
Abstract
Background:
Midlife cardiovascular risk factors (CVRF) are associated with reduced cognition and an increased risk of dementia.
Objective:
To further investigate this association using remote unsupervised online assessment of cognition and cardiovascular risk in middle-aged adults; and to explore the extent to which the association is altered by carriage of the APOE ɛ4 allele.
Methods:
The Healthy Brain Project is an online cohort of middle-aged cognitively unimpaired adults (40–70 years) who have undergone cognitive assessment and provided self-reports of demographic and health history. Cardiovascular risk was determined by ascertaining history of hypertension, hypercholesterolemia, diabetes mellitus, overweight (body mass index≥25), and current cigarette smoking. Participants (n = 2,480) were then grouped based on the number of reported CVRF into no CVRF, 1, 2, and≥3 CVRF. Associations between the number of CVRF as a continuous variable, CVRF group, and each individual CVRF with composite measures of attention, memory and subjective cognitive function were investigated.
Results:
Higher number of CVRF was associated with poorer attention (β= –0.042, p = 0.039) and memory (β= –0.080, p < 0.001), but not with subjective cognitive function. When considered individually, current smoking (β= –0.400, p = 0.015), diabetes (β= –0.251, p = 0.023), and hypercholesterolemia (β= –0.109, p = 0.044) were independently associated with poorer memory performance. APOE ɛ4 carriers with≥1 CVRF performed worse on memory than ɛ4 carriers with no CVRFs (β(SE) = 0.259(0.077), p = 0.004). This was not observed in ɛ4 non-carriers.
Conclusion:
In cognitively normal middle-aged adults, CVRF were associated with poorer cognition, particularly in the memory domain. These results support feasibility of online assessment of cardiovascular risk for cognitive impairment.
INTRODUCTION
Midlife cardiovascular risk factors, including hyp-ertension, diabetes mellitus, hypercholesterolemia, obesity, and cigarette smoking, are associated with an increased risk of late life cognitive impairment and dementia, including Alzheimer’s disease (AD) dementia [1–5]. There is also evidence of an association between cardiovascular risk and both fluid and imaging biomarkers of AD including amyloid-β [4], tau [6], and brain atrophy [7]. Cumulative vascular risk factor burden has also been shown to be associated with cognitive dysfunction during midlife, including risk factor exposure during early adulthood [8] and even during childhood [9]. Therefore, midlife is an important epoch for both the emergence of cardiovascular risk factors as well as their potential impact on cognition contemporaneously and later in life.
Natural history studies, particularly those condu-cted in adults who carry the apolipoprotein E (APOE) ɛ4 allele, show that the earliest signs of AD pathology begin decades prior to the development of clinical symptoms, typically during middle age [10–12]. Additionally, ɛ4 carriers are at greater risk of age-related cerebrovascular disease, including stroke [13–15] and post-stroke dementia [16], and associations between cardiovascular risk factors and cognitive dysfunction in older adults are most prominent in ɛ4 carriers [17–19]. The overlap between AD pathology and cardiovascular risk factors in midlife thus warrants further investigation. In particular, understanding the extent to which cardiovascular risk factors are associated with cognition in middle-aged adults may guide the development of therapeutic and preventative strategies designed to attenuate these impacts in middle-aged adults, and reduce the risk of dementia in later life.
One challenge to understanding associations bet-ween cardiovascular risk factors and cognition in middle-aged adults is that the magnitude of these relationships is likely to be subtle and large samples are therefore required to provide the statistical power to detect the relationships. Online platforms provide a unique and practical approach to addressing these challenges, as large amounts of data on at-risk individuals can be collected remotely while maintaining high test validity as well as participant acceptability. This approach can facilitate and accelerate understanding of disease risk factors and natural history, as well as the ability to remotely deliver putative risk reduction interventions. We have developed and optimized such digital assessment methods to measure different domains of cognition relevant to dementia, with high validity and reliability in unsupervised contexts [20–22].
