
Abstract
Background:
The prevalence of cognitive impairment in hemodialysis patients is notably high. In previous studises performed in the general population, cognitive impairment has been associated with increased mortality.
Objective:
We evaluated the relationship between global cognitive function tested by a short screening instrument and mortality in hemodialysis patients.
Methods:
Cognitive testing was performed in 242 maintenance hemodialysis patients under standardized conditions at baseline using the Montreal Cognitive Assessment (MoCA).
Cognitive impairment was defined as a MoCA test score ≤24 points, as published previously. All-cause mortality was monitored during a median follow-up of 3.54 years. Kaplan-Meier plot and Cox regression model adjusted for known risk factors for mortality in hemodialysis patients were used to examine a possible association between global cognitive function and all-cause mortality.
Results:
A MoCA test score ≤24 points resulted in a significant almost 3-fold higher hazard for all-cause mortality (unadjusted hazard ratio [HR]: 2.812; 95% confidence interval [95% CI]: 1.683–4.698; p < 0.001). After adjustment, this association was attenuated but remained significant (adjusted HR: 1.749; 95% CI: 1.007–3.038; p = 0.047).
Conclusion:
Impairment of global cognitive function measured by a short screening instrument was identified for the first time as an independent predictor of all-cause mortality in hemodialysis patients. Thus, implementing the MoCA test in clinical routine could contribute to a better risk stratification of this patient population.
INTRODUCTION
Cognitive impairment and dementia have a markedly elevated prevalence in hemodialysis patients compared to the general population [1–3]. The underlying pathogenesis is not fully understood so far, but given the high cardiovascular burden of this patient population, cerebrovascular disease most probably plays an important role. This is also supported by the observation that executive functions are impaired early in the course of dementia in hemodialysis patients [4] similar to patients with vascular dementia, where certain brain areas related to executive functions are most often affected [5].
Cognitive impairment is associated with compliance problems with respect to feeding habits, fluid restriction, and especially medication [6]. The socioeconomic aspect of increasing health care costs has to be taken into account as well [7]. Cognitive impairment and dementia were proven to lead to disability, hospitalization, dialysis withdrawal, and death [8–10]. Concerning mortality, the cited studies focused on patients with pre-diagnosed dementia and thus probably advanced stages of the disease. Only two studies investigating survival in hemodialysis patients performed cognitive testing: Griva et al. [11] and Drew et al. [12] were able to demonstrate an independent association between cognitive impairment and mortality in hemodialysis patients, but both studies did not apply an established short screening instrument or neuropsychological test battery to allow a reliable statement on global cognition.
Therefore, the main aim of our study was to evaluate a relationship between global cognitive function tested by a short screening instrument and all-cause mortality in a cohort of hemodialysis patients.
METHODS AND MATERIALS
Standard protocol approvals, registrations, and patient consents
All participants provided written informed consent. The study protocol was approved by the Ethics Committee of the Faculty of Medicine of the Technical University Munich and by the Ethics Committee of the Bavarian State Board of Physicians. This study is part of the Risk Stratification in End-stage Renal Disease (ISAR)-study of which the detailed study protocol was published recently [13]. The study is registered on ClinicalTrials.gov (registry number NCT01152892).
Study subjects
Patients were enrolled from nine hemodialysis centers in Munich and the greater Munich area from June 2011 until July 2013. Inclusion criteria were age over 18 years and being on maintenance hemodialysis for at least 90 days. Exclusion criteria were ongoing infection, pregnancy, malignancy with a life expectation of less than 24 months and incapacity to provide informed consent. In addition, non-native German speakers as well as patients with a motor disorder of the dominant hand or with a history of amaurosis or aphasia were excluded to prevent interference with cognitive testing.
As the assessment of cognitive function was performed as a sub study within the ISAR-study, cognitive testing was not conducted in every participating dialysis center and patients were allowed to choose whether they wanted to undergo cognitive testing. A flow diagram of the patient recruitment process is depicted in (Fig. 1).

Flow diagram of patient recruitment process. n, number; MoCA, Montreal Cognitive Assessment.
Cognitive testing
The cognitive testing instrument applied was the Montreal Cognitive Assessment (MoCA), a short screening test evaluating various subcategories/domains (visuospatial and executive function, naming, attention, language and verbal fluency, abstraction, recall, memory function and orientation) [14]. To determine cognitive impairment, a cut-off value of ≤24 points was used, as this cut-off score has been previously identified by two independent studies to be more sensitive and specific in hemodialysis patients [15, 16]. To warrant reliable results, testing was conducted in a standardized manner prior to a midweek dialysis session in a separate room [17]. All raters (medical doctors or doctoral candidates) were intensively trained by the same professional prior to performing patient assessments.
