
Abstract
Cerebral amyloid-β (Aβ) plaques are the hallmark biomarker of Alzheimer’s disease (AD) and are detectable decades before clinical symptoms. Modifying risk factors associated with Aβ accrual offers an opportunity for AD prevention. While midlife vascular health is linked to AD; there is minimal longitudinal evidence regarding the effect of midlife lipids on Aβ. We examined the association between midlife lipids and Aβ 20 years later. One hundred and twenty-two women had serum lipid profiles in midlife (1992, 45–57 years), and cerebral imaging, genotyping, and cognition measured 20 years later (2012/13, 66–77 years). Imaging was performed in 2012/13 via F-18 Florbetaben positron emission tomography (PET) and standard uptake value ratios (SUVR) were calculated. Lipid profiles and other predictors of high PET-SUVR levels (>1.2) were evaluated using multivariable logistic regression. Increases in low-density lipoprotein (LDL) cholesterol in midlife were associated with Aβ, adjusting for age, education, cholesterol medication, and cognition (AdjOR1.81, 95% CI 1.08–3.01, p = 0.024), but attenuated on adjustment for apolipoprotein E4 (APOE ɛ4). Aβ risk increased in women with APOE ɛ4 and midlife cholesterol >6.2 mmol/L (AdjOR9.59, 95% CI 2.94–31.31, p < 0.001), APOE ɛ4 and LDL >3.3 mmol/L (AdjOR9.00, 95% CI 2.89–28.03, p < 0.001), and APOE ɛ4 and cholesterol to high-density lipoprotein ratio ≥3.25 (AdjOR8.32, 95% CI 2.32–29.89, p < 0.001). Presence of APOE ɛ4 and midlife dyslipidemia compounded the risk for Aβ deposition, although no independent effect of midlife lipids was found. Lipid-modifying treatment in midlife could mitigate the risk of Aβ in women with a genetic predisposition for AD. To better inform prevention, future consideration should be given toward managing dyslipidemia in women carrying the APOE ɛ4 allele.
Keywords
INTRODUCTION
Alzheimer’s disease (AD) dementia is a public health concern for the aging population, with the risk doubling every five years over the age of 65 [1]. Cerebral amyloid plaques (comprised of amyloid-β [Aβ] peptides) and neurofibrillary tangles (comprised of hyperphosphorylated tau) are the neuropathological hallmarks of AD [2], with the accrual of Aβ able to be identified decades preceding clinical diagnosis [3, 4]. To date, the reversal of cognitive symptoms appears resistant to ‘anti-amyloid’ therapies [5]. This highlights the importance of identifying modifiable lifestyle factors associated with Aβ accrual, to provide options for early preventative therapies in people at risk of conversion to disease, before clinical symptoms manifest.
Midlife vascular health has been associated with the risk of developing dementia [6 –9]. However, the few studies examining vascular risk contributions to cerebral Aβ deposition in humans have produced inconsistent results, creating challenges around the appropriate risk factors to target in prevention. Reed and Colleagues (2014) demonstrated a cross-sectional relationship with low- and high-density lipoprotein cholesterol levels and increased Aβ in older adults [10]. While one longitudinal study showed midlife dyslipidemia to be the only vascular risk factor predictive of cerebral Aβ [11], others have found no independent effects of midlife cholesterol on late-life Aβ accrual [12, 13], with one study demonstrating only high triglyceride levels in midlife predicted Aβ deposition 20 years later [13].
The evidence to date has yielded marginal findings in regards to midlife lipid profiles affecting Aβ accrual, which may be in part attributed to sex- biases that have been overlooked in previous studies. Women are predisposed to having elevated lipid levels during and after menopause [14], and experience more rapid cognitive decline and risk of conversion to dementia [15]. The genetic risk variant for AD, apolipoprotein E allele ɛ4 (APOE ɛ4), may also interact differently in women posing a greater risk of clinical conversion from healthy aging to disease [16]. In this context, the current study aimed to investigate the effect of midlife lipid profiles on Aβ load 20 years later in a cohort of aging Australian women. Given the involvement of APOE in brain cholesterol metabolism, amyloid accrual, and AD risk [17], we also examined the role of APOE ɛ4 in this relationship.