The aim of this study was to investigate the nature and magnitude of associations between cardiovascular risk factors and cognition, determined from both self-report and objective assessment, in middle-aged adults who were assessed remotely using an online platform as part of their participation in the Healthy Brain Project [23]. We also explored the extent to which any associations between cardiovascular risk factors and cognition differed between APOE ɛ4 carriers and non-carriers.
METHODS
Participants
Participants enrolled in the Healthy Brain Project completed a series of online modules pertaining to basic demographics, medical history, and cognition. The overall objective of the Healthy Brain Project is to characterize risk factors and early characteristics of dementia during middle age. Recruitment and inclusion and exclusion criteria have been described previously [23]. Briefly, the Healthy Brain Project relies on an online, remote, unsupervised recruitment and assessment strategy and is housed within a web-based platform (healthybrainproject.org.au) which can be accessed from desktop computers, laptop computers, tablets, and mobile devices. Recruitment has been ongoing since 1 March 2016. Participants aged 40–70 years are included if they are currently residing in Australia (irrespective of citizenship); fluent in English; do not have a diagnosis of AD, Parkinson’s disease, dementia with Lewy bodies, or other known diagnosis of cognitive impairment; do not have a history of severe traumatic brain injury or other major neurological disease or insult (e.g., multiple sclerosis); do not have a diagnosis of a major psychiatric condition (e.g., schizophrenia, uncontrolled current major depressive disorder, or other psychiatric disorder); and do not use any approved medication for the treatment of AD (e.g., donepezil, galantamine, rivastigmine, or other approved medications).
As recruitment into the Healthy Brain Project is ongoing, the current report includes data that have been collected up to the most recent data freeze on 18 April 2020. On this date, 6,960 participants had enrolled in the Healthy Brain Project, and of those, 2,480 provided sufficient data (cognitive and self-reported cardiovascular risk) for analysis. A subset of participants (n = 1,401) also provided saliva samples for the purpose of APOE genotyping.
