
Abstract
Background:
Free and Cued Selective Reminding Test (FCSRT) is a reliable cognitive marker for Alzheimer’s disease (AD), and the identification of neuropsychological tests sensitive to the early signs of AD pathology is crucial both in research and clinical practice.
Objective:
The study aimed to ascertain the ability of FCSRT in predicting the amyloid load as determined from amyloid PET imaging (Amy-PET) in patients with cognitive disorders.
Methods:
For our purpose, 79 patients (71 MCI, 8 mild dementia) underwent a complete workup for dementia, including the FCSRT assessment and a [18F]florbetaben PET scan. FCSRT subitem scores were used as predictors in different binomial regression models.
Results:
Immediate free recall and delayed free recall were the best predictors overall in the whole sample; whereas in patients <76 years, all models further improved with immediate total recall (ITR) and Index of Sensitivity of Cueing (ISC) resulting the most accurate in anticipating Amy-PET results, with a likelihood of being Amy-PET positive greater than 85% for ITR and ISC scores of less than 25 and 0.5, respectively.
Conclusion:
FCSRT proved itself to be a valid tool in dementia diagnosis, also being able to correlate with amyloid pathology. The possibility to predict Amy-PET results through a simple and reliable neuropsychological test might be helpful for clinicians in the dementia field, adding value to a paper and pencil tool compared to most costly biomarkers.
Keywords
INTRODUCTION
Brain amyloid-β (Aβ) deposition is a key feature of Alzheimer’s disease (AD) starting many years before clinical symptoms and reaching a substantial plateau in mild cognitive impairment (MCI) [1, 2]. Subjects with biomarker evidence of AD pathology but no symptoms of dementia are considered to have “preclinical AD” [3], whereas in the presence of symptomatic disease stage, “prodromal AD” is diagnosed [4]. Prodromal AD is considered a transitional high-risk state for the progression of cognitive decline to AD dementia.
Both cerebrospinal fluid (CSF) and positron emission tomography (PET) amyloid markers have been incorporated into the revised research criteria for AD [5, 6], defining the corresponding pathological stages of cognitive symptoms that range along a continuum. Amyloid pathology is detectable in vivo through CSF Aβ42 sampling and amyloid PET (Amy-PET) radiotracers [7], and recent findings have demonstrated the superiority of Amy-PET over CSF biomarkers in terms of sensitivity/specificity and diagnostic accuracy for AD [8, 9]. Amy-PET tracers, including [18F]florbetaben, have displayed a very good concordance with amyloid load observed postmortem, binding to Aβ with high sensitivity and specificity [10, 11]. The use of Amy-PET and CSF biomarkers is essential for early identification and early intervention of AD in research and clinical care. However, as reported in a comprehensive meta-analysis [12], the prevalence of amyloid pathology increases with age, reaching more than 40% in the healthy elderly over 80 years. Accordingly, the use of Amy-PET should be carefully weighed in older patients (e.g., >75 years) where the presence of asymptomatic amyloid deposition is common and may impact the diagnostic value and the cost-effectiveness of the PET scans [13].
Up to now, Amy-PET data are mainly being used for the characterization of global amyloid burden into dichotomous positive/negative categories, though the identification of regional amyloid burden may help to improve the diagnostic accuracy. In this regard, the amyloid load in the precuneus and posterior cingulate cortex could be a more specific marker for AD, compared to the global burden [9, 14].
Given the widespread prevalence of cerebral amyloidosis in non-AD dementia and the healthy elderly, the efficacy of Amy-PET tracers in clinical practice is still under debate [15]. Moreover, Amy-PET scans are available in few tertiary memory centers, thus limiting the number of subjects who should undergo a complete assessment. For the above reason, more available tools sensitive to the early deficits, as neuropsychological tests, could be a valid alternative in everyday clinical routine. In this regard, as specifically recommended by the International Working Group (IWG) criteria [4, 16], the Free and Cued Selective Reminding Test (FCSRT) is particularly useful in assessing episodic memory impairment among patients with AD dementia. This tool, unlike other memory tests, has been developed to better control the learning process in order to ensure encoding and thus to distinguish retrieval from storage deficits, the latter being more specific for temporo-mesial dysfunction and AD degeneration [17]. In our experience, the FCSRT has been shown to be a reliable clinical marker for AD, by mapping the brain areas usually impaired in the disease [18]. Recent studies confirmed that decrements in FCSRT subitems correlate with AD pathology, detected by CSF biomarkers [19–21], and hippocampal atrophy measured by high field magnetic resonance imaging (MRI) [22–24].