MATERIALS AND METHODS
Study design and cohort
Participants were recruited from the Women’s Healthy Ageing Project (WHAP), an ongoing longitudinal cohort of Australian women aged between 45–55 years at baseline. Details of the WHAP cohort have been previously described [18]. Participants were included in this analysis if they had complete serum lipid profiles, brain imaging, and covariates.
Serum lipid profiles
Fasted blood samples (80 ml) were collected at both time points, processed and serum aliquots stored at –80°C until measurement. Cholesterol measures were obtained using the Olympus AU2700 Chemistry Analyzer, measuring total cholesterol (TC), high-density lipoprotein (HDL), and triglycerides. Low density lipoprotein (LDL) cholesterol levels were calculated using the Friedewald formula [LDL = (TC-HDL)— (triglyceride/2.2) [19] and adapted to International System (SI) of Units.
Positron emission tomography
Cerebral Aβ was measured using F-18 Florbetaben (18F-FBB) positron emission tomography (PET) scanning at the follow-up review (2012/13). Participants received 250 MBq of 18F-FBB intravenously, with a 20 min acquisition commencing 90 min post-injection. Standardized uptake values (SUV) were calculated for all brain regions examined, and standard uptake value ratios (SUVR) were generated by normalizing regional SUV by the cerebellar cortex [20], with atrophy-correction from structural magnetic resonance imaging (MRI). The cerebellum has been noted as an ideal reference for 18F-FBB and can detect earlier deposition of Aβ [20]. MRI scans were performed on a Siemens 3T Tim Trio Scanner and the structural sequences utilized for atrophy correction have been described previously [18]. Area-weighted means were calculated for each participant by averaging the frontal, superior parietal, lateral temporal, lateral occipital, and anterior and posterior cingulate regions. Neocortical SUVR, a global index of amyloid burden, is expressed as the average SUVR of the area-weighted mean. This index was used to stratify participants as low (PET-SUVR ≤1.2) and high (PET-SUVR >1.2) neocortical amyloid load using previously described cut-offs [13].
Covariates
Sociodemographic and lifestyle characteristics were assessed at baseline and follow-up as potential covariates influencing Aβ accrual. These included; age (years), education level, body mass index ([BMI]; calculated as weight (kg)/height (m2)), self-reported current smoking status (yes/no), self-reported use of cholesterol-lowering medication (yes/no), physical activity (frequency, days per week), self-reported current or prior diagnosis of hypertension and diabetes (2012/13 only). APOE allele, measured from whole blood collected in 2012/13, was categorized into APOE ɛ4 present (one or two ɛ4 alleles) or APOE ɛ4 not present (ɛ2/ɛ3 alleles). Global cognition was also measured in 2012/13 using the Mini-Mental State Examination (MMSE) score.
Statistical analysis
All continuous variables were tested for normality prior to data analysis using graphical (histogram) and analytical (Shapiro-Wilks test) methods. Participant demographics, anthropometric measures, biochemical data and the presence of APOE ɛ4 were compared in the high and low PET-SUVR groups using Pearson’s Chi-Square of Fisher’s exact for categorical data, and either Student’s T-test or Wilcoxon U-test for continuous or ordinal data. Although there are no definitive preventative guidelines for brain health, to enhance the clinical interpretation and relevance of risk reduction guidelines, lipid parameters were categorized as per the scales indicative of low to high risk of cardiovascular disease, based on the Australian Heart Foundation and The Royal Australian College of General Practitioners.