The Healthy Brain Project was approved by the Human Research Ethics Committee of Melbourne Health (HREC2016.199). All participants gave informed consent prior to enrolment and the study conforms to the principles outlined in the Declaration of Helsinki.
Cardiovascular risk assessment
Participants self-reported a history of hyperten-sion, hypercholesterolemia, diabetes mellitus, overweight (body mass index≥25), and cigarette smoking (currently smoking, or quit smoking < 1 year ago). Each item contributed a score of 1 (maximum score of 5). The distribution of cardiovascular risk factors (CVRF) in the sample was examined (Fig. 1) and, based on this, participants were grouped into 0 CVRF (n = 859), 1 CVRF (n = 1013), 2 CVRF (n = 443), and 3 + CVRF (n = 165).
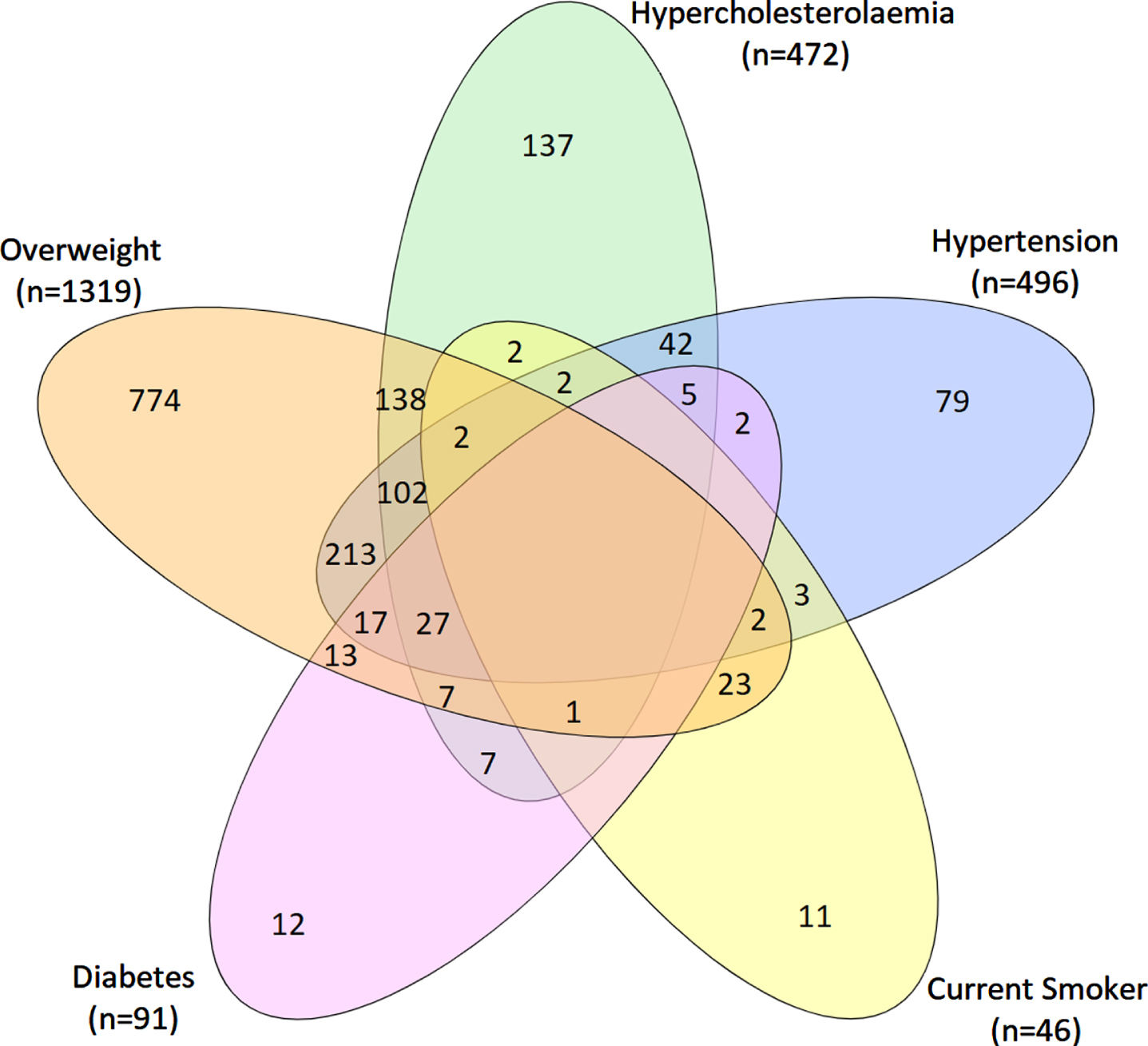
Co-occurrence of each cardiovascular risk factor.
Objective cognition
Participants completed the Cogstate Brief Battery (CBB) using an unsupervised, online study platform on their personal desktop computer or laptop. The CBB has been validated for the detection of subtle cognitive impairments in individuals at-risk of AD [24, 25] and has been optimized for remote, unsupervised assessments [20–22]. Participants were required to complete the CBB in one session, which took approximately 20 minutes. CBB tests are downloaded onto the browser, completed locally and then uploaded. This minimizes the impact of internet connectivity on test performance. The CBB has a game-like interface which uses playing card stimuli and requires participants to provide “Yes” or “No” responses. The interface presents four tests, Detection (DET), Identification (IDN), One Card Learning (OCL), and One-Back (OBK) [26, 27]. DET is a simple reaction time test shown to measure psychomotor function. IDN is a choice reaction time test shown to measure visual attention. The primary outcome measure for DET and IDN was reaction time in milliseconds (speed), normalized using a log10 transformation. OCL is a continuous visual recognition learning task that assesses visual learning within a pattern separation model. OBK is a task of working memory and attention. The primary outcome measure for OCL and OBK was the proportion of correct answers (accuracy), normalized using an arcsine square-root transformation.