In this study, we aimed at investigating the associations between Aβ deposition, revealed by Amy-PET, and baseline FCSRT subitems scores in <76 years and older patients with MCI and mild dementia and, at the same time, to assess the relationships between FCSRT subitems and Amy-PET scan focusing on the regional Aβ deposition in the precuneus/posterior cingulate cortex, a target area early and deeply involved in AD pathology. The possibility to predict Amy-PET results through a simple and reliable neuropsychological test might be helpful for clinicians in the dementia field, adding value to a paper and pencil tool compared to most costly biomarkers.
METHODS
Study population
The present study prospectively included 79 patients referred to the Center for Cognitive and Dementia Disorders (AUSL) and the Dementia Unit at the University Hospital of Parma. All patients underwent a complete routine work-up for dementia, encompassing general and neurological examination, routine blood tests, and structural imaging. The neuropsychological evaluation was made by a team of experienced neuropsychologists. It included specific cognitive domains for verbal and spatial memory, visuo-constructive, attentional and executive functions, logical reasoning, naming, and verbal fluency. The general cognitive level and abstract reasoning were assessed by the Mini-Mental State Examination (MMSE) and Raven’s Advanced Progressive Matrices (PM 47), respectively. Other tests included the Multiple feature target cancellation and Stroop test (attention and executive domains), FCSRT, delayed recall of the Rey-Osterrieth Complex Figure and the Digit Span forward (memory), Clock Drawing Test, the Rey-Osterrieth Complex Figure (praxis and visuospatial), the Boston Naming Test, the Semantic and phonological verbal Fluency Test (language), the Geriatric Depression Scale, and the Neuropsychiatry Inventory (mood and psychopathology), as well as ADL and IADL (basic and functional activities of daily living). In particular, verbal learning was investigated with the FCSRT [25]. Inclusion criteria were: objective cognitive deficits, an age range at the time of PET of 45–85 years, PET examinations within three months of the baseline neuropsychological assessment. Exclusion criteria were Clinical Dementia Rating >1 and MMSE total score less than 20, history of major psychiatric disorder or epilepsy, drug and/or alcohol abuse, other neurological conditions likely to affect cognition (i.e., hypoxia, head injury), clinically relevant abnormalities on neuroimaging, active malignancy and a history of major vascular events such as stroke/hemorrhage, previous participation in any experimental study with a disease-modifying therapy and/or an amyloid targeting agent. MCI diagnosis met the Peterson criteria [26, 27], while the clinical diagnosis of AD dementia was based on the National Institute on Aging-Alzheimer’s Association (NIA-AA) criteria [5]. Clinical diagnoses of the neurodegenerative diseases other than AD were established according to clinical criteria [28–32]. According to the neuropsychological profiles, MCI subjects (n = 71) were classified in the following four MCI subtypes: Amnestic MCI-Single Domain (aMCI-sd; n = 17), Non-Amnestic MCI Single Domain (naMCI-sd; n = 12), Amnestic MCI-Multiple Domain (aMCI-md; n = 27), and Non-Amnestic MCI-Multiple Domain (naMCI-md; n = 15). Globally, aMCI (sd and md) were 44/71 (62%).
The study was conducted according to the Declaration of Helsinki, and all study participants signed a written consent approved by the local Ethics Committee.