Spearman’s rank correlations were performed to examine the correlations between midlife (1992) and late-life (2012/13) lipid levels. The relationship between lipid profiles and other predictors of high PET-SUVR levels (>1.2) were evaluated using multivariable logistic regression. In the absence of any definitive SUVR cut-offs, sensitivity analysis was undertaken to check whether results remained consistent at different cut-off levels (1.1, 1.3, and 1.4). The models were adjusted for the factors either commonly reported in previous literature or were significantly associated with SUVR at baseline or in 2012/13 (if the variable was not measured at baseline). In addition, in order to not over-adjust the model, assuming sample limitations, the number of factors included in the model had to be restricted. Therefore, factors were not included if they strongly correlated with age, education and other covariates included in the model (physical activity and BMI were both strongly correlated with age (p < 0.001 for both), smoking correlated with education (p = 0.004)). A cumulative cardiovascular risk score was also not included in the model due to its collinearity with the individual lipids measured. The regression models were adjusted for age, education level, the use of cholesterol modifying medications, MMSE, and APOE ɛ4. Based on a priori hypothesis, structural equation models (SEM) were used to assess to what degree the impact of lipids on SUVR is mediated by APOE genotype. Statistical significance for all tests was set at p < 0.05 (two-sided) and analyses were conducted using STATA/SE 15.0 (StataCorp LLC, College Station, TX, USA).
RESULTS
Cohort characteristics
Two-hundred and forty-five participants completed a midlife baseline (1992) and follow-up (2012/13) assessment and were included in this study. Of those, 122 participants had a PET scan at follow-up (Fig. 1). Those who completed the follow-up assessment were less likely to smoke (16.3% versus 24.5%, p = 0.024) and more likely to have tertiary education (40.4% versus 28.3%, p = 0.01) compared to those who did not return for the follow up (Supplementary Table 1).
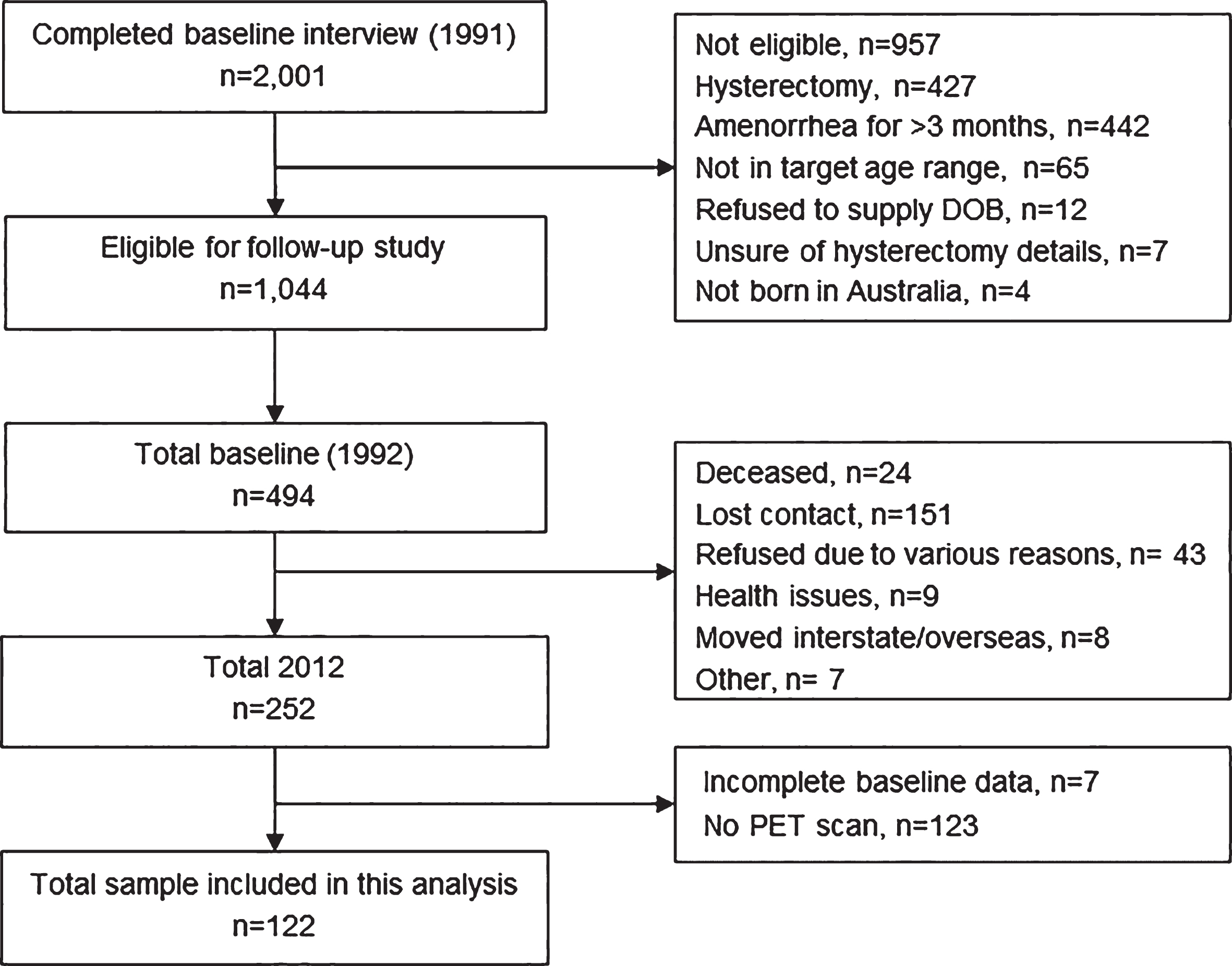
