
Abstract
Background:
Idiopathic normal pressure hydrocephalus (iNPH) remains a challenge to differentiate from subcortical ischemic vascular disease (SIVD). Despite major research efforts, the cerebrospinal fluid (CSF) biomarker profiles of the two diseases are still not known in detail.
Objective:
To determine if novel CSF biomarkers, neurofilament light (NFL) reflecting axonal damage, the synaptic protein neurogranin (NG), and the astroglial marker chitinase-3-like protein 1 (YKL-40), and the core Alzheimer’s disease (AD) biomarkers, amyloid-β 42 (Aβ42), total tau (t-tau), phosphorylated tau (p-tau), can differentiate iNPH from SIVD. Patients with AD and healthy controls (HC) were included for comparison purposes.
Methods:
Patients with iNPH (n = 28), SIVD (n = 30), AD (n = 57), and HC (n = 33) were retrospectively included from the Danish Dementia Biobank. All patients with iNPH had effect of shunt surgery with a follow-up period of 4 to 69 months. CSF biomarkers were measured using immunoassays.
Results:
Lower levels of NFL, NG, Aβ42, and t-tau were found in patients with iNPH versus SIVD, while YKL-40 and p-tau were similar in the two diseases. NFL and Aβ42 were the most reliable biomarkers to differentiate iNPH from SIVD with an area under the curve (AUC) on 0.82 and 0.80, respectively. Combining NFL with Aβ42, t-tau, and p-tau resulted in an AUC of 0.90, which was equivalent to the diagnostic accuracy of all six biomarkers combined.
Conclusion:
An addition of NFL to the CSF panel of Aβ42, t-tau, and p-tau may improve the differentiation of iNPH from SIVD.
INTRODUCTION
Idiopathic normal pressure hydrocephalus (iNPH) is one of the few potentially reversible causes of dementia. The characteristic symptom triad of gait disturbance, cognitive decline, and urinary incontinence is possibly explained by a disruption of the cerebrospinal fluid (CSF) dynamics. One theory is that impaired CSF absorption leads to a pathological flow of CSF into the periventricular white matter initiating a cascade of pathological processes such as edema, capillary microinfarctions, and potentially reversible neuronal degeneration [1, 2]. The ventricular system is enlarged and often surrounded by white matter lesions (WML) on magnetic resonance imaging (MRI) in patients with iNPH. The diagnostic workup can be challenging. Patients may present with symptoms and neuroimaging features that overlap with Alzheimer’s disease (AD) and subcortical ischemic vascular disease (SIVD) [3–5]; diseases which also commonly co-exist with iNPH [6]. The diagnostic process may be further complicated by the high prevalence of comorbidities among elderly, e.g., musculoskeletal conditions, lumbar spinal stenosis, and urinary problems [7]. The supplemental tests, such as the CSF infusion test or tap test, are associated with relatively low sensitivity and/or specificity and complication risk [8]. Consequently, the diagnostic criteria are ambiguous, and only a minority of patients suffering from iNPH receive the diagnosis and are offered a surgical CSF diversion [9]. Treatment is often delayed which may influence the postoperative clinical outcome [10, 11]. Therefore, new diagnostic tools are needed to improve diagnostic accuracy, which will possibly also lead to earlier diagnosis.
CSF biomarkers are obvious candidates for such diagnostic tools. Despite major research efforts, a CSF biomarker profile in iNPH has not yet been characterized [12]. A recent systematic review revealed that most research has been focused on the AD biomarkers amyloid-β42 (Aβ42), total tau (t-tau), and phosphorylated tau (p-tau) [13]. Here, most studies in iNPHshowed reduced concentrations of Aβ42 on a similar level to patients with AD. All amyloid-β-related proteins, e.g., amyloid peptides Aβ38 and Aβ40, are reduced in iNPH in contrast to AD [14, 15]. This indicates that different pathomechanisms, such as altered amyloid production due to periventricular hypometabolism or impaired clearance, may be involved in iNPH.
Data on tau proteins are more ambiguous with reports of mostly reduced or normal CSF levels of t-tau and p-tau in patients with iNPH [13, 16]. Therefore, major neurodegeneration or tau pathology in iNPH seems less convincing [17].
