
Abstract
Background:
There is only limited information available about the effect of age on course of cognitive decline in patients with onset of Alzheimer’s disease (AD) over the age of 64 years.
Objective:
We compared the rate of, and factors affecting, cognitive decline in patients with AD aged < 65 years (young-onset AD), 65–74 years (middle-onset AD), and ≥75 years (late-onset AD).
Method:
The study used longitudinal data from the Essex Memory Clinic which included a total of 305 participants; 56 had YOAD, 73 had MOAD, and 176 had LOAD. The rate of cognitive decline was measured using scores from the Mini-Mental State Examination (MMSE), and the data were examined using multilevel models analysis.
Results:
There was evidence of a difference in cognitive decline across the age groups with the YOAD group declining 2.8 MMSE points per year, those with MOAD declined 2.0 MMSE points per year, and the LOAD group declined 1.4 MMSE points per year.
Conclusions:
Patients with LOAD have a better prognosis than YOAD and MOAD. However, even between the MOAD and LOAD groups, age is a significant predictor of cognitive decline, with older patients having a more benign course.
INTRODUCTION
Alzheimer’s disease (AD) is conventionally defined as young- and late-onset AD (YOAD, LOAD) equating to age at onset <65 years and ≥65 years, respectively. There is an abundance of literature looking at the relationship between age, both as a continuum and dichotomized, with the progression of cognitive impairment in AD. The majority of studies found a faster rate of cognitive decline in younger patients when looking either at age at which a diagnosis of AD is ascertained [1–12], or the age of onset, that is when symptoms first begin [13, 14]. Some found no association between age of onset or diagnosis and rate of decline [15–20]. However, few studies have examined the effect of age on rate of decline within the LOAD group. As the prevalence of AD is increasing, and the UK population continues to age with a large AD cohort now aged over 65 years [21] there is a greater need for an understanding of the speed of decline of the disease and how age may affect this.
In this study, we looked at the age at which a diagnosis of AD was given and the rate of cognitive decline. Age at diagnosis is considered to be more reliable than age at onset which is dependent on patients/family members’ historical accounts and therefore subject to bias. The age at which a diagnosis of AD was given was split into <65 years and >65 years in line with the diagnostic classification of AD into YOAD and LOAD, respectively. We further stratified the over 65s in order to assess whether there was an effect of age on decline even within the over 65s. The LOAD group was subdivided into 65–74 years and ≥75 years. The 65–74 years old age group were defined as middle-onset AD (MOAD) and the ≥75 years old group were defined as late-onset AD (LOAD). The aim was to compare the rate of cognitive decline in patients with YOAD, MOAD, and LOAD. We also sought to identify any additional factors that may influence the rate of decline including sex, years in education and vascular risk factors.
METHODS
Participants
Patients were identified through the Essex Memory Clinic (EMC), a specialized memory assessment service that provides a detailed assessment of patients presenting with cognitive problems over the age of 40 following referrals from general practitioners (GP) and allied health professionals. The results of the assessments are stored on the memory clinic’s database following patient consent. If the outcome of an assessment reveals a diagnosis of dementia, then patients are usually discharged from the EMC and subsequently followed up and reviewed locally by their respective Older Adult Mental Health team. Patients were given a consensus diagnosis following discussion between two consultant old age psychiatrists, a clinical psychologist, and a memory clinic nurse. Between March 1993 and July 2015, 1.827 patients were assessed (see Fig. 1). Of those, 612 had a diagnosis of AD at their most recent clinic visit. The inclusion criteria were patients aged 40 years or greater; meeting diagnostic criteria for possible or probable AD at their most recent visit [22]; and at least 12 months follow up with repeated Mini-Mental State Examination (MMSE) score [23] following the diagnosis of dementia. Patients were excluded if they had history of severe mental illness or substance misuse, or a change of diagnosis following discharge. Three hundred and five patients were included in the final analysis (YOAD n = 56; MOAD n = 73; LOAD n = 176).
