
Abstract
Background:
Hypertension is an established risk factor for dementia. However, it is unclear whether there are differential effects of angiotensin converting enzyme inhibitor (ACEi) or angiotensin receptor blockers (ARB) on brain health. In human observational studies, the evidence for superiority of either agent remains unclear.
Objective:
To compare brain atrophy and cognitive decline between people treated with ACEi or ARB.
Methods:
Participants aged 55–90 years without dementia had brain magnetic resonance imaging and neuropsychological assessments performed at 3 time points. The sample was enriched with people with type 2 diabetes (T2D). Multivariable mixed models were used to examine longitudinal associations of antihypertensive medication class with change in cognition and total brain volume.
Results:
Of 565 people with longitudinal data, there were 163 on ACEi (mean age 69.9 years, T2D:64% with) and 125 on ARB (mean age 69.6 years, T2D:62%) at baseline. The baseline characteristics of those taking either an ACEi or ARB were similar with regards to age, sex, blood pressure control, and vascular risk factors. The mean duration of follow up was 3.2 years. The baseline association of ACEi and ARB use with total brain volume was similar in both groups. However, those taking an ARB had a slower rate of brain atrophy than those taking an ACEi (p = 0.031). Neither ACEi nor ARB use was associated with baseline cognitive function or cognitive decline.
Conclusions:
These results support the theory that ARB may be preferable to ACEi to reduce brain atrophy. The mechanisms underlying this differential association warrant further investigation.
Keywords
INTRODUCTION
High blood pressure is an established risk factor for the development of dementia [1]. Results from human observational studies and secondary observations in clinical trials of populations with high cardiovascular morbidity generally favor a beneficial effect of antihypertensive medications (AHM) on reducing dementia risk [2] but are not conclusive [3]. These studies report a wide variation in the magnitude of treatment effect [2, 4]. One possible explanation for this may be that various classes of AHM have differential effects on brain health independent of their blood pressure lowering effect [2, 5].
The Renin Angiotensin System (RAS) has been implicated in the development of cognitive decline [4, 7]. Postmortem studies reported an association between angiotensin converting enzyme and Alzheimer’s disease almost 40 years ago [8, 9] and were further supported by angiotensin I-converting enzyme gene association studies at the end of the last century [10]. A recent literature review reported that six out of seven identified human cohort studies described a trend for Angiotensin Converting Enzyme Inhibitor (ACEi) agents to be associated with a reduced risk of cognitive decline or dementia [2]. In the same review [2], four out of eight studies reported that Angiotensin II Receptor Blockers (ARB) were associated with a reduced risk of cognitive decline or dementia. The results from animal studies suggest that the location of interruption of the RAS may be important in modifying dementia risk but this is yet to demonstrated in human studies [6]. Amyloid-β protein, important in dementia development, is degraded by ACE [11, 12]. It may be that ARBs, which block RAS but do not inhibit the potentially beneficial action of ACE, may be particularly advantageous [13]. Although results from basic science research seemed to support this theory, those from human studies remain inconclusive [2, 4] with recent observational studies reporting a larger beneficial effect of ARB use on the risk of dementia than ACEi [14–16]. A potential limitation of human studies to date is that many were designed to examine neurocognitive measures as only secondary outcomes within the context of large-scale trials of cardiovascular disease, and therefore lacked sensitive and detailed neuropsychological testing or volumetric imaging measures of brain structure. To address these limitations, a number of clinical trials, mainly recruiting people with established Alzheimer’s disease or mild cognitive impairment have commenced to better understand the role of AHM [6].
The aim of this study was to compare differences in brain atrophy and cognitive decline between people taking ACEi and ARB using data from a community-dwelling sample of older people enriched with type 2 diabetes (T2D), as RAS agents are more commonly used in T2D.
