
Abstract
Background:
Amyloid pathology is a key feature of Alzheimer’s disease (AD) and can be assessed in vivo with amyloid positron emission tomography (PET) imaging.
Objective:
The objective of this study was to evaluate the incremental value of a PET scan with [18F]florbetaben, in terms of changes of diagnosis, diagnostic confidence, and treatment plan when added to a standardized diagnostic workup for cognitive disorders, with particular focus on the role of the neuropsychological assessment, including the Free and Cued Selective Reminding Test (FCSRT).
Methods:
A total of 104 patients (69 mild cognitive impairment, 35 dementia), with diagnostic uncertainty after diagnostic workup, were recruited from our memory clinic. [18F]florbetaben PET scans were interpreted as amyloid negative or positive on the basis of a semi-quantitative visual rating. Clinical diagnosis and diagnostic confidence for AD or non-AD dementia were rated before and after PET result disclosure, as was the impact of PET on the patient management plan.
Results:
There were 69/104 (66%) [18F]florbetaben positive scans, 51/62 (82%) patients were suspected as having AD before the PET scan and 18/42 (43%) were not. Overall, the data obtained at PET changed 18/104 diagnoses (17%) and increased diagnostic confidence from 69.1±8.1% to 83.5±9.1 (p < 0.001), with the greatest impact on diagnosis and confidence in PET negative patients with an initial diagnosis of AD (p < 0.01) and in early-onset patients (p = 0.01).
Conclusion:
Amyloid PET represents a source of added value in dementia diagnosis, with a significant effect on diagnosis and diagnostic confidence. However, the use of a complete neuropsychological assessment has an add-on value on limiting the amyloid PET influence on change of diagnosis, and the real impact of amyloid PET should always be weighed up together with an accurate standardized diagnostic workup.
INTRODUCTION
Brain amyloid-β (Aβ) deposition is a key feature of Alzheimer’s disease (AD) and is detectable in vivo through cerebrospinal fluid (CSF) Aβ42 sampling and amyloid positron emission tomography (Amy-PET) radiotracers [1].
Both CSF and PET amyloid markers have been incorporated into the revised research criteria for AD [2–4], even if recent findings seem to show that Amy-PET are better than CSF biomarkers in terms of sensitivity/specificity and diagnostic accuracy for AD [5]. The F 18 labeled tracers with a longer half -life have become available for clinical practice overcoming the limited clinical use of carbon 11-labeled of Pittsburgh Compound B. Amy-PET tracers, including [18F]florbetaben, have displayed a very good concordance with amyloid load observed postmortem, binding to Aβ with very high sensitivity and specificity [6, 7].
However, given the widespread prevalence of cerebral amyloidosis in non-AD dementia and the healthy elderly, the efficacy of Amy-PET tracers in clinical practice and their impact on diagnosis are still under debate. Indeed, a comprehensive meta-analysis reported positive scans in 51%, 38%, and 30% of patients with Lewy body dementia, corticobasal degeneration, and cerebrovascular disease, respectively [8]. A further meta-analysis showed that the prevalence of amyloid pathology increases with age, reaching almost 40% in the healthy elderly [9]. Therefore, the clinical use of Amy-PET has to be regulated by appropriate use criteria [10, 11]. As summarized by two systematic reviews [12, 13], a growing number of studies have explored the role of Amy-PET in clinical practice in terms of impact on the diagnostic and treatment plan. However, studies were often multicentric [14–16] or retrospective [17, 18] without a fully standardized protocol for the routine diagnostic workup, with the consequent risk of overrating the diagnostic value of Amy-PET. In this regard, both the quality and quantity of the neuropsychological assessment is highly variable across the different studies, and none of the studies would seem to assess the episodic memory impairment through the Free and Cued Selective Reminding Test (FCSRT), as specifically recommended by the International Working Group (IWG) criteria [2]. On the other hand, prospective single-center studies often had a small sample size [19–21].