Free and Cued Selective Reminding Test
The picture version of the FCSRT (pFCSRT) was used [25]. A card with four pictures is placed in front of the patient, and in the study phase, the subject is asked to point and name each item when the corresponding category cue is given verbally by the examiner. After the correct identification of all four items, the card is removed, and immediate cued recall of those four items is tested by verbally presenting the four corresponding cues. If the subject fails to recall an item in response to the corresponding cue, the card is shown again, the item must be selected and named, and then another opportunity of immediate cued recall is given to the subject. After the completion of the immediate recall of the four items, the next set of items is presented until all 12 items are identified and retrieved in cued recall. This procedure allows a correct initial encoding. The memory phase is then based on three subsequent recall trials, preceded by an interference task (counting backwards for 20 s). Each recall trial consists of two parts: 2 min to freely recall as many items as possible and cued recall of any non-retrieved item by means of the corresponding category cue. If the subject fails to retrieve the item with the category cue, he/she is verbally reminded of the item. After 30 min, delayed recall is proposed using the same procedure as in immediate recall. Six scores are then calculated: 1) immediate free recall (IFR): sum of free recall in trials 1, 2, and 3 (range 0–36); 2) immediate total recall (ITR): sum of free and cued recall in trials 1, 2, and 3 (range 0–36); 3) delayed-free recall (DFR) (range 0–12); 4) delayed total recall (DTR) (range 0–12); 5) Index of Sensitivity of Cueing (ISC): (IFR–ITR)/(ITR-36) (range 0–1); 6) number of intrusions.
The ISC is a measure dedicated to evaluating the efficacy of semantic cues during the retrieval processing from stored information; in the case of IFR = 36, ISC is set to 1.
Amyloid PET imaging
PET scans were performed using a whole-body hybrid system Discovery IQ (GE Healthcare) operating in the three-dimensional detection mode. The head holder was used to restricting patient movement, and the head movement was checked on a regular basis.
All cerebral emission scans began 90 min after intravenous injection of 4 MBq/kg weight (240–360 MBq) of [18F]florbetaben. For each subject, 10-min frames were acquired for all patients to ensure movement-free image acquisition. All Amy-PET sinograms were reconstructed with a 3-D iterative algorithm, with corrections for randomness, scatter, photon attenuation and decay, which produced images with an isotropic voxel of 2×2×2 mm and a spatial resolution of approximately 5-mm full-width at a half-maximum (FWHM) in the center of the field of view. The cerebellar white matter was used as the reference region for Amy-PET data.
Visual blinded PET image assessment was made by two trained, independent readers (M.S. and L.R.) with the previously described technique (excellent inter- and intra-reader agreement, k = 0.98) [33, 34]. The assessments of [18F]florbetaben PET images were made using a three-grade scoring system (RCTU, regional cortical tracer uptake) comparing the activity in cortical gray matter (frontal cortex, lateral temporal cortex, posterior cingulate cortex/precuneus, and parietal cortex) with activity in adjacent cortical white matter. The RCTU scores (1 = no binding, 2 = minor binding, and 3 = strong binding) were then condensed into a single three-grade scoring system for each PET scan, the BAPL (brain amyloid-β plaque load) score: 1 = no Aβ load, 2 = minor Aβ load, 3 = significant Aβ load and the resulting scores were then condensed into a binary interpretation (score 1 = negative; score 2 or 3 = positive). The rating of BAPL was based on a validated method that reached a sensitivity of 98% in an autoptic confirmation study [35]. Operationally, the BAPL score corresponded to the highest RCTU scores among the four regions of interest.
Statistics
BAPL (brain amyloid-β plaque load) scores condensed into binary interpretation (0 = negative; 1 = positive) were used as dependent variable in binomial regression models using different FCSRT scores.
Two different BAPL scores were used, the first involving the whole cortex (BAPLtotal), the latter including only the posterior cingulate cortex/precuneus (BAPLpp).
IFR, ITR, DFR, DTR, and ISC scores were used as predictors (independent variable) in different binomial regression models using a logit link functions [36]. Because of the high correlations between different FCSRT scores, each score was tested separately by the Wald test [37]. Models were fitted both in the whole sample and in the <76 years old group, giving a total of 4 models for each predictor.