An attention composite score was computed by averaging standardized scores for the DET and IDN tests. Similarly, a memory composite score was computed by averaging standardized scores for the OCL and OBK tests. All scores were standardized using the baseline mean and standard deviation of the whole sample, as described previously [25].
Subjective cognition
To measure subjective cognition, we used a modified version of the Cognitive Function Index (CFI). This modification was undertaken as the original CFI was designed for older adults. As such, some items were modified to include ecologically valid questions about subjective experiences of memory and thinking at work, and other relevant aspects of an individuals’ life, as previously described [23].
APOE genotyping
Genotek Oragene (OG-500) 2 ml saliva kits (including instructions on saliva collection) were mailed to participants who had completed at least 80% of assessments [28]. Saliva samples were forwarded to GenoFIND Services laboratory (Salt Lake City, UT, USA), where they were processed to extract targeted SNPs including for APOE (rs429358, rs7412).
Data analysis
All analyses were conducted in the statistical program R (v3.5.0). A series of chi-squares and analyses of variance (ANOVA) were conducted to determine demographic differences between the CVRF groups. For consistency, outcome measures on the attention composite and the subjective cognitive function total score were reverse scored so that negative scores indicate worse performance.
To determine the association between cardiovascular risk factors and objective and subjective cognition, a series of linear regressions were performed. A series of analyses of covariance (ANCOVA) with planned comparisons were also conducted to determine the magnitude of difference between the CVRF groups (0 [reference], 1, 2, 3+) on each measure of objective and subjective cognition. Magnitude of difference between groups was expressed as Cohen’s d. Finally, the association between each individual cardiovascular risk factor and objective and subjective cognition was evaluated.
To explore the extent to which associations bet-ween cardiovascular risk factors and cognition differed between ɛ4 carriers and non-carriers, an ANCOVA was conducted for each of the composite outcome measures of attention and memory, with CVRF group, ɛ4 status and the interaction between CVRF group x ɛ4 status as fixed factors.
All models were adjusted for age, sex, education, and depressive and anxiety symptoms. These covariates were chosen given the known and/or observed associations with both cardiovascular risk and cognitive performance. For all statistical comparisons, a p < 0.05 was considered to indicate statistical significance. Analyses were not adjusted for multiplicity as this report is one of the first to demonstrate relationships between self-reported cardiovascular risk factors and cognition measured remotely and in an unsupervised setting. However, the use of effect sizes protected against the over-interpretation of statistically significant but trivial effect sizes.
RESULTS
Demographic characteristics
A total of 2480 participants were included in the analysis, mean (SD) age 56.8 (7.0) years, 75.2% female. Participants included in the current analysis were comparable to those of the broader Healthy Brain Project sample (n = 6960); mean (SD) age 55.9 (7.8) years, 71.3% female. Table 1 summarizes key demographics and risk factors in the overall sample as well as the different CVRF groups. Figure 1 illustrates the co-occurrence of cardiovascular risk factors in the current sample. The highest CVRF group was significantly older, had fewer years of formal education and reported higher levels of depressive and anxiety symptoms than the no CVRF group (Table 1). The no CVRF group was also more likely to be female and employed. A significantly higher proportion of the highest CVRF group reported a first-degree family history of cardiovascular disease, history of heart disease, and history of atherosclerotic disease.
Demographic characteristics*
*ANOVA was used to determine group differences for continuous variables; Chi-Square was used to determine group differences for categorical variables.
Association between cardiovascular risk factors and objective and subjective cognition
Table 2 summarizes the association between the number of cardiovascular risk factors and objective and subjective cognition. After adjusting for age, sex, education, and depressive and anxiety symptoms, a higher number of cardiovascular risk factors was associated with poorer performance on both the attention (β= –0.042, p = 0.039) and memory composites (β= –0.080, p < 0.001, Table 2). The number of cardiovascular risk factors was not significantly associated with subjective ratings of cognition.
Effect of increasing number of cardiovascular risk factors on objective and subjective measures of cognitive function
*standardized beta coefficients.