Instead, the damage towards subcortical areas initiated by impaired CSF circulation may hypothetically result in release of the protein neurofilament light polypeptide (NFL) that constitutes the cytoskeleton of subcortical axons. It is considered a promising non-disease-specific biomarker of axonal damage [18] and correlates with WML in disorders such as multiple sclerosis [19], iNPH [20], and stroke [21]. This is in line with the reports of higher levels of NFL in iNPH than in HC [14, 22] with the exception of two recent studies that failed to replicate the results [15, 16].
The role of synapse loss in iNPH pathophysiology is still unknown. Neurogranin (NG) is located in postsynaptic dendrites and is a promising biomarker of synapse dysfunction in AD. Increased levels of NG are found already in early stages of AD where it associates with the degree of amyloid and tau pathology [23, 24].
Despite some indications of neuroinflammatory activity in iNPH [16, 26], solid evidence is still warranted. Chitinase-3-like protein-1 (YKL-40) is suggested to be a marker of neuroinflammation in several diseases [21, 28] through possibly astrocytic activation in the acute phase of the neuroinflammatory response [29]. It has been proven valuable in separating cognitive normal individuals from patients with mild cognitive impairment and AD and predicting disease progression [30]. Only one study has investigated YKL-40 in iNPH with negative results [15].
Neurodegeneration and (sustained) neuroinflammation are hallmarks of SIVD [31]. In iNPH, degradation of the neuronal structure may only play a minor role in the pathology of the disease, since symptoms can be partly or completely reversed depending on timing of treatment. Based on the above, we hypothesized that low levels of Aβ42 indicating amyloid pathology and decreased levels of NFL and t-tau would characterize iNPH in comparison to SIVD as a result of less neuronal damage in iNPH. We expected normal levels of NG, YKL-40, and p-tau in both diseases due to an insignificant impact of synaptic loss, acute inflammation, and tangle pathology on the development of both diseases. This is the first study to examine differences in the CSF profile of the novel biomarkers of neurodegeneration (NFL and NG) and neuroinflammation (YKL-40) in patients with iNPH and SIVD. We aimed to evaluate the potential of NFL, NG, YKL-40, Aβ42, t-tau, and p-tau to differentiate iNPH from SIVD and thereby determine which of these CSF biomarkers would be the most promising for use in clinical diagnosis. Patients with AD and HC were included for comparison purposes.
METHODS
Study participants
CSF and data on a total of 148 patients including 28 patients with iNPH, 30 with SIVD, 57 with AD, and 33 neurologically HC were collected retrospectively from the Danish Dementia Biobank. Between 2009 and 2016, the patients had been referred to cognitive evaluation at Copenhagen Memory Clinic, Department of Neurology, University Hospital of Copenhagen, Rigshospitalet, and Regional Dementia Research Centre, Department of Neurology, Zealand University Hospital on suspicion of a cognitive disorder. HC were volunteers enrolled for research purposes. As a minimum, patients and controls underwent diagnostic investigations including medical history, clinical examination, ECG, routine blood analysis, cognitive testing (Mini-Mental State Examination (MMSE), Addenbrooke’s Cognitive Examination, supplemented with neuropsychological examination in patients with mild or unclear symptoms), lumbar puncture, and structural imaging (head CT/MRI). Also, depending on the patients’ symptoms, a PET-FDG functional imaging was performed. All participants gave their written consent to be included in the Danish Dementia Biobank for the purpose of future research. This study was in accord with the Helsinki Declaration of 1975 and approved by the Committee on Health Research Ethics of the Capital Region of Denmark.
Clinical classification
Patients were diagnosed with iNPH if they fulfilled the iNPH international guideline criteria for “probable iNPH” including gait disturbance, cognitive impairment, and/or urinary incontinence [4]. Every patient’s medical record was evaluated to ensure that they at least fulfilled the required two out of nine gait criteria based on the clinical examination [4].
Further, enlargement of the cerebral ventricles on diagnostic imaging, which could not be explained by general atrophy, was required. All patients went through a lumbar infusion test, except for one who underwent a CSF tap test due to technical issues. If the diagnosis was uncertain after the supplemental testing (n = 9), a tap-test, an ICP monitoring test, and/or a ventricular liquor dynamic test was performed to increase the diagnostic certainty. All iNPH patients underwent shunt surgery. Patients were not included if they had a known cause of NPH (secondary NPH) or responded less than “fair” according to the “Black Scale for assessment of shunt outcome” on shunt implantation [32, 33]. The follow-up period was 23 months in average with a span from 4 to 69 months depending on the need for shunt revisions.