Statistical analyses were performed using RStudio 1.2.1114 (RStudio Team, 2018), R 3.5.1 (R Core Team, 2018) with “plotly”, “psych”, and “tidyverse” packages [38, 39]. The results were not corrected for multiple comparisons.
RESULTS
The patients’ general characteristics are shown in Table 1. The average age was 70.4±8.1 and 54.4% (n = 43) were male. The average years of education was 10.3±4.6 years, and the average MMSE score was 25.3±2.9. The Amy-PET was positive in 65.8% (n = 52) patients.
Demographic and clinical features
BAPL total, brain amyloid-β plaque load in the whole cerebral cortex; BAPL precuneus/posterior cortex, brain amyloid-β plaque load in the precuneus and posterior cingulate cortex; aMCI-sd, amnestic MCI-single domain; naMCI-sd, non-amnestic MCI-single domain; aMCI-md, amnestic MCI-multiple domain; naMCI-md, non-amnestic MCI-multiple domain.
According to the neuropsychological profiles and the clinical follow up, we intercepted six atypical presentations of AD (3 frontal variant of AD, 2 posterior cerebral atrophy, 1 logopenic progressive aphasia) among patients with amyloid positive scans (6 out of 52, 11.5%). In the Amy-PET negative group (n = 27), we diagnosed fifteen patients with neurodegenerative diseases other than AD (7 frontotemporal dementia, 3 corticobasal syndrome, 2 dementia with Lewy bodies, 2 suspected non-Alzheimer’s pathology, 1 progressive supranuclear palsy) and twelve patients with a non-neurodegenerative diagnosis (mainly a psychiatric disorder).
Considering the whole sample of patients (age 42–88 years), IFR (p = 0.035) and DFR (p = 0.021) significantly predicted the BAPLtotal results, whereas ISC showed a trend toward significance (p = 0.098). By using BAPLpp as dependent variable, all the regression binomial models were significant, with the best prediction maintained by DFR (p = 0.002) and IFR (p = 0.01) (Table 2, Figs. 1 and 2).
Odd ratios, 95% confidence intervals and p-values of the 20 different fitted models, resulting from five FCSRT predictors×2 samples (whole and <76 y)×2 cortical area (Total cortex and Precuneus/Posterior Cingulate cortex)
BAPL total, brain amyloid-β plaque load in the whole cerebral cortex; BAPL precuneus/posterior cortex, brain amyloid-β plaque load in the precuneus and posterior cingulate cortex; IFR, immediate free recall; DFR, delayed free recall; ITR, immediate total recall; DTR, delayed total recall; ISC, Index of sensitivity of cueing; (*) Increase of probability of Amyloid PET positivity (%) for each 0.1 point less.

FCSRT subitems scores and PET scan results (BAPLtotal, brain amyloid-β plaque load in the whole cerebral cortex) in the whole sample. IFR, immediate free recall; DFR, delayed free recall; ITR, immediate total recall; DTR, delayed total recall.

FCSRT subitems scores and PET scan results (BAPLpp, brain amyloid-β plaque load in the precuneus and posterior cingulate cortex) in the whole sample. IFR, immediate free recall; DFR, delayed free recall; ITR, immediate total recall; DTR, delayed total recall.
Considering only patients younger than 76 years (age 42–75), regression models with FCSRT subitems further improved. IFR (p = 0.019), DFR (p = 0.027), ITR (p = 0.013), and ISC (p = 0.014) significantly predicted the BAPLtotal results, whereas all the FCSRT subitem models were significant by using BAPLpp as dependent variable. Compared to the analysis of the whole sample, in patients ≤76 years, the best predictors of BAPL results (both BAPLtotal and BAPLpp) were represented by ITR and ISC (Table 2, Figs. 3–5). Further analysis of only patients >75 years (n = 25) found no significant predictive model. A point by point comparison between FCSRT subitem scores and the probability of being Amy-PET positive is provided in Supplementary Tables 1 and 2.