This study aimed at assessing the impact [18F]florbetaben PET has on (confidence in) the clinical diagnosis in mild cognitive impairment (MCI) and dementia patients referred to our memory clinic and undergoing a standardized diagnostic workup that includes an extensive neuropsychological assessment.
Another aim was to verify whether some demographic, clinical features (MCI subtypes or dementia) and pre-scan diagnostic confidence (e.g., high or low) affect the diagnostic value of PET scans.
METHODS
The present study included 104 consecutive patients admitted to the Dementia Unit of Parma for diagnosis of cognitive disorders between January, 2015 and November, 2016. All patients were given a complete clinical assessment, including neurological and physical examination, blood tests, magnetic resonance imaging, and a comprehensive neuropsychological assessment. The general cognitive level and abstract reasoning were assessed by the Mini-Mental State Examination (MMSE) and Raven’s Advanced Progressive Matrices (PM 47), respectively. Other tests included the Multiple feature target cancellation and Stroop test (attention and executive domains), Free and Cued Selective Reminding Test (FCSRT) and the Digit Span forward (memory), the Rey-Osterrieth Complex Figure, Clock Drawing test (praxis and visuospatial), the Boston Naming Test, the Semantic and phonological Fluency verbal Test (language), the Geriatric Depression Scale, and the Neuropsychiatry Inventory (mood and psychopathology), as well as ADL and IADL (functional daily living activity). A lumbar puncture was carried out on a subgroup of patients, but for the purpose of this study, the CSF results were not disclosed before the results of the impact of Amy-PET had been assessed. Inclusion criteria were objective cognitive deficits, age at PET scan between 45 and 85, no definite diagnosis or persisting diagnostic uncertainty after workup (defined as a pre-scan diagnostic confidence of <85% according to literature and previous clinical trials) [14–16]. Exclusion criteria were: an MMSE of <10 or a score greater than 2 on the Clinical Dementia Rating, previous participation in any experimental study with a disease modifying therapy and/or an amyloid targeting agent, any secondary cause of cognitive impairment that resulted from the dementia workup.
Clinical diagnosis was established at the end of the workup and prior to the Amy-PET scan, with the consensus of the neurologists in our memory clinic, according to clinical criteria [3, 22–27]. Pre-scan diagnostic groups were MCI (n = 69), AD (n = 18), frontotemporal dementia (FTD, n = 7) and other dementia subtypes (OD group, n = 10, including corticobasal syndrome, dementia with Lewy bodies, progressive supranuclear palsy, Parkinson disease dementia). MCI subtypes were amnestic (n = 15), non-amnestic (n = 25), and multidomain (n = 29). Based on MMSE score cutoff of 20, demented patients were considered as mild (n = 16) or moderate (n = 19).
Also the impact of Amy-PET on change in prescription of AD medication, patient follow-up and request for further diagnostic investigations (the patient management plan) was investigated. The study was carried out according to the declaration of Helsinki and all the participants gave written informed consent, approved by the local Ethics Committee.
Assessment of diagnostic confidence and utility
At the end of the routine dementia assessment, the neurologists of our memory unit were asked to stage cognitive impairment (MCI or dementia) and suggest the most probable diagnosis during a multidisciplinary meeting. A diagnosis was reached by consensus and they then indicated the corresponding diagnostic confidence for AD or non-AD on a scale ranging from 50–85%. As aforementioned, in case of no diagnostic doubt, diagnostic confidence was considered to be higher than 85% and the patient was not eligible for an Amy-PET scan and therefore excluded from the study. On the basis of the clinical information obtained from the dementia screening, MCI patients were classified as due or not to AD (MCI-AD versus MCI-not AD) and dementia groups as AD or non-AD (including FTD and OD patients). A score from 50–70% was considered as low diagnostic confidence (LC) and a score from 71–85% high confidence. Once the Amy-PET results had been disclosed, the patients were given a follow-up visit where a re-evaluation of the diagnosis with the corresponding diagnostic confidence was made. The average interval between the dementia workup and [18F]florbetaben PET scan was 71± 70 days.
