
Abstract
Background:
The diagnostic workup of idiopathic normal pressure hydrocephalus (iNPH) can be challenging due to an overlap in symptoms and neuroimaging features with other disorders. Despite a growing interest, a cerebrospinal fluid (CSF) biomarker profile in iNPH has not yet been identified.
Objective:
To determine the CSF biomarkers with the greatest evidence for differentiating iNPH from the most common differential diagnoses, Alzheimer’s disease (AD) and subcortical ischemic vascular disease (SIVD).
Methods:
A systematic literature search was conducted in PubMed to identify relevant articles up to July 2018 using the following MESH-terms: “Cerebrospinal fluid”, “diagnos*”, “hydrocephalus, normal pressure”. Relevant data were extracted to assess the risk of bias in the included studies.
Results:
Twenty-five studies including 664 patients with iNPH, 502 with AD, 57 with SIVD, 81 with other disorders, and 338 healthy controls (HC) were included. They investigated the diagnostic value of 92 CSF biomarkers. Most evidence existed for amyloid-β 42 (Aβ 42), phosphorylated tau (p-tau), and total tau (t-tau) in iNPH versus AD and HC: Aβ 42 did not differ between iNPH and AD, but was lower than in HC subjects. T-tau and p-tau were lower in iNPH versus AD on a level comparable to HC subjects. There was moderate or limited evidence for 62 and 88 biomarkers, respectively. Several plausible biases characterize the literature including small sample sizes and inconsistent diagnostic criteria.
Conclusion:
T-tau and p-tau may differentiate iNPH from AD and Aβ 42 from HC. A combination of these biomarkers may improve the diagnostic accuracy in iNPH.
Keywords
INTRODUCTION
Idiopathic normal pressure hydrocephalus (iNPH) is one of the few potentially reversible causes of dementia. The characteristic symptom triad of gait disturbance, cognitive decline, and urinary incontinence is possibly explained by a disruption of the cerebrospinal fluid (CSF) dynamics. Impaired CSF absorption leads to a pathological flow of CSF into the periventricular white matter initiating a cascade of pathological processes such as neuronal degeneration, edema, and capillary microinfarctions [1]. The ventricular system is enlarged and often surrounded by white matter lesions representing periventricular edema on magnetic resonance imaging (MRI). The diagnostic workup can be challenging for several reasons. First, the symptomatology and neuroimaging features of iNPH overlap with other disorders, such as Alzheimer’s disease (AD) and subcortical ischemic vascular disease (SIVD). The cognitive deficits in patients with iNPH are characterized by predominantly subcortical and frontal dysfunction including memory decline, attention and executive impairment [2]. In many cases, this resembles the clinical appearance of patients with AD and SIVD. Also, gait disturbance and urinary incontinence occur in both patient groups due to vascular pathology disturbing the complex subcortical network responsible for gait and micturition. Up to 89% of patients with AD have subcortical infarcts [3]. In addition to patients with iNPH, ventriculomegaly may also be observed in AD and SIVD as a result of cerebral atrophy rather than impaired CSF absorption. Therefore, diagnostic criteria for iNPH based on clinical and radiological findings may be inaccurate and include patients with neurodegenerative diseases [4]. Second, some researchers and clinicians identify iNPH subjects by their response to CSF tap test or shunt surgery to overcome the diagnostic challenges of iNPH. To diagnose a disease by its response to test or treatment is problematic, as the response can be very challenging to define. Lastly, no supplementary tests have achieved a sufficient level of sensitivity or specificity for iNPH [5].
In order to ensure accurate diagnosis and improve the prediction of shunt response, there has been a growing interest to identify CSF biomarkers characteristic of iNPH. The CSF surrounds and interacts with the brain parenchyma and is thereby able to reflect pathological processes of the brain. A CSF biomarker profile in iNPH has not yet been identified, which may be partly explained by the lack of specific pathology related to iNPH. To shed light on the complex pathology of iNPH and to optimize the diagnostic process of iNPH, we aimed to systematically evaluate the existing literature on CSF biomarkers and their ability to differentiate iNPH from the most common differential diagnoses, AD and SIVD. We determined the current most promising biomarkers of iNPH based on their diagnostic value. Furthermore, we summarize the potential biases that characterize the current state of research on CSF biomarkers in iNPH.
METHODS
Protocol
Prior to the data search, all authors agreed on a protocol describing the methods of the review. The systematic literature review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [6].
Eligibility criteria
Studies that investigated the diagnostic value of CSF biomarkers in patients with iNPH were eligible for review if they 1) were original work (not reviews or meta-analyses), 2) were in English, and 3) were published in full text. Studies were excluded if they 1) were animal studies or postmortem studies, 2) were duplicate publications of an identical dataset, 3) had a control group or a diagnostic group of relevance that consisted of less than ten individuals, 4) did not include healthy controls (HC) or other diagnostic groups besides patients with iNPH, 5) did not separate patients with iNPH from patients with secondary NPH, 6) did not primarily focus on CSF biomarkers, and 7) were commentaries or case reports.
