
Abstract
Empathy is essential for social interaction and a crucial trait to understand the intentions and behaviors of others and to react accordingly. Alzheimer’s disease (AD) affects both cognitive and emotional processes and can lead to social dysfunction. Empathy results from the interaction of four components: shared neural representation, self-awareness, mental flexibility, and emotion regulation. This review discusses the abilities and deficits of patients with AD from the perspective of subcomponents of empathy and integrates these facets into a model of human empathy. The aim was to investigate the components that are affected by AD and the ways in which patients are still able to empathize with others in their social environment. It concludes that AD patients show a pattern of relatively preserved affective aspects and impairments in cognitive components of empathy and points out specific areas with the need for further research.
INTRODUCTION
Humans are social beings, and our repertoire for understanding others is manifold. For example, we are able to cognitively understand the thoughts, beliefs, and intentions of others, an ability referred to as “mentalizing” or “Theory of Mind” (ToM). The discovery of mirror neurons [1, 2] provided evidence of humans’ ability to understand the motor intentions of others, based on shared neural representations. Additionally, there is an “emotional route” for the understanding of others, called emotional contagion. Cognitive and emotional abilities to share and understand thoughts, beliefs, and intentions of others have often been called cognitive empathy and emotional empathy. Decety and colleagues [3–7] integrated the concept of shared representations with cognitive and affective aspects in a model of human empathy.
Empathy is a crucial ability for comprehending the intentions and behaviors of others and adapting our own behavior to achieve successful interpersonal social functioning [8]. Cognitive and emotional components appear to be closely intertwined to create successful social functioning through our ability to empathize. Hence, investigating empathy in patients who suffer from cognitive and emotional deficits is a promising line of research to shed light on social dysfunction in these patients.
An estimated 46.8 million people worldwide suffer from dementia, and this number is projected to nearly double every 20 years [9]. Alzheimer’s disease (AD) is the leading cause of dementia worldwide. It is characterized as a progressive neurodegenerative disorder, whereby patients are often considered to have primarily cognitive impairments. However, dementia also clearly involves deficits in emotional processing that lead to behavioral dysregulation [10]. Two factors that may decisively affect the treatment of people with dementia (PwD) are changes in social cognitive aspects and emotional processing, and both have great relevance to everyday life and social relationships.
Of the diverse changes that accompany dementia, progressive deficits in social functioning that can cause problems with daily life, social difficulties, and social isolation are likely to be more stressful for patients and their caregivers than cognitive symptoms. Coen et al. [11] emphasized that behavioral and psychological symptoms of dementia (BPSD) are often more demanding for nursing staff and patients’ relatives than cognitive symptoms. BPSD range from aggression, anxiety, and depression to apathy and agitation [12]. In the case of AD, such symptoms as anosognosia and low functionality in daily life can lead to substantial caregiver burden, which is potentially linked to interpersonal stress [13,14, 13,14]. Although the changes may be subtle, there seems to be some preservation of emotional competencies [15] and interpersonal functioning in AD patients compared with other dementias [16, 17].
Initial research focused on cognitive impairments in AD patients, with less attention devoted to emotional deficits and competencies. In recent decades, however, the integration of emotional aspects in studies of AD has increased. Nevertheless, more research is needed in this field to explore emotional processing abilities in AD patients. Empathy plays an important role in successful socioemotional functioning. The present review discusses the extent to which AD leads to difficulties in the ability to empathize. Better insights into the empathic abilities of AD patients could help elucidate social dysfunction and promote interventions that seek to improve the quality of life of AD patients. We review current findings on empathy in AD and integrate these findings with the model of human empathy that was proposed by Decety and colleagues [3–7].
A model of human empathy
The model of empathy that was proposed by Decety and colleagues includes affective bottom-up and cognitive top-down processes that regulate the empathic response. The articles by Decety and colleagues [3–7] provide a detailed overview of the development of empathy and its subcomponents and different and overlapping neural correlates that underlie these components. The present review focuses on components of empathy and the ways in which they are affected by AD.
Decety and Jackson [4] defined empathy according to Ickes [18] as a complex form of psychological inference, in which observation, memory, knowledge, and reasoning are combined to yield insights into the thoughts and feelings of others. Despite the fact that empathy is considered a necessary precursor for prosocial behavior, it also helps us predict the behaviors of others and react accordingly [19].
Evolved biological predispositions build the bases for the development of empathic feelings and behavior through emotional bonds and social interaction [6]. Self-other-awareness and the self-regulation of emotions are important conditions for human empathy. Furthermore, empathy involves the affective experience of the others’ actual or inferred emotional state and understanding their emotional experience. The former is defined as the ability to share the emotional experience of another person and constitutes the affective component of empathy, which does not require conscious awareness. The latter can be viewed as its cognitive component and implies some minimal mentalizing ability and mental flexibility to adopt the subjective viewpoint of the other person [4].
