
Abstract
Individual cerebral small vessel disease (CSVD) may cause cognitive decline. However, the association between total burden of CSVD and cognitive deterioration in the general population remains unclear. We aimed to determine whether total CSVD score is associated with cognitive performance change and incident dementia in the general population. In the longitudinal population-based Taizhou Imaging Study, 556 participants free of neurological disorders underwent brain MRI and neuropsychological testing at baseline. A total of 456 participants were followed up for cognitive performance for a mean (standard deviation) of 4.6 (0.6) years. Total CSVD score (range 0–4) was calculated by assigning 1 point for the presence of each of the following markers: lacune, white matter hyperintensity, cerebral microbleed, and perivascular space. Beta regression was used to evaluate the association between total CSVD burden and MMSE score change. The association of prevalent CSVD with incident dementia was studied using Fisher’s exact test. CSVDs were present in 262 individuals (47.1%). The total CSVD score was significantly associated with MMSE score decline (p = 0.001). Compared to those with no CSVD, participants with 4 CSVD markers had a steeper decline in MMSE score (β: –0.53, 95% CI: –0.86 to –0.21; p = 0.001). A total of 15 participants developed dementia during follow-up. The presence of more than three CSVD markers at baseline was associated with a significantly higher risk of dementia (p = 0.020). Total CSVD burden appears to be associated with MMSE score decline and incident dementia in a general population in China.
INTRODUCTION
With the continuing increase in life expectancy, China is faced with the challenge of managing the growing burden of cognitive impairment and dementia. The incidence and prevalence of dementia increased rapidly from 1990 to 2010 and, according to conservative estimates, there are currently 9.19 million people living with dementia in China [1–3]. Identification of the risk factors and the early etiologic markers of cognitive impairment would help in health care planning and institution of treatment for patients with dementia.
Vascular pathology plays a prominent role in cognitive deterioration and dementia [4]. Evidence accumulated over recent years suggests that cerebral small vessel disease (CSVD) is important contributor to cognitive impairment, cognitive decline, and dementia [5–8]. White matter hyperintensity (WMH), lacune, cerebral microbleed (CMB), and perivascular space (PVS) are the main subtypes of CSVD commonly found in the magnetic resonance images of the elderly. Most of these changes are related to aging and are caused by underlying vascular pathology [9]. Previous studies have demonstrated that WMH [10], lacune [11], CMB [12, 13], and PVS [14, 15] are associated with worse cognitive performance and more rapid cognitive decline. A “total CSVD score”, calculated by combining individual CSVD markers, may better reflect the overall CSVD burden and serve as a useful predictor of clinical outcomes [16–18]. It could be a useful clinical tool, especially in countries like China, which have a high prevalence of CSVD [19, 20]. Several recent studies have shown that the total CSVD score is inversely associated with cognitive performance and cognitive decline [7, 21–23]. However, most of these studies were limited by their cross-sectional design [7, 23] or by the inclusion of only patients [8, 22]. Therefore, it is still uncertain whether the total CSVD score is associated with cognitive decline in the general population.
In this study we used the data from the prospective population-based Taizhou Imaging Study (TIS) to investigate whether the total CSVD score is associated with assessing by Mini-Mental State Examination (MMSE) score decline, and incident all-cause dementia over a 5-year follow-up.