Search
Two authors (AMH and CM) separately searched the database Pubmed for relevant articles published before July 2018. The following search strategy, including the filters “English” and “Human”, was applied: (“Cerebrospinal Fluid” [Mesh] OR CSF) AND diagnos* AND “Hydrocephalus, Normal Pressure” [Mesh]. Furthermore, studies from relevant reference lists were included.
Study selection
Initially, studies were screened by title and abstract by author CM and studies that were clearly irrelevant were excluded. Afterwards, two authors (AHS and CM) independently assessed the eligibility. The studies were discussed with the third and fourth author in case of disagreements.
Data items
The eligibility assessment was carried out using a data extraction form constructed as a checklist. The following data were extracted: the first author’s name, year of publication, country, study design, number of cases and controls, age, sex, inclusion and exclusion criteria, diagnostic criteria, CSF source and sampling, analytical methods, and CSF biomarker levels.
Synthesis of results
The biomarkers investigated in the included studies were grouped into three categories based on the level of evidence for their ability to differentiate iNPH from a specific diagnostic group. Biomarkers studied in minimum three studies with consistent results were classified as having most evidence. Biomarkers studied in two studies with consistent results or studied only once in a study with a large sample size of patients with iNPH (n≥30) were classified as having moderate evidence. Lastly, biomarkers studied twice with inconsistent results or studied once in a small study (n < 30) were classified as having limited evidence.
Risk of bias in individual studies
To address the risk of bias in the included studies, the following components of the extracted data were evaluated for potential sources of bias: 1) Selection of study population: Study design, sample size, age and sex, inclusion and exclusion criteria, and diagnostic criteria; 2) Pre-analytical and analytical variables: The circumstances of CSF sampling, analytical methods, and blinding of laboratory staff.
RESULTS
Study selection
The initial search revealed a total of 267 publications of which 246 were identified during the database search and 21 by hand search. Reviews, meta-analyses, guidelines, duplicates, comments, and case reports were excluded after screening titles and abstracts (n = 40). Full text assessment was done in 227 publications, which lead to the exclusion of further 202 papers, since they did not meet the inclusion and/or exclusion criteria. Thereby, 25 publications from 1991 to July 2018 were selected for analysis. A schematic flow chart of the literature search is illustrated in Figure 1.
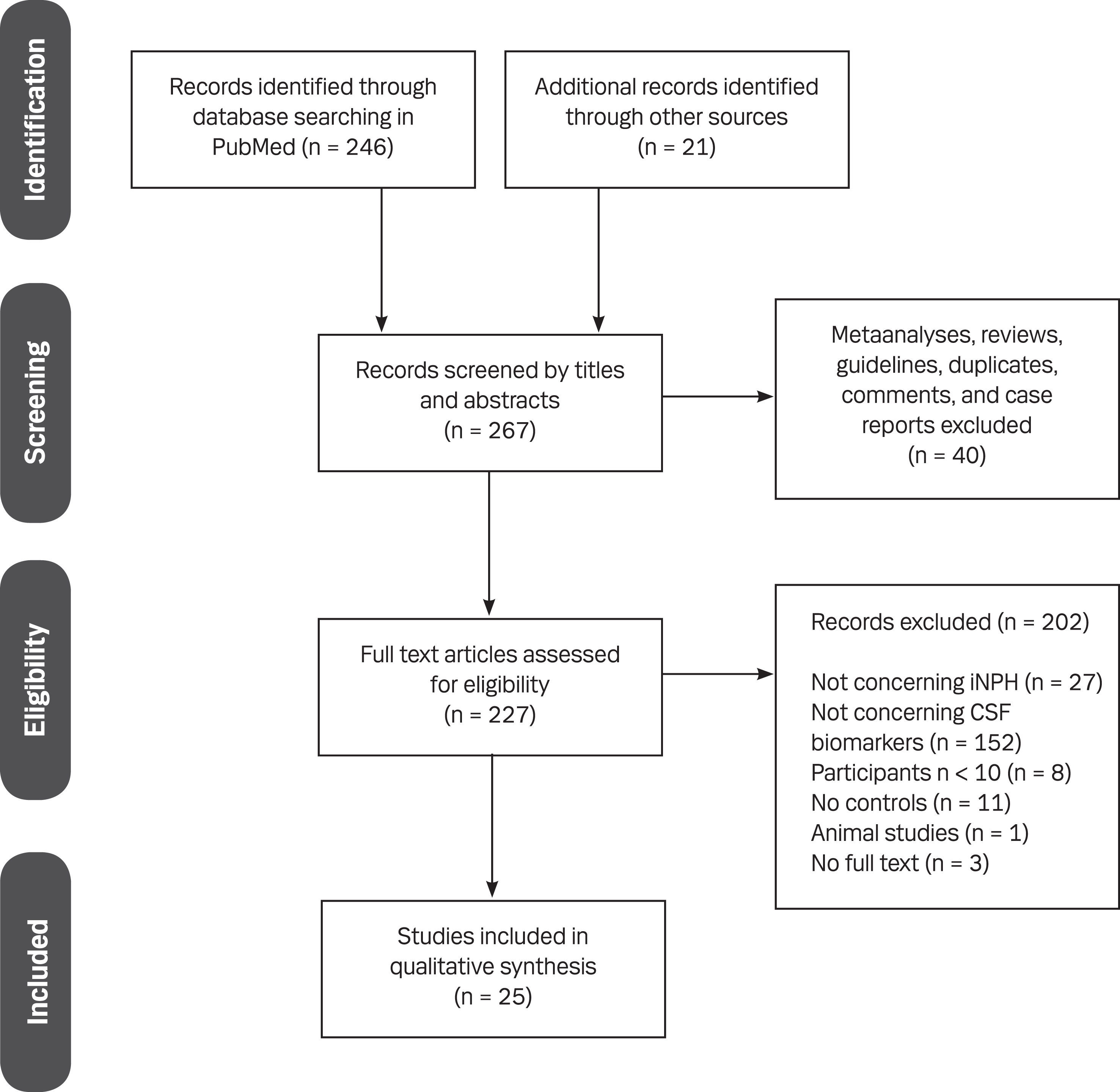
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram of the search strategy. The database search initially resulted in 246 publications in addition to 21 by hand search. Forty studies were excluded after screening of title and abstract, and 227 studies were assessed for eligibility, which resulted in a final inclusion of 25 studies.
Study characteristics