Amyloid PET imaging
PET scans were performed at the Dalla Rosa Prati PET Centre in Parma, using a whole-body hybrid system Discovery IQ (GE Healthcare) operating in the three-dimensional detection mode.
All cerebral emission scans began 90 min after an intravenous injection of 4 MBq/kg weight (240–360 MBq) of [18F]florbetaben. For each subject, 10-min frames were acquired for all patients to ensure movement-free image acquisition. All PET sinograms were reconstructed with a 3-D iterative algorithm, with corrections for randomness, scatter, photon attenuation, and decay, which produced images with an isotropic voxel of 2×2×2 mm and a spatial resolution of approximately 5-mm full-width at a half-maximum (FWHM) in the center of the field of view. Visual blinded PET image assessment was made by two trained, independent readers with a previously described technique (excellent inter- and intra-reader agreement, k = 0.98) [28, 29]. Visual assessments of [18F]florbetaben PET images were made using a three-grade scoring system (RCTU - regional cortical tracer uptake) comparing the activity in cortical gray matter (frontal cortex, posterior cingulate cortex/precuneus; lateral temporal cortex and parietal cortex) with activity in adjacent cortical white matter. The RCTU scores (1 = no binding, 2 = minor binding, and 3 = pronounced binding) were then condensed into a single three-grade scoring system for each PET scan, the BAPL (brain Aβ plaque load) score: 1 = no Aβ load, 2 = minor Aβ load, 3 = significant Aβ load and the resulting scores were then condensed into a binary interpretation (score 1 = negative; score 2 or 3 = positive).
Statistical analysis
The differences in the general characteristics between the diagnostic groups were assessed by the analysis of variance (ANOVA) and Pearson’s χ2 tests. The differences in diagnostic confidence before the Amy-PET between the diagnostic groups were assessed by ANOVA. Diagnostic changes limited to AD and non-AD patients after the Amy-PET were assessed by McNemar’s test, while changes in diagnostic confidence were assessed by paired samples T-tests. Differences in diagnostic confidence between AD and non-AD patients, with a positive or negative PET scan result, were assessed by a mixed factorial ANOVA with three independent Variables: a) AD (2 levels, AD versus non-AD, between); b) positivity to BAPL (2 levels, BAPL positive versus BAPL negative, between); c) time (2 levels, before the Amy-PET versus after the Amy-PET, within) resulting in a 2×2×2 design. The statistical analysis was performed with SPSS 23.0.
RESULTS
The patients’ general characteristics are shown in Table 1 and Supplementary Table 1. The average age was 69.1±8.6, 51.9% (n = 54) were male. The education was 9.8±4.6 y; the MMSE score was 23.7±4.6. The Amy-PET was positive in 66.3% (n = 69) patients.
Data are presented as mean±SD or n (%). Differences between groups were assessed using ANOVA with post hoc Bonferroni (age, education, MMSE) and χ2 tests (gender)
MMSE, Mini-Mental State Examination; AD, Alzheimer’s disease dementia; FTD, frontotemporal dementia; OD, other dementia diagnosis; aMCI > AD p < 0.05, bMCI > OD, p < 0.01; cMCI > AD/FTD/OD, p < 0.01
The impact on diagnosis
Overall, Amy-PET results confirmed the pre-PET clinical diagnosis in 82.7% of cases (86/104 patients). In 18 patients (17.3%), the initial diagnosis was changed after disclosing the Amy-PET results (McNemar’s test was not significant). No statistically significant differences were observed among the diagnostic groups in terms of diagnostic changes, also when the MCI subtypes were taken into consideration. A total of 81.8% (n = 36) of the patients in the MCI population with an MCI-AD diagnosis had a positive Amy-PET scan, whereas 83.3% (n = 15) of the patients in the AD group with an initial AD diagnosis had a positive scan. An overview of the impact Amy-PET had on clinical diagnoses is reported in Table 2.