According to Decety and colleagues, there are four macrocomponents of empathy that are underpinned by specific neural systems: shared neural representation, self-awareness, mental flexibility, and emotion regulation. These components are combined to create their model of empathy (Fig. 1), which is composed of three major functional components that dynamically interact to produce the experience of empathy in humans: affective sharing between the self and others (based on shared neural representations), self-other-awareness (self-awareness without confusion between the self and others), and mental flexibility (to adopt the subjective perspective of others and includes also regulation processes). Brain areas associated with affective sharing include the inferior parietal lobule, posterior superior temporal sulcus, anterior insula, premotor cortex, and the anterior cingulate cortex. The temporoparietal junction, temporal pole, posterior cingulate cortex, and medial prefrontal cortex are related to mentalizing [20]. The medial prefrontal cortex has been shown to be also involved in self-other differentiation [21].

Components of empathy according to Decety and colleagues. Left: The four macrocomponents of empathy. Right: The components of empathy in the model of Decety and colleagues. The mechanism of affective sharing is based on shared neural representations. Self-other-awareness is related to the ability to maintain a distinction between the self and others. Mental flexibility refers to perspective taking and regulation processes.
Decety and colleagues emphasized that both affective and cognitive components are crucial for creating the phenomenological experience of empathy through a dynamic interaction. For example, affective sharing without self-other-awareness results in emotional contagion. De Vignemont and Singer [22] also stated that empathy must be distinguished from related concepts, such as mentalizing, emotional contagion, sympathy, and empathic concern. Although the components of the model of empathy interact to create empathy, one must keep in mind that they are still distinct processes.
Alternative models of empathy include the Perception-Action Model (PAM) by Preston and de Waal [23]. At the core of the PAM is a mechanism that leads to a similar emotional state in the empathizer through motor mimicry and emotional contagion [24], but it also addresses more complex forms of empathy like, for example, emotion regulation and experience. Even though the authors acknowledge that mirror neurons cannot produce empathy only by themselves, the PAM emphasizes the role of mirror neurons located in the inferior frontal gyrus and parietal cortices as a neural basis of shared representations of perception and action [23]. The basis of the PAM is in accordance with the perception-action coupling suggested in the model by Decety and colleagues that lead to shared representations.
Another alternative is the self to other model of empathy (SOME) by Bird and Viding [25], which suggests five systems and a self/other switch to create empathy in the observer. It includes two input and appraisal systems that rely on deductive reasoning or associations with relevant stimuli, as well as on person-level cues like tone of voice or facial expression to signal another person’s affective state. This model also includes a mirror-neuron system that can lead to emotional contagion but is, according to the authors, not necessary for empathy to occur. The last two systems are the theory of mind system, which represents the mental state of the self and the other, and a system including the current affective state of the self simulating the other’s emotional state if affective sharing took place. We decided for the model by Decety and colleagues as the basis for investigating empathy in AD because it is a well-established and clearly structured model that allows for the investigation of its sub-components. Furthermore, the models have some overlap, with all of them assuming an affective empathy component as a bottom-up affective sharing mechanism, which keeps the distinction between the self and the other, as well as top-down cognitive control mechanisms like regulation and perspective taking.
SEARCH STRATEGY AND SELECTION CRITERIA
A comprehensive review of the literature was performed using electronic databases (PubMed, Google scholar) for papers published in English including keywords and synonyms associated with “empathy,” “affective sharing,” “contagion,” “self-other-awareness,” “self-other distinction,” “mental flexibility,” “regulation,” “perspective taking,” and “theory of mind (ToM)” paired with the keyword “Alzheimer” and “AD”. We manually searched the reference lists of identified articles for additional papers to supplement the electronic search, which was conducted until September 2018, without restrictions for time. We included reviews and meta-analyses that investigated relevant constructs (empathy and/or subcomponents) in neurodegenerative diseases only if they included AD patients. Studies were included when they compared AD patients to a healthy control group and/or pre-illness state. An exception is the study by Ramanan et al. [26], which does not include a healthy control group, but was considered relevant because of its data-mining and statistical modeling approach.
The section “self-other-awareness” focused on the distinction between the self and the other, but the amount of studies here is scarce. Nevertheless, we also included a few studies on self-awareness in AD. The literature on self-awareness and anosognosia in AD is vast and since this was not a focus of our review, we just intended to give a broad overview over this topic here. Information about authors and article type, as well as descriptions of used methods and relevant results of included studies can be found in the supplementary material (Supplementary Table 1).