METHODS
Study design and participants
For the present study, we used longitudinal data from the TIS, which is an ongoing population-based neuroimaging cohort study and a part of the Taizhou Longitudinal Study (TZL) [24], that was initiated in March 2013 in Taizhou City, Jiangsu Province, China. In the phase I of the TIS, participants were recruited from two villages (Lubao and Hutou) with previous high response rates in the TZL; these villages adjoin Taixing, a county under the administration of Taizhou City. Inclusion criteria were as follows: 1) Han Chinese aged 55–65 years and resident in Taixing for at least 10 years; 2) free of stroke, cancer, psychiatric disorders, and/or renal failure; 3) able to walk and communicate normally and independently, and able to provide information by self-reporting and participate in physical examinations; and 4) willing to provide informed consent. A total of 624 individuals were identified who satisfied these criteria. Of these, 62 either did not respond to the invitation to participate in the study or refused participation. The remaining 562 individuals (response rate 90.1%) were invited to undergo the baseline examination between March 2013 and January 2015. Follow-up with personal interview and expanded cognitive examinations were performed until August 2018 on 462 individuals. A total of 100 individuals did not complete follow-up for various reasons: death (n = 16), unwillingness to attend (n = 14), change of place of residence (n = 11), inability to cooperate (e.g., migrant worker, severe disease, psychiatric disorder; n = 57), and unknown reasons (could not be contacted by any means; n = 2). In addition, the baseline MMSE scores were not available for 6 individuals, and these were therefore excluded. Thus, a total of 456 individuals were included in the final analysis (Fig. 1).
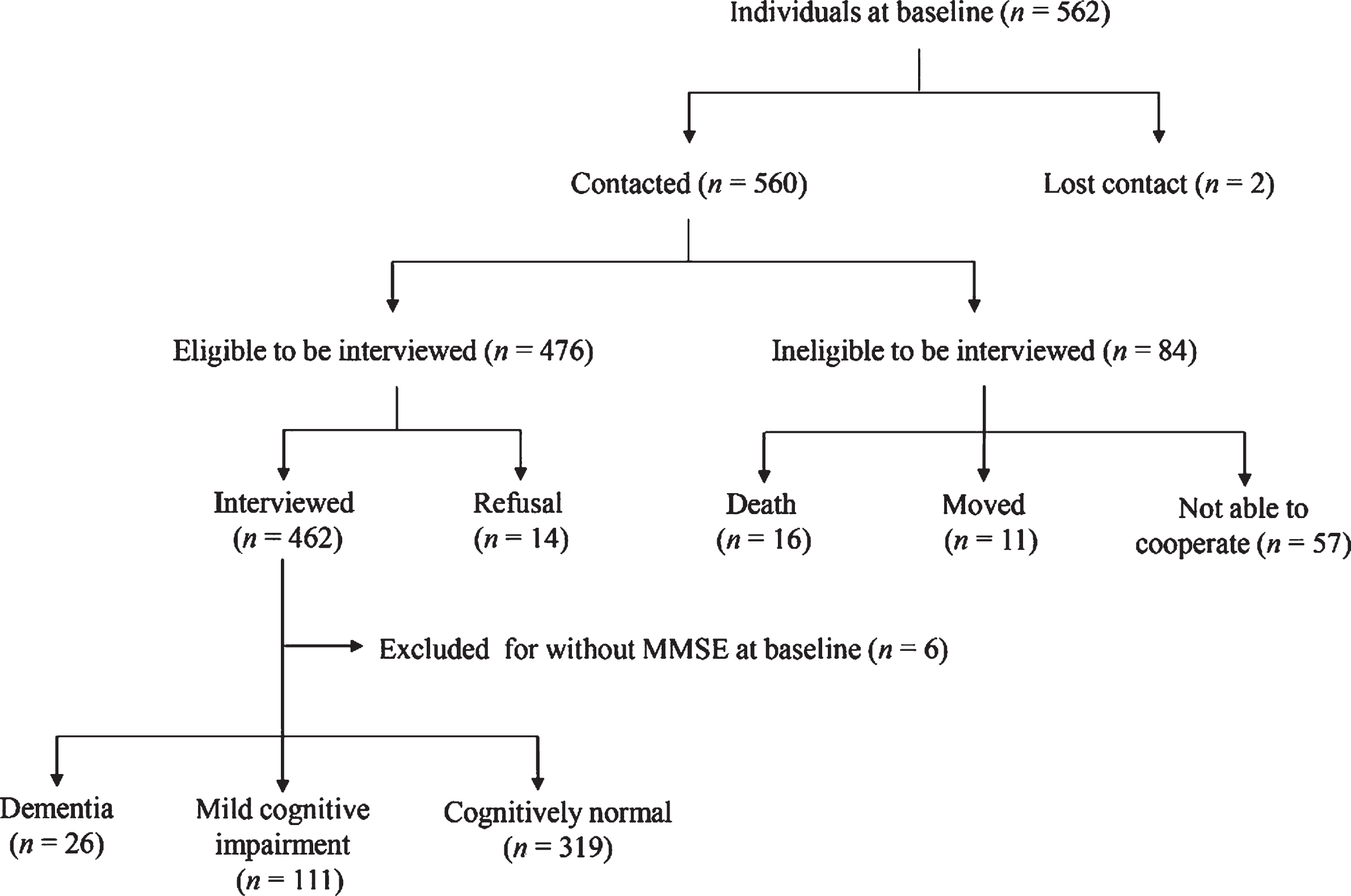
Flow chart of the follow-up for individuals’ cognitive function in the Taizhou Imaging Study.