MATERIALS AND METHODS
Study population
The sample was derived from two prospective cohort studies conducted concurrently within the same source population in Southern Tasmania (postcodes 7000–7199). In the first cohort, the longitudinal population-based Tasmanian Study of Cognition and Gait (TASCOG), people ≥60 years were randomly selected from the Southern Tasmanian electoral roll between December 2004 and 2010 [17]. In the second cohort, the longitudinal Cognition and Diabetes in Older Tasmanians (CDOT), residents of Southern Tasmania with T2D aged ≥55 years were recruited from the National Diabetes Service Scheme between January 2008 and January 2010 [18]. The National Diabetes Service Scheme is a register of people with a confirmed diagnosis of T2D made by a physician using standard criteria (fasting plasma glucose ≥7.0 mmol/L, random plasma glucose ≥11.1 mmol/L, or 2 h glucose ≥11.1 mmol/L after oral glucose tolerance test). The same definition was applied to TASCOG participants to confirm or exclude T2D status. Exclusion criteria were identical for both studies— being resident in a nursing home, insufficient English for cognitive testing, or any contraindication to MRI scan. Both groups were followed up twice at approximately 2 and 4 years after baseline assessment. For this analysis, additional exclusion criteria included a history of dementia or Parkinson’s disease (determined by self-report using a standardized questionnaire) [19]. Ethics approval was obtained from the Southern Tasmanian Health and Medical Human Research Ethics Committee and the Monash University Human Research Ethics Committee approved the study and informed written consent was obtained from all participants.
Measurements
All study measurements used in this analysis were collected in both cohorts using the same techniques and tools.
BP and classification of AHM use
Systolic and diastolic blood pressures (BP) were measured by an Omron M4 sphygmomanometer and calculated as the mean of three consecutive seated brachial blood pressure measures from the right arm at each study review. Each participant’s medication use was recorded by a nurse who sighted medications in a face-to-face interview to obtain an accurate list of medications actually taken by the participant. These medication lists were manually reviewed and classified according to drug type. Participants were first classified as being on any AHM (yes/no) and then as being any RAS (yes/no). Participants using RAS agents were classified further as either being on an ACEi or ARB.
Cognitive function
A comprehensive battery of neuropsychological tests was used to measure cognition: (a) Verbal fluency using the Controlled Word Association Test (COWAT, using the letters F, A, and S; Category Fluency (animals) [20]; (b) Executive function-interference with the Victoria Stroop test— using the color minus word sub-tests [21]; (c) Working memory with the Digit Span subtest of the Wechsler Adult Intelligence Scale— Third Edition (WAIS-III) [22]; (d) Attention-processing speed using the Victoria Stroop Dot tests, Symbol Search and Digit Symbol Coding subtests of the WAIS-III [22]; (e) Visuospatial ability using the Rey Complex Figure copy task [20] (f) Verbal Memory using the Hopkins Verbal Learning Test-revised generating scores for total immediate recall, delayed recall, and recognition memory [20]; and (g) Visual memory with a delayed reproduction after 20 minutes of the Rey Complex Figure [20]. For each individual test, we standardized scores at each visit by creating z scores using the mean and SD from the baseline visit. These domain scores were also averaged to create a global cognitive score and the average scores for each of the 7 listed cognitive domains. Domain scores with more than one cognitive test were re-standardized to a SD of 1. Similar to previous work [19, 23–25], the re-standardized scores were used in the regression analysis to allow comparison of associations across cognitive domains.