EMPATHY IN ALZHEIMER’S DISEASE
Unfortunately, studies that have investigated empathy in dementia, especially AD, are still relatively scarce. Moreover, the majority of studies used the Interpersonal Reactivity Index (IRI), a questionnaire to assess empathy. It consists of four subscales, perspective taking and fantasy to measure cognitive empathy, and empathic concern and personal distress to assess affective empathy. One study was recently conducted by Dermody and colleagues [16]. They investigated cognitive and affective aspects of empathy in dementia patients using caregiver ratings on the IRI. The results showed that AD patients were only impaired in cognitive aspects of empathy compared with healthy age- and education-matched controls, whereas affective components were preserved. These deficits were related to predominantly left-sided temporoparietal atrophy. Statistically controlling for overall cognitive dysfunction ameliorated the empathy-related cognitive deficits in AD patients, and the authors concluded that socioemotional deficits mainly arise because of global cognitive dysfunction rather than a loss of empathy itself in AD patients. These findings are in line with the results from a study by Narme and colleagues [27]. The authors found that the AD group differed from healthy controls only on the perspective taking subscale of the IRI after statistically controlling for age and gender. The study by Rankin and colleagues [28] also supports these results, and furthermore, did not find direct anatomic evidence of empathy loss in AD patients. Synn and colleagues [29] reported lower scores for affective and cognitive empathy in AD patients relative to healthy controls by using caregiver ratings of the empathic concern and perspective taking subscale of the IRI. Moreover, the authors did not find differences to patients with frontotemporal dementia (FTD).
In contrast, Alladi et al. [30] did not find impairments in affective or cognitive aspects of empathy in AD patients, based on caregiver ratings on the IRI comparing scores before and after disease onset. Another study using caregiver informed IRI ratings supports these results by also not finding significant differences on any of the four subscales between AD and healthy controls [31]. Moreover, a study by Hsieh and colleagues [32] did not find significant associations between loss of empathy in AD patients, measured with the IRI, and carer variables like burden and relationship quality. Fernandez-Duque and colleagues used more naturalistic stimuli to examine empathy in dementia [17]. Three people had given an interview about emotionally relevant events in their lives. The participants in the study watched a video of these interviews and were asked to answer questions about the feelings of these three people. AD patients exhibited no impairment in inferring the people’s emotions in the first two videos, which showed clear positive and negative emotions. The emotions that were displayed in the third interview were more ambiguous and variable. The video presented a mother who had more ambiguous feelings about her recent motherhood. In this case, the AD patients’ performance became impaired relative to healthy older adults. The AD patients presented an overoptimistic bias, meaning they endorsed a more positive description of the third interviewee compared with the healthy controls. The authors [17] explained this result from the perspective of a global discrimination hypothesis. They concluded that AD patients might have relied on a global judgment about the interviewee’s overall feelings and situation rather than trying to decode each particular thought or emotion. They also stated that the exact mechanism of this bias was unclear. In accordance with their conclusion, one could infer that these results reflect cognitive impairment in perspective taking or a simpler and less nuanced understanding of more subtle emotional contents (i.e., motherhood in general is considered a happy event).
These studies reported different results with regard to empathy in AD, ranging from no difficulties at all to exclusively cognitive empathy impairments to problems only in inferring more complex and sophisticated emotions. Nevertheless, most studies reported AD patients to be able to experience empathy despite their deficiency in certain cognitive and affective domains. Furthermore, recent reviews also point to a relative preservation of affective empathy and a loss in cognitive empathy, which is related to the overall cognitive decline including ToM and perspective taking abilities [33–35]. The following sections take a closer look at the components of empathy to address the issue of which of them may be more compromised in AD.
Affective sharing
This process is based on the fact that perception and action are functionally intertwined in the human nervous system, and this perception-action coupling leads to shared representations [3–6]. Shared representations between the self and others mean that the perception of a given behavior in others automatically activates the representation of that behavior in the self [23], thus leading to the process of affective sharing.
Before considering affective sharing from the perspective of AD, a fundamental issue is whether AD diminishes such basic skills as facial expression recognition because the most accessible information that specifies an individual’s affective state is information that is conveyed through the face [36]. Klein-Koerkamp and colleagues [37] found in a meta-analysis that AD patients were significantly impaired in their emotion decoding abilities. These difficulties were found in various emotional tasks, for various stimuli, for different types of emotion, and for different degrees of disease severity. After the authors controlled for the cognitive deficits, the patients’ emotional abilities were still worse than those of healthy controls. The authors [37] concluded that the impairments in emotion decoding abilities in AD patients cannot be solely explained by cognitive deficits. McLellan et al. [36] reported similar results in their literature review. However, these authors emphasized that because of the very different results that have been reported in the literature, the issue of whether AD patients are generally impaired in their ability to accurately decode emotional facial expressions remains unresolved. Furthermore, unclear is whether these deficits are caused by a general cognitive decline or verbal or spatial deficits or whether it reflects an impairment in specific emotion-processing mechanisms, although they could not find clear evidence of the latter [36].
Other studies found different results. For example, Bucks and Radford [38] reported a relatively preserved ability to recognize and identify non-verbal affective cues in emotional facial expressions and emotional prosody in AD patients, but they did observe a decline in general cognitive ability. Moreover, the authors could also not confirm differences in the recognition of different emotions (i.e., happiness, sadness, anger, fear, and neutral) among AD patients. Studies by Torres and colleagues [39] and Phillips et al. [40] provided evidence that AD patients present emotion decoding impairments, especially when facial expressions become subtler [40] or when complex emotional situations are involved [39]. Kemp and colleagues [41] suggest that emotion perception deficits in AD could be secondary to their cognitive deficits, rather than a primary impairment in the perception of emotion.