Clinical and demographic data
Patients’ demographic and clinical data were gathered from dialysis protocols and medical charts at the time of inclusion. For laboratory parameters, blood samples were obtained prior to a midweek dialysis session at the time of study inclusion and were analyzed by ISO (International Organization for Standardization) certified laboratories. Mortality was obtained until September 2016 by medical reports, databases of each dialysis center or by contacting the attending physician or next of kin. Cause of death was defined in accordance with the ISAR Endpoint Committee [13]. The presence of cardiovascular disease was defined as a composite of either peripheral artery occlusive disease and/or coronary artery disease; arterial hypertension was defined by the regular use of antihypertensive medication and hypercholesterolemia by a total cholesterol level >200 mg/dl and/or the regular use of statins. Nicotine abuse was defined by the regular use of tobacco products or cessation of smoking within 5 years prior to study enrollment. Blood pressure was measured shortly before the initiation of a midweek hemodialysis session at the time of inclusion. Patients who received a kidney transplant (n = 20) or who were lost to follow-up (n = 4) were monitored until the last known regular hemodialysis session and were considered censored afterwards.
Statistical analysis
Being part of the ISAR-study, the hypotheses of this sub study were pre-specified and published in the study protocol in BMC Nephrology [13]. Statistical analysis was performed using IBM SPSS Statistics version 22. Median follow up period was calculated from study enrollment until death, last follow up, day of kidney transplantation or in case of lost to follow up, last recorded dialysis session. MoCA raw values, which were not corrected for educational level, were used for all statistical analyses since we believe that an extra point is not sufficient to adjust for lower educational level as it is proposed by the MoCA test [14].
This approach was also pursued in our previous publications, where we adjusted for educational level as an additional variable in statistical analyses [16, 18].
The study population was divided into two groups on the basis of their MoCA raw score, where a test result of ≤24 points indicated cognitive impairment and >24 points indicated normal cognitive function. A Kaplan Meier plot for time to death was computed, the log-rank test was performed to test for a difference in survival between groups.
The hazard ratio of cognitive impairment (based in MoCA raw score ≤24 points) on mortality was calculated in a univariate Cox regression analysis and in a multivariate Cox regression analysis to adjust for other risk factors for mortality. Based on known risk factors for mortality in hemodialysis patients, the following variables were considered for adjustment in the multivariable Cox model: age, BMI, arterial hypertension, diabetes, nicotine abuse, cardiovascular disease, dialysis vintage (defined as cumulative time on regular maintenance hemodialysis in months), time per dialysis session (in hours), Kt/V, etiology of ESRD, albumin, CRP, hemoglobin, calcium, phosphate, and PTH [19–26]. As the number of predictors that can be included in the multivariate Cox regression model is limited by the number of events [27, 28], 7 to 10 predictor variables could be included in the multivariate Cox regression model, given the number of 69 events in this study cohort [13]. To determine the variables with significant effect on survival in our cohort, consecutive univariate Cox regression analyses (Supplementary Table 1) were calculated for the above-mentioned variables. In addition to cognitive impairment, seven variables (age, diabetes, cardiovascular disease, dialysis vintage, time per dialysis session, albumin, and peripheral systolic blood pressure) were significantly associated with mortality and were subsequently entered in the multivariate Cox regression analysis of the effect of cognitive impairment on mortality. Data are shown as median (interquartile range) for continuous variables and quantity (% of total) for categorical variables. For all statistical tests, a significance level of 0.05 was used.
RESULTS
Patients’ characteristics and cognitive function at baseline
A total of 242 patients with a median age of 69.0 years were included, 71.5% of them were male. The median dialysis vintage of the cohort was 41.1 months with a median duration of 4.33 hours per dialysis session. Further baseline characteristics are provided in Table 1.
Baseline characteristics of the cohort
*There were missing values for the variables HsCRP (n = 6) and PTH (n = 4). Continuous variables are given as median (interquartile range), categorical variables as number (%). Blood pressure is presented as peripheral systolic blood pressure (pSBP) and peripheral diastolic blood pressure (pDBP). Cardiovascular disease is defined as presence of either coronary artery disease and/or peripheral artery occlusive disease. HsCRP denotes high sensitivity C-reactive protein and PTH parathyroid hormone (**reference range: 15–65 pg/ml).
The median MoCA raw score achieved by the patients was 25 points. A total of 115 (47.5%) patients were classified as cognitively impaired (Table 2).