MRI brain (total brain and lateral ventricular volume)
Brain MRI prior to January 2011 was performed using a 1.5-Tesla scanner (LX Horizon, General Electric, Milwaukee, WI) using the following sequences: high-resolution T1-weighted spoiled gradient echo (repetition time (TR) 35 ms, echo time (TE) 7 ms, flip angle 35°, field of view 240×240 mm; voxel size 1 mm3) comprising 120 contiguous slices; fluid-attenuated inversion recovery (FLAIR) (TR 8,802 ms, TE 130 ms, inversion time 2,200 ms; voxel size 0.50×0.50×3 mm). MRI after January 2011 was performed using a new 1.5-Tesla scanner (Syngo, Siemens, Erlangen, Germany) using the following sequences: high-resolution T1-weighted MPRAGE (TR = 1910 ms, TE = 3.14 ms, flip angle 15°, field of view 235×250 mm; voxel size 1 mm3) comprising 160 contiguous slices; FLAIR (TR = 8500 ms, TE = 92 ms, inversion time 2,438 ms; voxel size 0.9×0.9×3.5 mm).
T1-weighted and FLAIR scans for each patient were aligned using the co-registration facility of SPM12 (http://www.fil.ion.ucl.ac.uk/spm/). The FreeSurfer v5.3 longitudinal pipeline [26] was used to estimate total brain volume and intracranial volume. T2-weighted white matter hyperintensities (WMH) appear hypo-intense on T1-weighted scans and can be misclassified as gray-matter by FreeSurfer. Misclassifications were corrected using WMH masks generated from the co-registered FLAIR scans. Volume measures were calibrated between scanners by using a dataset of 11 participants imaged on both scanners. Two trained expert stroke physicians determined the presence of MRI infarcts and microbleeds at baseline. All image analyses were blinded to age, sex and cognitive outcome measures.
Covariates
Potential covariates included baseline age (centered to 55 years), sex, education (years), and self-reported history of ever-smoking, myocardial infarct, hypercholesterolemia, hypertension, and stroke. Additionally, we included T2D (as previously defined) and ApoE4 genotype derived from whole blood DNA.
Analysis
Demographic and clinical between-group differences were examined using t-tests and Chi squared tests. For longitudinal analyses, we used mixed models (mle, unstructured covariance) to examine the associations of baseline AHM use with change in MRI brain measures, global cognitive function, and the individual cognitive domains. Time since baseline measurement was the fixed effect and main effects were for AHM use and an interaction between AHM and time. Random effects for the intercept and slope were fitted for each individual, allowing participants to have different scores at baseline and rates of change in the dependent variable (MRI brain or cognitive measures). All models were adjusted for baseline age, sex, education, waist-hip ratio, T2D, ApoE4 carrier status (and intracranial volume for MRI measures). To examine whether the effect of AHM use was independent of BP, we further adjusted for baseline mean systolic and diastolic BP. Further exploratory analysis was subsequently performed for all classes of AHM and in those on AHM monotherapy with no AHM use as the reference group. Degrees of freedom (df) were calculated using the Kenward–Roger method [27]. Analysis was performed using STATA 15 (StataCorp LP College Station TX).
RESULTS
Of a baseline total sample of 711 participants, a further 4 participants with dementia and 2 participants with Parkinson’s disease were excluded leaving a total of 705 participants at baseline. Cognitive data were available for 700 people (>98% of European decent) at baseline, 504 at phase 2, and 431 at phase 3. Brain imaging data were available for 616 people at baseline, 388 at phase 2, and 298 at phase 3. Table 1 describes the characteristics of those who had at least 1 brain MRI available for analysis. Of these, 565 (80%) had at least one follow-up visit and contributed to further analyses. Within each of the drug use categories of no AHM, ACEi use, and ARB use, the characteristics of people with or without brain imaging at each time point was broadly similar (Table 2).
Sample characteristics at study entry
BP, blood pressure; AHM, antihypertensive medication; RAS, renin angiotensin system; ACEi, angiotensin converting enzyme inhibitor; ARB, angiotensin II receptor blocker; ApoE4, apolipoprotein E4 carrier; MRI, magnetic resonance imaging; WMH, white matter hyperintensity.
Characteristics of participants and drop outs at each time point
BP, blood pressure; AHM, antihypertensive medication; ACEi, angiotensin converting enzyme inhibitor; ARB, angiotensin II receptor blocker; ApoE4, apolipoprotein E4 carrier; T2D, type 2 diabetes.