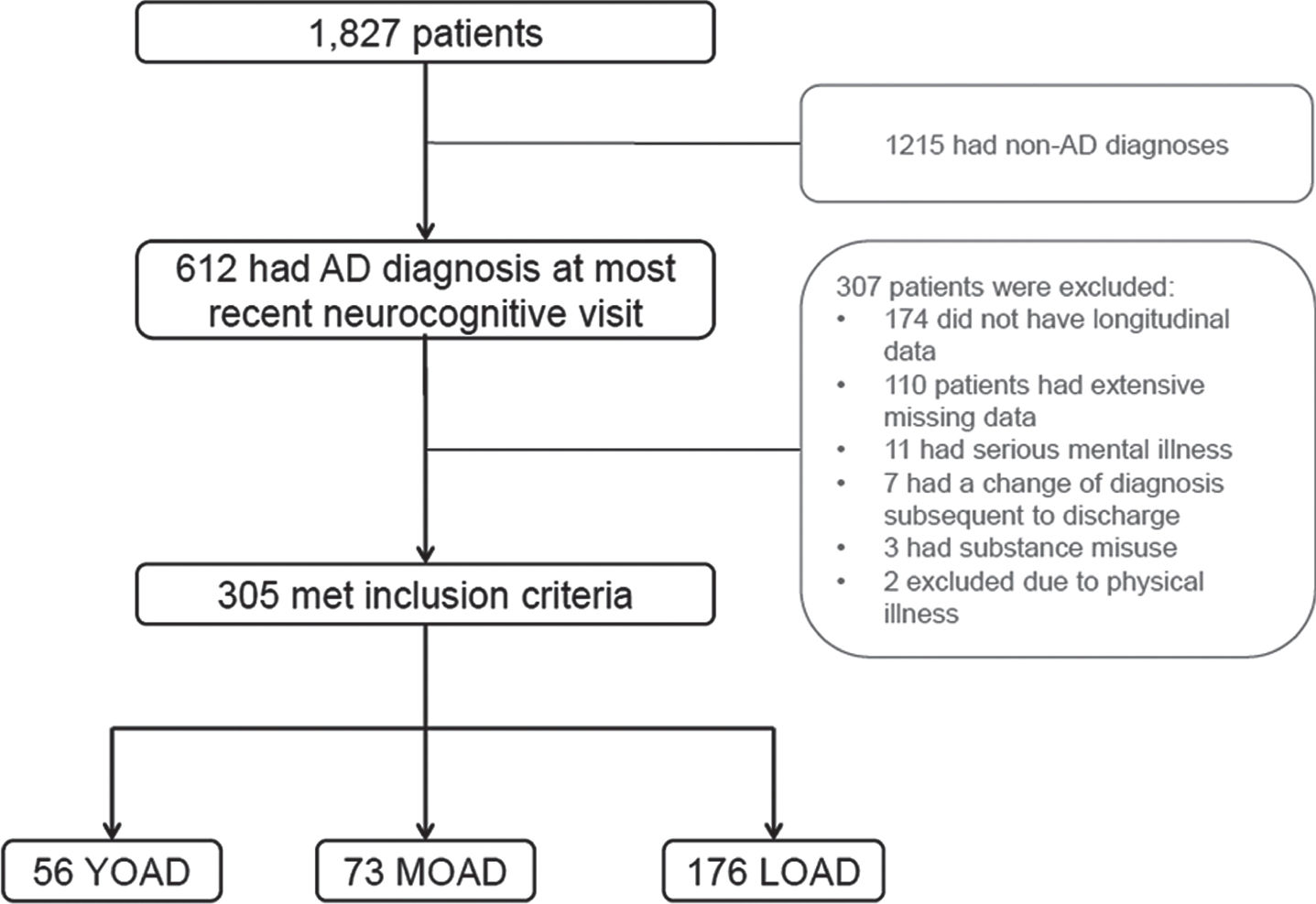
Study flowchart.
Procedure
For each eligible patient demographic data, smoking (current and ex combined into one value versus never smoked), drinking habits, and vascular risk factors including history of myocardial infarction, hypertension, hypercholesteremia, diabetes, and the Hachinski Ischemic Score (HIS) were recorded [24]. We considered baseline MMSE score to be the score obtained at the time of AD diagnosis. Follow-up MMSE scores were taken at subsequent routine clinical assessments. The data were then transferred into SPSS (version 19) for analysis.
Statistical analysis
For baseline group comparisons, Mann-Whitney, χ2 tests, and independent t-tests were used where appropriate depending on the variable and distribution type. In view of the hierarchical structure of our longitudinal data, i.e., repeated measures of MMSE scores for each individual, a multilevel models analysis approach was adopted. This approach improves statistical power, as it accounts for within-person correlations over time, allows different numbers of assessments, can be used with datasets with missing data, and allows for varying time intervals between assessments [25].
