
Abstract
Subjective cognitive complaints in cognitively normal individuals are a relevant predictor of Alzheimer’s disease (AD), cerebrovascular disease, and age-related tauopathy. Complaints starting after the age of 60 increase the likelihood of preclinical AD. However, this criterion is arbitrary and current data show that neurodegenerative disorders likely start before that age. Further, data on the role of subjective complaints below the age of 60 in individuals qualifying for subjective cognitive decline (SCD) are lacking. We investigated the association of subjective cognitive complaints with an extensive number of neuroimaging, demographic, clinical, and cognitive measures in individuals fulfilling criteria for SCD below and above the age of 60. Nine complaints were scored in 416 individuals. Complaints were related to a higher load of white matter signal abnormalities, and this association was stronger the more subclinical changes in personality, interest, and drive were reported. In individuals <60 years, complaints were associated with lower global cognitive performance. In individuals ≥60 years, complaints were related to greater global brain atrophy and smaller total intracranial volume, and this association was stronger the more subclinical difficulties in activities of daily living were reported. Also, complaints were associated with increased depressive symptomatology irrespective of age. We conclude that complaints below the age of 60 may be associated with subtle signs of brain pathology. In the community, screening for risk of future cognitive decline should include subjective cognitive complaints, depressive symptomatology, and subclinical reduced cognition (<60 years)/activities of daily living (≥60 years), supported by basic neuroimaging examinations.
Keywords
INTRODUCTION
Subjective cognitive decline (SCD) has been postulated as the first clinical manifestation of Alzheimer’s disease (AD) [1]. However, an open discussion is when to start considering complains as a predictor of neurodegenerative diseases. The SCD Initiative (SCD-I) proposed that complaints starting after the age of 60 increase the likelihood of preclinical AD [1]. This criterion stands on “the increasing prevalence of AD-related neuropathological alterations starting at midlife, which may trigger SCD after neuronal dysfunction affects cognitive abilities” (quoted from [1]). However, the SCD-I acknowledges that the cut-off of 60 years is arbitrary and current data show that neurodegenerative disorders begin up to 20 years before the onset of dementia [2], thus likely starting before the age of 60. Furthermore, although it is suggested that complaints below the age of 60 may be more closely related to non-neurodegenerative causes [1], there are almost no studies in individuals under that age who fulfill inclusion criteria for SCD (i.e., Table 1 in [1]). Instead, most of the studies had been conducted in individuals with psychiatric diseases [3 –5], non-AD neurological diseases [6 –11], or other medical disorders [12 –16]. The only exception is two studies limited to healthy women at the time of menopause [17, 18]. Some data can also be extracted from studies with mean age below the age of 60, but including wide age ranges exceeding that age [19 –25]. Hence, data on the role of subjective complaints below the age of 60 in individuals qualifying for SCD are lacking.
Questions to assess subjective cognitive complaints in the GENIC cohort
The questions were referred to approximately the last six months and were coded as 0 (absence of complaint) or 1 (presence of complaint). Answers were summed up and the total of complaints was obtained ranging from 0 (no complaints) to 9 (maximum number of complaints).
Recent research shows that in community-based cohorts, SCD may also be related to cerebrovascular disease [26] and age-related tauopathy [27], besides AD. A common feature of these three processes is brain neurodegeneration, which can be reliably measured in vivo with structural magnetic resonance imaging (sMRI). Previous sMRI studies have shown smaller volume of the hippocampus and medial temporal cortex in SCD individuals [28 –32]. Both are common findings in AD but also in other pathologies affecting the medial temporal lobes [33, 34]. The association between SCD and white matter signal abnormalities (WMSA), a surrogate marker of cerebrovascular disease, has also been reported [35].
Our first aim was to investigate the association of SCD with neuroimaging, cognitive, clinical, and demographic measures on a large cohort of community-dwelling individuals spanning a broad range of age (33 to 86 years). Our second aim was to further investigate these associations separately on individuals <60 years and ≥60 years of age by stratifying the cohort in two age subgroups. Different neuropathological mechanisms were studied throughout sMRI biomarkers of cerebrovascular disease (i.e., WMSA), as well as both regional and diffuse brain neurodegeneration (i.e., hippocampal and global brain atrophy). Since one of the main challenges of current cross-sectional studies in SCD is that the association between complaints and disease profile measures may be masked by premorbid levels and other factors such as depressive symptomatology or aging [36 –39], we applied a novel multivariate approach that investigates all these dimensions simultaneously, minimizing the confounding effect of premorbid levels and other extraneous variables [40].