The TIS was approved by the Ethics Committee of the School of Life Sciences, Fudan University, Shanghai, China (institutional review board approval number: 469). Written informed consent was obtained from each participant before data collection.
Baseline characteristics of the TIS
At the baseline of the TIS, demographic data (birth date, sex, and years of education), lifestyle characteristics (cigarette smoking and alcohol drinking), and medical and medication history of all participants were obtained via a detailed interviewer-administered questionnaire. Blood pressure (BP) was measured in the right upper arm in a sitting position after the participant had rested for 10 min in a quiet room. Two measurements were made 5 min apart, and the mean was recorded. Hypertension was defined as blood pressure≥140/90 mmHg, a previous diagnosis of hypertension, or treatment with antihypertensive drugs. Venous blood samples were collected by certified nurses in the morning between 7 AM and 8 AM after overnight fasting. Serum fasting glucose, total cholesterol (TC), triglyceride (TG), high-density lipoprotein cholesterol (HDL-C), and low–density lipoprotein cholesterol (LDL-C) were assayed using an automatic biochemical analyzer (TBA-40FR; TOSHIBA Corp., Tokyo, Japan). Diabetes was defined as fasting plasma glucose level≥7.0 mmol/L, previous diagnosis of diabetes, or antidiabetic drugs use. Hyperlipidemia was defined as TC≥5.2 mmol/L, or TG≥1.7 mmol/L, previous diagnosis of hyperlipidemia, or current use of lipid-lowering drugs. All examinations were conducted at the Taizhou People’s Hospital, Taizhou City, Jiangsu Province, China.
Genotyping of apolipoprotein E ɛ4 (APOE ɛ4, rs7412 and rs429358) was performed on coded genomic DNA samples using Axiom Precision Medicine Research Array. An APOE ɛ4 carrier was defined as an individual with at least one ɛ4 allelic variant.
Brain MRI acquisition and CSVD assessment
Baseline brain MRI was performed for all of 562 participants on the same 3.0T scanner (Magnetom Verio Tim scanner; Siemens, Erlangen, Germany) with a pre-determined multi-sequence protocol in Taizhou People’s Hospital. The MRI sequences included T1-weighted (T1W) and T2-weighted (T2W) imaging, fluid attenuated inversion recovery (FLAIR), T2*-weighted gradient recalled echo (T2*-WGRE), proton density-weighted imaging (PDWI), perfusion-weighted imaging (PWI), diffusion tensor imaging (DTI), and time of flight 3D (TOF–3D) magnetic resonance angiography. The parameter settings of each MRI sequence are listed in Supplementary Table 1.