Multilevel models were used to assess associations between age at diagnosis and the rate of cognitive decline as measured by the MMSE. All assessments, including baseline, were taken into account. A random intercept and random slope were used for the analysis. The intercept represented the initial MMSE score, and the slope represented the rate of change in MMSE scores across time. The first model included terms for age at diagnosis; time; sex; years of education and the interactions between age at diagnosis and time; sex and time; and years of education and time, with the MMSE score as the dependent variable. Any non-significant covariates were then removed from the model, and the variables smoking, alcohol use, and vascular risk factors were added to see if there was an association between them and initial MMSE status and/or rate of decline. In the final model reported here, only variables with a significant association with initial MMSE status and/or rate of decline were retained. From this model, the baseline MMSE and annual change in MMSE for patients with different age at diagnosis could be calculated.
The continuous variable education was centered (mean subtracted from individuals’ scores) before the analysis. Age was trichotomized (<65 years, 65 to 74 years, and >74 years). All analyses were conducted using SPSS version 21, with the significance level set at 0.05.
Ethics
The relevant Local Research Ethics Committee (NRES Committee South West – Cornwall and Plymouth and Exeter) gave ethical approval for the study.
RESULTS
Study demographics
Fifty-six (18%) patients had YOAD, 73 (24%) had MOAD, and 176 (58%) had LOAD (see Tables 1 and 2). The mean age at diagnosis of persons with YOAD was 59.7 years (range 48 to 64) and of MOAD 71.1 years (range 65 to 74). LOAD comprised a larger sample size of 176, mean age 80.2 years (range 75 to 92). There was no evidence of a difference in sex distribution between the three groups. Those with YOAD had an increased number of years in education compared to those with MOAD and LOAD (p < 0.01). There was no evidence of a difference between the duration of symptoms prior to diagnosis in the three groups. However, the first symptom of YOAD patients was more likely to be changes in mood such as anxiety and/or depression. There was also no evidence of a difference to our findings after adjusting for length of symptoms. The baseline severity [(as measured using the MMSE and Cambridge Cognition Examination (CAMCOG)] of patients with YOAD was worse compared to those with MOAD and LOAD (p < 0.001). There was no difference in baseline severity between the MOAD and LOAD groups. The MOAD group had a greater number of follow ups compared to YOAD (p < 0.01). Of the possible covariates affecting cognitive decline the MOAD and LOAD groups had a higher rate of hypertension (p < 0.01); there were no differences in the other vascular measures, or smoking and alcohol habits. Fewer individuals with LOAD were taking the anti-dementia drug memantine in addition to their cholinesterase inhibitor (p < 0.01).
Baseline demographics and clinical characteristics between individuals with young-onset (YOAD, <65 years), middle-onset (MOAD, 65–74 years), and late-onset (LOAD, >75 years) Alzheimer’s disease
Pairs of letters a and b indicate pairs that differ at p < 0.05. 3-way continuous tests are Kruskal-Wallis, 2-way continuous tests are Mann-Whitney. Sex variable p-value from Chi-Square test. First symptom variable p-value from Fisher’s exact test. MMSE, Mini-Mental State Examination; CAMCOG, Cambridge Cognition Examination.
Clinical characteristics (percent yes)
Pairs of letters a and b indicate pairs that differ at p < 0.05. All comparisons are χ2. YOAD, young-onset Alzheimer’s disease; MOAD, middle-onset AD; LOAD, late-onset AD; MI, myocardial infarction; AChEI, acetylcholinesterase inhibitor.
Findings from the analysis
The initial model included terms for age at diagnosis; time; sex; years of education and the interactions between age at diagnosis and time; sex and time; and years of education and time, with the MMSE score as the dependent variable. All covariates were significant at p < 0.05 with the exception of the interactions between time and years of education, and time and sex. The non-significant terms were dropped from the model and the following parameter estimates were obtained: for a patient with YOAD of average education and female sex, the initial MMSE status was 19.4 points. At baseline the MOAD group had an MMSE score 4.8 points higher (p < 0.01); individuals with LOAD had an MMSE score that was 3.9 points higher (p < 0.01 versus YOAD); male sex was associated with an increase of 1.1 MMSE points (p < 0.05); and each extra year of education was associated with an increase of 0.3 MMSE points (p < 0.05). Regarding rate of change, YOAD patients declined by 0.23 MMSE points per month. Those with MOAD declined by 0.17 MMSE points per month (p < 0.05), and those with LOAD declined by 0.11 MMSE points per month (p < 0.01). Using estimated regression lines of MMSE score by time, the rate of decline in patients with YOAD was 2.7 MMSE points per year. At 48 months (in a prototypical YOAD patient with an initial MMSE of 19.4), the estimated MMSE score is 8.5. Patients with MOAD declined 2.0 points per year. At 48 months (in a prototypical MOAD patient with an initial MMSE of 24.3), the estimated MMSE score is 16.3. Patients with LOAD declined 1.3 points per year. At 48 months (in a prototypical LOAD patient with an initial MMSE of 23.4), the estimated MMSE score is 18.1.