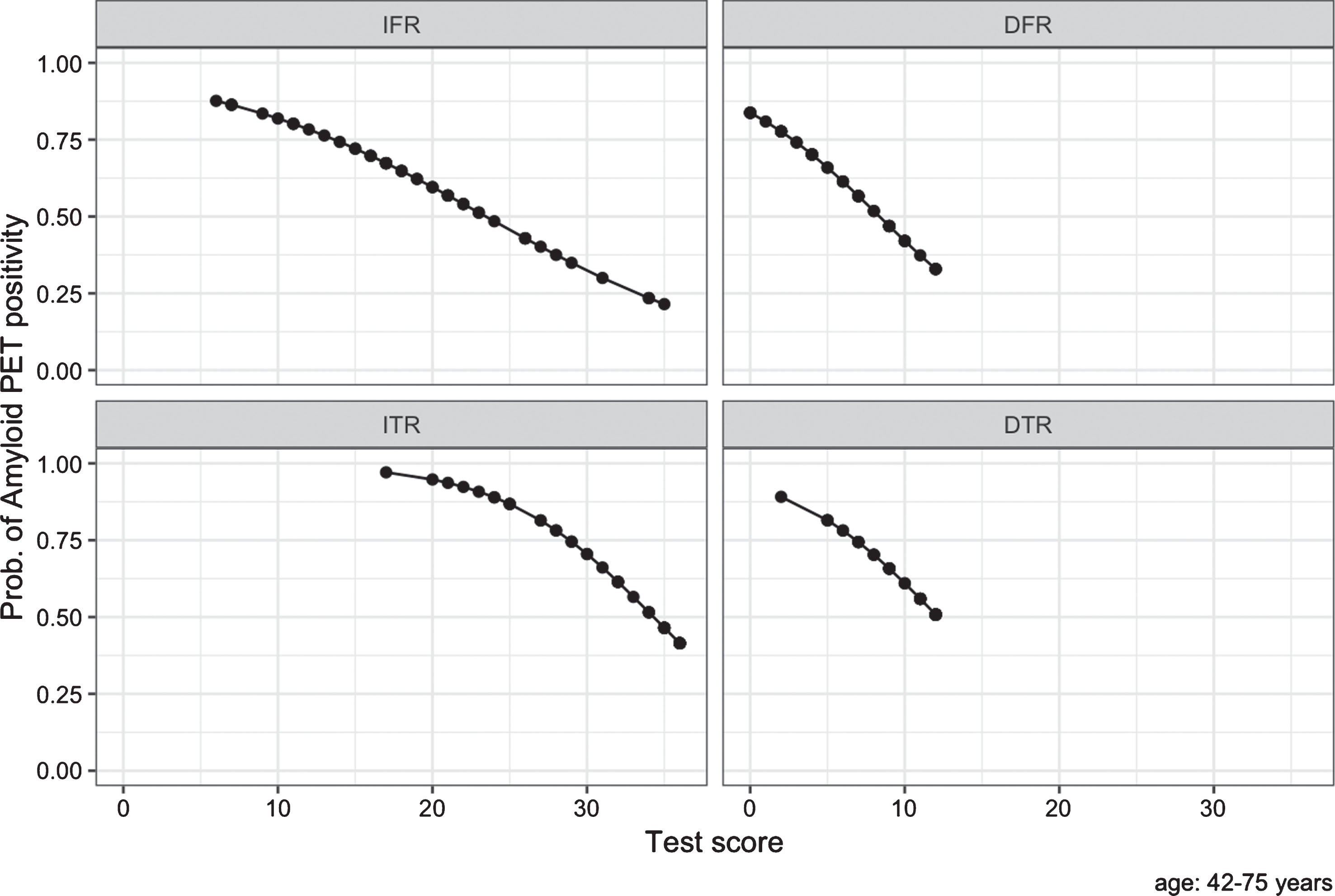
FCSRT subitems scores and PET scan results (BAPLtotal, brain amyloid-β plaque load in the whole cerebral cortex) in <76 y patients. IFR, immediate free recall; DFR, delayed free recall; ITR, immediate total recall; DTR, delayed total recall.