The 25 publications included 664 patients with iNPH, 502 with AD, 57 with SIVD, and 338 neurologically and/or somatically HC. Additionally, 81 patients with other disorders were also included denoted as “Other diagnoses” in Supplementary Tables 1 to 5. They had the following diagnoses: multi-infarct dementia [7], vascular dementia [8], multiple sclerosis, lymphoma, rheumatoid arthritis, epilepsy, amyotrophic lateral sclerosis, myelopathy, Graves’ disease, and transient global amnesia [9], patients without AD and where iNPH was refuted due to a negative CSF tap test or a negative shunt response [10], patients with mixed iNPH-AD or patients who suffered from unspecified diagnoses [11]. The included studies investigated a total of 92 CSF biomarkers. They could be categorized into five groups dependent on the pathology reflected by the individual biomarker: neurodegeneration [11 –14], demyelination [11 , 13–15], neuroinflammation [11–13 , 16], AD pathology [9 , 17–27], and other pathologies [7 , 28–31]. Most of the 92 biomarkers were investigated in comparison with HC (n = 68), while fewer were studied in comparison with patients with AD (n = 57), “Other diagnoses” (n = 30), and SIVD (n = 5). The biomarkers amyloid-β 1-42 (Aβ 42), total-tau (t-tau), and phosphorylated tau (p-tau) were associated with most evidence for their ability to differentiate iNPH from AD and HC subjects, since they were investigated in minimum three studies with consistent results (Table 1). Moderate evidence existed for 62 biomarkers, whereas 88 biomarkers only had limited evidence (Tables 2 and 3).
CSF biomarkers with most evidence for their ability to differentiate iNPH from a diagnostic group
iNPH, idiopathic normal pressure hydrocephalus; CSF, cerebrospinal fluid; Aβ 42, amyloid-β 1-42; t-tau, total-tau; p-tau, phosphorylated tau; AD, Alzheimer’s disease; HC, healthy controls.
CSF biomarkers with moderate evidence for their ability to differentiate iNPH from a diagnostic group
iNPH, idiopathic normal pressure hydrocephalus; CSF, cerebrospinal fluid; Aβ 42, amyloid-β 1-42; t-tau, total-tau; p-tau, phosphorylated tau; AD, Alzheimer’s disease; HC, healthy controls; SIVD, subcortical ischemic vascular disease; NFL, neurofilament light protein; MBP, myelin basic protein; IL, interleukin; INF, interferon; MCP, monocyte chemoattractant protein; TNF, tumor necrosis factor; sAβPP, soluble amyloid-β protein precursor; LRG, leucine-rich alpha-2-glycoprotein; DHEA, dehydroepiandrosterone. *The biomarker was investigated in two studies with consistent results.
CSF biomarkers with limited evidence for their ability to differentiate iNPH from a diagnostic group iNPH versus AD
iNPH, idiopathic normal pressure hydrocephalus; CSF, cerebrospinal fluid; Aβ 42, amyloid-β 1-42; t-tau, total-tau; p-tau, phosphorylated tau; AD, Alzheimer’s disease; HC, healthy controls; SIVD, subcortical ischemic vascular disease; MBP, myelin basic protein; IL, interleukin; INF, interferon; MCP, monocyte chemoattractant protein; TGF, transforming growth factor; TNF, tumor necrosis factor; sAβPP, soluble amyloid-β protein precursor; AChE, acetylcholinesterase; BuChE, butyrylcholinesterase; MHPG, 3-methoxy-4-hydroxyphenylglycol; YKL-40, chitinase-3-like protein 1; sCD40L, soluble CD40 ligand; APL1β, amyloid precursor-like protein 1 β. *The biomarker was investigated in two studies with inconsistent results.