Data are presented as mean±SD or n (%). No differences between groups were observed using ANOVA with post hoc Bonferroni (pre and post-PET diagnostic confidence, Δ diagnostic confidence)
AD, Alzheimer’s disease dementia; FTD, frontotemporal dementia; OD, other dementia diagnosis.
A negative PET scan in patients with an initial diagnosis of MCI-AD or AD led to a change in diagnosis in 10/11 (90.9%) of patients, whilst a positive scan in MCI-non AD changed the diagnosis in 41.6% (5/12). In FTD patients with a positive scan (2 out of 7), diagnosis changed to AD. The diagnosis was changed to AD in 25% (1/4) of the patients in the OD group that had a positive PET scan. Patients with a lower pre PET diagnostic confidence (51–70%) had more diagnostic changes (15 versus 3 p = 0,01) compared to the high confidence group (71–85%).
The impact on diagnostic confidence
No difference in diagnostic confidence prior to Amy-PET was observed among the diagnostic groups. Overall, the pre-PET diagnostic confidence increased from 69.1±8.1% to 83.5±9.1 after the PET results had been disclosed (p < 0.001), with a more evident, but not statistically significant increase, in the FTD group (Fig. 1). There was an increase in the diagnostic confidence in 93 patients (89%), whilst a decrease or no change was observed in 5 and 6 patients, respectively. Those patients whose