METHODS
Participants
A total of 416 individuals were selected from the GENIC cohort [41], a community-based study from the Canary Islands (Spain). Inclusion criteria fulfilled the basic SCD criteria from the SCD-I (Table 1 in [1]): 1) Preserved global cognition and activities of daily living, operationalized as a Mini-Mental State Examination (MMSE) [42] score ≥24, a Blessed Rating Dementia Scale (BRDS) [43] score ≤4, and a Functional Activity Questionnaire (FAQ) [44] score ≤5; 2) Normal cognitive performance in comprehensive neuropsychological assessment using pertinent clinical normative data and own sample descriptive values (i.e., individuals did not fulfill cognitive criteria for mild cognitive impairment or dementia); 3) No abnormal findings such as stroke, tumors, hippocampal sclerosis, etc., in MRI, when available, according to an experienced neuroradiologist; (4) No medical history of neurological and psychiatric disorders (including a diagnosis of major depression), systemic diseases or head trauma; and 5) No history of substance abuse. Subjects’ recruitment in the GENIC-database was done through primary care health centers, advertisements in local schools, and relatives and acquaintances of the research staff, covering a representative sample in terms of age, sex, and education. Participation was completely voluntary and all the participants gave written informed consent approved by the local ethics committee.
Cognitive and clinical assessment
A comprehensive neuropsychological protocol was applied covering processing speed, attention, executive functions, premotor functions, memory, visuoconstructive, visuoperceptive, and visuospatial functions, and language functions (Supplementary Table 1). In addition, global cognition was assessed with the MMSE. Functional status was assessed with the FAQ and the BDRS, including three subscales for 1) performance of everyday activities, 2) habits, and 3) personality, interest, and drive. Depressive symptomatology was assessed with the Beck Depression Inventory (BDI, 21-items version) [45], when individuals were younger than 63 years of age, and the Geriatric Depression Scale (GDS, 15-items version) [46], when 63 years or older. This age cut-off is based on recommendations for using the GDS scale in the elderly, defined as 65±2 years (i.e., the lower limit equals 63 years) in the GENIC study [41]. Therefore, this age cut-off is independent of the SCD-I age cut-off for SCD (i.e., 60 years), which is used in the current study for the different age subgroups (<60 years and ≥60 years). The mean (SD) BDI score in the whole cohort was 5.75 (4.61). The mean (SD) GDS score was 2.26 (2.31). Because BDI and GDS satisfy the principle of measure invariance [47], scores from both scales were transformed into z-scores and combined into one variable for statistical analysis (BDI-GDS composite) [48]. The Wechsler Adult Intelligence Scale (WAIS-III) Information subtest [49] was scored and used as an indicator of crystalized intelligence/education as in previous studies [41 , 51]. The level of education attained was also recorded.
Subjective cognitive complaints
Subjective complaints were studied through nine yes/no questions referred to changes in approximately the last six months (Table 1). Answers were coded as 0 (absence of complaint) or 1 (presence of complaint). Answers were summed up and the total of complaints was obtained ranging from 0 to 9. These nine questions cover in a simplified manner the five different cognitive domains included in validated scales such as ECog [52], further extending the domains covered by the only questionnaire validated in Spanish, i.e., SCD-Q [53]. Item-by-item correspondence among these three methods can be seen in Supplementary Table 2. Of note, both ECog and SCD-Q are endorsed by the SCD-I, and ECog is the most commonly used scale among the participating studies of that world-leading initiative [54]. In this study, we use ‘subjective cognitive complaints’ when we refer to this continuous variable or complaints themselves, otherwise the term SCD is used to refer to the clinical diagnosis.
Magnetic resonance imaging
Participants were scanned using a 3.0T GE imaging system (General Electric, Milwaukee, WI, USA), located at the Hospital Universitario de Canarias in Tenerife, Spain. A three-dimensional T1-weighted Fast Spoiled Gradient Echo (FSPGR) sequence was acquired in sagittal plane: repetition time/echo time/inversion time = 8.73/1.74/650 ms, field of view 250×250 mm, matrix 250×250 mm, flip angle 12°, slice thickness = 1 mm, voxel resolution = 1×1×1 mm. Full brain and skull coverage was required for the MRI datasets and detailed quality control was carried out on all MR images according to previously published criteria [55].
The T1-weighted images were processed and analyzed with the FreeSurfer 5.1.0 image analysis suite (http://surfer.nmr.mgh.harvard.edu/) (see Supplementary Table 3 for full details and references) through our database system [56]. The hippocampal volume (left + right) and the estimated total intracranial volume (TIV) were selected for this study. Further, a proxy of global brain atrophy was calculated using the BV/CSF index [57], where BV stands for brain volume (i.e., total grey matter volume + total white matter volume) and CSF stands for the total volume of the cerebrospinal fluid. This index correlates with clinical measures, CSF biomarkers, and cognition, and has been proposed for staging individuals according to the degree of global brain atrophy and for monitoring disease progression [56]. Lower values of the BV/CSF index denote more atrophy. WMSA were segmented on T1-weighted images using the probabilistic procedure implemented in FreeSurfer, subsequently extended to label white matter lesions [58]. This procedure has demonstrated sensitivity in measuring white matter damage both in healthy individuals and in AD patients [59, 60]. These WMSA are correlated with hyperintensity volumes measured on T2/FLAIR, as well as with microstructural white matter changes as measured on diffusion tensor imaging data [60]. Careful visual quality control was performed on the output data obtained from FreeSurfer, and manual edits were applied when needed.