Patients with SIVD were diagnosed according to the VASCOG-criteria [34]. The occurrence of WML and lacunar infarcts were observed on MRI on T2-weighted images and evaluated by two experienced neurologists using the Fazekas scale [35]. A score of minimum 2 was required for patients with SIVD to be included.
Diagnosis of AD were made according to the NIA-AA criteria [36]. There were no indications of hereditary AD among the patients.
The median disease duration for iNPH was two years (range = 1–15 years), for SIVD it was three years (range 0.5–14 years), for AD it was three years (range = 0.5–12 years) defined by the number of years between onset of symptoms and lumbar puncture.
The neurological HC did not have subjective or objective signs of cognitive disorder. Control participants with a Fazekas score above 1 or WML above the expected for their age were excluded. Moreover, individuals with any neurological, psychiatric, or physical disease potentially causing cognitive impairment were excluded.
CSF analyses
During the diagnostic examination, a CSF sample was obtained from the participant by puncture in the L3-L4 or L4-L5 intervertebral space. YKL-40 concentration was measured using a commercially available enzyme-linked immunosorbent assay (ELISA) (R&D Systems, Minneapolis, MN, USA). NG and NFL concentrations were determined using in-house ELISAs as previously described in detail [24, 37]. Commercially available INNOTEST ELISA kits were used to measure the levels of Aβ42, t-tau, and p-tau as described by the manufacturer (Fujirebio, Ghent, Belgium). In all four diagnostic groups, there was an unfortunate lack of data regarding values of Aβ42, t-tau, and p-tau (iNPH = 4, SIVD = 3, AD = 12, HC = 10).
Statistical analyses
Analysis of demographic, clinical, and neuroimaging data was carried out using Kruskal-Wallis test on interval and ordinal data whereas Chi-Square test or Fisher’s exact test were applied on categorical variables. Mann-Whitney U-test was used on the interval and ordinal variables for pairwise comparisons of the diagnostic groups, if significance initially was found. To test the association between biomarker concentrations and the diagnostic groups, linear models adjusted for age and sex were applied. Receiver operating characteristic (ROC) curves were made to evaluate the diagnostic power of the individual biomarker and in combination by Orthogonal Projections to Latent Discriminant Analysis (OPLS-DA). The Variable of Importance Projection (VIP) score was obtained to illustrate the relative contribution of the individual biomarker. The statistical analysis was carried out using IBM SPSS Statistics 25 and R (version 3.6.0, The R Project for Statistical Computing). The R package ropls was used for OPLS-DA analysis [38].
RESULTS
Demographics, clinical, and neuroimaging factors
This study included 28 patients with iNPH, 30 with SIVD, 57 with AD and 33 HC. The demographic, clinical, and neuroimaging data of the study participants are displayed in Table 1. There was no statistical difference in the sex distribution among the diagnostic groups. The HC group was significantly younger than the iNPH, SIVD, and AD group. Patients with SIVD and AD had significantly lower MMSE scores versus patients with iNPH and HC as expected. Evans Index separated iNPH from the other diagnostic groups. Clinical strokes, lacunar infarcts, hypercholesterolemia and Fazekas score were significantly more common or pronounced in patients with SIVD in comparison with patients with AD, iNPH, and HC.
Demographics, clinical, and paraclinical factors of study participants
Pairwise comparisons of interval and ordinal variables were assessed by Kruskal Wallis test and Mann-Whitney U-test. Categorical variables were assessed by Chi-Square test or Fisher’s exact test. f, female; m, male; SD, standard deviation; MMSE, Mini-Mental State Examination; TIA, transient ischemic attack. ap < 0.05 versus SIVD; bp < 0.05 versus AD; cp < 0.05 versus HC.
CSF biomarker concentration in the diagnostic groups
Patients with iNPH had lower levels of NFL, NG, Aβ42, and t-tau compared with patients with SIVD (Table 2, Fig. 1). No difference in YKL-40 and p-tau were seen between the two disorders. Low levels of NFL, NG, YKL-40, t-tau, p-tau separated iNPH from AD, while Aβ42 levels were similar in both diseases. In comparison to HC, patients with iNPH had decreased levels of NG, Aβ42, t-tau, and p-tau and similar levels of NFL and YKL-40.