To the initial model, the variables smoking, alcohol use, and vascular risk factors were added to see if there was an association between them and initial MMSE status and/or rate of decline. Only diabetic status was significantly associated with initial MMSE status and no variables were associated with rate of decline. In the final model, all non-significant covariates were dropped. In the final model, the initial MMSE score of diabetic patients was 1.7 points higher (p < 0.05) than non-diabetic patients. All other parameter estimates were essentially unchanged from the initial model, including no change to the level of statistical significance.
To supplement the analyses above, we directly compared initial MMSE status and rates of decline based on the final model for MOAD versus LOAD. In this model, the following parameter estimates were obtained: for a patient with MOAD of average education, female sex, and non-diabetic status the initial MMSE status was 24.0 points. At baseline the LOAD group had an MMSE score 0.8 points lower (p = 0.14). Regarding rate of change, MOAD patients declined by 0.17 MMSE points per month. Those with LOAD declined by 0.11 MMSE points per month (p < 0.01; (see Fig. 2).

Initial MMSE status (top) and rates of decline (bottom) for YOAD, MOAD, and LOAD.
Of the 305 cases studied, 54 only had 2 assessment time points. The results of patients with only 2 time points could be perceived as being less reliable. We therefore conducted a sensitivity analysis excluding cases with only 2 scores. The repeated analyses gave broadly similar results. However, additional years of education and diabetes were no longer associated with higher initial MMSE status. The rate of decline of early-onset cases decreased (from –0.23 to –0.20 MMSE points per month). This was still significantly different from zero. This slight reduction in rate of decline meant that there was no longer a significant difference in rate of decline between early- and middle-onset cases. However, there continued to be significant differences in rate of decline between early- and late-onset cases, and middle-onset and late-onset cases.
DISCUSSION
Summary of main findings
Patients with YOAD had a baseline MMSE score of 19.3. Patients with MOAD had a higher baseline MMSE score of 24.0, whereas those with LOAD had a score of 23.2 It, therefore, did not follow a consistent trend that older patients presented with higher MMSE scores at baseline.
In terms of rate of decline from the time of diagnosis, individuals with YOAD declined 0.23 MMSE points per month, those with MOAD declined 0.17 MMSE points per month, and those with LOAD declined 0.11 MMSE points per month. This equates to the YOAD individuals declining by 2.7 MMSE points per year, those aged 65 to 74 declining by 2.0 points per year, and individuals with AD aged 75 and over declining by 1.3 points per year.
The difference in baseline severity between those with YOAD and MOAD/LOAD may have accounted for a faster rate of decline in the YOAD group. Arguing against this, baseline severity was similar between those with MOAD and LOAD and yet the MOAD group declined faster than the LOAD group.
Findings in the context of other literature
The baseline MMSE for those with YOAD was significantly lower and the rate of decline faster compared to those with MOAD and LOAD. Accurate diagnosis of YOAD is challenging, particularly in the early stages, and as a consequence these patients tend to present late to memory services. Accordingly, they are more cognitively impaired at time of diagnosis, and as a result start antidementia therapy later than individuals with MOAD/LOAD. Yet interestingly in this sample patients with YOAD did not have a longer length of symptoms compared to those with LOAD.
It could be argued that worse baseline severity of patients with YOAD accounts for their faster decline in the present sample. A systematic review looking at predictors of rate of decline concluded that more impaired patients declined faster, although the authors also acknowledged considerable heterogeneity amongst findings [26].
Yet interestingly in our study, whilst patients with YOAD had lower baseline MMSE scores and a faster rate of cognitive decline than those aged >65 years, there was a different pattern within the >65 years age group. The initial MMSE score of patients with MOAD did not significantly differ from that of patients with LOAD, but the MOAD patients declined more quickly. Therefore, while greater baseline severity may have contributed to increased rate of decline in the YOAD groups, this cannot be said for the differences in progression between MOAD and LOAD. This suggests that even within patients aged over 65 at diagnosis, age at diagnosis is a significant predictor of decline. Furthermore, in a meta-analysis of 10 AD clinical trials there was no difference in baseline MMSE across any of the age at diagnosis groups (range 48 to 105 years), and yet the older patients declined more slowly. Therefore, in wider research the overall association between age at diagnosis and rate of decline appears to hold across all age groups, regardless of baseline severity [27].