Similar to the aforementioned studies that investigated empathy in AD, a cognitive component seems to contribute to the emotional decoding deficits that are found in some studies. Additionally, two of the aforementioned studies also point to difficulties in the perception of more complex emotions. Although there is no systematic pattern of a deficit with regard to basic emotional processing, current evidence suggests that AD leads to some type of impairment in emotional decoding abilities.
Another important point is the mirror neuron network that plays a key role in affective sharing [4, 25]. Disruptions of the mirror neuron network in the inferior parietal cortex have been associated to prodromal AD [42–44]. A recent study supports this hypothesis and found a gradual posterior-anterior decline of the mirror neuron network related to the AD pathology [45].
Nevertheless, Sturm and colleagues [46] found a linear increase in emotional contagion in mild cognitive impairment (MCI) and AD patients. To our knowledge, this is the only study to date that explicitly investigated emotional contagion in AD. According to these results, AD appears to increase the affective aspect of empathy, meaning that AD patients may be more sensitive to affective sharing than healthy controls. This result needs to be confirmed in future studies. Moreover, the authors used caregivers’ ratings on the IRI as a measure of emotional contagion instead of using a naturalistic experimental setting. Nonetheless, they confirmed their results on the neuronal level. Using structural magnetic resonance imaging (voxel-based morphometry), they found an association between the degradation of temporal lobe structures (i.e., smaller volume in the right inferior, middle, and superior temporal gyri, right temporal pole, anterior hippocampus, parahippocampal gyrus, and left middle temporal gyrus) and an upregulation of emotional contagion. These temporal lobe structures play an important role in affective signal detection and emotion inhibition. One explanation could be that less efficient emotion inhibition leads to a change in interpersonal emotional reactivity and thus to a dysregulation of emotional contagion in the sense of an intensification of automatic affective sharing [46].
This greater ability for affective sharing can be viewed as an advantage that perhaps partly compensates for cognitive deficits in AD with regard to empathy. In contrast, the disinhibition of emotional contagion may make AD patients more vulnerable to negative emotions that are expressed by people in their social environment, which could lead to greater anxiety [46].
Shared representations between the self and others provide a neurophysiological basis for social cognition through the automatic activation of motor representations or emotions [4]. According to the model of human empathy, the mechanism of affective sharing is necessary but not sufficient for empathic understanding. Two other important aspects are self-other-awareness and mental flexibility, which are discussed in the following sections.
Self-other-awareness
Knowledge of the mental states of others is based on knowledge of the self. A reasonable assumption is that other-awareness implies consideration of the perspective of another person. However, self-awareness (i.e., to see the self as an object of knowledge) also requires a capacity for secondary representation [4]. Although some conditions can lead to impairments in the sense of self, such as somatoparaphrenia and psychosis, we usually do not confuse the self and others. To maintain a distinction between these two and to determine the source of feelings, empathy is crucial [3–7].
Unfortunately, studies that investigate self-other-awareness and the distinction between self and other in AD patients are scarce. Studies in the field of self-awareness indicate a decline in AD patients with regard to the self-appraisal of cognitive, behavioral, and physical traits [47], memories of words that were previously recorded in the patient’s own voice [48], ratings of the patient’s own task performance [49], and cognitive and emotional functioning [50] among others. Shany-Ur and colleagues [50] state that self-awareness involves modality-independent as well as modality-specific anatomical regions. The authors found that overestimation of functioning in PwD is related to atrophy in dorsal frontal, orbitofrontal and subcortical regions, like the anterior insula, thalamus, putamen and caudate.
Moreover, Mograbi et al. [51] found that between 63% and 81% of PwD, including AD patients, suffer from self-awareness impairments, especially regarding their own cognitive abilities.
In contrast, the results of other-awareness in AD are more ambiguous. A study by Zamboni and colleagues [47] did not find significant discrepancies between AD patients’ ratings of cognitive, behavioral, and physical traits of another person and the other persons’ ratings himself, while being less able to rate themselves on a list of traits. These higher discrepancies for questions regarding themselves were related to decreased activation in medial prefrontal and anterior temporal regions, whereas there were no differences in MCI or control groups for neither self- nor other-condition.