CSF biomarker levels in the diagnostic groups
Data is shown as mean (SD). Units are pg/mL. YKL-40 in ng/ml. Mann-Whitney U test was used for analysis of data. NFL, neurofilament light polypeptide; NG, neurogranin; YKL-40, chitinase 3-like 1 protein; Aβ42, amyloid-β 42; T-tau, total tau; P-tau, phosphorylated tau; iNPH, idiopathic normal pressure hydrocephalus; SIVD, subcortical ischemic vascular disease; AD, Alzheimer’s disease; HC, healthy controls; ns., nonsignificant.
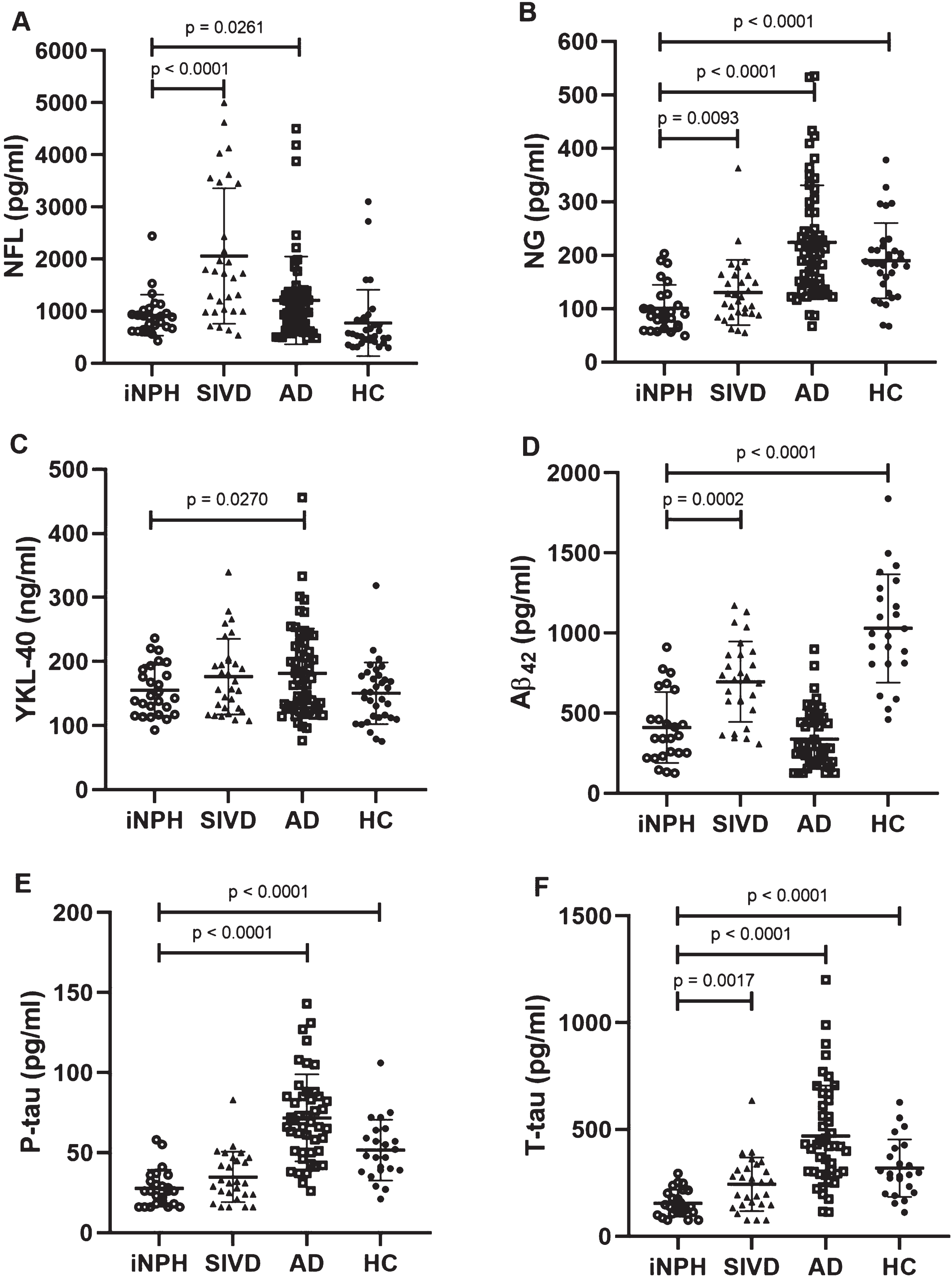
Scatter plots showing the CSF concentration distribution of all six biomarkers among patients with iNPH, SIVD, AD, and HC. Error bars represent median and interquartile range. A) NFL, B) NG, C) YKL-40, D) Aβ42, E) P-tau,9 F) T-tau. NFL, neurofilament light polypeptide; NG, neurogranin; YKL-40, chitinase 3-like 1 protein; Aβ42, amyloid-β 42; T-tau, total tau; P-tau, phosphorylated tau; iNPH, idiopathic normal pressure hydrocephalus; SIVD, subcortical ischemic vascular disease; AD, Alzheimer’s disease; HC, healthy controls.