Neurodegeneration
Four studies examined neurofilament light protein (NFL), a biomarker of axonal damage, in patients with iNPH (n = 158), AD (n = 16), “Other diagnoses” (n = 23), SIVD (n = 26), and HC (n = 63) [11 –14] (Supplementary Table 1).
There was moderate evidence for NFL in patients with iNPH in comparison with the four diagnostic groups: Two studies replicated increased levels of NFL in iNPH versus HC [13, 14], whereas one study with a smaller sample size did not find any difference between iNPH and HC [12]. Two larger studies did not find any difference in NFL between iNPH and AD, “Other diagnoses”, and SIVD [11, 14].
Demyelination
Myelin basic protein (MBP) and sulfatide are believed to signal ongoing demyelination. The biomarkers were studied in two studies each, including patients with iNPH (n = 159), AD (n = 16), “Other diagnoses” (n = 23), SIVD (n = 45), and HC (n = 43) [11 , 13–15] (Supplementary Table 2).
Similar levels of sulfatide in patients with iNPH and HC and similar levels of MBP in iNPH versus AD and “Other diagnoses” were associated with moderate evidence [11 , 13–15]. MBP in iNPH versus HC and sulfatide in iNPH versus SIVD yielded limited evidence [13 –15].
Neuroinflammation
A total of 24 biomarkers characteristic of neuroinflammation were studied in four studies including patients with iNPH (n = 116), AD (n = 16), “Other diagnoses” (n = 23), and HC (n = 60) [11–13 , 16] (Supplementary Table 3).
Most of the biomarkers (n = 22) were studied once in a large study, and thereby had moderate evidence [11]. The remaining biomarkers (n = 20) were studied once in small studies or studied twice with inconsistent results yielding limited evidence [12 , 16]. Besides increased levels of MCP-1, IL-1β, IL-6, and IL-10 in iNPH versus HC, all biomarkers were under detection limit or did not differ between patients with iNPH and the other diagnostic groups.
AD pathology
Fifteen studies investigated a total of nineteen biomarkers related to AD pathology [9 , 17–27]. The biomarker levels were investigated in patients with iNPH (n = 404) in comparison with patients with AD (n = 349), “Other diagnoses” (n = 26), SIVD (n = 38), and HC (n = 235) (Supplementary Table 4).
Aβ 42, t-tau, and p-tau were associated with most evidence for their ability to differentiate iNPH from other diagnostic groups. A total of nine studies investigated the levels of Aβ 42 in patients with iNPH versus AD, and seven studies, including 186 patients with iNPH and 298 with AD, found comparably low levels of Aβ 42 in iNPH and AD. The seven studies included three large studies [21, 23], one with unclear age distribution among patients with iNPH and AD [11], and four smaller studies with age-matched patients with AD [17 , 25]. The remaining two studies found increased Aβ 42 in iNPH versus AD [26, 27]. The mean biomarker value±one standard deviation in the two diagnostic groups overlapped in all nine studies.
In comparison with HC, Aβ 42 was abnormally lower in iNPH in eight studies, including 205 patients with iNPH and 205 HC subjects, out of nine studies. They included two large studies, which both failed to have age-matched HC subjects [14, 21], and six smaller studies [12 , 24] including two studies without equal age distribution among patients [25, 26]. The ninth study found no difference in Aβ 42 between iNPH and HC [27]. There was no overlap in mean biomarker value±one standard deviation or median, interquartile range (IQ) between the two diagnostic groups in six out of nine studies [19 , 26].
In contrast, the levels of t-tau and p-tau were lower in patients with iNPH than in patients with AD. T-tau was decreased in iNPH versus AD in seven studies, including 195 patients with iNPH and 305 with AD, out of nine studies. They included three large studies [21 –23] and four smaller studies with age-matched patients with AD [24 –27]. The two remaining studies reported no difference in t-tau between iNPH and AD [11, 17]. The mean biomarker value±one standard deviation or median, IQ of the two diagnostic groups did not overlap in five out of nine studies [22 –26].
The level of t-tau in iNPH did not differ from HC in four studies, including 85 patients with iNPH and 68 HC subjects, out of seven studies. The four studies included one large study and three small studies without equal age distribution among patients [20 , 24–26]. The three remaining studies found decreased [13, 14] and increased levels of t-tau in iNPH versus HC [24]. The mean biomarker value±one standard deviation or median, IQ of the two diagnostic groups overlapped in all seven studies.
Eight studies, including 211 patients with iNPH and 321 with AD, out of nine studies reported decreased levels of p-tau in iNPH versus AD. They included three large studies with age-matched patients with AD [21 –23] and five small studies [20 , 27], where all but one study had equal age distribution among the two patient groups [17]. The ninth study found no difference in p-tau between iNPH and AD [11]. The mean biomarker value±one standard deviation or median, IQ of the two diagnostic groups did not overlap in five out of nine studies [20 , 26].
