebrovascular events [70–73]. The connection with VaD is supported in our results were nearly three-quarters of our subjects with VaD presented with HT. It remains to be investigated whether HT alone affects cognitive function or if it is the effect of higher blood pressure on the cardiovascular system that is the cause. This also accounts to DM which is often accompanied by CaVD as well as HT [55]; do these diseases together have a synergetic effect on cognitive function or do they all contribute independently?
Some studies imply that there is a connection between AD and HT [16, 27], whereas others claim the opposite [28, 74]. The Hisayama study reported no connection between AD and HT but between VaD and HT. Interestingly, Mielke et al reported remarkable effects of an SBP of >160 mmHg on cognitive decline in patients with AD but no such influence of an SBP of >140 mmHg. Unfortunately, in this study we were not able to specifically study SBP of >160 mmHg, albeit 37% of the AD cases presented with HT (>140/90 mmHg). This is admittedly a considerable amount of cases, but is still a lower percentage of HT than in the MD group and only half as much as the prevalence of HT in the VaD group.
We did also include patients with reported anti-hypertensive therapy as having HT. We did not differentiate between type of treatment nor the effect of treatment. Several studies that have been focused on the effect of anti-hypertensive treatment on cognitive decline have not found it to have any results [70–72] and a Cochrane review of randomized clinical trials found no considerable indication that anti-hypertensive treatment could prevent dementia [75]. Remarkably, in the Syst-Eur trial [76], 2,418 subjects mostly with AD (clinical diagnosis only) showed that blood pressure lowering treatment for 2 years resulted in decrease in dementia compared with placebo. Further, in a meta-analysis of 11 clinical trials, Staessen et al. concluded that treatment with diuretic or dihydropyridine calcium-channel blockers may reduce the risk of dementia even though a general anti-hypertensive treatment does not affect the risk [77].
Worth mentioning is that both two large trials, the SHEP and SCOPE trials [70, 71], had intentions to investigate the consequence of anti-hypertensive treatment on cardiovascular and cerebrovascular events and only as the secondary intention studying the effects on cognitive decline, which resulted in conclusion of the studies when the primary measures were answered. The SHEP trial had isolated SBP of an average of 150 mmHg while the Eur trial had blood pressures below 150 mmHg. The question is, if both the SHEP and Scope studies had been prolonged for more years, would they have seen effects on cognitive decline and would treatment have shown a beneficial outcome with an established blood pressure below 140/90? At the same time, studies in Sweden show that only 20–30% of patients with anti-hypertensive treatment reach the goal of a blood pressure below 140/90 [69], hence making it difficult to evaluate whether reaching this treatment goal has an effect on cognitive decline or not, as the patient groups would be small.
The Swedish Council on Health Technology Assessment in Health Care (SBU) presented a report in 2004 that more than 50% of the Swedish population over 65 years had HT [78]. Comparing this with our results, both the AD and MD group presented prevalences below these numbers. The VaD group, however, presented with higher prevalence of HT than that of the normal population in Sweden. Hence, these results do not support the alleged connection of HT and AD
We also examined the presence of myocardial hypertrophy, increased heart weight, and nephrosclerosis on autopsy since these morphological changes are highly connected with HT [37–41]. They also followed the same pattern of prevalence as HT in our study groups. The same results applied for HTA in the brain, a disorder highly associated with HT [45], thus these four morphological changes corroborated with the found prevalence of HT among the three dementia groups.
Strengths and weaknesses
A strength of this study was that the confirmation of diagnosis was made by the same pathologist, which precludes the risk of different interpretations on the findings from different pathologists, and that the diagnostic procedures had the similar format.
There was missing information on some of the individuals. This lack was due to either incomplete medical records or a suboptimal registration of diagnoses to the NDR. Among all three groups (n = 286), data was missing on HT in 71 cases and on DM in 94 cases. These cases were omitted in the respective statistical analysis which hence somewhat weakened the calculations. Further, we recorded among our cases a total of 7 individuals with DM recorded in the referral documents or patients’ records, but not known to the NDR.
A certain aspect of this study, which we consider being a veritable strength, not often seen in previous studies, is the combination of both observable morphological macro- and microscopical findings on autopsy of individuals with a clinically diagnosed dementia disease and clinical data from medical records and the NDR. This study design allowed us to gain accurate information regarding atherosclerosis, nephrosclerosis, myocardial infarction, and HTA, as these findings were based on observations at autopsy, and furthermore often were quantified for severity degree in the primary report. On the other hand, even though all autopsies were performed in the same department using the similar implementation, they were done by different pathologists, which could in some cases lead to different reading of the severity degree of cardiovascular and cerebrovascular pathologies. As this was a retrospective study, it is also a limitation that the autopsies were carried out without a study protocol in perspective. This may be balanced by the benefit of the long period of time covered in this study, i.e., the longitudinal value of the autopsy report consistency. The different pathologists were trained to follow the same general routine and employed a template regarding performance and reporting of autopsies. As these autopsies were done with a clinical diagnostic purpose without the current study in mind, we were not able to control for inter-rater variability.
Another point of strength of this study is that information regarding HT and DM was collected from medical records and the NDR. These disorders were thus clinically diagnosed (the patients still in life). This means that, like the autopsies, this information was generated by clinicians not affiliated with the current study, as part of routine practice, hence “blinded” to the objectives in the present study.
In summary, our study showed a nominal difference in the prevalence of atherosclerosis in the coronary arteries and the aorta (without formal statistical analyses performed) between the three dementia groups, AD, MD, and VaD, as well as a statistically significant difference of clinically recorded DM and HT between the groups. The VaD group exhibited the highest prevalence of all studied disease manifestations and of both DM and HT, whereas the AD group had the lowest prevalence for all above. The MD group was in all cases in-between the other two groups. DM was as prevalent in our AD group as for the normal Swedish population of similar age.
Conclusion
With these results of low prevalence of CaVD, a relatively low prevalence of HT and low prevalence of DM in AD, we find no support for the alleged association between AD and CaVD and CaVD risk factors. Hopefully this study will contribute to better knowledge of different dementia types and it stresses the importance of ascertaining an accurate diagnosis, even after death, to draw the accurate conclusions about disease associations and risk factors.