Comparison of ACEi and ARB use
A total of 163 people were taking an ACEi and 125 were taking an ARB on study entry. A total of 11 people were taking both ACEi and ARB and were excluded from analysis. The baseline characteristics of those taking either an ACEi or ARB were similar with regards to age, sex, blood pressure control, and vascular risk factors and are described in detail in Table 1 and across time points in Table 2. Although those taking an ARB had lower baseline volume of WMH, and lower prevalence of brain infarct or microbleeds, these differences were not statistically significant (all p > 0.19). The baseline association of ACEi and ARB use with total brain volume was similar in both groups (p for difference = 0.99). However, adjusting for age, sex, T2D, education, blood pressure, waist-hip ratio, and ApoE4 status there was an interaction between type of RAS inhibitor and brain atrophy over time, whereby those taking an ARB had a slower brain atrophy than those taking an ACEi (interaction β= 2.06, df = 152, p = 0.031). The association of time (years) with brain volume was –6.7 (df = 167, p < 0.001). Figure 1 displays the interaction between RAS agent and total brain volume change over time in the above model. The addition of baseline WMH volume, presence of brain infarcts and microbleeds to the above model resulted in minimal change (interaction β= 2.03, p = 0.033). Neither ACEi nor ARB use were associated with baseline cognitive function or cognitive decline (Table 3). When stratified by diabetes status (i.e., repeating the analysis in the subgroup of people with T2D and then the subgroup of people without T2D), the above associations were no longer statistically significant (data not shown).