No difference in levels of p-tau was found between patients with iNPH and HC in five studies, including 108 patients with iNPH and 140 HC subjects, out of seven studies. One study had a large sample size without age-matched subjects [21], which was also the case in two studies [26, 27] out of four small studies [20, 24]. The two remaining studies reported lower levels of p-tau in iNPH versus HC [13, 14]. The mean biomarker value±one standard deviation or median, IQ of the two diagnostic groups overlapped in all seven studies.
Among the remaining biomarkers, fourteen had moderate evidence, and twenty-one biomarkers showed limited evidence for their ability to differentiate iNPH from other diagnostic groups (Tables 2 and 3).
Other pathologies
The remaining biomarkers (n = 46) represented other pathologies than the ones described above. They were further subdivided into biomarkers characteristic of neurosteroid metabolism, neuroprotection, immunological reactions, neurotransmission, and others such as sodium and water homeostasis, prostaglandin, and brain metabolism (Supplementary Table 5).
The biomarkers were examined by ten studies, which included patients with iNPH (n = 265), AD (n = 173), “Other diagnoses” (n = 45), and HC (n = 95) [7 , 28–31].
No biomarkers characteristic of other pathologies were associated with the highest level of evidence. Thirty-one biomarkers had moderate evidence, which included leucine-rich alfa-2-glycoprotein (LRG) as the only biomarker that was studied twice with consistent results [29, 30] (Table 2). Here, LRG was increased in patients with iNPH compared to HC. The remaining fifteen biomarkers had limited evidence since they were only studied once in small studies (Table 3).
Risk of bias
Selection of study population
– Study design
All 25 studies were cross-sectional case-control studies and in eighteen of them, the data collection was performed retrospectively [8–12 , 28–31]. Selection bias is especially important to avoid, since recruitment often is carried out in Memory Clinics. Here, the enrollment of patients may be biased towards patients with more severely affected cognitive function and thus with possible neurodegenerative or vascular comorbidity. Only two studies reported blinding of laboratory staff [11, 21].
– Sample size
Seventeen of the included studies had small sample sizes (iNPH < 30), which may be due to the low prevalence of the disease [7–10 , 29–31]. The sample size ranged from 11 to 62 patients with iNPH, 10 to 165 patients with AD, 12 to 26 patients with SIVD, and 10 to 72 HC. The small sample sizes may have contributed to the number of insignificant results in the included studies.
– Age and sex
Not all studies were successful in recruiting diagnostic groups with equal age and sex distribution. Eleven studies had at least two diagnostic groups without age-matched subjects [8 , 30], whereas three studies lacked equal sex distribution [7 , 21]. In six studies, we were not able to evaluate the age and/or sex distribution of the diagnostic groups due to missing data [10 , 29].
In one study with age-matched diagnostic groups, the patients with iNPH and HC were characterized by a broad age range (44 to 70 years and 42 to 77 years, respectively) [31]. T-tau, p-tau, soluble amyloid-β protein precursor (sAβPP) and sAβPPβ showed correlation with age [17, 23], whereas no studies reported any effect of sex category on biomarker levels. This emphasizes the need for especially equivalent age distribution among the individuals to avoid biased results.
– Inclusion and exclusion criteria
To assess the population of patients with iNPH, we evaluated whether the following aspects were considered as part of the inclusion and exclusion criteria: Supplementary testing of patients under suspicion of iNPH, methods for assessing improvement after supplementary testing, surgery and choice of shunt system, and methods and timing for assessing post-surgery improvement.
Supplementary tests were done on patients with iNPH in eighteen studies, and most performed the tap test [8 , 27] or the tap test in combination with an infusion test [7 , 30]. Others conducted a lumbar drainage [16, 28], intracranial pressure (ICP) monitoring [11, 31], or an unspecified “CSF withdrawal” [25]. Five studies did not sufficiently describe if patients improved after the supplementary tests or had abnormal CSF dynamics [7 , 27], and only nine studies out of eighteen described how the effects of the intervention were assessed [7 , 31]. In one study, improvement after a CSF tap test was defined as 10 % increase of walking speed [22], others evaluated “walking, memory and fine skills in arms” [7]. Only two studies had similar outcome assessment (Tinetti gait test) of the supplementary tests [9, 21]. In twelve studies, not all patients were offered a shunt [19, 31], or it was unclear if the included patients had gone through a surgery [7–9 , 25–27]. A ventriculo-peritoneal (VP) shunt was inserted in most studies [10–13 , 28–30]. Two studies chose a lumboperitoneal shunt [20, 23], one inserted a VP shunt or an endoscopic third ventriculostomy [15], while five studies lacked information about their choice of shunt system [14 , 31]. Out of the thirteen studies, where all patients underwent surgery, only eight studies reported that all patients improved from shunt implantation [10 , 28–30]. The remaining five studies did not separate shunt-responders from non-responders in the statistical analyses [7 , 19].