Statistical analysis
A step-wise strategy was followed in this study. Step 1: data dimensionality was reduced by applying orthogonal partial least squares (OPLS) to latent structures on 75 measures (4 demographic, 5 clinical, and 66 cognitive measures) (please see the next paragraph for a detailed explanation of OPLS). Step 2: once the main variables associated with complaints were identified in step 1, multiple linear regression was conducted in order to investigate partial effects and interactions between the selected variables. This allowed further variable reduction for a final regression analysis, which included these and the neuroimaging variables (Step 3).
The multivariate data analysis method OPLS [61] was used to investigate the association between a continuous outcome variable (i.e., subjective cognitive complaints) and numerous predictors (i.e., demographic, clinical, and cognitive measures). OPLS provides the opportunity to analyze many variables simultaneously and observe inherent patterns in the data. Importantly, the method successfully handles issues related to multiple testing and multicollinearity among predictive variables [62]. Briefly, OPLS tries to maximize the covariance between the outcome variable and the predictors. Information related to this association is found in the first component of the model (predictive component). The other orthogonal components in the model, if any, relate to variation in the data not connected to the effect of interest. Each model receives a R2(X), a R2(Y), and a Q2(Y) value, being Y referred to criterion variables and X to predictor variables. R2(X) represents the explained variance between Y and X, for the predicted and the orthogonal components. R2(Y) represents the model goodness of fit and refers to the fraction of the Y variation modeled in the component, using the predicted model. Q2(Y) reflects the predictive power of the model. The significance of a model is based on the Q2(Y) parameter and is reported as acceptable (Q2 > 0.1), good (Q2 > 0.5), and optimal (Q2 > 0.9) [62]. Further, a Q2 > 0.05 value can also be reported as a trend.
Results can be visualized in loadings plots (Fig. 1), where predictors are presented on the x-axis according to the extent to which they predict a given outcome. Values above zero denote a positive association with the outcome (Y), while measures below zero denote a negative association. Covariance between Y and X is plotted on the y-axis. Jack-knifed confidence intervals are showed for every predictor for bias estimation and the standard error. Measures with confidence intervals that include zero have low reliability in the model.

OPLS models loading plots. Predictors are presented on the x-axis according to the extent to which they predict a given outcome. Values above zero denote a positive association with the outcome (Y), while measures below zero denote a negative association. Covariance between Y and X is plotted on the y-axis. Jack-knifed confidence intervals are showed for every predictor for bias estimation and the standard error. Measures with confidence intervals that include zero have low reliability in the model. Panel A represents the loading plot for the demographic and clinical variables. Panel B represents the loading plot for the cognitive variables. Education Level: illiterate (0); acquired reading and/or writing skills (1); primary level (2); secondary level (3); university level (4). MMSE, Mini-Mental State Examination; BDRS, Blessed Dementia Rating Scale; FAQ, Functional Activity Questionnaire; BDI, Beck Depression Inventory; GDS, Geriatric Depression Scale; WAIS, Wechsler Adult Intelligence Scale.
Multiple linear regression (backwards, with the best general lineal model - bestglm - method for variables exit) was used to investigate the partial association of subjective cognitive complaints with demographic, clinical, and cognitive measures. The selection of the predictors for this model was based on the loading plots from the previous OPLS models, and further supported by findings from previous studies [63 –68]. Multiple linear regression (backwards, bestglm) was also used to study the partial association of subjective cognitive complaints with global brain atrophy (i.e., BV/CSF index), hippocampal volume, and WMSA. In these models, the interaction between all pairs of predictors was also tested. ANOVA was used for mean comparison of continuous variables. The Chi-square test was used for categorical variables. A p-value≤0.05 (two-tailed) was considered significant in these analyses.
Model assumptions were checked in all the cases by visual inspection of residuals and data distribution, as well as by inspecting the pertinent statistical parameters. The OPLS models were conducted in SIMCA (Sartorius Stedim Biotech). All other statistical analyses were conducted using the R statistical software (R Foundation for Statistical Computing, Vienna, http://www-R-project.org), including the bestglm package.
RESULTS
The demographic and clinical characteristics of the study sample are shown in (Table 2a). Regarding the subjective cognitive complaints, 193 participants reported no complaints, whereas 223 participants endorsed between 1 and 6 complaints (mean = 0.97; median = 1; SD = 1.19). Less than 2% of the individuals in this cohort had sought for neurological assessment due to SCD.
Demographic and clinical characteristics
1Education Level: illiterate (0); acquired reading and/or writing skills (1); primary level (2); secondary level (3); university level (4). 2BDI and GDS scores were transformed into z scores and combined into one variable. 3Subjective cognitive complaints were studied through nine yes/no questions as explained in the methods and (Table 1). WAIS, Wechsler Adult Intelligence Scale; MMSE, Mini-Mental State Examination; BDRS, Blessed Dementia Rating Scale; FAQ, Functional Activity Questionnaire; BDI, Beck Depression Inventory; GDS, Geriatric Depression Scale.