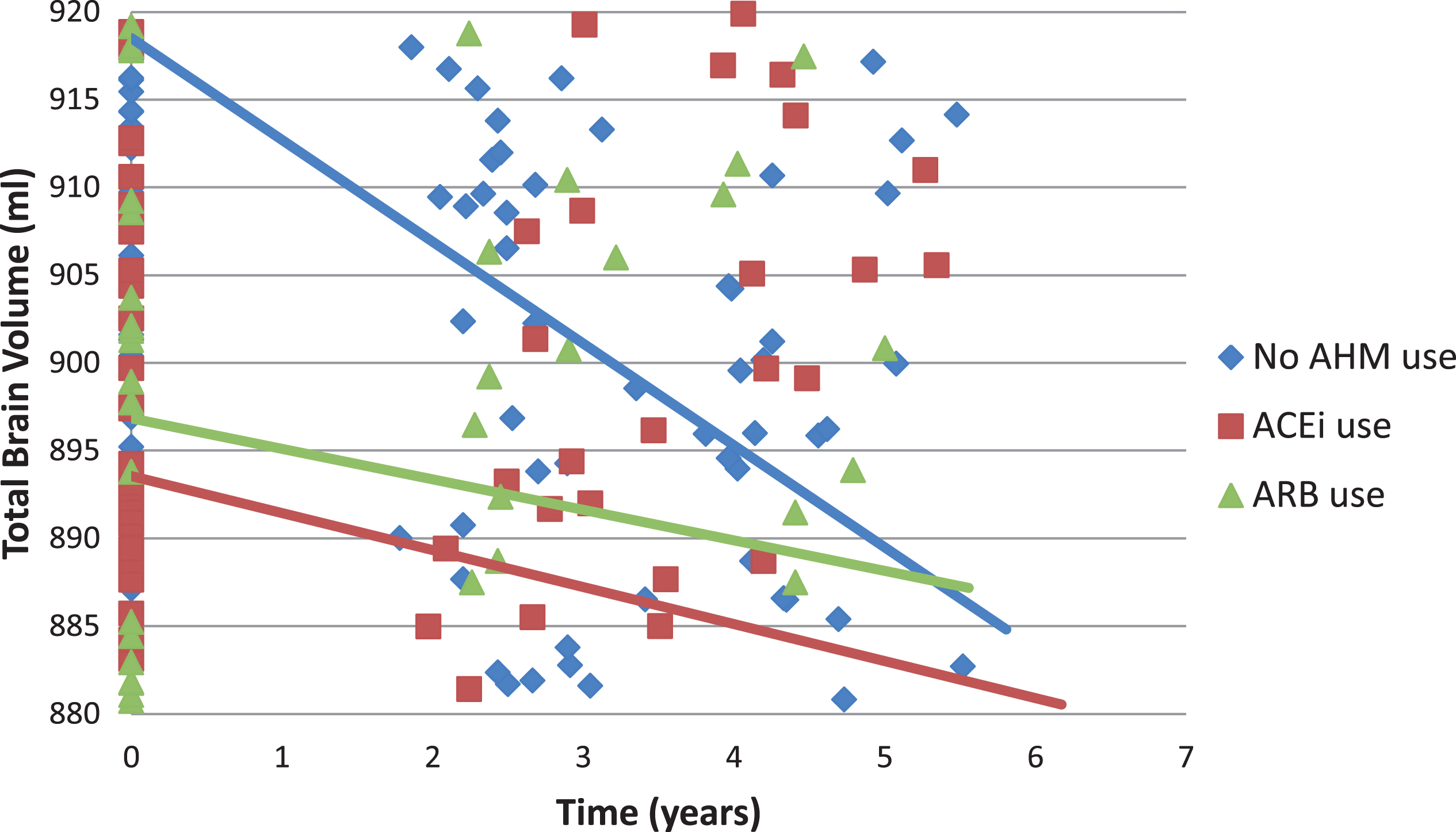
Associations between antihypertensive medication use and total brain volume over time. Adjusted for baseline age, sex, education, systolic blood pressure, diastolic blood pressure, history of hypertension, waist hip ratio, ApoE4 status, and total intracranial volume.
Associations between blood pressure agent use and cognitive function
Adjusted for baseline age, sex, education, systolic blood pressure, diastolic blood pressure, history of hypertension, waist hip ratio, ApoE4 status. ACEi, angiotensin converting enzyme inhibitor; ARB, angiotensin II receptor blocker; AHM, antihypertensive medication.
Exploratory comparisons of different monotherapies
Use of any blood pressure lowering agent
There were 368 people (mean age 70.2 years, SD 7.4) on at least one AHM and 198 not on any AHM (mean age 68.9 years, SD 7.3). The mean duration of follow up was 3.2 years. Compared with those not on AHM, and adjusted for age, sex, T2D, blood pressure, history of hypertension, ApoE4 status and BMI, people on AHM had lower total brain volume across all time points (β= –10.98, 95% CI –20.31 to –1.66, df = 541, p = 0.021). However, using this same model, there was no interaction between use of a blood pressure lowering agent and time on total brain volume (p = 0.31). Compared with those not on AHM, those taking at least one AHM had lower global (p = 0.03), processing speed (p = 0.008), and visuospatial function (p = 0.006) across all time points (Table 3). There was an interaction between AHM use and time on verbal fluency scores, whereby those on AHM had a greater rate of decline in verbal fluency than those not on AHM (β= –0.05, p = 0.007).