Furthermore, Bond et al. [48] found that AD patients’ memories of words that were presented in the voices of others were less consistently affected than when it was the patient’s own voice. By contrast, Mograbi and colleagues [52] found that AD patients differed from healthy older adults in terms of ratings of the performance of an imagined other. Patients suggested that others of similar age would do as well as they themselves would do in memory and reaction time tasks, despite their cognitive impairments. This is consistent with their lack of self-performance awareness, but it also demonstrates their difficulties in assuming the perspective of others. A study by Ruby et al. [53] investigated AD patients’ awareness of personality traits of the self and another person from both first- and third-person perspectives. The results indicated a decline of accuracy in self-awareness in AD patients and impairments in the judgment of personality traits of another person. The authors concluded that to appropriately attribute social emotions (e.g., selfishness, boringness, and politeness) to oneself or another person, a third-person perspective is needed, which is perhaps a notable impairment in AD patients. During the self-personality assessment, AD patients showed stronger recruitment of the intraparietal sulcus than control participants. When assessing their personality from a third-person view, the posterior dorsomedial prefrontal and orbitofrontal cortex were more activated than in elderly controls, but similar to young controls. While the authors interpret the first result as a familiarity-based reliance on non-updated personal semantic information to assess the self, they suggest that AD patients, due to their memory deficits, rely more on inferring and monitoring when evaluating the self from a third-person perspective [53].
Self-awareness in AD is likely affected by cognitive impairments, more specifically episodic memory impairments that lead to difficulties in updating representations of the self [54]. Such episodic memory impairments are referred to as mnemonic anosognosia [55]. It has also been suggested anosognosia may be executive in nature, with difficulties in error monitoring and metacognition that underpin unawareness of the disease. The neural networks that mediate executive functions show some overlap with those that support perspective taking [56–58], so neurodegeneration at these sites may lead to both self- and other-unawareness. Moreover, it has been shown that the medial prefrontal cortex, that is involved in differentiating between the self and others, is impaired in AD patients [59–61]. Nevertheless, AD patients more accurately identify dementia in others than in themselves [62]. This was investigated using a vignette method, whereby PwD could frequently correctly identify the problems of the depicted persons with dementia or healthy aging, although they scored lower than controls. Evidence of greater awareness of others in unaware patients has also been suggested in other conditions [63]. Considering these studies, Morris and Mograbi [55] proposed a revised cognitive awareness model (CAM), in which different modules store self and non-self information, thus including the possibility of impairments in self-awareness with preserved other-awareness.
Self-other-awareness develops in early childhood [64], based on knowledge about the self and dynamic interrelations with others [4]. A reasonable assumption is that AD patients are able to maintain the distinction between the self and others. Bond et al. [48] reported that AD patients could successfully attribute tactile events to the self versus external agents, indicating that AD patients retain intact tactile body schema processing and are able to distinguish between the self and others. This may suggest that problems in self-awareness in AD are more pronounced for knowledge about the “AD-self” rather than reflecting a general disability of self-other-awareness.
Mental flexibility and self-regulation
As mentioned above, empathy can be felt in a variety of situations which requires us to adopt more or less consciously the subjective perspective of another person, which is also called mentalizing or ToM [19]. For this purpose, some form of active inhibitory mechanism is necessary to regulate the own perspective to allow cognitive and affective flexibility in evaluating the perspective of another person. Moreover, top-down information processing and control, such as self-regulation, are also needed to modulate one’s own emotions in order to not be overwhelmed by them and to not experience them as aversive [3, 4, 6]. Thus, appropriate emotion regulation strategies play an important role in managing and optimizing intersubjective transactions between the self and others; in doing so, such strategies allow for empathic experiences [4].
Goodkind and colleagues [65] examined instructed and spontaneous emotion regulation in dementia patients and age-matched healthy controls. They presented an aversive acoustic startle stimulus to the participants under three conditions: 1) unwarned without instructions to downregulate their emotions, 2) warned without instructions to downregulate, and 3) warned with instructions to downregulate. The investigators measured overall somatic activity and emotional facial expressions. The downregulation of emotions in terms of somatic activity did not differ between groups. With regard to emotional facial expressions as a marker of downregulation, AD patients only presented moderate impairment in the “warned with instruction” condition, in which they were less able to downregulate their emotions compared with controls. The authors concluded that this deficit in AD was caused by greater cognitive demands (e.g., remembering a countdown until the startle stimulus appeared, tracking its progress, and remembering the instructions) that were inherent to the instructed downregulation. However, because of their relatively good performance in the “warned without instruction” condition, the authors conclude that AD patients were able to naturally downregulate their emotional response to an aversive stimulus. Thus, AD patients appear to be able to regulate their emotions successfully in situations that do not overtax memory and other cognitive resources [65]. Another group of dementia patients that was investigated suffered from frontotemporal lobar degeneration (FTLD). In contrast to AD patients, this group was unable to spontaneously downregulate their emotions. The authors concluded that this pattern is consistent with the lack of social concern and social inappropriateness, which are important symptoms of FTLD [66].