Baseline characteristics of study participants
APOE, apolipoprotein E; CMB, cerebral microbleeds; CSVD, cerebral small vessel disease; IQR, interquartile range; MMSE, Mini-Mental Status Examination; PVS, perivascular space; TGV, total grey matter volume; TIV, total intracranial volume; WMH, white matter hyperintensity. #There are 28 (6.1%) missing data in APOE ɛ4 status, 9 and 7 missing data in TGV and TIV at baseline and at follow-up, respectively.
Diagnosis of all subtypes of CSVD was according to the Standards for Reporting Vascular Changes on Neuroimaging (STRIVE) [25]. Periventricular and deep WMHs were identified on FLAIR and T2-weighted sequences [26]. The severity of WMHs was rated using Fazekas scale (0-3). Only participants with moderate and severe WMHs (Fazekas score ≥ 2) were defined as presence of WMH in our study. Lacunes were defined as small (3–15 mm in diameter) cavities filled with fluid with the same signal characteristics as cerebrospinal fluid (CSF), and usually surrounded by a hyperintense rim on FLAIR sequence. CMBs were defined as round or ovoid hypointense lesions on T2*-WGRE sequence; the diameters of the CMBs ranged from 2 mm to 5 mm. Large PVSs were round or tubular deficits with CSF-like signal and a short axis≥3 mm in the subcortical area, without a rim or area of high signal intensity on FLAIR sequence. All scans were read by two experienced neurologists (MC and QY) who were blinded to all participants’ information. They reviewed images independently using Horos software (version 1.1.7). The final report was based on a consensus. In case of disagreement another, senior neuroradiologist (WJT) was consulted. The kappa values for WMH, lacune, CMB, and PVS were 0.896, 0.783, 0.752, and 0.827, respectively. In addition, Freesurfer version 6.0.0 (http://surfer.nmr.mgh.harvard.edu/fswiki/) was used to evaluate the volume and thickness of brain regions.
The total CSVD score for each individual was calculated by assigning a score of 1 point for the presence of each of the four MRI markers (WMH, lacune, CMB, and PVS). Thus, the total CSVD score could range from 0 to 4 [7, 23].
Assessment of cognitive function
Baseline global cognitive function was assessed with MMSE [27] on the same day as the MRI. During follow-up, in addition to MMSE, all individuals received an expanded neuropsychological test battery that assessed four cognitive domains-memory, executive function and attention, visuospatial function, and language. Two separate versions of the neuropsychological battery were used according to the education level of the individual, since reading and writing skills were required in certain tests [28]. Different cognitive domains (memory, executive function and attention, visuospatial function, and language) were assessed as follows:.
For participants with≥6 years of formal education: Memory: immediate and delayed recall (3 min and 20 min) in the Chinese version of auditory-verbal learning test [29]; Executive function and attention: conflicting instruction task and trail-making test A/B (TMT) [30, 31]; Visuospatial function: clock drawing test (CDT) [32]; Language: animal fluency test (AFT) [33].
For participants with < 6 years of education:
The neuropsychological test battery that we used has been previously validated in Chinese population-based studies [28, 31–33]. The tests were administered by neurologists and neuropsychologists (YZW, MYD, PXL, and MC) in our study team. Changes in global cognitive function were calculated by subtracting the baseline MMSE score from the follow-up MMSE score.
Diagnosis of dementia
A neurologist (MC) and a clinical neuropsychologist (QHG) reviewed the medical and cognitive assessment data and reached a consensus regarding the presence or absence of dementia, using the Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5) criteria [35]. Dementia was also recorded as present if individuals had been diagnosed with dementia at the cognitive clinic.
Incident dementia was recorded as such if individuals without evidence of dementia at baseline developed any form of dementia over the 5-year period follow-up. For non-dementia screening at baseline we used education-stratified cutoff points of MMSE, as proposed in a previous Chinese population-based study [27]; these cutoffs were as follows: ≤17 for illiterate individuals, ≤ 20 for participants with 1–6 years of education, and≤24 for individuals with≥7 years of education.