ROC analysis revealed that Aβ42 and NFLwere the most reliable biomarkers to differentiate iNPH from SIVD with an area under the curve (AUC) on 0.80 and 0.82, respectively. In Fig. 2A, the diagnostic accuracy of the individual biomarkers is illustrated including the biomarkers combined (OPLS-DA) with an AUC of 0.90. Figure 2B displays the relative contribution of the individual markers by a VIPscore. An OPLS-DA model based on NFL in combination with the three AD core biomarkers without NG and YKL-40 had the same AUC (0.90) as the model with all six biomarkers included.

The diagnostic accuracy of the individual biomarkers and in combination for the differentiation between iNPH and SIVD. A) ROC curves of the CSF biomarkers suggest that NFL has most potential in differentiating iNPH from SIVD (AUC = 0.82), while YKL-40 has the least potential (AUC = 0.59). The diagnostic accuracy improves when combining all six biomarkers (OPLS-DA, AUC = 0.90). B) The VIP plot displays the relative contribution of each biomarker to the OPLS-DA model. Especially NFL and Aβ42 contribute to the differentiation of iNPH from SIVD. NFL, neurofilament light polypeptide; NG, neurogranin; YKL-40, chitinase 3-like 1 protein; Aβ42, amyloid-β 42; T-tau, total tau; P-tau, phosphorylated tau; AUC, area under the curve; iNPH, idiopathic normal pressure hydrocephalus; SIVD, subcortical ischemic vascular disease; AD, Alzheimer’s disease; HC, healthy controls; OPLS-DA, Orthogonal Projections to Latent Structures Discriminant Analysis; VIP, Variable Influence on Projection.
DISCUSSION
In this study, we found that NFL, NG, Aβ42, and t-taucould distinguish iNPH from SIVD by lower levels of all four biomarkers in iNPH versus SIVD. NFL and Aβ42 performed best in the differentiation of the two diseases. The biomarker levels in patients with AD and HC, who were included for comparison purposes, matched previous published levels [28, 40].
The higher level of NFL in patients with SIVD compared to patients with iNPH is in accordance with the general belief that axonal loss is a more dominant pathology in SIVD, which may explain the irreversibility of this disease in contrast to iNPH. A previous study reported no difference in NFL between iNPH and SIVD [22]. Here, the prevalence of several comorbidities was higher among patients with iNPH in general, compared to our selected iNPH-group. It is known that comorbid diseases such as cardiovascular disease are associated with WML [41]. Therefore, the lower NFL levels in our patients with iNPH versus SIVD may have been due to a lower Fazekas score. A recent systematic review and meta-analysis illustrated the distribution of CSF NFL in neurological conditions [42]. Here, a tendency towards slightly higher levels of NFL in large vessel dementia (VaD) compared with iNPH was observed. Though, it should be noticed that these data were based on only two studies including a total of 56 patients with iNPH and two studies including 491 patients with VaD with no distinction between SIVD and VaD. In contrast to our findings of increased levels of NFL in SIVD versus iNPH, two other studies reported equal levels of NFL in patients with iNPH and patients with VaD [16, 43]. In this subtype of vascular dementia, the subcortical regions may be less affected by axonal loss resulting in less leakage of NFL into the CSF in comparison with SIVD. Also, both shunt-responders and non-responders were included in the iNPH-group of the two studies, which may have resulted in higher NFL levels among these patients compared with our iNPH-group without non-responders [16, 43].