diagnosis was changed after the PET had lower pre-scan diagnostic confidence levels (63±7.1% versus 70.4±7.8%, p < 0.01). The Amy-PET had a greater effect on confidence in younger patients (≤65 years) than it did in those > 65 years of age (19.4±8.2 versus 12.5±9.8, p = 0.01). When only the confidence for an AD diagnosis is considered, the greatest change in diagnostic confidence was seen to be related to a negative Amy-PET scan in those with an initial diagnosis of AD (p < 0.01) (Figs. 2 and 3). A 2×2×2 mixed factorial ANOVA was performed to assess diagnostic confidence changes (2 levels within each factor: pre-PET and post-PET confidence) between AD and non-AD patients (2 levels between each factor) with a positive or negative PET scan result (2 levels between each factor). Predictably, main effects resulted significant, with more confident diagnosis after PET disclosure (0.55±0.20 versus 0.56±0.34; F (1,100) = 25.25; p < 0.001; η2 = 0.20) in AD patients (0.71±0.17 versus 0.29±0.18; F (1,100) = 204.57; p < 0.001; η2 = 0.67) with a positive BAPL PET result (0.69±0.20 versus 0.29±0.14; F (1,100) = 170.46; p < 0.001; η2 = 0.63).
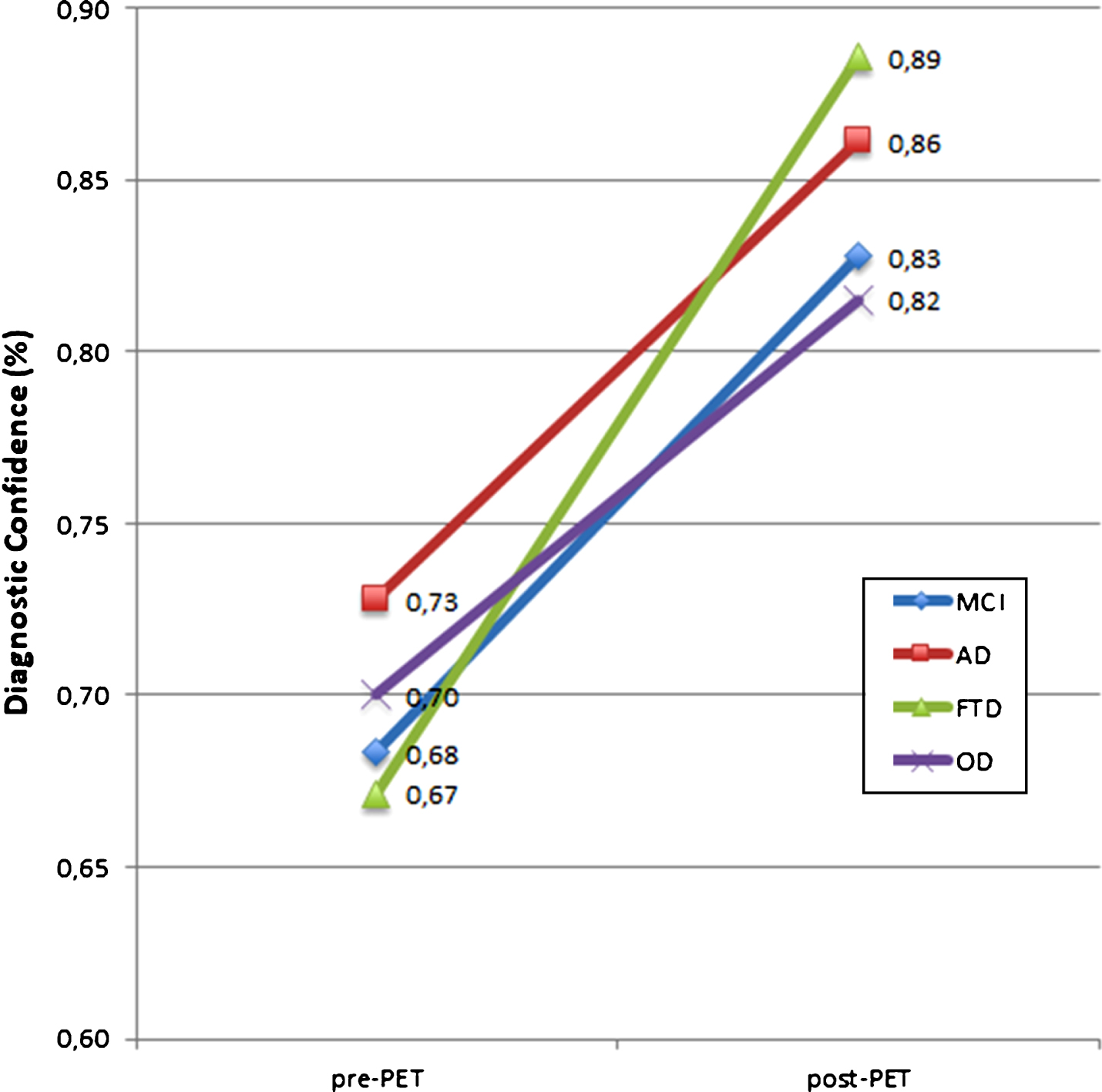
Diagnostic confidence pre and post PET disclosure. AD, Alzheimer’s disease dementia; FTD, frontotemporal dementia; OD, other dementia diagnosis; MCI, mild cognitive impairment.