Cognitive testing at baseline
Values are presented as median (interquartile range). MoCA, Montreal Cognitive Assessment.
Outcomes: All-cause mortality
The median follow-up period was 3.54 years. In this period 69 deaths were observed, of which 28 (40.6%) were due to cardiovascular causes (sudden cardiac death n = 16, heart failure n = 7, myocardial infarction n = 2; stroke n = 2; pulmonary embolism n = 1). Table 3 provides further information about the follow-up outcomes.
Outcomes: All-cause mortality
N, number (% of total); IQR, interquartile range.
Association between global cognitive function and all-cause mortality
The Kaplan-Meier plot stratified by global cognitive function at baseline is shown in (Fig. 2). The log-rank test revealed a significant association between better performance on the MoCA test and all-cause mortality (p < 0.001).
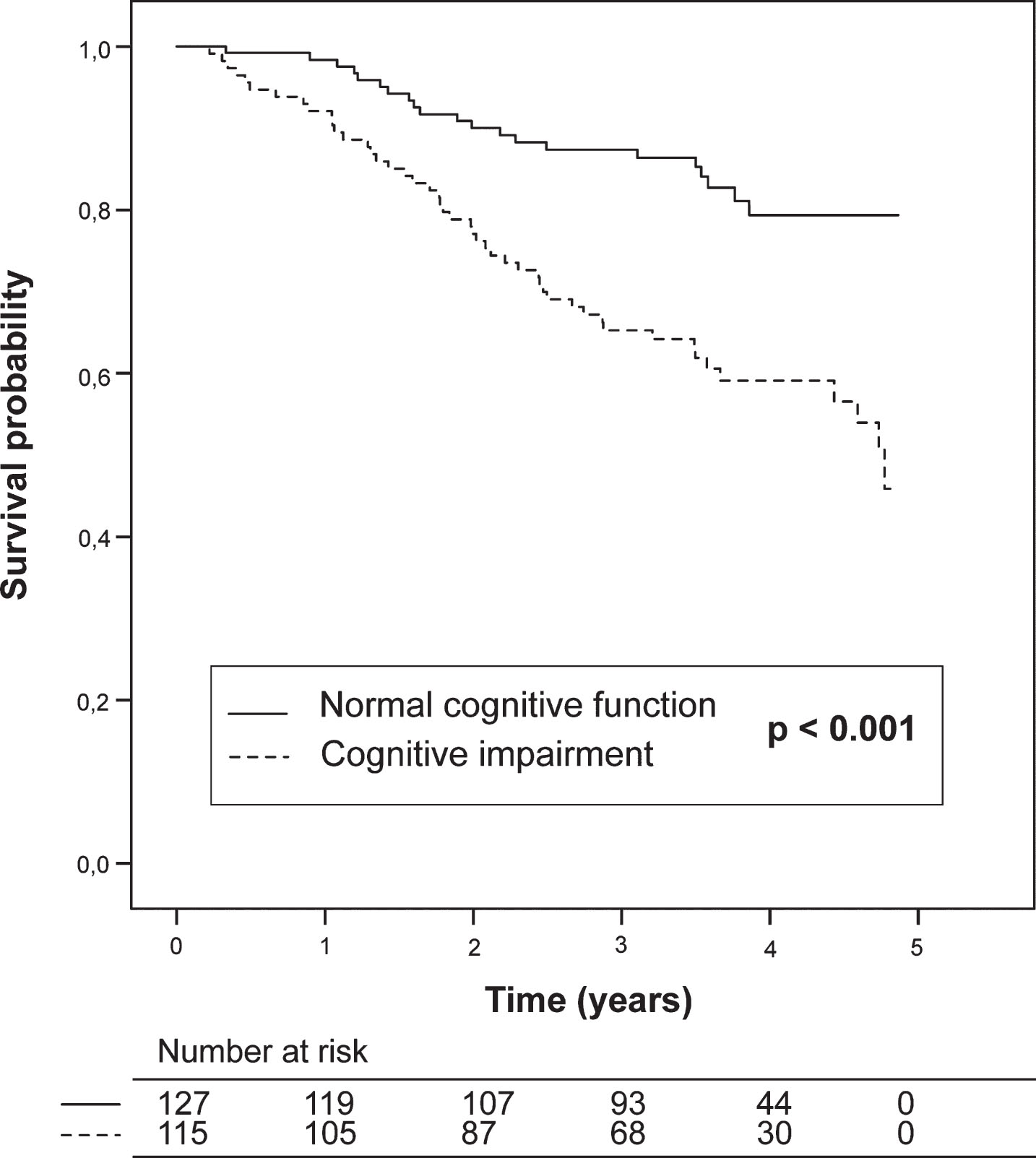
Kaplan-Meier plot for all-cause mortality stratified by cognitive function. Cognitive impairment is defined as Montreal Cognitive Assessment raw score ≤24 points. Log-rank test was used to compare both groups.