Flow diagram of participant inclusion into this study. Chart outlining the selection of the participants for the current study from the larger Women’s Healthy Ageing Project (WHAP) longitudinal study.
The average age, education, BMI, smoking status, prevalence of diabetes or hypertension, and frequency of physical activities did not differ between participants with elevated (>1.2) and normal SUVR (≤1.2). Participants with elevated SUVR were more likely to carry the APOE ɛ4 allele (65% versus 25%, p < 0.001) (Table 1). There was a 10-fold increase in the use of cholesterol modifying medications from baseline to follow-up, being 19% higher in the elevated SUVR group (57% versus 37%), although not reaching statistical significance (p = 0.093). Those with elevated SUVR had higher midlife total cholesterol (6.27±0.99 versus 5.80±0.96 mmol/L), LDL (4.22±0.93 versus 3.69±0.93 mmol/L) and total cholesterol to HDL ratios (3.98 (3.6–4.8) versus 3.66 (2.93–4.19)) (Table 2). Mid- and late-life total cholesterol, LDL cholesterol, total cholesterol to HDL ratio and late-life triglycerides were also all higher in those who were APOE ɛ4 positive (Table 2). Presence of APOE ɛ4 did not have an effect on mid- or late-life HDL cholesterol levels.
Demographic characteristics of the study cohort
aNote: APOE ɛ4 genotype data missing for 3 participants. Results reports as N (%) or as specified. The differences between groups were assessed using: Student’s t-test used for age; Mann-Whitney U-test for BMI and PET-SUVR; Fisher’s exact for smoking, education and the use of cholesterol modifying medications in 1992; and Chi2 for APOE ɛ4 and the use of cholesterol modifying medications in 2012/13. BMI, body mass index; MMSE, Mini-Mental State Examination; PET, Positron-emission tomography; SUVR, Standardized uptake volume ratio.
Differences in midlife and late-life lipid levels by PET-SUVR levels and APOE ɛ4 status
Results reported as mean (SD) or median (Q1–Q3). Between group differences assessed using either T-test or Mann-Whitney U-test as appropriate. HDL, high-density lipoprotein; LDL, low-density lipoprotein; PET, Positron emission tomography; PET-SUVR, Standardized uptake volume ratio; SD, standard deviation; IQR, interquartile range.