Diagnostic confidence for an AD diagnosis in
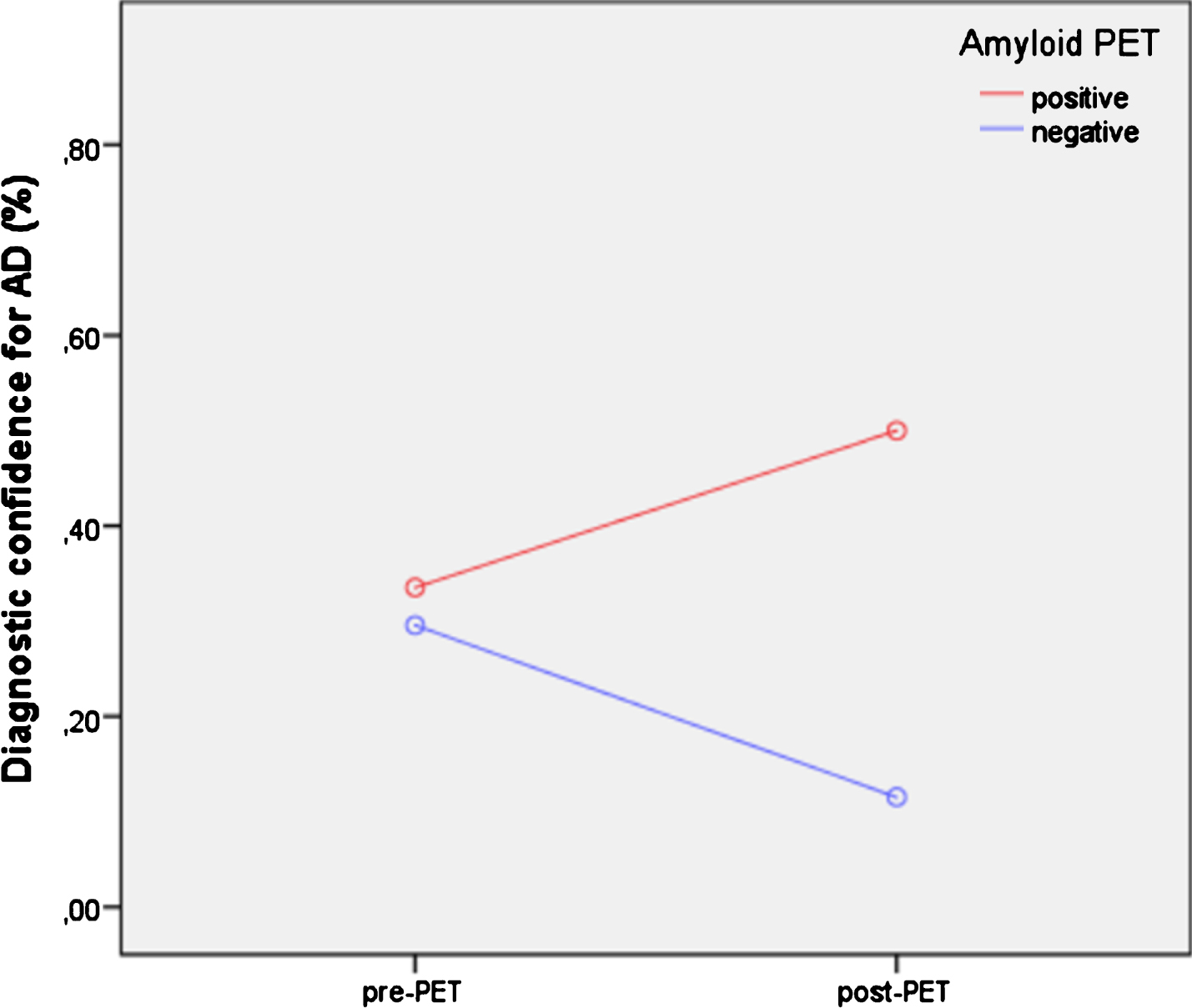
Diagnostic confidence for an AD diagnosis in
The impact on patient management
The PET results impacted the patient management plan in 73/104 patients (70%). When the medication prescription was taken into consideration, the disclosure of the PET results led to a change in only 7 patients (6.7% of the whole sample; 20% if only dementia patients are considered). Five of those with an initial diagnosis of non-AD dementia and a positive PET result, started Alzheimer medication. A negative PET scan led to a discontinuation of symptomatic therapies for AD in 2 cases (see Supplementary Table 2). The PET results determined a change in planned care in 46% of the patients leading to a shorter follow-up time in MCI PET positive cases. Also, a request for ancillary investigations in 19.2% (in most of the cases, an FDG-PET scan) was consequent to the disclosure of PET results. Globally, a positive PET result impacted on the medication prescription in suspected non-AD dementia and the follow-up of MCI patients, while a negative PET had more influence on the request for further diagnostic investigations (59% versus 15%, p < 0.05).