Monotherapy
Of those taking BP lowering medications, a total of 166 were taking a single medication (64 on ACEi, 45 on ARB, 24 on β-blocker, 18 on calcium channel blocker (CCB), and 15 on diuretic). On study entry, those taking an ACEi had lower total brain volume than people not taking any hypertensives (β= –12.7, 95% CI –24.12 to –1.33, df = 333, p = 0.029) but there were no other statistically significant differences in total brain volume when comparing other monotherapies with no AHM treatment adjusting for age, sex, T2D, blood pressure, history of hypertension, ApoE4 status, and BMI. There were no interactions between any of the BP lowering agents and time on brain volume (see Supplementary Figure 1). Supplementary Table 1 describes the associations of the different classes of AHM with the cognitive outcomes adjusting for baseline age, sex, education, systolic blood pressure, diastolic blood pressure, history of hypertension, waist hip ratio, and ApoE4 status. At baseline, those taking an ACEi had poorer performance in global (p = 0.02), executive (p = 0.04), and visuospatial function (p = 0.02), those taking an ARB had poorer visuospatial function (0.02), those taking an β-blocker had poorer global (p = 0.02), verbal (p = 0.04), and executive function (p = 0.004) and those taking a CCB had poorer processing speed (p = 0.006) visuospatial function (p = 0.02), and visual memory (p = 0.01) but better executive function (0.01) than those not taking AHM. Those taking CCB had a greater rate of decline in verbal memory (0.003) than those not on BP lowering agents or taking other AHM.
DISCUSSION
In this sample, enriched with people with T2D, we found those taking an agent targeting the RAS had slower rates of atrophy than those on neither/no AHM. We also found that the use of ARB agents was associated with slower rates of brain atrophy than those taking ACEi, independent of blood pressure control. The size of this association was small, and the clinical significance of this association remains unclear. These results suggest that ARBs may have a beneficial effect on brain atrophy by mechanisms other than their blood pressure lowering effect.
Similar to other studies [2], we report a possible beneficial effect of RAS inhibitors on brain ageing. Although there was a suggestion of beneficial effect of other AHMs, such as CCBs, we lacked the statistical power to have a high degree of confidence in these findings. Isolating the effects of other AHM is challenging in observational studies as many people require at least two agents to successfully control blood pressure, and recent guidelines recommend two first-line agents for the management of stage 2 hypertension [28]. As such, the ability to analyze people using monotherapy is limited. Similarly, we lack the statistical power to sub-analyze the specific ACEi or ARB agent used. Making these distinctions is important as there are variations in the ACE catalytic domains of specific ACEi that affect amyloid-β degradation [6] and potentially dementia risk. There are also within-class differences in blood-brain barrier permeability in ACEi [29] and, to some degree, ARB [30] that require more understanding and may have important implications for dementia risk [6]. Supporting this, one observational study of 414 people (mean age 75 years) taking ACEi noted centrally acting ACEi use was associated with less cognitive decline and a lower rate of progression to dementia than peripherally acting ACEi [31]. Another study, using the Alzheimer’s Disease Neuroimaging Initiative (ADNI) dataset, reported the use of centrally acting ACEi and ARBs was associated with better memory performance than all other groups [32].
Our finding that the use of any AHM and RAS inhibitors was associated with lower brain volume on study entry is likely related to the indication for AHM use. Such indications could include, but not be limited to, hypertension, T2D, and chronic kidney disease. Our sample was enriched with people with T2D who, as described in previous work in this sample were more likely to be prescribed an ACEi or ARB and have better blood pressure control [18]. A sample enriched with people with T2D has the advantage of likely including more people taking RAS inhibitors but may come with heightened risk factor identification and management in a person with known high risk of vascular complications, limiting generalizability. If the indication for AHM explains the differences in brain volume seen on study entry then it is likely that this indication bias is removed by the mixed longitudinal modelling, allowing the isolation of the beneficial effect of both ACEi and ARB. This would explain our finding of between-group differences at baseline but the absence of a subsequent association with greater rates of cognitive or structural brain decline.
To our knowledge, only one other study has examined the associations of RAS inhibition and longitudinal changes in brain volume [32]. This study used the ADNI dataset to compare 183 people with hypertension taking an ARB to people with hypertension taking any other AHM (n = 621) and those with normal blood pressure (n = 782). The authors found no between-group differences in brain volume change over three years but reported an association between centrally acting ACEi and ARB use and reduced WMH development in post hoc exploratory analysis. The between-agent differences we report may be the result of our sample having a larger burden of cerebrovascular disease and T2D than ADNI [32, 33] and a longer period of follow up with measurements at three time points providing additional statistical sensitivity to detect subtle changes. The benefits of including brain volume measures as an early marker of brain health are becoming increasingly recognized and are now beginning to be included as study outcome measures in AHM clinical trials [6, 34].