The association between midlife lipids and Aβ 20 years later
Presence of APOE ɛ4 was a strong predictor of having high SUVR >1.2, after adjustment for age, education, cholesterol lowering medications, and MMSE (Odds Ratio (OR) 5.55, 95% CI 2.00–15.41, p = 0.001). Increased levels of LDL cholesterol in midlife was associated with the increased risk of evaluated PET-SUVR 20 years later even after adjustments for age, education, use of cholesterol lowering medications, and MMSE (OR 1.81, 95% CI 1.08–3.01, p = 0.024), but became not significant after the adjustment for APOE ɛ4 (OR 1.47, 95% CI 0.84–2.57, p = 0.175 (Table 3).
Relationship between midlife lipid levels (1992) and high PET-SUVR 20 years later
Adjusted model 1 - adjusted for age, Education and cholesterol lowering medications. Adjusted model 2 - adjusted for age, Education, use of cholesterol lowering medications and Mini-Mental State Examination Score. Adjusted model 3 - adjusted for age, Education, use of cholesterol lowering medications, Mini-Mental State Examination Score and APOE ɛ4. Results in boldface indicate statistical significance. HDL, high-density lipoprotein; LDL, low-density lipoprotein; PET, positron emission tomography; PET-SUVR, standardized uptake volume ratio.
Using clinical risk cut-offs, midlife total cholesterol >6.2 mmol/L was associated with a higher risk of high PET-SUVR (OR 2.86, 95% CI 1.11–7.34, p = 0.030); however, this association attenuated after adjustment for other factors (Table 3). No associations were observed between levels of triglyceride or HDL cholesterol levels and high SUVR. Sensitive analyses for alternate cut-offs of high SUVR displayed similar direction of results (Supplementary Tables 2–4).
There were no significant correlations between mid- and late-life LDL (rho = 0.12, p = 0.08) or mid- and late-life total cholesterol (rho = 0.13, p = 0.05) levels. When examining the association between late-life lipids and high PET-SUVR, neither higher levels of LDL cholesterol (OR 1.03, 95% CI 0.69–1.54, p = 0.889) or total cholesterol (OR 1.10, 95% CI 0.77–1.57, p = 0.615) were associated with high PET-SUVR.
The association between APOE ɛ4, midlife lipid levels, and Aβ 20 years later
Path diagrams from adjusted mediation models, with unstandardized estimates for direct and indirect effects of APOE ɛ4 and lipid levels are displayed in (Supplementary Figure 1). The presence of the APOE ɛ4 independently predicted the likelihood of having high PET-SUVR (β 0.27, 95% CI 0.24–0.32), having high total cholesterol (β 0.26, 95% CI 0.20–0.30) and high LDL cholesterol (β 0.19, 95% CI 0.02–0.37). There was no effect of APOE ɛ4 on PET-SUVR via any lipids (Supplementary Figure 1).
The presence of the APOE ɛ4 allele and having had high levels of total or LDL cholesterol in midlife led to 9-fold increase in the risk of high PET-SUVR in late-life (Fig. 2). Similarly, those with high total cholesterol/HDL ratios over 3.25 and presence of the APOE ɛ4 genotype had an 8-fold increase in the risk of high PET-SUVR levels. While those who had APOE ɛ4 with high HDL (>1.5 mmol/L) still had a 3-fold risk in high PET-SUVR, this was lower than the overall independent risk of APOE ɛ4.