A high level of NFL is found in several neurodegenerative disorders such as frontotemporal dementia and progressive supranuclear palsy [44, 45] which indicates that NFL is not a disease-specific marker. Moreover, NFL is already considered a plausible prognostic marker of disease activity in multiple sclerosis [46] and a risk factor of mild cognitive impairment in a community population [47]. Since serum and CSF NFL correlates positively [48], serum NFL may be applicable as screening tool for neurodegenerative disorders in patients with cognitive impairment in primary care units. With this study, we show that NFL may also be valuable in memory clinics by improving the differential diagnosis of iNPHin combination with a CSF biomarker panel of Aβ42, t-tau, and p-tau. The highest and second highest level of NFL in our iNPH-group was 2,441 ng/L and 1,530 ng/L, respectively, with a 95% confidence interval of 922±160 (data not shown). Therefore, we suggest a cut-off value of NFL between 1,082 ng/L and 2,441 ng/L to distinguish between patients with iNPH and patients with SIVD, who have higher levels of NFL. However, more studies are needed to define a validated cut-off value.
No evidence for an inflammatory component as part of the pathophysiology of iNPH or SIVD was found, since YKL-40 did not differ between iNPH, SIVD, or HC. No other studies have investigated the difference in YKL-40 between patients with iNPH and SIVD, but others did report similar results in patients with iNPH versus HC and VaD versus HC, respectively [15, 49].
Despite our findings of decreased levels of NG in iNPH in comparison to SIVD, AD, and HC, synaptic degeneration may still contribute to the pathophysiology of iNPH. Several studies have reported a promising potential for NG as an AD-specific marker since increased levels are found in patients with AD [49–51]. Recently, reduced levels of NG have been found in other neurodegenerative disorders such as Parkinson’s disease (PD) suggesting a different pathomechanism from AD [52]. One study proposed that the reduced levels of NG in Parkinson’s disease reflect presynaptic pathology in the form of Aβ and α-synuclein dysmetabolism with a secondary effect on postsynaptic spines and consequently reduced synaptic activity [53]. In contrast, the increased levels in AD may result from loss of postsynaptic spine integrity and thereby synaptic degeneration. More studies are needed to clarify the pathophysiological mechanisms behind the reduced levels of NG in iNPH.
So far, only one study has investigated Aβ42 levels in iNPH and SIVD and failed to find any difference between iNPH and SIVD [54]. In our study, Aβ42 was one of the most reliable biomarkers to differentiate the two entities with a significantly lower level in iNPH versus SIVD. The discrepancies may be due to more strict diagnostic criteria of SIVD today than was the case when the previous study was published in 2004 [54]. As we have previously proposed, the low levels of Aβ42 may be caused by either a general reduction of brain metabolism in the periventricular areas or an accumulation of Aβ plaques as a cause or a consequence of impaired CSF clearance [13]. A plausible pathophysiological overlap between iNPH and AD is in line with previous reports of high levels of AD pathology in patients with iNPH, even in shunt-responsive patients [6]. As an alternative, the coexistence of AD in iNPH could partly be explained from an epidemiological point of view as an age-related disorder (AD) concomitant with a rare disorder (iNPH). More studies are needed to replicate the findings and clarify the circumstances of reduced Aβ42 in iNPH in comparison to SIVD.
T-tau and p-tau, markers of general neurodegeneration and tangle pathology, respectively, wereall within normal range in patients with iNPH and SIVD with significantly lower levels of t-tau in iNPH. This is in agreement with two other studies, though one reported significantly lower levels of t-tau and p-tau in iNPH versus SIVD, whereas one found no difference in t-tau between the two diseases [22, 54]. Despite levels within normal range, the findings may indicate greater neuronal damage in SIVD than in iNPH, which is also supported by the higher levels of NFL in SIVD versus iNPH, and no tangle pathology in any of the two diseases.
Limitations
Surprisingly, unexpectedly high levels of t-tau and p-tau were found in the HC group. We believe that this most likely indicates that some healthy individuals who volunteer for dementia research may have early signs of neurodegenerative processes that are not discovered by standard dementia evaluation. Moreover, levels of NFL did not significantly differ between patients with iNPH and HC subjects despite adjusting for the age difference between the two groups. Two other studies reported similar findings [15, 16] whereas others found increased levels in patients with iNPH versus HC [14, 22]. A recent meta-analysis reported a positive correlation between age and NFL in HC and in most neurodegenerative diseases [42]. Unfortunately, studies on this association in iNPH is limited [22].