In AD patients, Nash et al. [67] did not find differences in perceived emotion regulation capacity that was measured by the Difficulties in Emotion Regulation Scale and affective empathy that was measured with the IRI between AD patients and controls. However, AD patients had more inhibitory failures in the Hayling Sentence Completion Test and lower self-reported cognitive empathy. Nevertheless, refuting their hypothesis, the authors did not find a relationship between emotion regulation and inhibitory control or between cognitive empathy and inhibitory control. With regard to the reported cognitive empathy deficits, the authors speculated about the existence of a different underlying mechanism apart from cognitive disinhibition that contributes to these deficits in AD. Concerning the lack of a hypothesized relationship between emotion regulation and cognitive inhibition, the results of a study by Henry and colleagues [68] are also somewhat surprising. AD patients and controls watched amusement film clips coupled with three different instructions (i.e., spontaneous expression, suppression, or amplification of emotion). The results indicated that the intentional use of suppression was intact in AD patients, whereas both groups had difficulties with the amplification of emotions. Their results are also in agreement with Nash et al. [67], who did not find a relationship between cognitive disinhibition and emotion regulation in AD. Hence, neither of these studies related cognitive disinhibition in AD patients to emotion regulation deficits. Although deficits in cognitive inhibitory control are prominent features in AD, Amieva et al. [69] concluded that this is not a consequence of the breakdown of general inhibitory processes, and an inhibitory mechanism may indeed be preserved in AD. Thus, AD appears to have a strong impact on tasks that require controlled inhibition but a considerably smaller impact on tasks that require more automatic inhibition [68]. Moreover, Henry et al. [68] discussed their results from the perspective of models of aging that consider that some emotion control processes are relatively more automatic in older age. They suggested that emotion regulation strategies, such as the effective behavioral suppression of emotions, may depend on well-practiced, automatic processes by the time one reaches older adulthood. This is consistent with a range of studies that reported that emotional experiences change with age [70–73]. Leclerc and Kensinger [74] found that older adults exhibited greater activity in areas that are associated with emotion regulation, namely the prefrontal cortex, compared with younger adults, and less activity in the amygdala, an area that is responsible for processing emotionally arousing stimuli, when viewing negative images compared with neutral images.
Additional evidence that AD patients possess relatively intact emotional regulation abilities, at least for some of its forms despite their cognitive deficits (e.g., disinhibition), derives from the phenomenon of habitual emotion regulation. Gyurak and colleagues [75] reasoned that the frequent use of a given explicit strategy can quickly render the initiation of the strategy more implicit during regulation, thus making it more implicit over time. Hence, a reasonable speculation is that AD patients are able to conduct at least more automatic, spontaneous emotion regulation processes successfully.
The last component of empathy that is considered here is the ability of adopting the perspective of another person. The number of studies investigating cognitive ToM, measured for example using first and second order false belief tasks, and affective ToM, which can be assessed using the Faux-Pas or the Reading the Mind in the Eyes Test, in PwD increased in the last decade. Using different perspective taking tasks, Marková et al. [76] reported diminished overhead and first-person view perspective taking abilities in AD patients, while people with MCI were only impaired in the first-person view task. Studies showed that AD patients perform relatively normal in first order false belief tasks [77–82], and are impaired in higher order false belief tasks [77, 80–83], which could be secondary to their cognitive impairments (especially executive functions) [41, 85] or episodic memory deficits [29] rather than reflecting a primary impairment in ToM. Moreover, Fliss et al. [84] found that, while patients in moderate stages of the disease were impaired in first and second order false belief tasks, patients in early phases showed only deficits in second order false belief tasks. This suggests a decrease of ToM abilities with the progression of the disease [84, 86].
A data mining study by Ramanan and colleagues [26] also found that difficulties of AD patients in cognitive ToM tasks do indeed not reflect a genuine ToM deficit, but are rather mediated by a particularly executive cognitive decline. This is consistent with the results of a systematic review by Sandoz et al. [87] and a meta-analysis by Bora and colleagues [88]. Bora et al. [88] found that AD patients’ ToM deficits are only modest relative to their general cognitive dysfunction and compared with patients with FTD. Furthermore, the authors found that a longer disease duration and the degree of general cognitive deterioration lead to more severe ToM deficits in both types of dementia. Sandoz and colleagues [87] stated that the deficits in ToM task performance that are caused by AD are mainly attributable to a decline in cognitive and executive abilities and do not reflect a specific ToM impairment. Other studies interpreted their results as a genuine ToM impairment in AD patients [83, 89], whereas Laisley and colleagues [86] found that impairments in working memory and executive functions were associated only to more complex cognitive ToM abilities. The different results are maybe due to the inclusion of AD patients at different stages of disease severity [86, 90]. Concerning affective ToM, although not central to this article but reported for completeness, the results are more ambiguous. Some studies did not find an impairment in affective ToM [77, 84], while others did [79, 86]. Fliss et al. [84] suggested that affective ToM abilities could be affected by decreasing decoding abilities of facial emotions.