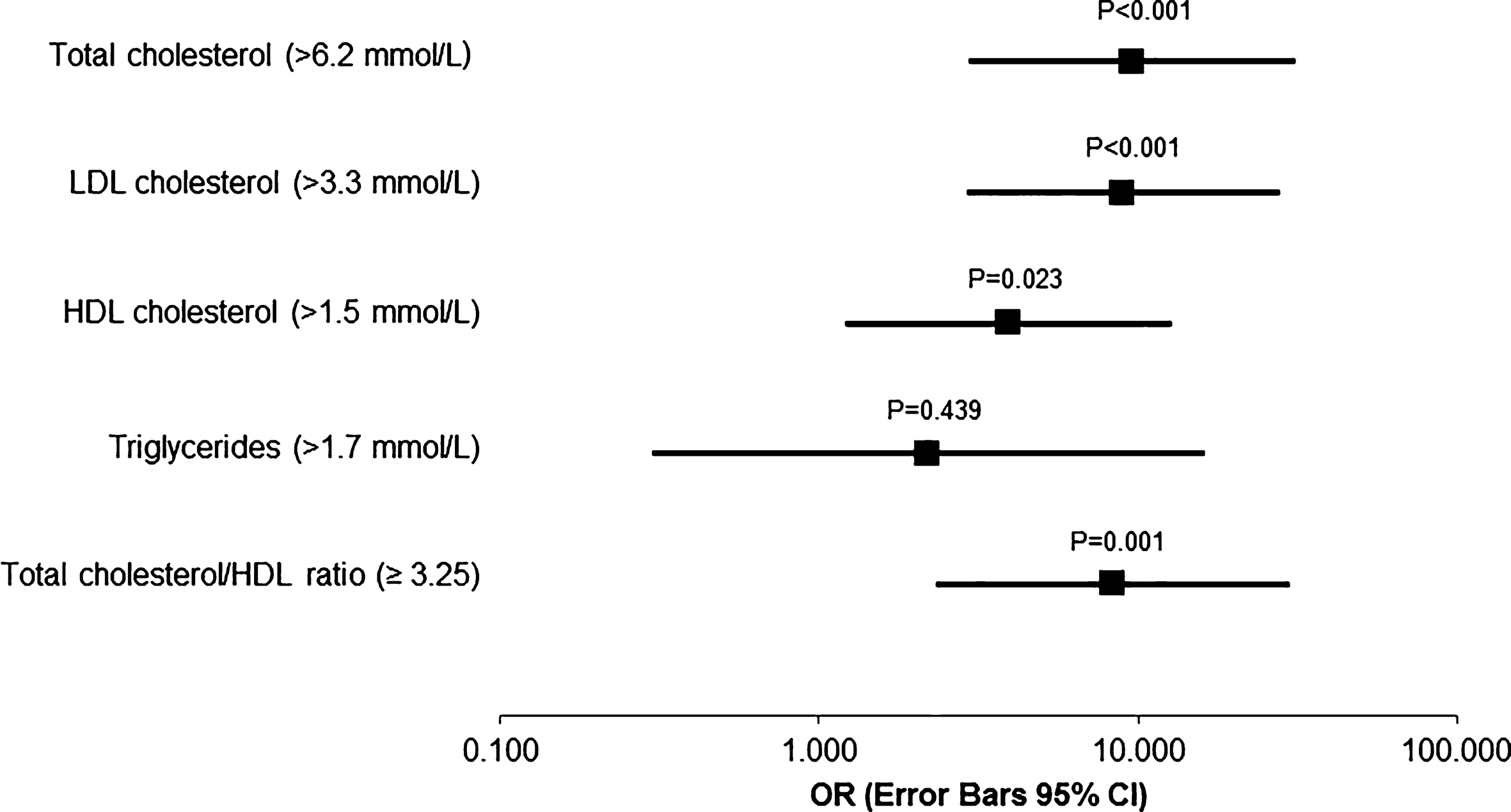
Forest plot for the effect of apolipoprotein ɛ4 presence combined with high midlife lipid levels on amyloid-β 20 years later. HDL, high-density lipoprotein; LDL, low-density lipoprotein. Results are adjusted for age, education, cholesterol lowering medication and Mini-Mental State Examination.