Multivariate association of subjective cognitive complaints with demographic, clinical, and cognitive measures in the whole sample
OPLS models were conducted to investigate the association between subjective cognitive complaints and numerous demographic, clinical, and cognitive variables. Model 1 included 4 demographic and 6 clinical variables, and model 2 included 65 cognitive variables. Please see Supplementary Table 4 for a complete description of the variables included in these models. The demographic-clinical model was the one achieving the best performance (R2(X) = 0.208; R2(Y) = 0.206; Q2 = 0.169). A higher number of subjective cognitive complaints was associated with increased depressive symptomatology (i.e., BDI-GDS composite and higher scores in BDRS-personality, interest, and drive) (Fig. 1a). Age was the most important demographic variable showing that a higher number of subjective cognitive complaints was associated with older age (Fig. 1a). The cognitive model (R2(X) = 0.344; R2(Y) = 0.082; Q2 = 0.063) achieved low quality, showing a weak association with subjective cognitive complaints. The five most important cognitive variables in this model were Visual Reproduction delayed, Stroop sheet 2, Visual Reproduction immediate, verbal fluency - animals, and Block Design total WAIS-III score (Fig. 1b).
Partial association of subjective cognitive complaints with demographic, clinical, and cognitive measures in the whole sample
A multiple linear regression model was conducted to further understand the interaction between the demographic, clinical, and cognitive measures. Subjective cognitive complaints were the criterion (Y) variable. Based on the OPLS models reported above, age, BDI-GDS composite, BDRS-personality, interest, and drive, Visual Reproduction delayed, Stroop sheet 2, Visual Reproduction immediate, verbal fluency – animals, and WAIS-III Block design were selected as predictors (X). The model was significant (F (3,410) = 33.081; p < 0.001, R2 = 0.189), showing a significant partial association of depressive symptomatology (i.e., BDI-GDS composite) (ß= 0.344; p < 0.001), BDRS-personality, interest, and drive (ß= 0.243; p < 0.001), and age (ß= 0.025; p < 0.001) with subjective cognitive complaints. There were no significant interactions.
Partial association of subjective cognitive complaints with global brain atrophy, hippocampal volume, and WMSA in the whole sample
MRI data were available for 237 participants. The MRI subsample had younger age, higher education level, and higher WAIS-III Information and MMSE scores as compared with the subsample without MRI data (Supplementary Table 5). These findings are due to lack of MRI data in the first wave of assessments where mostly participants of 65 years or older were recruited. The OPLS models 1 and 2 reported above were repeated including only individuals from the MRI subsample. We observed virtually the same results than in the whole sample (Supplementary Table 6).
A multiple linear regression model was conducted to investigate the association of subjective cognitive complaints with the BV/CSF index (estimation of global brain atrophy), hippocampal volume, and WMSA. The TIV, BDI-GDS composite, BDRS-personality, interest, and drive, and age were also included in the model. The model was significant (F (7,228) = 14.159; p < 0.001; R2 = 0.282). The interaction between the BV/CSF index and age (t (235) = –3.457; p < 0.001) revealed that greater global brain atrophy (i.e., lower values in the BV/CSF index) was associated with a higher number of complaints, and this association was stronger the older the age (Fig. 2a). The interaction between WMSA and BDRS-personality, interest, and drive (t (235) = 2.126; p = 0.035) indicated that a higher WMSA load was associated with a higher number of subjective cognitive complaints, and this association was stronger the more changes in BDRS-personality, interest, and drive were reported (Fig. 2b). Further, higher depressive symptomatology was an independent predictor of a higher number of complaints (β= –0.338, p < 0.001).