Table 3 summarizes the associations between CVRF group and objective and subjective cognition. After accounting for the effects of age, sex, education, and depressive and anxiety symptoms, there was a significant association between CVRF group and performance and the memory composite only (p < 0.001). Planned comparisons indicate that when compared to the 0 CVRF group, the 1, 2, and 3 + CVRF groups performed significantly worse on memory, with the magnitude of differences small-to-moderate, by convention (Table 3, Fig. 2). The 2 CVRF group showed significantly worse subjective cognitive performance compared to the 0 CVRF group, although the magnitude of this difference was small (Fig. 2). There were no significant differences between CVRF groups for the attention composite.
Effect of CVRF group on objective and subjective measures of cognitive function
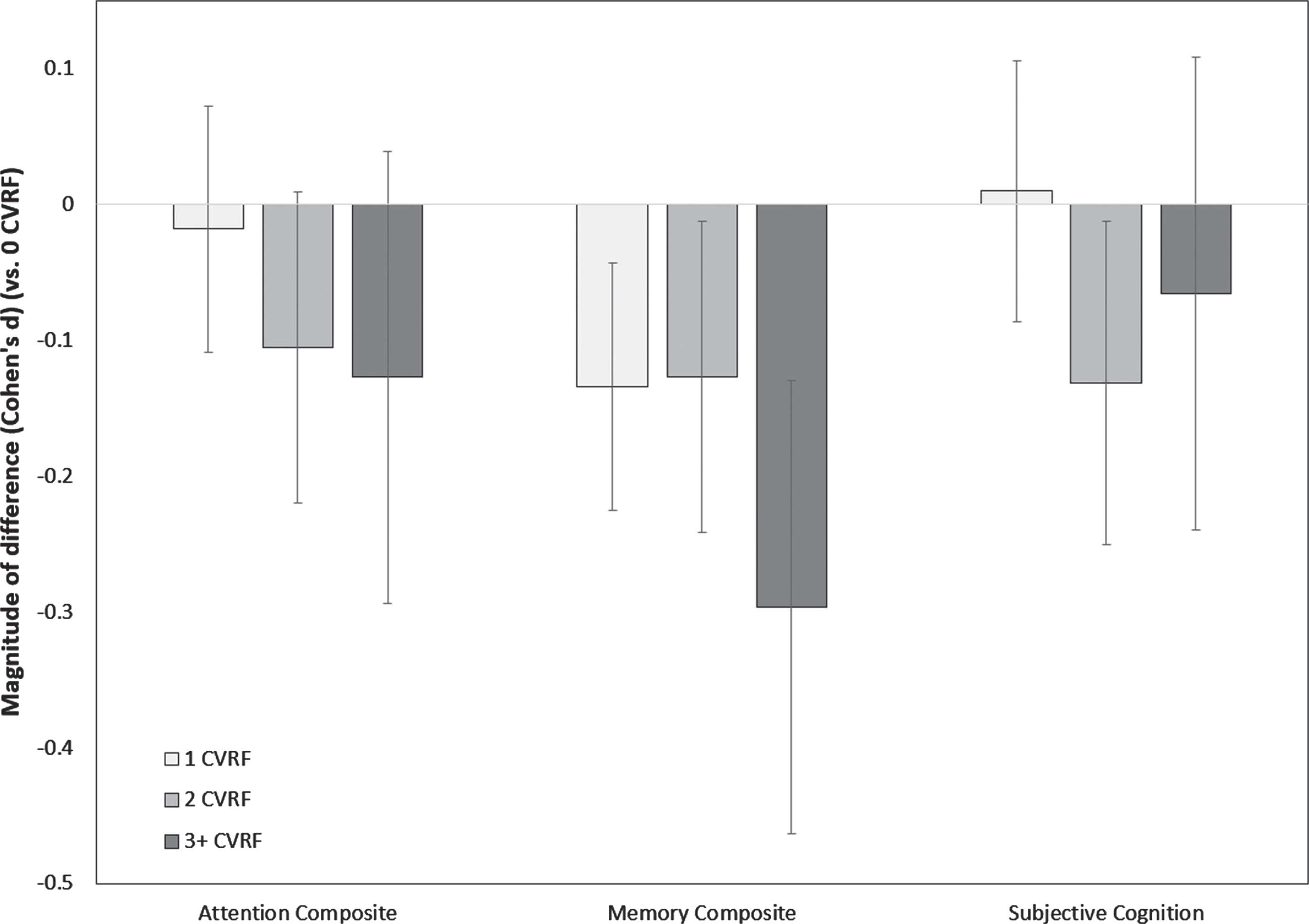
Magnitude of difference between the 0 CVRF group (represented by the “0” line) and 1 CVRF, 2 CVRF and 3 + CVRF groups on the attention composite, memory composite, and subjective cognitive outcome (error bars represent 95% confidence intervals). Negative values indicate worse performance.