There was limited consistency in the eight studies that reported the assessment method of surgical outcome. Two Swedish studies [12, 13] preferred the iNPH scale by Hellström et al. 2012 [32], two Japanese studies applied the modified Rankin Scale and iNPH Grading Scale [19, 23], while the remaining studies chose different assessment methods [10 , 28]. Three studies evaluated the shunt response 6 months after surgery [12 , 23], whereas four studies assessed the effects after 1–3 months [10 , 29], and one study between 3–6 months after surgery [14]. One study did not report when the outcome assessment was performed [19].
Regarding the selection of HC, only one study analyzed CSF from neurologically and somatically HC recruited from the general population [13]. The HC subjects in the remaining studies were recruited from hospitals. In seven studies, the choice of HC subjects was questionable. One study sampled their HC subjects from an Emergency Room, where a lumbar puncture was performed due to persistent headache to rule out meningeal syndrome [31]. The HC subjects of a recent study were suspected for iNPH but rejected after MRI and lumbar drainage [16]. Another recent study included individuals with subjective cognitive impairment without evidence of dementia [21]. Five studies did not sufficiently describe the HC subjects and/or how they were recruited [8 , 27]. The remaining studies included HC subjects who were referred to surgery due to a somatic disorder (e.g., hernia surgery) [7 , 24] or who suffered from other neurological diseases such as tension-type headache, incidental unrupted aneurysm, and chronic polyneuropathy [26 , 28–30].
Exclusion criteria for patients with iNPH were limited. Only one study excluded patients with severe back and spinal problems [14], one study considered alcohol and drug history as exclusion criteria [27], and six studies excluded patients with other dementia and/or brain diseases [7 , 27].
Out of the seventeen studies, which included HC subjects, five did not mention any exclusion criteria concerning dementia and/or other brain diseases [16 , 28], and only four studies required a somatic and neurological examination of the controls [8 , 31]. The general lack of inclusion and exclusion criteria limits the interpretation of the included studies’ results and may complicate future attempts of replication.
– Diagnostic criteria
Since iNPH is a disease without specific pathological findings, it has continuously been a challenge for researchers to define appropriate diagnostic criteria for their studies. Especially before the first evidence-based guidelines were published in 2004 in Japanese [33] and in 2005 in English [34], studies may have suffered from severe clinical heterogeneity. The second edition of the international Japanese guidelines was published in 2012 [35].
In this review, we assumed that studies published before 2007 (n = 6) were possibly initiated before the guidelines were established and therefore did not follow these recommendations [33, 34]. Overall, the guidelines of 2005 define probable iNPH by a history (e.g., insidious onset), brain imaging (e.g., ventricular enlargement), clinical (e.g., at least two triad symptoms), and physiological criteria (CSF opening pressure between 5–18 mmHg). Only two studies published before 2007 applied similar diagnostic criteria by requiring all three triad symptoms to be present, had similar imaging criteria and performed a tap test as a minimum [8, 30]. Three studies differed by only requiring one symptom to be present [7 , 31]. Another study only briefly stated “the diagnosis was based on clinical symptoms, the results of neuroimaging and improvement after CSF withdrawal” [24].
Out of the nineteen studies published in 2007 or after, only thirteen studies referred to the guidelines from 2004, 2005, or 2012 [10 , 29]. Seven studies applied the diagnostic criteria for probable or definite iNPH [10 , 29], whereas six studies referred to possible iNPH or did not specify further [12 , 27]. The six studies that did not apply the international guidelines included studies with no physiological criteria [14, 24], with only one symptom as the clinical criteria [11, 14], with no clinical criteria [16] or unspecified clinical criteria [28]. One study applied “modified Ishikawa (2004) criteria for iNPH plus elevated CSF cerebral aqueductal flow by MRI and gait improvement” after tap test [9].
Pre-analytical and analytical variables
– CSF sampling
All studies examined CSF samples collected from the lumbar space. Two studies also included ventricular samples [11, 13]. CSF biomarkers may have substantial diurnal variation [36]. Despite this, most studies (n = 15) did not report when the lumbar puncture was performed during the day; only seven studies described that the samples were collected in the morning [7 , 27]. Some studies had collected the samples prior to surgery [12 , 24], prior to a predictive test [7 , 28], or on the day of clinical evaluation [26].
The total CSF volume sampled was reported in only 10 out of 25 studies and ranged from 2 ml to 40 ml [7 , 31]. Earlier studies have analyzed the impact of CSF sample volume on the levels of Aβ 42, t-tau and p-tau and found little effect [37]. However, these analyses should be repeated for all other potential biomarkers.
In a recent study, the lumbar samples were either collected prior to a 24 h intraventricular ICP monitoring or 24–48 h after the procedure was initiated [11]. The authors did not consider the possibility of altered CSF biomarker levels due to the intracranial procedure. Another study collected the samples during a 5-day lumbar drainage [16].