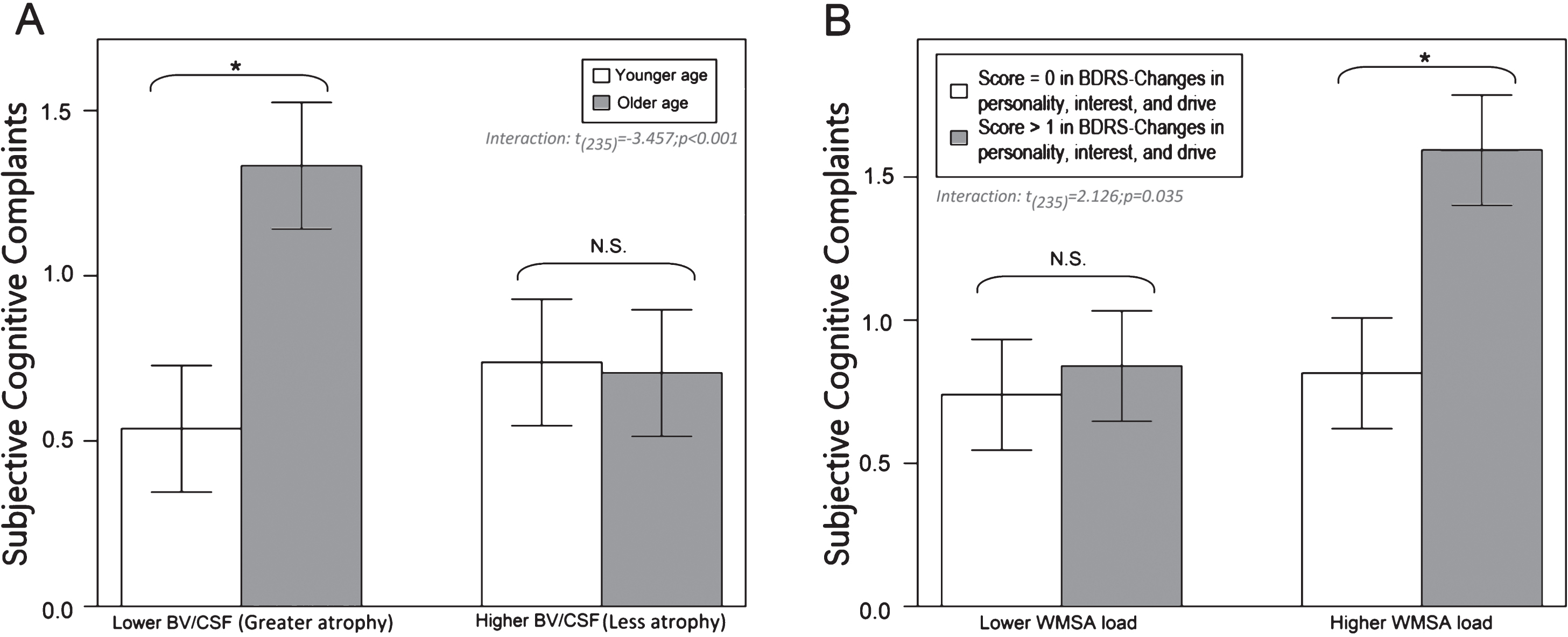
Interactions between neuroimaging, demographic, and clinical variables in the prediction of subjective cognitive complaints in the whole sample. All the variables are continuous in the models but they were dichotomized using the median value for visualization purposes. Bars represent the mean of subjective cognitive complaints and the jack-knifes represent 95% confidence intervals. Panel A represents the interaction between the BV/CSF index (median = 52.34) and age (median = 53). Panel B represents the interaction between WMSA (median = 1639) and BDRS-personality, interest, and drive (median = 0). BV/CSF, brain volume/cerebrospinal fluid; WMSA, white matter signal abnormalities; BDRS, Blessed Dementia Rating Scale. Note: *≤0.05 (two-tailed).
Associations in age subgroups (<60 years and ≥60 years)
Table 2b shows the demographic and clinical characteristics of the two age subgroups (<60 years, n = 209; ≥60 years, n = 207). The <60 years old subgroup endorsed significantly less subjective cognitive complaints, had higher education level, higher WAIS-III information subtest score, higher MMSE score, and lower values on the BDI-GDS composite (Table 2b). The demographic and clinical characteristics of the two age subgroups including only individuals from the MRI subsample are provided in the Supplementary Table 7.
The same OPLS and multiple linear regression models performed for the whole sample were conducted separately in these two age subgroups. Only the model including clinical and demographic measures resulted significant for the two age subgroups. In individuals <60 years (R2(X) = 0.174; R2(Y) = 0.229; Q2 = 0.163), a higher number of subjective cognitive complaints was associated with increased depressive symptomatology (i.e., BDI-GDS composite), higher scores in BDRS-personality, interest, and drive, and lower performance in MMSE. In individuals ≥60 years (R2(X) = 0.171; R2(Y) = 0.260; Q2 = 0.194), a higher number of subjective cognitive complaints was associated with increased depressive symptomatology (i.e., BDI-GDS composite), and higher scores in FAQ and BDRS-performance of everyday activities.
Regarding the neuroimaging measures, the multiple linear regression model for individuals <60 years was significant (F (3,160) = 11.699; p < 0.001; R2 = 0.165). The interaction between the BV/CSF index and the BDI-GDS composite (t (162) = 2.471; p = 0.015) indicated that more depressive symptomatology was associated with a higher number of complaints, and this association was stronger the lesser the global brain atrophy (i.e., higher values in the BV/CSF index) (Fig. 3a). In individuals ≥60 years, the regression model was also significant (F (7,64) = 6.224; p < 0.001; R2 = 0.340). The interactions between the BV/CSF index and BDRS-changes in performance of everyday activities (t (72) = –3.022; p = 0.003), and between the TIV and FAQ (t (72) = –2.615; p = 0.011) indicated that a higher number of complaints was associated with greater global brain atrophy and smaller TIV, and these associations were stronger the more changes in performance of everyday activities were reported (according to both the BDRS and FAQ, respectively) (Fig. 3b, c). Further, higher depressive symptomatology was and independent predictor of a higher number of complaints (β= 0.478, p < 0.001).