Patients with cognitive impairment at baseline had a significant almost 3-fold higher hazard for all-cause mortality compared to patients with normal cognitive function (unadjusted HR: 2.812; 95% CI: 1.683–4.698).
Other unadjusted predictors that significantly increased the risk for mortality, as identified by univariate Cox regression analyses, were age (HR: 1.063; p < 0.001), diabetes (HR: 2.428; p < 0.001), and cardiovascular disease (HR: 3.277; p < 0.001), while higher peripheral systolic blood pressure (HR: 0.987; p = 0.023), longer dialysis vintage, longer time per dialysis session (HR: 0.994; p = 0.023 and HR: 0.645; p = 0.049, respectively) and higher serum-albumin (HR: 0.293; p < 0.001) significantly reduced the risk for mortality (Table 4). The results of the univariate Cox regression analysis for all variables, including the non-statistically significant variables, are presented in Supplementary Table 1.
Univariate and multivariate Cox-regression analyses
Cognitive impairment was defined as a MoCA score ≤24 points. pSBP, peripheral systolic blood pressure; HR, hazard ratio; CI, confidence interval.
The significantly increased HR of cognitive impairment on mortality, identified in the univariate Cox regression analysis, remained significant in the multivariate Cox regression analyses. After adjusting for age, diabetes, cardiovascular disease, dialysis vintage, time on dialysis, albumin and peripheral systolic blood pressure, the significant adjusted HR of cognitive impairment was 1.749 (95% CI: 1.007–3.038; p = 0.047). Other variables with significant HR to all-cause mortality in the multivariate model were age, cardiovascular disease, albumin and peripheral systolic blood pressure (Table 4). With respect to 95% CIs, associations were more pronounced for albumin and cardiovascular disease and somewhat weaker for age, cognitive impairment, and peripheral systolic blood pressure.
Post-hoc, we repeated the multivariate Cox regression model adding a variable cerebrovascular disease, defined as a history of either TIA or ischemic/hemorrhagic stroke. The variable cerebrovascular disease did not attain statistical significance (adjusted HR: 1.038; 95% CI: 0.595–1.810: p = 0.897); and the HR of cognitive impairment at baseline on mortality remained largely unchanged (adjusted HR: 1.741; 95% CI: 0.999–3.036: p = 0.051).
Given the high cardiovascular burden and proposed cerebrovascular pathogenesis of cognitive impairment in hemodialysis patients, we considered analyzing the HR of cognitive impairment on mortality due to cardiovascular causes. Unadjusted Cox-regression demonstrated a significant effect (unadjusted HR: 3.077 with 95% CI: 1.355–6.989 and p = 0.007). We refrained from calculating a multivariate Cox regression model due to the small number of cardiovascular events (n = 28) limiting the number of confounders for adjustment [27, 28].
DISCUSSION
In this cohort study, we analyzed the association between global cognitive function, evaluated by the MoCA test, and all-cause mortality in a cohort of 242 maintenance hemodialysis patients. After a median observational interval of 3.54 years, almost one-third (28.5%) of study patients had died, confirming the high mortality of hemodialysis patients. Cognitive impairment at the time of study onset resulted in an almost 1.8-fold higher hazard for all-cause mortality after adjustment for commonly known risk factors. Thus, we were able to demonstrate a significant relationship between impaired global cognitive function measured by a short screening instrument and all-cause mortality in hemodialysis patients. The HR of the predictor cognitive impairment was the second largest and comparable to the impact of cardiovascular disease, underpinning the relevance of impaired cognition in assessing patients’ mortality risk. This association has previously been demonstrated in the general population [29, 30], but to our knowledge this is the first description in a cohort of hemodialysis patients. Two previous studies focusing on cognitive function and mortality in hemodialysis patients performed cognitive testing, but unlike our study, in both studies a battery combining various individual tests was applied: Griva at al. [11] conducted a study in 145 prevalent hemodialysis and peritoneal dialysis patients (mean age 50 years, 64.8 % male), whereby a total of 6 different neuropsychological tests (Trail Making Test Part A, Trail Making Test Part B, Symbol Digit Modalities, Rey Auditory Verbal Learning Memory Test, Benton Visual Retention Test and Grooved Pegboard) was carried out, each examining different cognitive domains. Cognitive impairment, defined as performing 1 SD less than normative values on 2 or more cognitive tests, was an independent predictor of all-cause mortality (adjusted HR: 2.53), which is per se in accordance with our results. However, no established short screening instrument or neuropsychological test battery to reliably confirm impairment of global cognition was used. Another limitation of this study consisted of the omission of important risk factors for mortality in hemodialysis patients in multivariate analysis such as albumin as surrogate parameter for protein energy wasting.