Although we report brain structural differences between groups, we did not find consistent cognitive differences. This lack of correlation between cognitive and brain structural measures may reflect the small effect size (∼30% of the size of the effect of time) that may not be large enough to result in detectable cognitive changes. Future studies, over longer time periods are required to understand the clinical significance of the associations we report.
Both vascular and neurodegenerative pathways have been implicated in explaining how ARB may have a beneficial effect on brain health. The specific targeting of ARB to Angiotensin II receptors (AT1 and possibly AT2) may result in greater vasodilation and improved cerebral blood flow than ACEi [35, 36]. Head-to-head studies comparing ACEi and ARB are lacking but results from animal models of stroke suggest that ARB may also have an anti-inflammatory action and neuroprotective role in humans [37, 38]. The results for a small number of studies suggest that ARB use is associated with lower AD pathology on autopsy [39] possibly via a beneficial effect on brain tau concentrations [40]. Supporting these observations, the ACE-sparing effect of ARBs may help preserve the proteolytic action of ACE on amyloid-β [11]. Future studies are required to confirm our findings taking advantage of advances in dementia biomarker development such as in vivo neuroimaging of amyloid and tau as well as serum and cerebrospinal fluid analysis to better understand the mechanisms through which ARB may be beneficial.
This study has a number of limitations. We followed people for a relatively short period of time and it may be that larger signals would be identified in cognition and brain structure over a longer period of time. We examined AHM use on study entry only and not for changes in medication use over time. Data regarding duration of exposure to AHM was unavailable in this study. As such we are unable to improve confidence in our results by exploring whether the duration of AHM use was associated with the size of the cognitive and structural associations we describe. Furthermore, the absence of this data prevents modelling of changes in AHM classes that commonly occur during an individual’s clinical management of hypertension. Clinical drug trials described in the review by Kehoe et al. [6] are actively recruiting participants that will collect this data. Similar to other longitudinal studies, a proportion were lost to follow-up. Our analytical techniques allowed us to reduce the impact of different follow up periods for participants but does not completely eliminate this potential source of bias. Due to an unavoidable change in MRI scanner during our study period, we were unable to measure whether changes in WMH volume play a mediating or modifying role. Future studies, in cohorts with a larger burden of cerebrovascular disease may be able to further examine whether ARB have beneficial effects and explore if this is via more traditional cerebrovascular pathways. A further limitation associated with MRI scanner change was the loss of an ability to examine the regional distribution of brain volume loss. It would be of interest if the regions of volume loss were consistent with the greater ACE activity seen in the medial hippocampal, parahippocampal, and temporal region in postmortem studies of people with Alzheimer’s disease [8, 9]. Strengths of our study include the careful collection and classification of AHM use based on direct interview and use of a broad battery of neurocognitive tests and detailed serial brain MRIs allowing great sensitivity to detect subtle changes.
In summary, those taking agents targeting RAS appear to have reduced volume loss compared to those not taking an AHM. ARB use may be associated with slower rates of brain atrophy than ACEi. There was no association between individual RAS inhibitor use and cognitive decline. The effect sizes we report are small, of uncertain clinical significance and may only manifest over long time periods.
Footnotes
ACKNOWLEDGMENTS
Dr. Moran is a recipient of an NMRC-ARC Dementia Research Development Fellowship. Dr. Beare is a recipient of NHMRC project grants. Dr. Callisaya is a recipient of an Alzheimer’s Australia Research Foundation Grant & NHMRC Early Career Fellowship. Dr. Srikanth is a recipient of a NHMRC Practitioner Fellowship.