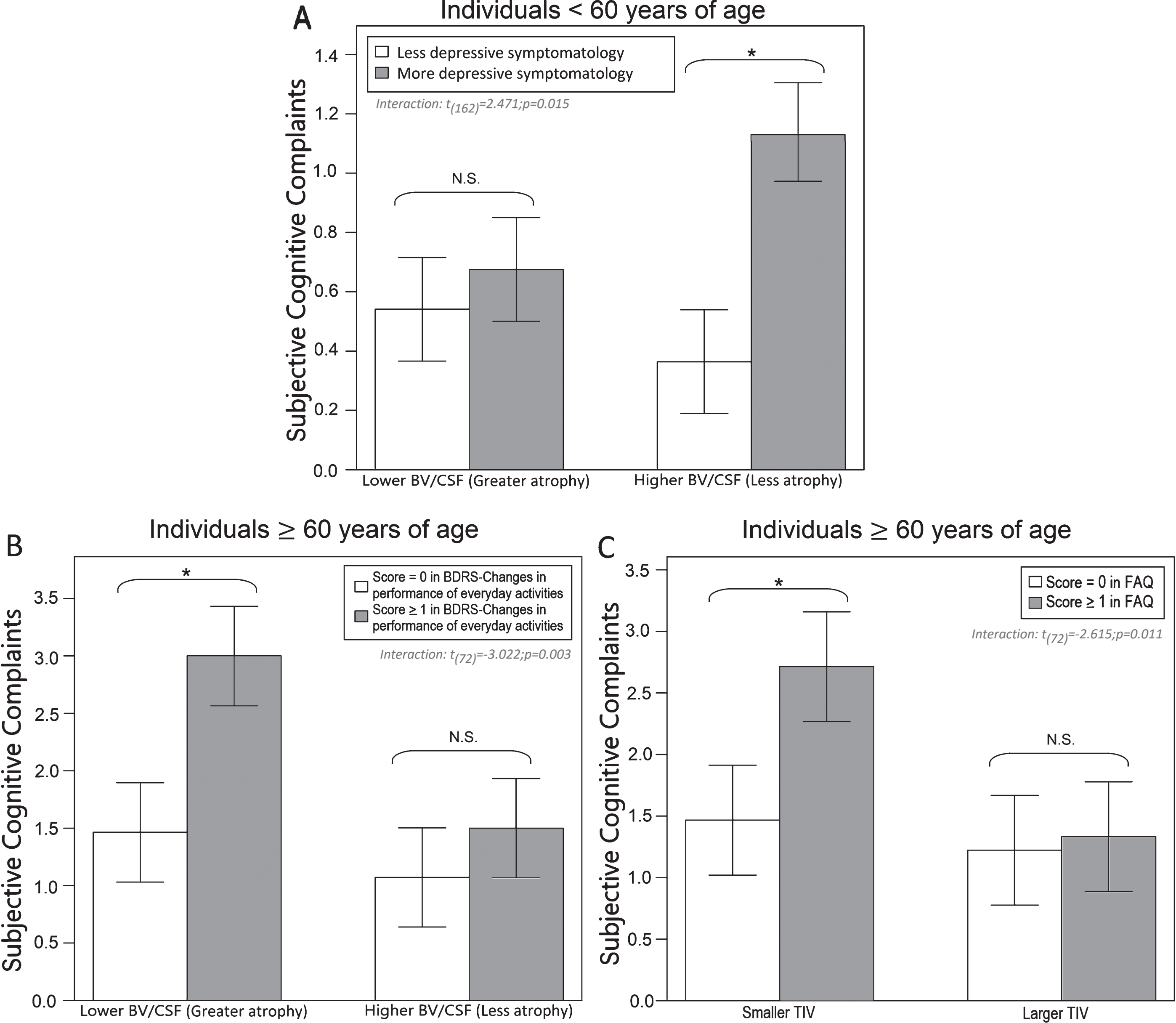
Interactions between neuroimaging and clinical variables in the prediction of subjective cognitive complaints in the age subgroups. All the variables are continuous in the models but they were dichotomized using the median value for visualization purposes. Bars represent the mean of subjective cognitive complaints and the jack-knifes represent 95% confidence intervals. Panel A represents the interaction between the BV/CSF index (median = 60.05) and the BDI-GDS composite (median = 0) in individuals <60 years. Panel B represents the interaction between the BV/CSF index (median = 38.76) and BDRS-changes in performance of everyday activities (median = 0) in individuals ≥60 years. Panel C represents the interaction between TIV (median = 1406854) and FAQ (median = 0) in individuals ≥60 years. BV/CSF, brain volume/cerebrospinal fluid; BDI, Beck Depression Inventory; GDS, Geriatric Depression Scale; TIV, total intracranial volume; FAQ, Functional activity questionnaire. Note: *≤0.05 (two-tailed).
DISCUSSION
To our knowledge, this is the first study investigating the association between subjective cognitive complaints and an extensive number of neuroimaging, demographic, clinical, and cognitive measures, in individuals fulfilling criteria for SCD below the age of 60. Associations were also investigated in individuals above the age of 60 as well as in the whole cohort for results comparison. In the whole cohort, our findings indicate that a higher number of complaints is associated with older age, more depressive symptomatology, and subclinical changes in personality, interest, and drive (BDRS subscale). However, important age-dependent interactions with global brain atrophy and the WMSA load were revealed. Below the age of 60, complaints were associated with lower performance in MMSE, independently of depressive symptomatology and scores in BDRS-personality, interest, and drive. The current study exposes relevant associations, helping to integrate findings from separate previous studies, revealing several novel findings, and showing the potential clinical role of subjective cognitive complaints in individuals from the community who have predominantly not sought for medical help yet (less than 2% of the individuals in this cohort did seek for neurological assessment). Below we elaborate more on these issues.