As mentioned earlier, the possibility of comorbid AD or SIVD in the study participants or even misdiagnosis due to similar clinical and imaging features in iNPH, SIVD, and AD may have led to some degree of misdiagnosis. To address this aspect, neuropsychological examinations and/or PET-FDG scans were performed to improve the diagnostic certainty. Among our patients with iNPH, all patients had less than two positive AD biomarker (Aβ42, p-tau, t-tau) and only three patients had a Aβ42/p-tau ratiop <6.43 as cut-off value for AD applied by others (data not shown) [55]. In the SIVD-group, only one patient had at least two positive AD biomarkers and all presented with a normal Aβ42/p-tau ratio. Future studies may consider additional biopsy or postmortem verification of the final diagnosis or current comorbidities to overcome this issue.
The sample size for each diagnostic group was relatively small, which is reflected in rather large standard deviations for several of the biomarkers.
The retrospective nature of this study led to missing data such as neuroimaging data on some patients with AD due to less frequent use of MRI scans at the time of diagnosis. Also, data for CSF levels of Aβ42, t-tau, and p-tau was unavailable in 29 patients due to different clinical practices throughout the sampling period.
Disease duration as a clinical variable was not included in our statistical analyses since it did not differ between the diagnostic groups. Several studies have failed to find any correlation between disease duration and the six biomarkers investigated in this study [30, 57]. However, NFL has shown promising potential as a marker of disease severity in, for example, frontotemporal dementia, AD, multiple sclerosis, VaD, and amyotrophic lateral sclerosis [48, 58–60]. Due to the heterogenous pathophysiology and clinical manifestations of the diseases studied here, disease severity could not reliably be defined across all groups, but longitudinal studies of NFL in each group would be relevant future studies.
In this exploratory study, we conducted a two-center retrospective investigation on a highly selected group of patients who fulfilled the international diagnostic guidelines of iNPH and who had effect of shunt surgery with an average follow-up of 23 months. Hence, our choice of study cohort does not necessarily reflect the target population of patients with iNPH since many patients do not improve from surgery possibly due to prolonged disease duration and irreversible changes or comorbidities. In future studies, where knowledge about the pathophysiology and CSF biomarker characteristics of iNPH is greater, inclusion of a more heterogeneous study population of iNPH would be relevant.
Conclusion
In summary, our findings support the use of a panel of CSF biomarkers to differentiate iNPH from SIVD. Patients with iNPH showed a CSF pattern of lower levels of NFL, NG, Aβ42, and t-tau in comparison topatients with SIVD. NFL performed best in separating the two entities. A combination of NFL, Aβ42, p-tau, and t-tau differentiated iNPH from SIVD as efficiently as all six biomarkers combined. In clinical use an addition of NFL to the already widely used CSF panel of AD core biomarkers may improve the diagnostic accuracy of patients with iNPH and SIVD. Future studies are needed to validate this extended CSF panel in the diagnostic process of dementia disorders and to explore the potential pathophysiological role of subcortical neurodegeneration, amyloid pathology, and synaptic dysfunction in iNPH.
Footnotes
ACKNOWLEDGMENTS
This study was made possible due to financial support from The Family Hede Nielsen Foundation, The Lundbeck Foundation, “The Faculty of Health and Medical Sciences’ Fund for academically employed graduates and students at the University of Copenhagen”, and “Grocer Christian Andersen and wife Ingeborg Ovidia Signe Andersen, born Schmidt’s Scholarship”.
HZ is a Wallenberg Scholar supported by grants from the Swedish Research Council (#2018-02532), the European Research Council (#681712), and the Swedish state under the agreement between the Swedish government and the county councils, the ALF-agreement (#ALFGBG-720931). KB holds the Torsten Söderberg Professorship in Medicine at the Royal Swedish Academy of Sciences, and is supported by the Swedish Research Council (#2017-00915), the Swedish Alzheimer Foundation (#AF-742881), Hjärnfonden, Sweden (#FO2017-0243), and a grant (#ALFGBG-715986) from the Swedish state under the agreement between the Swedish government and the county councils, the ALF-agreement.