Statistical analysis
Continuous variables were summarized as mean (standard deviation, SD) or median (with interquartile range, IQR) when appropriate. Categorical variables were summarized as frequencies (%). The Student’s t–test and Kruskal–Wallis test was used to compare normally and non-normally distributed continuous variables, respectively. The Pearson chi-squared test was used for comparisons of categorical variables.
We investigated the association of total CSVD score with MMSE score decline and incident dementia, using participants without CSVD as the reference group. We first used Kruskal–Wallis test to compare the difference in MMSE score changes for different CSVD scales. Next, considering the change in MMSE score as a bounded continuous variable, with distribution significantly different from a normal distribution, we used beta regression to assess the association between total CSVD score and 5-year follow-up cognitive change [36–38]. To be specific, the dependent variable, i.e., changes of in MMSE score, was first mapped to the open interval (0, 1) following by the transformation [36]:
Statistical analysis was performed using R, version 3.5.1 (https://www.r-project.org/) and SPSS, version 19.0 (IBM Corp., Armonk, NY, USA). Differences were considered to be statistically significant at p < 0.05.
RESULTS
Baseline characteristics of the study population
The baseline characteristics of 556 individuals who underwent full baseline examination are summarized in Table 1. The mean (SD) age was 59.26 (2.72) years; 259 (46.6%) were men. These individuals had received formal education for a median of 6 years (IQR: 0, 9 years). The prevalence of hypertension, diabetes, and hyperlipidemia was 55.0%, 14.0%, and 54.7%, respectively. Current smokers, current alcohol drinkers and APOE ɛ4 carriers constituted 40.5%, 32.7%, and 16.5% of the study population, respectively. The median baseline MMSE score was 27 (IQR: 23, 29). CSVD was present in nearly a half of the study population (47.1%, n = 262). Among the MRI markers, PVSs were the most prevalent (28.1%, 156/556), followed by lacunes (26.6%, 148/556), CMBs (18.3%, 102/556), and WMHs (10.4%, 58/556). The median of TGV and TIV were 552.9 (IQR: 506.6, 587.9) cm3 and 1493.8 (IQR: 1384.2, 1602.6) cm3, respectively.
Of the 556 individuals, 456 underwent follow-up cognitive function assessment, with a mean (SD) interval of 4.6 (0.6) years from the baseline examination (Fig. 1, Table 1). We compared the baseline characteristics of individuals with and without follow-up. The mean (SD) age of individuals with follow-up was significantly higher than that of individuals without follow-up (59.39 [2.73] versus 58.66 [2.64] years; p = 0.015). However, there were no significant differences in the prevalence of baseline CSVD markers, brain volume, or other demographic characteristics between those with and without follow-up examination.
CSVD and MMSE score decline
Table 2 shows the baseline CSVD scores of the 456 individuals with follow-up examination: 237 (52.0%) individuals scored 0 points, 122 (26.8%) scored 1 point, 42 (9.2%) scored 2 points, 34 (7.5%) scored 3 points, and 21 (4.6%) scored 4 points.
Association (regression coefficient [95% confidence interval [CI]]) of prevalent cerebral small vessel disease (CSVD) with cognitive change after 5-year follow-upa
aCognitive change was defined as the difference between MMSE score at follow-up and the score at baseline; a negative change score indicated MMSE score decline. Model 1 was univariate; Model 2 was adjusted for age and sex; Model 3 was further adjusted for baseline MMSE score, follow-up time interval, current smoking, current alcohol drinking, years of education, hypertension, and the ratio of total grey matter volume to total intracranial volume. Abbreviations are as listed in Table 1. Bold values indicate p < 0.05.
After median 4.7 years (IQR: 4.0, 5.0)—i.e., 2073.1 person-years of follow-up—there was a statistically significant decline in MMSE: the median MMSE score decreased from 27 (IQR: 23, 29) at baseline to 24 (IQR: 19, 27) at follow-up (p < 0.001). The MMSE score of the individuals with 4 CSVD markers was significantly lower than that of individuals with no CSVD marker at baseline (p = 0.040; Fig. 2).