Thirteen studies provided information regarding the type of containers used for sampling and storage [9 , 31]. Two studies only reported that “low protein binding tubes” were used [18, 19]. The choice of tubes is especially relevant in studies measuring Aβ peptides, since they tend to adhere to plastic tubes in contrast to polypropylene tubes [37]. The three studies that did use plastic tubes were not analyzing Aβ peptides [16 , 31]. Unfortunately, six studies measuring Aβ peptides lacked information about their choice of containers [11 , 25].
– Analytical methods
Most of the biomarkers in the included studies were measured using different immunoassays: ELISA [11–14 , 30], multiplex immunoassay [11–13 , 16], immunoblotting [9, 10], chromatography immunostaining [14, 15], immunonephrelometric assay [8], and radioimmunoassay [31]. Other methods were liquid-chromatography [7 , 28], photometric analysis [7, 9], and capillary electrophoresis-mass spectrometry [18]. All studies that yielded consistent results applied identical analytical method, except in studies investigating Aβ 42 in patients with iNPH versus HC. Here, two out of nine studies used multiplex immunoassays [12, 13] instead of ELISA [14 , 24–27] to measure the levels of Aβ 42.
To replicate earlier findings, it is essential to thoroughly describe the analytical procedure of the study. This was not done in 9 out of the 25 studies [8 , 30]. As mentioned earlier, only two studies reported that laboratory staff was blinded [11, 21].
In the evaluation of older studies, it is especially important to be aware of the assay sensitivity. A study from 1997 measured the cholecystokinin-8 (CCK-8) levels in patients with iNPH with a radioimmunoassay [31]. Out of sixteen patients, twelve had CCK-8 levels under the detection limit. The value of the detection limit was then assigned the twelve patients, when the statistical analyses were performed. Therefore, further interpretation of the CCK-8 levels should be done with caution. In a recent study, several biomarkers were under the lowest limit of detection [11]. Instead, they were graded as zero concentration in the statistical analyses.
DISCUSSION
In this systematic literature review, we summarized the existing literature on the diagnostic value of CSF biomarkers in iNPH. A total of 25 studies and 92 biomarkers were evaluated, where the majority focused on biomarkers related to AD pathology. Sixty-two biomarkers were associated with moderate evidence, whereas 88 biomarkers only had limited evidence. Aβ 42, p-tau, and t-tau were the only biomarkers that yielded consistent results in at least three studies and thereby had most evidence for their ability to differentiate between iNPH and the following diagnostic groups: Aβ 42 was lower in both patients with iNPH and AD compared to HC, whereas p-tau and t-tau were higher in patients with AD than in patients with iNPH and HC. These findings indicate that levels of t-tau and p-tau are within normal range in patients with iNPH and not abnormally increased as observed in patients with AD. More interestingly is the observation that Aβ 42 is lower in patients with iNPH compared with HC and overlaps the levels characteristic of AD.
A recent meta-analysis based on ten studies reported equally lower levels of Aβ 42 in iNPH versus HC and lower levels of t-tau and p-tau in iNPH versus AD [38]. On the contrary, they found slightly higher levels of Aβ 42 in iNPH versus AD and decreased levels of t-tau and p-tau in iNPH compared with HC. Four studies, that all reported results supporting our findings, were included in our review but not in the meta-analysis [12 , 25]. Two out of four studies were published after the meta-analysis was published [20, 21]. Taken together, Aβ 42 does not consistently separate iNPH and AD. Most likely, the discrepancies reflect bias in literature search. Despite the additional four studies, only three studies investigated Aβ 42 in iNPH versus AD [20 , 25] and HC [12 , 21], while less examined t-tau in iNPH versus HC [21], t-tau in iNPH versus AD [17, 23], p-tau in iNPH versus AD and HC [16, 17]. The four studies, except for one [17], had small sample sizes and distinct diagnostic criteria. Considering the remaining 88 biomarkers, only NFL was studied more than twice and was thereby eligible for a meta-analysis. Based on these observations, more studies are needed to strengthen the tendencies presented by this review through a novel meta-analysis.
CSF biomarkers specific for iNPH will be especially helpful in patients with atypical clinical presentations, i.e., in patients where cognitive dysfunction dominates or in patients with concomitant cerebrovascular disease burden. In patients with clinical symptoms, the potential ability of Aβ 42 to separate HC from iNPH and AD is of less importance. In contrast, t-tau and p-tau may provide an added diagnostic value in a clinical setting with their ability to differentiate between iNPH and AD.