FCSRT subitems scores and PET scan results (BAPLpp, brain amyloid-β plaque load in the precuneus and posterior cingulate cortex) in <76 y patients. IFR, immediate free recall; DFR, delayed free recall; ITR, immediate total recall; DTR, delayed total recall.
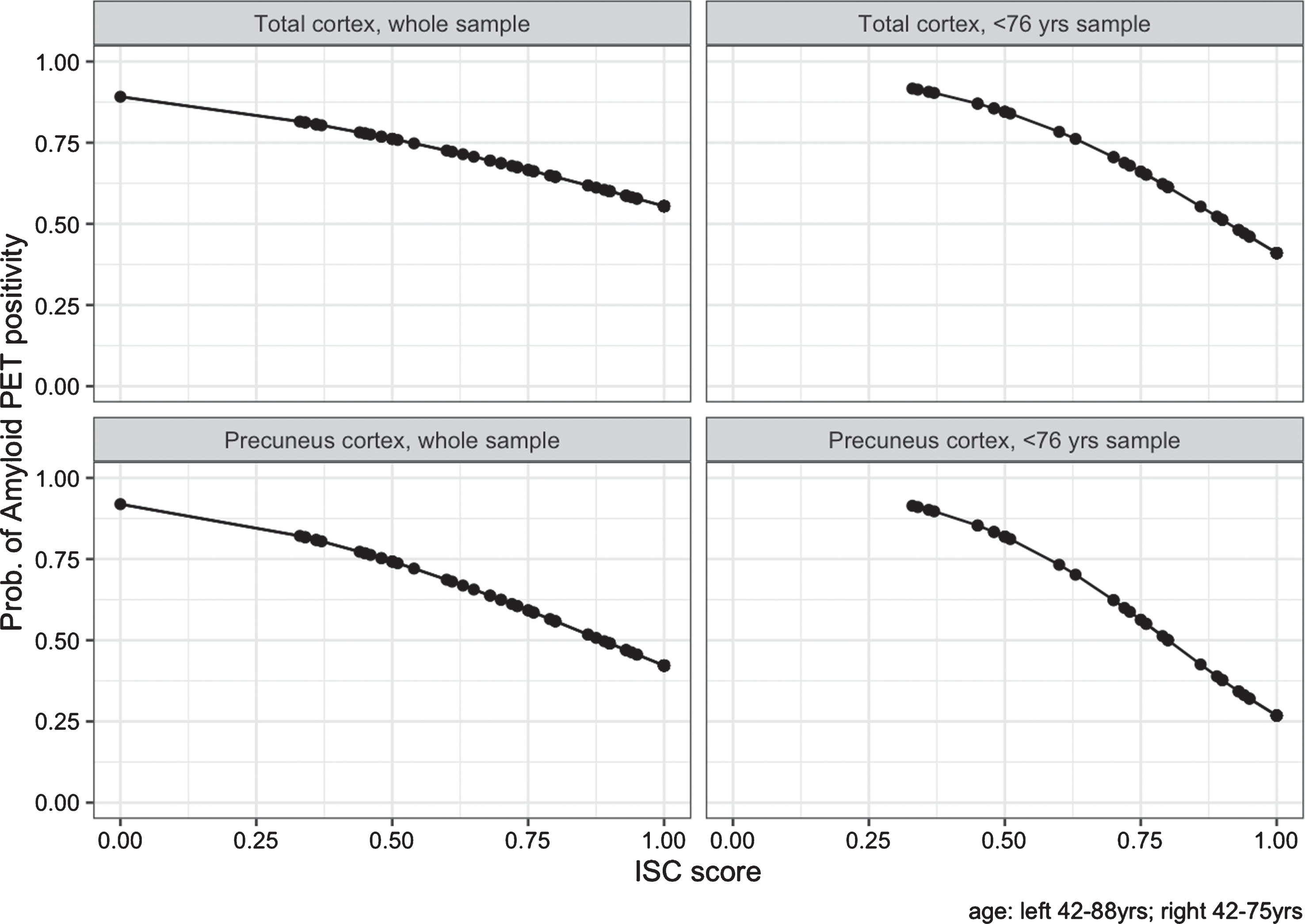
Index of sensitivity of cueing (ISC) scores and PET scan results. On the left in the whole sample, on the right in <76 y patients. Above Amy-PET as BAPLtotal, below Amy-PET as BAPLpp.