DISCUSSION
This study estimated the incremental value and diagnostic impact of [18F]florbetaben PET when added to the routine diagnostic workup for dementia in our memory clinic. Indeed, the assessment of the diagnostic utility of Amy-PET in clinical settings is an essential step for its correct definition as an AD biomarker. Our study aimed at investigating the value of Amy-PET in the final diagnosis and therapeutic strategies, and to provide a reliable picture of its impact in everyday clinical settings. Considering the new strict 5-phase approach, proposed for the validation of AD biomarkers, our study could be included as a phase IV study [30].
Overall, it was observed that the Amy-PET results did not have a strong impact on diagnoses, i.e., it led to changes in diagnosis in only 17.3% of the patients. Conversely, it did significantly increase diagnostic confidence in all the diagnostic groups (89%). When only patients with a high diagnostic confidence were taken into consideration, i.e., the neurologists had less diagnostic doubts even before the PET scans, there were only three diagnostic changes. The impact of Amy-PET on diagnostic confidence was in line with previous studies [14–21], while the percentage of diagnostic changes was significantly lower than that reported in literature (17.3% versus about 30% of cases) [12]. Although an overall comparison among different studies is not easily feasible, the lower rate of change in diagnosis does not seem to be explained by the general characteristics of the study population, (i.e., age, cognitive status, and different dementia subgroups). In our study a slightly higher rate of positive PET was observed but most notably, when AD was suspected (MCI-AD or AD) before PET disclosure, only 11 patients (17.5%) had a negative scan, a result well below the average (31.5%) reported by clinical studies [13]. In this regard, the presence of a fully standardized protocol for the routine diagnostic workup represents a valid ally to avoid misdiagnosis. Moreover, an accurate routine diagnostic assessment is mandatory if a correct request and interpretation of second line investigations are to be made, among which amyloid PET is included. However, considering our results, we believe that the key element is represented by a complete neuropsychological assessment, especially in MCI and mild dementia, where only specific cognitive domains are impaired. We are of the opinion that very often the neuropsychological assessments are limited to neuropsychological batteries, i.e., Alzheimer’s Disease Assessment Scale cognitive subscale, which are able at staging cognitive impairment but less accurate when there is a need to explore the specific cognitive domains. Making a comparison with the data available in the literature, only few studies accurately describe the neuropsychological battery [16, 20], and in one large study, only 60% of patients underwent a neuropsychological assessment [15]. Moreover, none of the studies seem to assess the impairment of episodic memory— the cognitive hallmark of AD— by the means of the FCSRT. This tool, unlike other memory tests, has been designed to better control the learning process in order to ensure encoding and thus to distinguish retrieval from storage deficits, the latter being more specific for temporo-mesial functioning and AD degeneration. In our experience, the FCSRT has been shown to be a reliable clinical marker for AD, by mapping the memory networks usually impaired in the disease [31]. The use of FCSRT was also recommended by the International Working Group [2].
A negative scan in suspected AD before PET disclosure led to diagnostic changes in non-AD diseases in 91% of cases, confirming the high negative predictive value of amyloid imaging probes. Despite the inconsistent scan, one patient had AD diagnosis confirmed by our clinicians, supporting the evidence that a small percentage of clinical AD are characterized by neuropathological findings other than Aβ, such as argyrophilic grain disease, hippocampal sclerosis or tangle predominant dementia [32] (classified as suspected non amyloid pathology according to the NIA-AA criteria for AD). Moreover, the sensitivity of [18F]florbetaben for brain amyloid pathology is 98%, meaning that there may be about two false negatives in our sample [33].