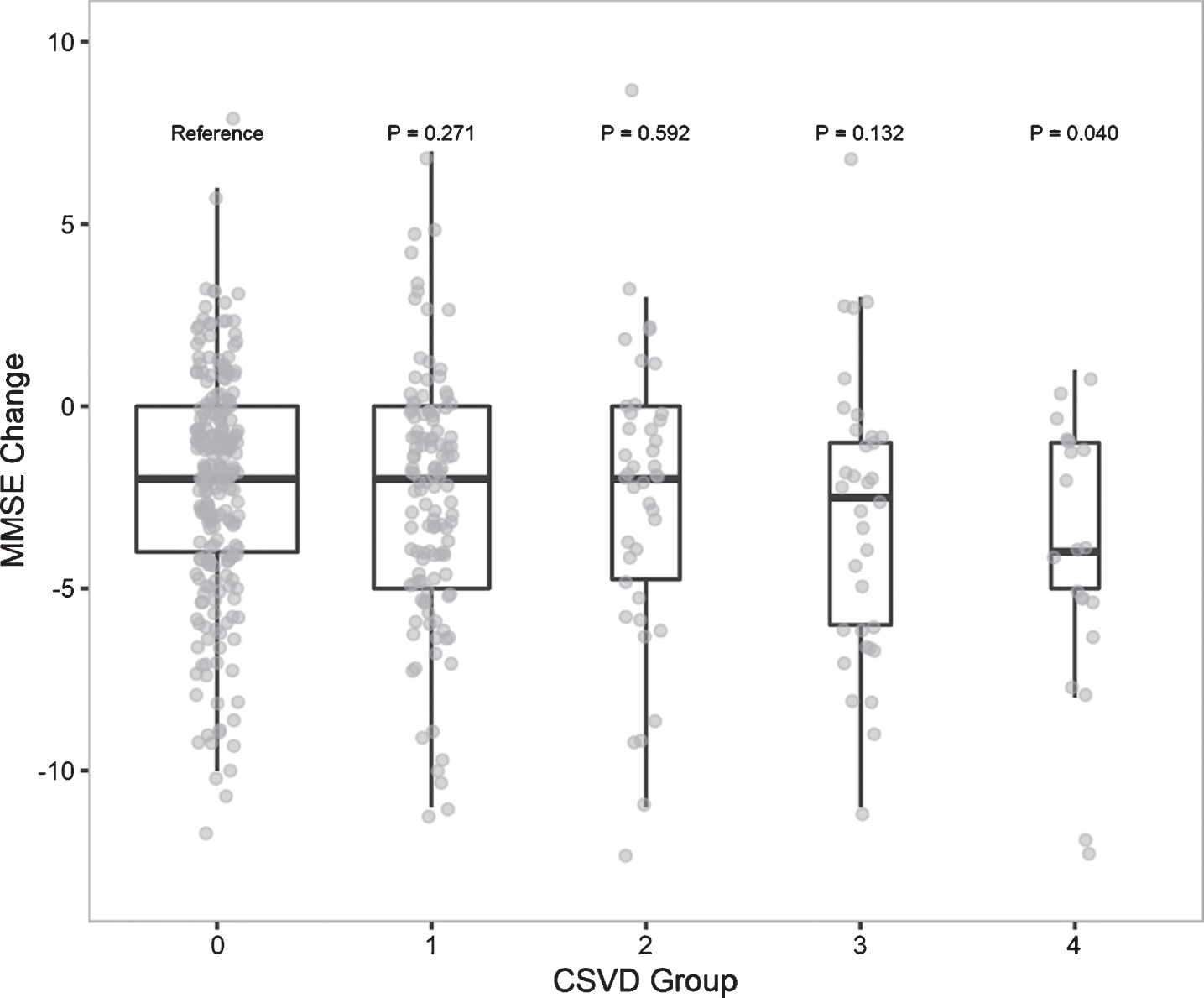
MMSE score change in different CSVD score groups. Cognitive change was defined as the difference between MMSE score at follow-up and the score at baseline, a negative change score indicated MMSE score decline. Kruskal–Wallis Test was used to compare difference in MMSE score change, using people without CSVD as the reference group. Abbreviations are as listed in Table 1.