DISCUSSION
In this study, we provided evidence of the ability of FCSRT to predict the [18F] florbetaben PET results and thus the Aβ deposition in MCI and mild dementia population.
The present study tried to track how the probability of having an Amy-PET+ changed across the different scores and subitems of the FCSRT. As a general rule, low subitem scores had a high likelihood of being Aβ positive. In the whole sample, more than 80% of the patients with an IFR score of less than 10 (out of 36) are positive to Amy-PET (Fig. 1, Supplementary Table 1). These results should be taken into account in clinical settings in order to avoid more costly biomarkers, suchas Amy-PET.
As reported in appropriate use criteria [13], the use of Amy-PET should be carefully weighed in older patients (e.g., >75 years) where the presence of “asymptomatic” amyloid deposition is common and may play a confounding role [12]. In this regard, we performed an ad hoc analysis in patients younger than 76 years. As expected, in this population, the ability of pFCSRT to predict brain amyloidosis improved, but interestingly, changed the best predictors among the different subitems. While in the whole sample free recall (both IFR and DFR) scores better discriminated among Amy-PET+ and –, in subjects younger than 76 years, we found a significant association of Amy-PET results to ITR and ISC scores, with a probability of being [18F]florbetaben positive greater than 85% when ITR score is less than 25 (out of 36), and greater than 95% when ITR score is less than 20. Also an ISC score of less than 0.5 is associated with positive scans in more than 85% of the patients (Figs. 3 and 5, Supplementary Tables 1 and 2). The stronger relationship between younger subjects and decline in ITR compared with free recall supports the hypothesis that in younger patients, when the semantic cue is ineffective, it reflects more the early hippocampal dysfunction than it appears in older patients where, more often, mixed pathology coexist [40].
FCSRT scores’ prediction would seem to be less effective when scores are high, resulting in a limited negative predictive value. At the same time, the prediction ability of FCSRT was globally reduced when we considered only patients >75 years. Nevertheless, this is not surprising, considering the high prevalence of amyloid pathology in MCI and demented patients, especially in the older ones.
Although a complete comparison is not easily feasible, a comprehensive meta-analysis reported that the prevalence of Aβ pathology in MCI patients not further classified (mean age 67.9 years) is 47.9% (1,533 out of 3,195 patients) [12]. In a comparable population of our study, considering the age and cognitive status (Table 1), the only use of FCSRT allowed us to better stratify the prevalence of brain amyloidosis from 20% to more than 90% (Fig. 3). Moreover, in these subjects, IFR score could be useful to improve the negative predictive value, since a score of more than 30 and 33, correlated with the presence of amyloid pathology in less than 30% and 25% of the cases, respectively (Supplementary Table 1).
At variance with the current opinion that FCSRT is helpful only in amnestic presentations of AD [6], it is important to note that our study tried to offer a realistic picture of the diagnostic utility of FCSRT in a real-world tertiary clinical setting which also includes atypical presentations of AD. Moreover, the reliability of the results, despite the presence of patients with suspected non-Alzheimer’s pathology (SNAP according to the NIA-AA criteria) and with non-neurodegenerative diseases (psychiatric disorders in particular, often mimicking amnestic MCI), should be taken into consideration to strengthen the clinical use of FCSRT. Today, despite the great progress in the biological definition of AD [6], the neuropsychological examination remains an important tool in the process of defining different cognitive profiles among dementias and patient selection for clinical trials. In this regard, FCSRT has been already shown to be a reliable marker for AD by correlating with both metabolic [18, 42] and structural networks [23, 43] involved in the early phases of the disease. Moreover, the recommendation by IWG criteria on its clinical accuracy in differentiating typical (amnestic) AD from other neurodegenerative diseases is highly corroborated by a large amount of literature where participants tested positive at the FCSRT were at higher risk to develop AD than subjects with normal FCSRT scores. FCSRT was also able to predict years before AD diagnosis [19, 45].