Association between individual cardiovascular risk factors and objective and subjective cognition
When all cardiovascular risk factors were considered simultaneously, and after accounting for the effects of age, sex, education, and depressive and anxiety symptoms, only current cigarette smoking, diabetes, and hypercholesterolemia were independently associated with poorer performance on the memory composite (Supplementary Table 1). Hypertension, and being overweight were not significantly associated with performance on the memory composite. No individual cardiovascular risk factor was associated significantly with performance on the attention composite, or with subjective cognition (all ps > 0.05) (Supplementary Table 1).
Association between APOE ɛ4, CVRF, and cognition
Of the 2,480 participants included in this analysis, 616 participants were not provided a saliva sampling kit due to COVID-19 restrictions on the collection of biological samples in 2020. Of the 1,864 participants who were provided a saliva sampling kit, 1,401 (75.2%) participants returned a saliva sample to enable APOE genotyping (Supplementary Table 2). The prevalence of APOE ɛ4 carriage was 33.4% with no differences in the proportion of ɛ4 carriers by CVRF group (Table 1).
When participants were grouped into having no CVRFs versus one or more CVRFs, there were no significant interactions between CVRF groups and APOE ɛ4 on the attention or memory composites (Supplementary Table 3). However, pairwise comparisons indicated that APOE ɛ4 carriers with at least one CVRF performed worse on the memory composite than ɛ4 carriers with no CVRFs, β(SE) = 0.259 (0.077), p = 0.004, with the magnitude of difference between groups being moderate by convention, d (95% CI) = 0.33 (0.13, 0.52). Conversely, in ɛ4 non-carriers, CVRF groups did not differ in memory performance, d (95% CI) = 0.12 (–0.02, 0.25), p = 0.255. CVRF groups did not differ in performance on the attention composite in ɛ4 carriers or non-carriers, all ps > 0.809.
DISCUSSION
In a cohort of cognitively normal middle-aged participants undergoing online, unsupervised remote health and cognitive testing, independent and statistically significant associations were observed between cardiovascular risk factors and cognition, particularly in the memory domain. The largest effect size (a small to medium effect) was observed in the subgroup with three or more cardiovascular risk factors, and of all individual risk factors, the strongest associations with cognitive dysfunction were for cigarette smoking, diabetes, and hypercholesterolemia.
These results add further weight to the known associations between cardiovascular disease and cognition, most of which have been observed using traditional in-person assessment methods. While methodological differences limit direct comparison between our study and others, the effect sizes obs-erved in our study are comparable to other studies investigating the association between cardiovascular risk and cognitive performance, thereby providing further validation for the use of remote platforms for the assessment and identification of at risk-individuals [29–31]. Our findings also reinforce the notion that associations between cardiovascular health status and cognitive dysfunction can be observed even in in middle age and even within the spectrum of normal cognition. Interestingly, the strongest and most consistent association was seen with memory. The specificity of this relationship suggests that the observed association between cardiovascular risk factors and cognition is unlikely to be related to secondary cardiovascular disease related phenomena (such as reduced general health, level of motivation, or sensorimotor deficits), which would have given rise to a more general reduction across both attention and memory. However, this hypothesis will need to be tested in future studies that utilize a broader neuropsychological test battery and where biomarkers of AD and cerebrovascular disease have been measured.