DISCUSSION
In aging women, the presence of the APOE ɛ4 allele increased both midlife cholesterol levels and Aβ deposition, suggesting an absence of any independent effect of midlife lipids on late-life Aβ. However, those carrying the APOE ɛ4 allele and having high cholesterol in midlife had a compounded risk of cerebral Aβ deposition 20 years later, which was greater than the risk from APOE ɛ4 alone. Having protective levels of HDL cholesterol appeared to reduce some of the APOE ɛ4 risk for high Aβ, although did not eliminate it. In line with evidence for midlife dyslipidemia increasing the risk of AD [6 –9] and cognitive decline [21], our findings suggest that this relationship may be attributed to a link between APOE ɛ4, midlife dyslipidemia, and Aβ deposition, which appears to be particularly unique to women. While clinical trials are needed to confirm these findings, our results shed light on an age-window in midlife, where management for dyslipidemia in women with an increased genetic predisposition for developing AD, may mitigate the risk of Aβ accrual and subsequent conversion to disease.
Previous studies have yielded inconsistent findings regarding the effect lipid profiles have on Aβ deposition. While cross-sectional evidence suggests high LDL and low HDL were related to greater Aβ deposition in an elderly population [10], longitudinal studies have not produced the same results. Two studies have shown either midlife dyslipidemia [11] or triglyceride levels [12] to be predictive of late-life Aβ, while another showed only an effect of cumulative vascular risk factors, with no independent effect of cholesterol [10]. Contrary to our findings, these previous studies showed no influence of APOE genotype. While our findings are in line with previous data showing an APOE ɛ4 modified effect on cardiovascular disease and risk of cognitive decline [22], one fundamental point of difference can be attributed to the sex distribution between the current and previous studies. In our cohort of women, the presence of APOE ɛ4 appeared to be the influencing factor for both midlife dyslipidemia and late-life Aβ deposition. It is well understood that women are more likely to possess the APOE ɛ4 allele [23 –25] with recent evidence also revealing the influence of female sex on the APOE ɛ4 risk for conversion to AD [16]. In this context APOE ɛ4 may interact with midlife vascular risk factors differentially in women compared with men.
The menopause, which is unique to women, encompasses both an increase in lipid levels and risk of cerebrovascular disease [14]. Together with the direct effects of APOE ɛ4 on midlife dyslipidemia and Aβ deposition, the existence of both risk factors appeared to exacerbate the risk of amyloid-deposition in women. Type of menopause has also been suggested to play a role in midlife vascular and metabolic health, with evidence to suggest those who undergo surgical menopause may have greater levels of Aβ deposition [26] and a greater metabolic risk profile [27 –29]. Given all women in this study had undergone non-surgical menopause, future investigation into the risk of vascular and amyloid pathologies following various forms of menopause is needed. Traditionally, lipid-modifying medications have been prescribed with the goal of reducing absolute cardiovascular risk, rather than individual lipid levels [30]. Our findings now suggest that maintaining a healthy lipid profile in midlife, particularly in women with the genetic risk variant for AD, could be an important preventative approach to reduce the risk of Aβ accumulation and subsequent disease in aging women.
The current findings reflect the proposed mechanisms by which APOE ɛ4 may interact with cholesterol to affect Aβ accrual [31, 32]. The APOE ɛ4 polymorphism and dyslipidemia both raise the risk of atherosclerosis [33], which in turn can damage cerebral vessels and the endothelium of the blood-brain barrier [34]. Additionally, a direct link between high circulating and high cerebrospinal fluid levels of cholesterol has also been proposed through oxysterol influx [32, 35]. The additional risk of APOE ɛ4 may also suppress neuronal cholesterol efflux through preferential binding with LDL, creating a less efficient environment for Aβ clearance [36]. Although not measured in this study, these mechanisms may help explain the deleterious associations with circulating total and LDL cholesterol observed, rather than a protective effect of HDL in people that were APOE ɛ4 positive. Together with the reduced ability for APOE ɛ4 to aid in releasing cholesterol from the brain, the presence of both risk factors may lead to altered cholesterol metabolism, oxidative stress, and inflammatory cytokines, interfering with the clearance of cerebral Aβ proteins.