The present study demonstrated that FCSRT correlates with the amyloid load by using a visually-based method Amy-PET scan. The possibility to assess the AD pathology, through a simple tool (as FCSRT), was also the main aim of recent studies, where the amyloid pathology was often determined through CSF biomarkers and in healthy subjects. Wagner et al. [21], using the word version of FCSRT (wFCSRT), found in MCI that free and total recall were the best indicators between CSF AD-positive and CSF AD-negative, thus improving the CSF-based AD classification accuracy. Schindler et al. [20], on a large sample of cognitively healthy subjects, found the free recall portion of FCSRT the best and earliest indicator of the declining cognition in the high CSF tau/Aβ42 group, while for Papp et al. [19], cued recall was found to be the best parameter in identifying Aβ positive normal individuals at highest risk of clinical progression. Based on pFCSRT performance, Grober et al. [45], developed the Stages of Objective Memory Impairment (SOMI) model, where amyloid positivity starts from SOMI level 1 (subtle memory impairment) and through multiple intermediate steps ending to level 3 when storage impairment is associated with amyloid, tau, and neurodegenerative signs of dementia. Operationally, in SOMI 1, free recall score ranges from 30 to 25, while total recall is normal, and patients are at risk for clinical AD.
The most recent research on Amy-PET tracers is trying to overcome the interpretation of the results just as positive and negative and only as a global burden of amyloid pathology. If the mean levels of amyloid accumulation may not be the most reliable discriminator in MCI, preliminary observations seem to suggest that the identification of regional amyloid load may help to improve the diagnostic accuracy [46, 47]. Therefore, we performed a further regression analysis focusing on the regional uptake in the precuneus/posterior cingulate cortex as the dependent variable. The inclusion of this area comes from convergent evidence on the pivotal and early role of the precuneus and posterior cingulate cortex in AD degeneration [48–50] Moreover, the Amy-PET uptake in a single brain area as the precuneus/posterior cingulate cortex seems to be more specific for AD compared to global uptake [9]. FCSRT subitems further improved their ability to predict the Amy-PET scan when using the precuneus/posterior cingulate cortex (BAPLpp) instead of BAPLtotal. In particular, FCSRT improved its specificity when the target area was the BAPLpp (i.e., in <76 years group, less than 15% of patients had BAPLpp + with IFR scores close to the maximum) (Fig. 4).
Overall, few studies have explored the relationships between FCSRT scores and Amy-PET results and/or neuropathological stages [51], and, to our knowledge, our results are among the first showing a clear and prompt-to-use demonstration of the ability of the test in predicting AD pathology. Considering the cost-effectiveness and the limited availability of Amy-PET scans, the evidence provided in the present study suggests the need to include the FCSRT test in the assessment of MCI and mild dementia.
Limitations
Despite the robust results provided, we acknowledge that the present study has some limitations that need to be addressed. Given the naturalistic approach, the study included not only persons with MCI but also a small percentage of mild dementia (10.1%, 8 out of 79), thus reducing the homogeneity of the sample. Secondly, [18F]florbetaben scan analyses were not based on semi-quantitative methods, such as quantification using standardized uptake value ratios (SUVRs). However, the add-on value of SUVRs in clinical practice is still under debate, and some studies report that the two methods perform similarly in classifying Amy-PET scans as positive or negative for brain Aβ [52]. Lastly, in the absence of a control group of healthy subjects and given the lack of statistical significance in the small sub-group of patients over 75 years, our approach and results need to be validated by further studies, especially in older patients.
Conclusion
FCSRT has been confirmed to be a valid tool in dementia diagnosis, also being able to predict the amyloid pathology in the early phases of the disease. Future studies on MCI and cognitively healthy subjects at risk of developing dementia are needed to help more appropriate patients’ selection for prevention policies and clinical trials.