Depressive symptomatology was the factor achieving the strongest association with subjective cognitive complaints, both in individuals younger and older than 60. Importantly, individuals with mayor depression and/or taking antidepressants were excluded from this study. The association between SCD and depressive symptomatology is a well-established finding in the literature [69 –72]. This finding has led some authors to question the usefulness of SCD as a risk factor for dementia [68 , 74]. However, the real role of depressive symptomatology in SCD individuals is still poorly understood. Clinical depression in itself is a well-known risk factor for dementia [75], especially, AD and vascular dementia [26]. Increasing evidence indicates shared pathophysiological mechanisms in clinical depression and AD. For instance, dysregulation of the hypothalamic–pituitary–adrenal system and neuroinflammation is present in both. Further, an association between the APOE ɛ4 allele and depression in community-based cohorts has been shown [76]. Chronic inflammation accompanying AD pathology may lead to depressive symptoms decades before cognitive decline [77]. Thus, depressive symptomatology in coexistence with SCD in healthy individuals may indeed reflect the presence of a neurodegenerative disease in the preclinical stage. A few studies have reported an association between SCD and amyloid burden after controlling for depressive symptomatology [78, 79]. Furthermore, a recent study demonstrated an association between SCD and increased tau pathology in the entorhinal cortex after adjusting for depressive symptomatology [27]. Altogether, this research and our current data support the idea that both depressive symptomatology and SCD might be coexisting early manifestations of an underlying neurodegenerative disease. The topic thus warrants future investigation, as it has also been recognized in a recent report from the SCD-I [80].
In the current study, age was an important modulator of the association between complaints and different clinical and neuroimaging variables. Although this finding was not unexpected, our current data stand as one of the few reports in individuals below the age of 60 who fulfill the criteria for SCD [1]. We observed that individuals younger than 60 years endorsing complaints evidenced lower MMSE scores. The association of SCD with lower MMSE scores has been referred in previous community-based studies including older age ranges [81, 82]. Since our MMSE result was independent of depressive symptomatology and subclinical changes in personality, interest, and drive, it cannot be excluded that reduced performance in MMSE at the subclinical level is actually related to some neurodegenerative process. We elaborate on this interpretation further down in connection with the imaging findings. Individuals 60 years or older who endorsed complaints evidenced subclinical changes in activities of daily living (both BDRS and FAQ), in addition to more depressive symptomatology. Other authors also reported an association between SCD and poorer performance in activities of daily living [83]. In these interpretations we refer to subclinical changes because SCD was associated with elevated scores in the BDRS and FAQ, as well as reduced scores in the MMSE, but these scores were always within the normal range (i.e., they do not surpass standard thresholds for clinical impairment). However, whether this finding precedes transition to clinical levels in the future can only be ascertained in longitudinal studies.
Capturing an association between SCD and objective cognitive performance in cross-sectional studies is challenging [68]. Some community-based studies have found a significant association [38, 68], but negative results have also been reported [84, 85]. By definition, objective cognitive impairment is excluded from the diagnosis of SCD [1]. However, subclinical cognitive decline is expected, and is thought to be detected by the individuals while remaining elusive to objective cognitive testing [68]. A reason for this is complaints referring to changes in time, whereas cross-sectional cognitive scores mostly represent current performance, likely influenced by premorbid levels [68]. Indeed, longitudinal studies have shown future cognitive decline in individuals with SCD [86]. However, it is also true that previous cross-sectional studies addressing this association frequently included either too rough cognitive measurements, or very few sensitive cognitive variables, normally in small samples, and predominantly looking at memory complaints [54]. A strength and novelty of the current study is that we aimed to capture this association by covering a broad range of cognitive complaints and cognitive measures not restricted to memory, and by applying an advanced multivariate method that may reduce the effect of extraneous variables such as premorbid cognitive levels and other factors [40, 62]. We detected a weak association between complaints and several cognitive measures, of which, the most relevant were visual reproduction, verbal fluency - animals, and the WAIS-III Block design total score. These measures have previously been identified as early markers of cognitive decline [40 , 48], and have been reported in other SCD studies [63 –67].
Findings from neuroimaging studies suggest that brain pathology seems to be captured earlier by subjective cognitive complaints than by routine cognitive testing [87]. We found a strong association of the higher number of complaints with greater global brain atrophy and WMSA load, rather than with specific atrophy in the hippocampus. Further, we detected several interesting interactions. A higher number of complaints was related to greater global brain atrophy, and this association was stronger the older the age. Also, a higher number of complaints was related to a higher WMSA load, and this association was stronger the more subclinical changes on personality, interest, and drive were reported, regardless of their age. Thus, individuals endorsing complaints and showing evidence for either global brain atrophy or WMSA may be on the pathway to a neurodegenerative disease. In individuals younger than 60 years, a higher number of complaints was associated with more depressive symptomatology, and this association was stronger in individuals with less global brain atrophy. Since in individuals younger than 60 years a significant association was observed with reduced MMSE, it is possible that brain changes are present but cannot be detected by the neuroimaging measures used in the current study. Connectivity analyses may be of interest since synaptic dysfunction is suggested to precede overt brain atrophy in the early stages of AD [88]. Hence, future studies should investigate more fine-grained neuroimaging techniques to elucidate whether depressive symptomatology below the age of 60 could be reflecting early changes in brain microstructure or connectivity. Alternatively, SCD below the age of 60 might just be reflecting non-neurodegenerative causes, as suggested by the SCD-I [1]. We hope that our current findings encourage future research on SCD cohorts below the age of 60, so that definitive conclusions can be drawn. In individuals older than 60 years, a higher number of complaints was associated with greater global brain atrophy and smaller TIV, and this association was stronger the more subclinical difficulties in activities of daily living were reported. Therefore, complaints could reflect the subclinical impact of global brain atrophy on activities of daily living, independent of depressive symptomatology, with the affected individuals endorsing 1.5 complaints more on average. It has been suggested that larger TIV might be protective against the onslaught of aging and neuropathological processes [89]. For this reason, TIV is commonly used as a proxy of brain reserve. Our finding suggests that individuals with less brain reserve may be more vulnerable to pathology, reflected by both the complaints and increased subclinical difficulties in activities of daily living. These individuals also endorsed 1.5 complaints more on average.