Several hypotheses have been proposed to explain the reduced levels of Aβ 42 in iNPH. One theory is that the characteristic increase of solution in the brain of patients with iNPH has a diluting effect on CSF proteins. This has been rejected as no changes have been described in CSF albumin pre-and postoperatively or in inflammatory biomarkers in parallel to the increase of sAβPP-derived proteins [12]. Another possible explanation is a dual pathology in iNPH and AD. Brain biopsies of patients with iNPH have shown AD pathology in 22–75% of patients [39, 40], and 46% of shunt-responders developed a neurodegenerative disorder during a five-year follow-up [41]. The observation of reduced levels of Aβ 38, Aβ 40, Aβ 42, sAβPPα, and sAβPPβ in iNPH argues against this theory, since a general reduction of all these biomarkers is not seen in AD. Finally, others argue that a general reduction in the production of sAβPP in patients with iNPH is due to a decline in brain metabolism in the periventricular zone as seen in PET and MRI studies [42]. The increase of sAβPP-derived peptides after shunt implantation could be interpreted as a normalization of the periventricular metabolism. Also, the shunt insertion may generate a reduced tension on periventricular white matter leading to a normal clearance of extracellular fluid into the ventricular space. One may consider if the impaired CSF clearance can lead to an accumulation of Aβ plaques and thereby increase the risk of AD in patients with iNPH. Alternatively, the formation of Aβ plaques may be the primary cause of the reduced CSF clearance initiating a cascade of dilated ventricles, increased tension on periventricular space, and impaired brain metabolism.
P-tau signals neurofibrillary tangles in AD, whereas t-tau marks unspecific neurodegeneration associated with neuronal dysfunction and disease progression in AD [43]. Earlier studies argue that t-tau and p-tau in iNPH are lowered due to inadequate interstitial fluid drainage into the CSF caused by the hydrocephalus [38, 44]. Since we now find most evidence for levels of t-tau and p-tau within normal range in iNPH, the difference from AD may be explained by the consideration that iNPH is not a neurodegenerative disease. Though, the observation of increased NFL in iNPH versus HC in two out of three studies suggests that neurodegeneration in white matter regions may be a component of the pathological mechanisms of iNPH.
Unfortunately, this review has certain limitations and the findings should be interpreted with caution. The majority of the included studies had small sample sizes and diagnostic groups without appropriate age matching. Moreover, the nonrestrictive inclusion criteria of controls may have been a contributing factor including various CSF tap volume.
Most importantly, there was a large discrepancy in the diagnostic criteria regarding 1) the choice of supplementary testing and the following assessment of improvement, 2) whether to include patients who had undergone a shunt surgery or not, 3) how and when to examine patients’ improvements, and 4) whether shunt responders should be separated from non-responders in the statistical analyses.
The lack of consensus in clinical criteria, treatment, and outcome measurement in iNPH has led to reconsideration of iNPH as an entity [4]. Nevertheless, recent long-term follow-up studies indicate that shunt surgery is advantageous for patients with triad symptoms, since 40% show postoperative improvement and 60% report a better general health condition postoperatively [43, 44]. As described in the introduction, iNPH may be diagnosed by response to shunt surgery or tap test, although we and others consider this controversial [4]. When we compare studies using tap test or shunt response as inclusion criteria with studies using only clinical criteria, we find the same tendencies regarding Aβ 42, t-tau, and p-tau in iNPH as described above, although the level of evidence decreases due to a lower number of studies (data not shown). Despite this, we suggest that future studies should aim to have clearly defined clinical and paraclinical criteria in order to increase the diagnostic certainty in the included subjects.
CONCLUSION
In this review, we evaluated the existing literature on the diagnostic potential of CSF biomarkers in iNPH versus AD and SIVD. In conclusion, we found most evidence for low levels of p-tau and t-tau in iNPH versus AD equal to the level of HC and low levels of Aβ 42 in iNPH versus HC equal to the level of patients with AD. The diagnostic challenge in daily practice is to discriminate iNPH from differential diagnoses or comorbidities such as AD and SIVD. Therefore, we find t-tau and p-tau as the most useful biomarkers in a clinical setting by facilitating the separation of iNPH from AD. More investigations are needed to further explore the potential of the remaining biomarkers.
In contrast to neuroinflammation and demyelination, we found evidence indicating that AD pathology and the non-specific phenomena of white matter degeneration may contribute to the pathological processes of iNPH. Though, a specific pathology of iNPH is still unknown. Moreover, the review also reflects a huge inconsistency in studies on iNPH biomarkers. They were characterized by several plausible biases such as small sample sizes and inconsistent diagnostic criteria. Together, it may compromise the diagnostic power of the results. To overcome these limitations in future research, coordinated efforts must be applied in establishing a standardized protocol for diagnostic evaluation of CSF biomarkers in iNPH. A large-scale prospective study involving multiple centers should be initiated, where only patients with iNPH should be considered. Otherwise, data should be analyzed separately from secondary NPH. Diagnostic criteria should agree with the current international guidelines. The inclusion and exclusion criteria of the control groups should be strictly stated. A common accepted outcome scale should be applied during a postoperative follow-up period of minimum a year [47]. An agreement on the analytical method of choice is required to enable a more accurate comparison of measurements. Finally, the diagnostic sensitivity and specificity of the individual biomarker and in combination with other biomarkers should be provided. Together, it would be a great step toward an improvement of the diagnosis and differential diagnosis of iNPH.