After PET disclosure, the diagnosis was changed to AD in 8 (28%) patients with a pre-scan diagnosis of non-AD. Noteworthy is the fact that diagnosis was changed to AD in FTD and other dementia groups in 100% and 25% of cases, respectively. Among the non-AD dementia subtypes, FTD has a lower amyloid load than do healthy subjects of the same age. Consequently, a positive scan has a high negative predictive value in suspected FTD. In this context, amyloid PET allows for the often difficult clinical distinction between an atypical presentation of AD (frontal variant and logopenic progressive aphasia in particular) and FTD. In the OD group with positive PET, we observed a significantly lower rate of change in diagnosis (25% versus 74%) compared to the results reported by a systematic review [13]. This difference probably reflects the improvement of knowledge on amyloid pathology achieved in recent years and our results are not surprising considering the global prevalence of amyloidosis in non-AD dementia [9]. To confirm this, our results are in line with the diagnostic change rate reported by Zwan et al. [34] in a recent study. As to the standardized workup, the knowledge of the prevalence of Aβ deposition in dementia syndromes is a key prerequisite for a correct request and interpretation of amyloid PET scans. Therefore, although a negative PET result remained the most useful clinical source of added value, both in suspected AD (Fig. 2) and non-AD, physicians can extrapolate diagnostic information also from the positive predictive value of amyloid PET imaging.
It was observed that the impact on diagnostic confidence was more pronounced in early onset patients where there is less probability of “age-related” brain amyloidosis [8], which is typically observed in older patients. As reported in appropriate use criteria [11], the use of amyloid PET should be carefully weighted in older patients (e.g., >75 y) where the presence of asymptomatic amyloid deposition is common and may play a confounding role in a correct diagnosis.
Overall, Amy-PET scans had little impact on the medication plan (6.7% of the whole population, 20% excluding MCI patients) and led to the prescription of symptomatic drugs for AD in only five patients. On the other hand, a negative scan led to a discontinuation of AD therapies in two subjects, a decision that, although controversial, is justified by reports of adverse effects and ineffectiveness in etiologies other than AD [35, 36]. The low impact of Amy-PET on treatment plans depends on the lack of disease modifying drugs for AD and the absence of valid therapies in patients with mild cognitive symptoms that represented most of our studied population. Moreover, the low rate of change in diagnosis reported in our study, as well as a conservative approach (where no MCI patients were treated with cholinesterase inhibitors), may have influenced the low impact on the treatment plan. However, when making a cost/effective analysis of amyloid PET imaging, it is obligatory to take the fundamental role amyloid biomarkers play in patient selection into consideration for future clinical trials. Likewise, also the advantages related to a negative scan and a benign diagnosis in MCI patients is not to be underestimated. In the MCI condition, a positive PET significantly increases the risk of progression to dementia at any age. In addition, it allows attention to be focused on those patients at high risk of clinical progression, shortening the follow-up time and allowing for planning of the best non-pharmacological strategies (e.g., physical training, cognitive stimulation).
Limitations
The present study tries to offer a realistic picture of the utility of Amy-PET imaging in a routine, naturalistic, tertiary clinical setting. Nevertheless, given the design of the study, it is important to note that the outcome is a real reflection of the investigators opinions and behaviors, not the result of a gold standard correct diagnosis or proof of an effective management choice. For the same reason, even though our standardized workup, which includes a complete neuropsychological assessment, seems to impact on the diagnostic value of Amy-PET, this conclusion cannot be considered as a general principle of clinical practice yet.
Conclusions
Amyloid PET is a useful tool and a source of added value in dementia diagnosis, being able to change diagnosis in nearly 1 patient out of 5, significantly increasing the diagnostic confidence. However, in clinical practice, the use of a complete neuropsychological assessment, including the FCSRT, may reduce the amyloid PET influence on change of diagnosis, and the real impact of amyloid PET should always be weighed up together with an accurate standardized diagnostic workup. Further studies are required to better investigate the impact of first-line investigations, including, above all, the neuropsychological assessment, on the diagnostic value of amyloid PET. In this regard, future research should also focus on cost-effectiveness for the correct implementation of amyloid PET in clinical practice.
DISCLOSURE STATEMENT
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/18-0646r3).