Each of the CSVD marker was significantly associated with MMSE score change, except for CMB (boundary significant; p = 0.054) (Supplementary Table 2). Individuals with four CSVD markers had worse performance on the MMSE test than individuals with no CSVD marker at baseline (full adjusted mean model regression coefficient, –0.53, 95% CI: –0.86 to –0.21; p = 0.001). There was a trend for significant decrease in MMSE score with increase in CSVD score (ptrend = 0.001 in the full adjusted model). However, the presence of any one CSVD marker was not associated with a decline in MMSE scores in either the univariate or the adjusted models (Table 2). Additionally, we observed no significant interactions between age and duration of follow-up or baseline MMSE score on the association of CSVD and MMSE change. Moreover, the association of CSVD and MMSE change was not substantially affected when further adjusted APOE ɛ4, diabetes, and hyperlipidemia in sensitivity analysis.
CSVD and incident dementia
Of the 456 individuals who completed follow-up, 403 were diagnosed as dementia free at baseline. Over the mean 4.6 years of cognitive follow-up, using the expanded neuropsychological battery, we diagnosed 15 (3.7%) individuals with incident all-cause dementia. Dementia was significantly more likely in those with > 3 CSVD markers at baseline than in those with no CSVD marker (10.9% versus 2.4%; p = 0.020). Individuals with 1 or 2 CSVD markers also had higher incidence of dementia than those with no CSVD marker, but the differences were not significant (5.1% versus 2.4%, p = 0.190; and 3.4% versus 2.4%, p = 0.747, respectively).
DISCUSSION
This community-based prospective study was performed to determine whether the total CSVD score is associated with cognitive performance change and incident all-cause dementia. We found that 47.1% of individuals had at least one MRI marker of CSVD, indicating high CSVD prevalence in rural Han Chinese population aged 55–65 years. The accumulation of MRI markers of CSVD was associated with accelerated MMSE score decline. Furthermore, the risk of dementia was significantly higher in individuals with > 3 CSVD markers.
To the best of our knowledge, the relationship between total CSVD burden and cognitive performance change in general population has not been reported earlier. CSVD has been found to be prevalent in patients with cognitive problems or cerebrovascular high-risk factors, and even in the normal elderly population [7, 22]. The prevalence of any one CSVD in our study population (47.1%) was higher than that reported in Ecuadorian (39.0%) [23] and Japanese (28.1%) population [41], but lower than that in a Scottish population (55.6%) [7]. Differences in age distributions between the studies undoubtedly contributed to this difference. However, it needs to be noted that the frequency of high CSVD score (i.e.,>3 CSVD markers) was higher in this studied population than that in the Scottish population mentioned earlier (12.1% versus 4.6%). We chose the age range of 55–65 years for this study because these individuals are old enough to have CSVD features on MRI, while being young enough to survive for follow-up. However, the relatively young age of the study population may have resulted in an underestimate of CSVD prevalence. The actual prevalence is almost certainly higher, which makes studies about the association between CSVD and cognitive performance on this population particularly important.
Many studies have suggested that CSVD has significant influence on cognitive performance and is one of the most common causes of cognitive impairment and incident dementia [5, 15]. However, all of these studies examined the relationship of only a single CSVD marker with dementia. In preventive and therapeutic trials, indicators that can reflect the overall impact of CSVD on the brain would be better for guiding decisions. The total CSVD score, as a simple and pragmatic way to assess completed brain damage, has been used previously in clinical practice [16–18].