Limitations and future directions
The measurement of LDL cholesterol was generated using the clinically recognized Friedewald equation [37, 38], which may underestimate LDL levels, particularly in individuals with high triglycerides [39]. As the average triglyceride levels in our cohort were in the normal range (<1.7 mmol/L), the use of this equation is unlikely to have materially affected the results. Of interest in future research would be the measurement of LDL subclasses, particularly LDL particle diameter, since the inflammatory consequences of LDL seem to be greater in smaller LDL particles [40, 41], while triglyceride concentration is inversely proportionate to LDL diameter [42]. As we did not have data on LDL particle size or other LDL subclasses, we were unable to examine these associations in our cohort. Additionally, the absence of the measurement of tau proteins precludes our ability to discuss the effect of midlife lipids on all neuropathology biomarkers of Alzheimer’s disease. In women, the APOE ɛ4 risk has been associated with a more robust acceleration in tau pathology. Recent evidence has also suggested that midlife triglycerides were more strongly associated with abnormal Aβ42/phosphorylated tau ratios than PET Aβ [12], warranting future examination of midlife lipid profiles on a range of AD biomarkers. Although our sample size is larger than previous studies measuring cerebral Aβ [10], healthy retention bias, which is common in longitudinal cohort studies, may have influenced the lower numbers of Aβ positive participants and overall power. Nevertheless, our results share similarities with a recent large-scale behavioral paper from the Atherosclerosis Risk in Communities study [21], which showed the relationship between midlife total cholesterol, LDL and triglycerides on 20-year cognitive decline to also be modified by APOE ɛ4. Lastly, examination of a female-only cohort is a considerable strength of this study, given the high prevalence of vascular risk factors, APOE ɛ4 presence, and AD onset in women. However, our findings were unable to examine whether APOE ɛ4 affects this relationship in men. Potential sex-specificity of lipid associations with Aβ accrual merits further investigation and replication.
Conclusions
The current findings suggest the presence of APOE ɛ4 primarily explains the association between midlife dyslipidemia and late-life Aβ deposition in women. Women carrying the APOE ɛ4 genotype and who experienced dyslipidemia in midlife had a compounded risk of Aβ deposition 20 years later. While clinical trials are needed to confirm these findings, lipid-lowering medication administered in midlife may only mitigate the risk of Aβ deposition and subsequent conversion to disease in women with the APOE ɛ4 risk variant.
Footnotes
ACKNOWLEDGMENTS
Funding for the Healthy Ageing Program (HAP) has been provided by the National Health and Medical Research Council (NHMRC Grants 547600, 1032350 & 1062133), Ramaciotti Foundation, Australian Healthy Ageing Organisation, the Brain Foundation, the Alzheimer’s Association (NIA320312), Australian Menopausal Society, Bayer Healthcare, Shepherd Foundation, Scobie and Claire Mackinnon Foundation, Collier Trust Fund, J.O. & J.R. Wicking Trust, Mason Foundation and Alzheimer’s Australia. Inaugural funding was provided by VicHealth and the NHMRC. The Principal Investigator of HAP (CSz) is supported by the National Health and Medical Research Council. EH is supported by an Australian Government Research Training Program Scholarship.
We would like to acknowledge the contribution of the participants and their supporters for their time and commitment for over 20 years to the University. We thank Melbourne Health Pathology services for providing blood biomarker storage and analyses. We thank the research assistants who assisted in data collection. A full list of all researchers contributing to the project and the membership of our Scientific Advisory Board is available at ![]() . We are thankful to our participants, team, partners and supporters for making this study of now more than 20 years possible.
. We are thankful to our participants, team, partners and supporters for making this study of now more than 20 years possible.
This study was approved by the University of Melbourne Human Research Ethics Committee (HREC: 931149X, 1034765, 1105251 & 750632.1), and all participants provided written informed consent. Participants did not receive a stipend for participating in this study. The study was conducted in accordance with the National Health and Medical Council Ethical Conduct in Human Research and Declaration of Helsinki.