The ToM network includes at least the posterior superior temporal sulci, the adjacent temporoparietal junction, the precuneus, and the medial prefrontal cortex [41, 85]. According to Fortier et al. [90], a deficit in the temporoparietal junction, which is frequently reported in AD patients [91], may be central to understanding ToM impairments in this patient population. Le Bouc and colleagues [92] reported a correlation between the severity of the deficit in inferring someone else’s beliefs and a hypometabolism in the left temporoparietal junction. This kind of deficit was predominant in the AD group. The FTD, group on the other hand, was particularly impaired in inhibiting their own mental perspective, which was associated with hypometabolism in the right lateral prefrontal cortex.
In summary, emotion regulation and perspective taking abilities appear to be relatively preserved in early stages of the disease, as long as the situation does not overwhelm the cognitive capacities of patients. Most studies show a decline in perspective taking abilities with decreasing cognitive abilities and thus, with the progression of the disease. Moreover, emotion regulation and perspective taking to some extent involve inhibitory mechanisms. At least concerning emotion regulation, AD patients may rely more on automatic inhibitory mechanisms than on controlled ones, which may help them satisfactorily cope with task demands.
LIMITATIONS AND FUTURE DIRECTIONS
The conclusions drawn from this review must be considered keeping some limitations in mind. The number of studies investigating empathy and its subcomponents in AD is still relatively small, especially regarding emotional contagion and self-other distinction. Moreover, most studies used small samples and different methods, as well as included patients in different stages of the disease. Therefore, it is not surprising that sometimes results differ or are even controversial. On top of that, a lack of experimental and more naturalistic studies raises questions about the ecological validity of results and their generalization into daily life. Furthermore, the subcomponents themselves are complex psychological processes, each underpinned by its own neural network. Thus, it represents a huge challenge to summarize them in a single model. Here, we just tried to give an overview about how these processes could be affected by the disease and how that diminishes the empathic abilities of AD patients. To the best of our knowledge, this is the first review exploring empathic abilities and its subcomponents in depth in AD. Exploration and investigation of emotional abilities in AD has just begun and with more research being done in the field, the present conclusions can be modified and extended.
Nevertheless, we believe that some conclusions can be drawn from the presented studies. Figure 2 shows a revised version of the model of human empathy for AD, depicting the influence of cognitive changes on components of the model. The effect of general cognitive impairments on emotion regulation abilities can be viewed in accordance with Henry et al. [68]. AD patients are able to conduct more automatic, spontaneous emotion regulation and present difficulties in tasks that require the controlled inhibition of emotional responses. With regard to their ToM abilities, evidence indicates that AD patients have more pronounced deficits in more complex tasks, which can be attributed to a decline in cognitive and executive abilities [87]. Memory deficits may also influence performance in ToM tasks [29], in which AD patients may be unable to keep all details in mind that are required to infer the beliefs of others [82].
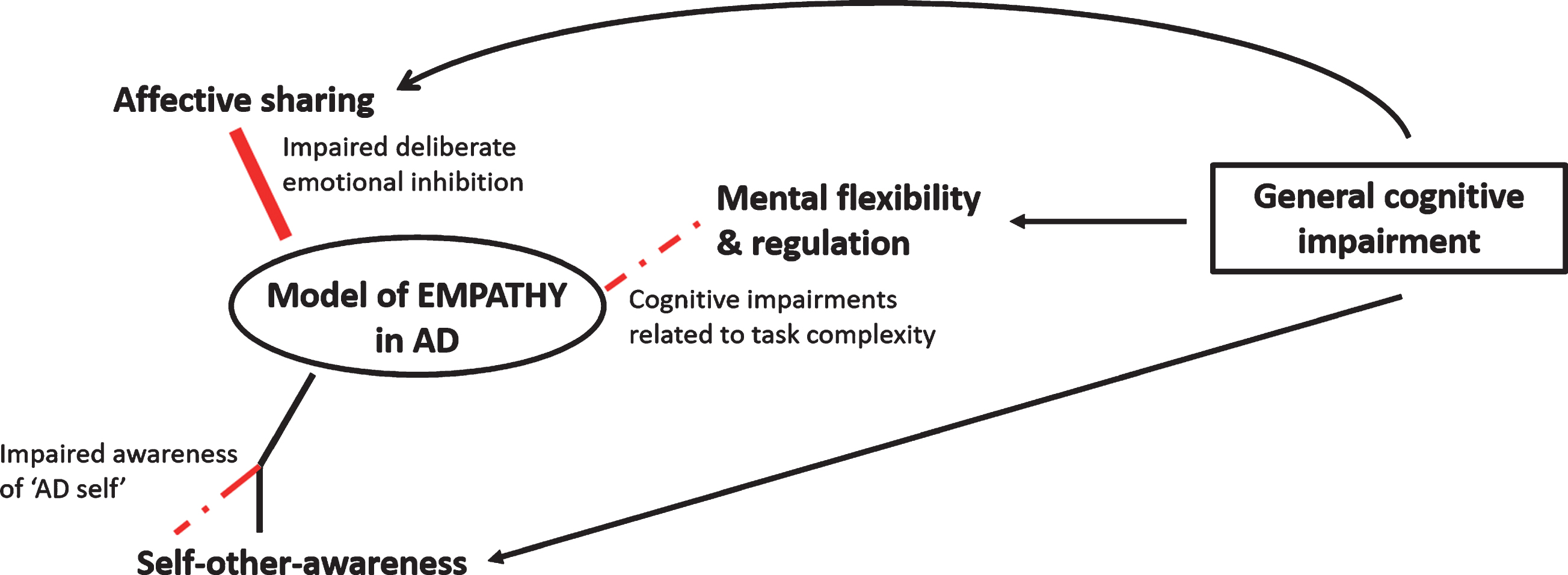
A draft of the empathy model in AD. The figure highlights the processes that are most likely affected by the AD pathology. Deficits in empathy can mainly be attributed to their general cognitive impairment, particularly in executive functioning and memory. AD patients appear to be able to regulate their emotions and conduct ToM tasks to a certain degree, at least in earlier stages of the disease. But they can present difficulties when task demands become more complex. Thus, mental flexibility and regulation, which comprise the cognitive aspect of empathy, are somewhat impaired in AD (indicated by the dashed line). Moreover, general cognitive impairments also influence the affective aspect of empathy. Less emotion inhibition could lead to greater emotional contagion and thus lead to the intensification of automatic affect sharing (indicated by the thicker line). Furthermore, cognitive impairment leads to problems of awareness that are related to the “AD-self,” whereas other awareness appears to remain mostly intact. However, there is no evidence of confusion of the self and others in AD. In contrast to AD, patients with FTD seem to present a primary impairment in empathy related abilities. Thus, their deficits cannot be mainly explained by other cognitive impairments.