Some limitations should be mentioned. Our study is cross-sectional and longitudinal analyses are important to demonstrate whether individuals fulfilling SCD criteria below the age of 60 will eventually develop neurodegenerative diseases. We are currently collecting follow-up data. We do not have data on amyloid pathology and the apolipoprotein ɛ4 allele, two factors that have previously shown associations with SCD in the context of AD [68 , 84]. However, we investigated a community-based cohort, where the a-priori prevalence of AD is lower than in clinical cohorts [90]. In contrast, vascular risk factors and age-related tauopathies are more prevalent [27]. Thus, we focused on neurodegeneration and cerebrovascular biomarkers, as well as on factors such as age and depressive symptomatology. Studying other mood factors such as anxiety is warranted.
We conclude that some subtle signs of brain pathology are associated with SCD in individuals below the age of 60. In particular, the WMSA load was associated with complaints and subclinical changes on personality, interest, and drive. Further, lower MMSE performance was also associated with complaints, irrespective of depressive symptomatology. Thus, future studies need to investigate fine-grained neuroimaging techniques to elucidate whether complaints could be reflecting early changes in brain microstructure or connectivity below the age of 60. We acknowledge, however, that depressive symptomatology was an important predictor of complaints in individuals below the age of 60. We discuss that the real role of depressive symptomatology in SCD individuals needs to be elucidated in future research before discarding the validity of a SCD diagnosis below the age of 60. Based on our current findings and other recent research [27 , 79], we propose that depressive symptomatology in healthy individuals may be a symptom of an unspecific neurodegenerative disease, mostly catalyzed by the subjective cognitive complaints. Whether depressive symptomatology is a surrogate marker of an underlying neurodegenerative disease independent of SCD, or it is indeed a consequence of SCD, which in turn emerge as the primary surrogate marker of such disease, remains to be answered. Our findings may have important social and clinical implications for the management of SCD before or as soon as individuals seek for medical help. Screening for people at risk of future cognitive decline should be done in the community for the triad subjective cognitive complaints, depressive symptomatology, and subclinical reduced cognition (<60 years)/activities of daily living (≥60 years). Computed tomography or basic MRI could support this screening in primary care, previous to specialized attention. Our current data also add to the previous literature by providing one of the few reports on a large sample of community-dwelling individuals younger than 60 years of age.
Footnotes
ACKNOWLEDGMENTS
This research has been supported by the Fundaci ó n Canaria Dr. Manuel Morales (convocatoria 2012, 2014 y 2017); Fundaci ó n Cajacanarias; the Swedish Foundation for Strategic Research (SSF), the Strategic Research Programme in Neuroscience at Karolinska Institutet (StratNeuro), the Swedish Research Council (VR), the Åke Wiberg foundation, Hjärnfonden, Alzheimerfonden, Demensfonden Stiftelsen Olle Engkvist Byggmästare, and Birgitta och Sten Westerberg. The funders of the study had no role in the study design nor the collection, analysis, and interpretation of data, writing of the report, or decision to submit the manuscript for publication. The authors would like to thank Dr. Diaz-Flores Varela (Hospital Universitario de Canarias, Tenerife, Spain) for his collaboration in the inspection of magnetic resonance images for inclusion criteria; Dr. Antonio Rodríguez for providing access to participants and helpful assistance; Raquel Rial for English proof reading; the Servicio de Resonancia Magn é tica para Investigaciones Biom é dicas del SEGAI (University of La Laguna, Spain). Data used in preparation of this article is part of the GENIC-database (Group of Neuropsychological Studies of the Canary Islands, University of La Laguna, Spain. Principal investigator: Professor José Barroso. Contact: Dr. Daniel Ferreira, E-mail daniel.ferreira.padilla@ki.se). The following collaborators contributed to the GENIC-database but did not participate in analysis or writing of this report (in alphabetic order by family name): Rut Correia, Aida Figueroa, Nerea Figueroa, Eloy García, Lissett González, Teodoro González, Zaira González, Cathaysa Hernández, Edith Hernández, Nira Jiménez, Judith López, Cándida Lozano, María Antonieta Nieto, María Sabucedo, Elena Sirumal, Marta Suárez, Manuel Urbano, and Pedro Velasco.