The different rates of decline in AD depending on age at diagnosis may be connected to the observation that age-associated neuropathologies are not mutually exclusive. It is likely that there are interactions of different pathological processes or proteins that seem to aggravate each other [28]. Neuropathological studies suggest older adults are more likely to have simultaneous presence of multiple pathologies in the brain which may accelerate disease progression [28–30]. However, from our sample of older patients and similar to other studies [2–27], we found older adults had a slower rate of decline. A possible explanation for this is that younger individuals have a more “pure” and greater degree of AD pathology, whereas the “older” brain often has mixed neuropathologies [29]. Younger onset of AD is associated with greater grey matter atrophy, increased glucose hypometabolism and greater tau deposition measured using neuroimaging [31]; neuropathologically more severe senile plaques, neurofibrillary tangles, and synapse loss [8]; as well as greater deficits in the neurochemical acetylcholine and other neurotransmitters such as adrenaline [32]. One large neuropathological study found that, while AD and other neurodegenerative pathologies were associated with progressive cognitive decline, some types of vascular pathology did impair cognition but the effect was stable over time [33]. In our study, the MOAD and LOAD groups had a higher rate of hypertension compared to the YOAD group, and there was a difference in the HIS score between the LOAD and YOAD groups suggesting the possible addition of vascular pathology in older patients. In this study, therefore it is likely that the typical LOAD patient had more cerebrovascular disease than YOAD patients. However, the effects of mixed pathologies on clinical progression in AD remains an area of uncertainty, and there is a need for further studies to combine clinical and neuropathological data in particular to ascertain which pathologies are contributing to cognitive baselines, decline, and trajectories [30].
Methodological considerations
The study included a large sample of patients with AD, and there was a higher rate of inclusion of patients with YOAD compared to similar studies. There was also a substantial length of follow-up for all and a clear effect of age at diagnosis on the rate of cognitive decline was shown. Multilevel modelling is statistically powerful as it allows for repeated measurement of outcomes (MMSE) which can vary in number and interval between patients. All observations, including baseline, were a part of our analysis, but in view of the longitudinal nature of the study only patients with at least 12 months follow up with repeated MMSE score were included.
The limitations to this study are that there were no postmortem data available, nor biomarkers to add weight to the clinical diagnosis, and therefore some patients may have had an alternative diagnosis to AD. There are also possible confounding factors which have not been accounted for including APOE genotype, concomitant medications, and effectiveness of cholinesterase inhibitor medications such as agent and dose. Additionally, our longitudinal measure of cognition, the MMSE, has limitations. A previous study found that the measure of the rate of changes in MMSE scores were not as reliable when observations were separated by less than 36 months [34]. Furthermore, our data by nature reflects patients who returned to services for follow-up assessment, and therefore may not generalize to patients who are seen only once in clinic. However, all patients included in the analysis were assessed in a uniform manner against stringent diagnostic criteria.
A further limitation to consider is using ‘age at diagnosis’ of AD as opposed to ‘age at onset’. This may have introduced bias into the results as some patients may present later to memory services. Also, as discussed earlier, the diagnosis of YOAD in the early stages can be challenging which may result in these patients presenting later to memory services. Subsequently, they are more cognitively impaired at the time of diagnosis, and MMSE rate of change tends to accelerate for people with lower scores. It is therefore possible that age and the severity of cognitive impairment at diagnosis both influence the rate of decline in AD.
Clinical and research implications
It is important for clinicians to have an understanding of demographic variables affecting the course of cognitive decline in those with AD so that they can relay to patients and their carers the likely progression and help them to plan and prepare for the future. In the research setting, when recruiting patients, it is important to consider the age at onset of participants, since our and other studies have shown there is a reliable association between age at onset and rate of decline. Researchers testing interventions should consider the use of stratified randomization based on age at diagnosis rather than age at study entry.
Conclusion
In conclusion, we found there was some evidence of slower decline at older ages. The greater baseline severity of the YOAD is unlikely to have fully accounted for the increased rate of decline versus those >65. The MOAD group declined faster than the LOAD group despite the two groups having similar baseline MMSE scores. Therefore, even within patients aged over 65 at diagnosis, age is a significant predictor of decline. Other than age there were no independent variables in our data analysis significantly associated with the rate of decline in AD.