Of note, in the context of older cognitively imp-aired adults, frank cerebrovascular disease (including stroke and imaging markers of cerebrovascular burden), is associated more typically with attentional impairment rather than memory deficits [32]. Interestingly, other studies in younger healthy cohorts such as ours have reported associations between vascular markers and poorer memory function rather than attentional deficits, suggesting that the mechanisms by which cerebrovascular risk factors lead to cerebrovascular disease and cognitive impairment may change over time [28].
The contribution of genetic risk to the association between cerebrovascular risk factors and memory is an important consideration and may provide some insights into whether the differences in cognitive function observed in the current study represent the preclinical stages of AD. In the main analysis, there was no significant interaction between APOE ɛ4 status and vascular risk status, on either aspect of cognition. There was a suggestion of an association between CVRF group and memory in a post-hoc analysis restricted to APOE ɛ4 carriers when CVRF groups were dichotomized into no risk factors versus any risk factors. Given that APOE ɛ4 carriage is the strongest genetic risk factor for sporadic late life AD, one potential explanation is that the observed differences in memory may reflect underlying accumulating AD pathology. Cerebrovascular disease may also potentially augment the effects of incipient AD pathology in such participants [33]. However, these hypotheses warrant further investigation and confirmation in the future as no markers of AD pathology were measured in the current study. In addition, the cross-sectional design of this study limits our ability to explore this association fully, and this will be the focus of a larger longitudinal analysis in the future.
There were no significant associations between cardiovascular risk and individuals own subjective cognition. This is not fully unexpected given the demographic profile of participants (cognitively normal middle-aged adults) included in this study. This suggests that the memory differences observed in the current sample are too subtle to be perceived by individuals. This is also consistent with previous studies which indicate that subjective cognitive concerns are more strongly associated with mood symptomatology than underlying AD pathology [34, 35]. Whether these differences are sufficient to impact functional or occupational performance or activities of daily living will be explored in more detail in future studies. This lack of a clear association between cardiovascular risk and subjective cognition also suggests that remote screening for early cognitive decline in midlife should always include some objective assessments of cognition, and in particular memory, rather than relying on individuals rating of their own cognitive difficulties.
Self-reported cardiovascular risk factors were common in this cohort of middle-aged adults, with more than half being classified as overweight, and one in five reporting hypertension. Current smoking was the least common risk factor (∼2%), although notably, more than a third of the group reported any smoking history (current or past). Importantly, self-reported vascular risk factors may underestimate the prevalence of actual vascular risk factors due to participant under-reporting or undiagnosed risk factors, and hence the associations we detected may be conservative. For example, the Australian Institute of Health and Welfare recently estimated that the prevalence of hypertension (both controlled and uncontrolled) in Australian adults was 33.7% [36], which is higher than the 20% observed prevalence in this study. Moreover, the prevalence of high BMI (classification of overweight or obese) in Australian adults is estimated at 63% [37], which is also higher than the observed prevalence in the current study. In addition to the issue of underreporting, it is also well recognized that research participants (particularly in studies of cognitive aging and AD) tend to have higher levels of education and lower prevalence of cardiovascular disease than the general population [38, 39]. This may have led to further underestimation of the true association between cardiovascular risk and cognition in the general community.