More research is needed on the influence of different aspects of cognitive impairment on the different components of the model of empathy. Unclear are the effects of controlled cognitive inhibition versus automatic cognitive inhibition on emotion regulation abilities in AD patients and the influence of memory and executive function deficits on self-other-awareness. Although some studies have investigated self-awareness and other-awareness in AD, a dearth of studies have explored the borders between self- and other-awareness in AD patients (e.g., tracking the origin of feelings [self versus other]). In the context of empathy, unknown is whether the deficits of AD patients in more complex emotional situations are caused by impairments in perspective taking or whether such difficulties reflect a deficit in emotional abilities.
The combination of preserved skills and deficits in AD patients with regard to empathy is in accordance with Decety and Jackson [4], who did not assume a single source of empathy deficit in different conditions because of its multidimensional nature. The ability to experience empathy depends on various processes. Some components may compensate for other components, and the overall ability to empathize may be viewed as a continuum. Interactions with the social environment are essential for human beings. Declines in social relationships and interactions, combined with social isolation, substantially affect AD patients’ quality of life. Even if AD patients exhibit impairments in cognitive abilities to share and understand the thoughts, beliefs, and intentions of others, they may be able to utilize more emotional processes to fulfill these tasks. Furthermore, preserved competencies in the emotional domain can be used as a resource in AD patients [15]. A deeper understanding of emotional processing in PwD could lead to the greater participation of these patients in social life, thus improving the quality of life of both patients and their caregivers. A future goal is to incorporate current knowledge about AD in the domain of empathy and social functioning and thus promote further research in this field. By extending our understanding of the ways in which AD affects emotional abilities, we may be able to adapt clinical and home care to the individual needs of patients and caregivers.
CONCLUSION
The goal of this review was to explore empathy in AD and investigate the subcomponents of empathy that are affected by the disease according to the model of human empathy. Emotional processing/decoding, affective sharing, self-other-awareness, mental flexibility, and self-regulation abilities in AD patients were briefly reviewed. Although the performance of AD patients differed from healthy controls in all aspects that were reviewed herein, AD patients were still able to perform basic emotional processes that contribute to empathy, whereby their difficulties can largely be attributed to their cognitive impairments. Furthermore, AD patients do not exhibit impairments in all domains of cognitive processes that are related to empathy. Emotion self-regulation and perspective taking are partly based on the ability of cognitive inhibition to regulate one’s own emotions or perspective. Both aspects have been shown to be preserved to a certain degree in AD patients, and they may rely more on automatic inhibitory mechanisms that are considered to be less affected by the disease [68, 69].
By contrast, the majority of studies reviewed here, reported intact affective empathy in AD [16, 35]. Furthermore, AD patients seem to have a greater ability of affective sharing, reflected by greater emotional contagion [46]. Shared representations between the self and others are at the core of the proposed model of human empathy and provide a neurophysiological basis for social cognition. Although this enhanced ability could make AD patients more prone to negative emotions that are expressed by other people in their social environment, it may also be used to compensate for cognitive deficits in AD with regard to empathy. The pattern of relatively preserved aspects of affective empathy and impairments in components of cognitive empathy in AD also indicates the importance and intertwined nature of interactions between cognition and emotion in producing a holistic experience and the ability of socioemotional functioning.