A more recent study by Drew et al. [12], which was comparable to our cohort in terms of sample size and demographical characteristics, took a similar approach: Two cognitive domain scores, executive and memory function, were derived from a battery of different neurocognitive tests. Only the relationship between executive function and all-cause mortality remained significant after adjusting for demographics, dialysis-related factors, cardiovascular disease, heart failure, and stroke. The overall score of the Mini-Mental State Examination (MMSE), which was used as a screening test to exclude patients with severe cognitive impairment, was not associated with all-cause mortality. This might be explained by the fact, that the MMSE in contrast to the MoCA is less sensitive to early stages of cognitive impairment and accounts less for executive function [31, 32], the cognitive domain, which seems to be impaired early in hemodialysis patients suggesting a vascular type of dementia in these patients [4, 34].
While the aforementioned studies excluded patients with more advanced stages of cognitive impairment, two previous studies focused on the relationship between previously diagnosed dementia and survival in dialysis patients [8, 10]. Cognitive testing was not performed. Both studies identified dementia as an independent risk factor for all-cause mortality. This underlines our findings especially with respect to patients with severe dementia, who might not be adequately addressed by our study (see below). Besides, cognitive impairment is often underdiagnosed in hemodialysis patients, emphasizing the importance of cognitive testing in this context [32, 35].
Although we intended to evaluate the association between cognitive impairment and cardiovascular mortality, as they may share a common pathogenesis in hemodialysis patients, we had to refrain from this investigation considering the small number of cardiovascular events in our cohort limiting the power to adequately control for all relevant confounders. At least in the unadjusted analysis impaired cognition resulted in a HR >3 for cardiovascular mortality. Future studies with larger study populations and longer follow ups might reveal a possible association in hemodialysis patients.
There are several limitations to our study: first, patients with advanced cognitive impairment might be underrepresented within our study cohort, as patients already suffering from marked cognitive impairment might not have volunteered to participate in the study. Even though we did not a priori exclude patients with a preexisting diagnosis of dementia, the effect between cognitive impairment and mortality might therefore be even greater in a representative hemodialysis cohort. However, impaired cognition resulted in one of the highest HR despite being only mildly impaired in this cohort. This underscores the importance of implementing standardized cognitive testing in the staging of hemodialysis patients in order to detect cognitive impairment already at early stages providing a longer window of opportunity to modify this risk factor.
The lack of control for cerebrovascular disease might be considered another limitation, as cerebrovascular disease is an important risk factor for mortality in the general population and its prevalence is markedly elevated in hemodialysis patients. The post-hoc analysis including cerebrovascular disease yielded a non-significant HR of 1.038 on all-cause mortality. Cognitive impairment and cerebrovascular disease probably share a common pathogenesis (atherosclerosis of cerebral micro- and macrocirculation) in hemodialysis patients. This assumption is further supported by the high cardiovascular burden and the early impairment of executive functions in this patient population, as already stated above [4, 5]. Nevertheless, apart from cardiovascular disease (see below) cerebrovascular disease may be considered more carefully in future studies dealing with mortality and cognitive impairment in hemodialysis patients.
Lastly, the number of events, especially cardiovascular events, was relatively small in our cohort, compelling us to make a selection among possible confounders in the multivariate analysis. Larger cohorts and longer follow-up intervals will help to further explore the impact of cognitive impairment on mortality and especially cardiovascular mortality. Also, the impact of cognitive impairment, which remained only marginally significant despite the high HR of 1.749 in the multivariate approach, could be further evaluated in such studies.
In conclusion, the present study demonstrates a relationship between impairment of global cognitive function tested by a short screening instrument and all-cause mortality in a cohort of hemodialysis patients for the first time. Thus, the MoCA test could serve as an easily applicable tool in clinical routine in the future to identify those hemodialysis patients at risk of cardiovascular events and death. Implementing the MoCA test into a risk stratification algorithm may contribute to improved medical care. Nevertheless, additional studies are needed to further explore the cause of cognitive impairment in dialysis patients and to find possible avenues of prevention.