Traditional approaches to the assessment of cardiovascular disease and dementia risk typically require participants to attend detailed in-person assessments which are expensive, time-consuming, and may limit the involvement of participants residing outside of metropolitan areas. Online unsupervised approaches such that used in the Healthy Brain Project and the Brain Health Registry can facilitate the rapid recruitment of large diverse community-based samples in a cost-effective manner, which also allows continued participation despite potential restrictions imposed by the COVID-19 global pandemic. We and others have previously demonstrated both the acceptability and usability of the unsupervised cognitive testing used in the Healthy Brain Project [21, 22]. Moreover, several clinical trials have evaluated interventions aimed at mitigating cerebrovascular contributions towards cognitive impairment and dementia [40, 41]. Logistical challenges of such interventional strategies include the early identification of at-risk individuals, large-scale delivery of interventions, and the ability to monitor participants for the long periods of time required to measure clinically meaningful changes in cognition. The use of digital platforms such as the Healthy Brain Project to remotely identify individuals at risk of cognitive dysfunction related to cardiovascular risk factors might facilitate enrolment into clinical trials, including trials utilizing remote delivery of lifestyle interventions, to reduce this risk. Linking such platforms to national health records would further maximize their reliability and utility.
This study has some limitations. First, the reliance on self-reporting of vascular risk factors may lead to an underestimation of the true prevalence of these risk factors and therefore their associations with cognitive function. This is a common limitation of studies conducted entirely remotely, although it is balanced by the wide geographical reach of the study and large sample size. Second, the lack of data on the level of control of the measured vascular risk factors (e.g., blood pressure control, medication adherence, HbA1c level) prevents an examination of the impact of such factors on the observed associations. Third, the cross-sectional design of the current study may limit the detection of more subtle effects on cognition, and longitudinal associations between cognition and CVRF will be examined in future analyses. Together, these limitations may partially explain the lack of significant associations observed with hypertension and being overweight, both of which have been identified as important individual risk factors previously [42]. Fourth, given that the overall objective of the Healthy Brain Project is to understand the earliest stages of AD, many of the recruitment strategies have focused on people with a family history of this condition. This is reflected in the high proportion of participants with a first-degree family history of dementia and/or APOE ɛ4 carriage. Our findings should therefore be considered within this context. Fifth, our study has consistently recruited more women than men. While we have adjusted our analyses for sex, replication of these findings in other cohorts with a more balanced female:male ratio is important. Finally, inclusion in this analysis required completion of a minimum dataset of cardiovascular risk factors and cognitive tests, which was not universal within the overall Healthy Brain Project and may have led to a selection bias.
These limitations notwithstanding, the results of this study suggest that remote and unsupervised assessment of cardiovascular risk and cognition in cognitively normal middle-aged people can identify important associations between cardiovascular risk status and memory performance, which may represent early interactions between AD and cerebrovascular pathology, although this will require further exploration and will be the focus of future studies. No consistent differences were observed between APOE ɛ4 carriers and non-carriers although a post-hoc analysis did suggest that the association between cardiovascular risk and memory was restricted to APOE ɛ4 carriers when participants were dichotomized by the presence or absence of any cardiovascular risk factors. Overall, these findings have important implications suggesting that remote and unsupervised screening for cardiovascular risk factors for cognitive dysfunction during middle age is feasible, and this could potentially lead to interventions designed to target these disease processes in order to reduce late life dementia risk.
Footnotes
ACKNOWLEDGMENTS
We thank all Health Brain Project participants for their commitment and dedication to helping advance research into midlife risk and protective factors for dementia.
The Healthy Brain Project (healthybrainproject.org.au) is funded by the National Health and Medical Research Council (GNT1158384, GNT1147465, GNT1111603, GNT1105576, GNT1104273, GNT1158384, GNT1171816), the Alzheimer’s Association (AARG-17-591424, AARG-18-591358, AARG-19-643133), the Dementia Australia Research Foundation, the Bethlehem Griffiths Research Foundation, the Yulgilbar Alzheimer’s Research Program, the National Heart Foundation of Australia (102052), and the Charleston Conference for Alzheimer’s Disease. We thank our study partners (PearlArc, SRC Innovations, Cogstate Ltd and Cambridge Cognition) for their ongoing support.
YY Lim is supported by an NHMRC Career Development Fellowship (GNT1162645). MP Pase is supported by a Heart Foundation Future Leader Fellowship (GNT102052). RF Buckley is supported by a National Institutes of Health K99-R00 award (K99AG061238).