In this population-based study, high total CSVD burden was significantly associated with MMSE score decline. A few previous studies have examined the relationship between total CSVD score and cognition. Huijts et al. [8] found that accumulation of MRI markers of CSVD in patients with hypertension and first-ever lacunar stroke was associated with decline in global cognition and information-processing speed. More recently, Banerjee et al. [22] confirmed that total CSVD burden was correlated with cognition in a small memory clinic population. Two previous population-based studies conducted in healthy older adults also demonstrated that the total CSVD score was significantly associated with worse cognitive performance [7, 23]. However, all of the studies mentioned above were either cross-sectional in design or performed on patients. The only longitudinal study—which was performed on 130 hypertensive patients (91 with hypertension and 39 with lacunar stroke)—found that the total CSVD score could predict global cognitive decline and executive function during follow-up [21].
An important finding in the present study was the strong association of high burden of CSVD on incident dementia. The relationship between total CSVD score and incident cognitive impairment (mild cognitive impairment or dementia) has not been reported previously in any population-based longitudinal studies.
The major strengths of our study include the longitudinal population-based design with a relatively long 5-year follow-up period, as well as the use of the same high resolution 3T MRI scanner. However, our study has several limitations. First, MMSE was used alone to assess the cognitive function at baseline; we therefore can only comment on the relationship between total CSVD score and MMSE score decline. However, it must be pointed out that MMSE has been previously used as a cognitive assessment tool to calculate global cognition, and as a single test tool to calculate the global cognition [7, 22]. In addition, we could not evaluate the relationship between total CSVD burden and incident MCI. Second, participants who attended follow-up were significantly older than those lost to follow-up, and this might have biased the association between total CSVD burden and cognition. However, the results were robust even after full adjustment for age and other potential confounders. Moreover, the mean age of participants in our study was lower than that of participants in most previously published similar studies (59.4 years versus 58.7–72.7 years) [7, 21–23], which also supports the reliability of our results to some extent. In addition, we could not treat the incident CSVD as confounding in the relationship of total CSVD score at baseline and cognitive performance change, since the brain MRI was not conducted at follow-up. Third, the relatively small sample size and the inclusion of only rural residents affects the generalizability of our results; however, the significant association of total CSVD score and worse cognitive performance was confirmed a previous larger study [7]. In addition, the second round of TIS has been initiated, and the results of multiple examinations on a larger sample are expected, which will help clarify the association between CSVD and cognition.
Conclusion
In conclusion, accumulation of MRI markers of CSVD appears to be associated with worse performance on the MMSE, and incident dementia in a general population aged 55–65 years resident in rural China. A high total CSVD score, based on the presence of lacune, WMH, CMB, and PVS, may be useful for predicting future cognitive deterioration.
Footnotes
ACKNOWLEDGMENTS
We would like to thank Dr. Weijun Tang, Qi Yang, Qihao Guo, Ding Ding, Mengyuan Ding, and He Wang for their help with MRI image rating and neuropsychological data reviewing. We are grateful to all the participants for their cooperation. We thank the personnel from Fudan University Taizhou Institute of Health Sciences, the staff of Taizhou People’s Hospital and Taixing Disease Control and Prevention Center (CDC) for their assistance in conducting the medical interviews and data collection. This study was supported by the National Key Research and Development program of China (grant number: 2017YFC0907002, 2017YFC0907501, 2017YFC0907201), the International Science and Technology Cooperation Program of China (grant number: 2014DFA32830), the Key Research and Development Plans of Jiangsu Province, China (grant number: BE2016726), the Key Basic Research Grants from Science and Technology Commission of Shanghai Municipality, China (grant number: 16JC1400500), and Shanghai Municipal Science and Technology Major Project (grant number: 2017SHZDZX01).