
Abstract
Background:
Characterizing the earliest demonstrable cognitive decline in middle-aged adults at risk of Alzheimer’s disease (AD) will allow for the better understanding of the early disease trajectory, and the provision of therapies prior to clinical symptom onset. We developed an online platform— healthybrainproject.org.au (Healthy Brain Project; HBP)— to recruit, assess, and monitor at-risk middle-aged adults.
Objective:
Describe the HBP methodology and report baseline characteristics and adherence indices of participants.
Methods:
Between February 2017 and August 2018, 4,000 community-based middle-aged Australian adults with a first or second-degree family history of dementia enrolled at our website (healthybrainproject.org.au). Participants were directed to complete five modules: “Basics”, “Health History”, “How You Feel”, “How You Live”, and “How You Think”. Of these, 1,816 participants have received a saliva sampling kit for genetic analysis.
Results:
Participants had a mean (SD) age of 55.5 (6.8) years, 11.8 (3.4) years of education, and annual personal income of AUD$68,830 ($35,044). Participants took 26.4 (49.7) days after enrolment to complete questionnaires and cognitive tests. Most participants were from Victoria (63%), followed by New South Wales (14%). Most participants (74%) were female and 76% identified as Caucasian. Approximately 36% of participants completed all modules (n = 1,450), and 56% (n = 2,221) completed 4 out of 5 modules. Most saliva kits (89%) had been returned.
Conclusion:
The HBP joins a handful of online registries worldwide that assess and monitor a large cohort of individuals at risk of AD. Our study extends on these efforts by focusing on midlife, where the earliest signs of cognitive and pathological changes will manifest.
Keywords
INTRODUCTION
The number of individuals living with dementia, of which Alzheimer’s disease (AD) is the most common cause, is projected to rise to ∼14 million by 2050. Studies evaluating AD biomarkers indicate that AD pathophysiological changes can begin up to 30 years before the onset of clinical symptoms. For example, abnormally high levels of amyloid-β (Aβ+) are detected (e.g., using positron emission tomography [PET] neuroimaging or cerebrospinal fluid [CSF] sampling) in 30% of cognitively normal (CN) adults aged over 60 years [1]. Despite the absence of clinical symptoms, prospective studies conducted over relatively brief periods (e.g., 1–3 years) show increased rates of cognitive decline and brain volume loss, as well as a higher risk of progression to AD or mild cognitive impairment (MCI), in Aβ+ CN older adults [2 –5]. In recognition of this important preclinical stage, Aβ+ CN adults who show decline from their previous level of cognitive function are now defined as being on the AD continuum [6, 7]. Identification of such individuals is critical for future AD therapeutic trials [8, 9], but this will require careful longitudinal evaluation as abnormalities in cognitive function, mood, and behavior at this early disease stage are subtle [3] and may require more sensitive tests (e.g., using novel smartphone or online-based tests).
The notion that early AD-related cognitive decline exists on a wide continuum has also been applied to AD biomarkers. Prospective biomarker studies suggest that even before Aβ concentrations reach levels of abnormality, subtle increases in the rate of accumulation provide a signal that AD pathogenesis has begun [10, 11]. Further, rates of Aβ accumulation are fastest in the earliest stages of preclinical AD and correspond with faster rates of cognitive decline [12]. More recently, we observed that in individuals with subthreshold Aβ levels, those who carried at least one copy of the apolipoprotein E (APOE) ɛ4 allele showed faster Aβ accumulation [13]. Others have also observed that falling levels of CSF Aβ42 can be detected in ɛ4 carriers as early as in the mid-40s [14]. Abnormal Aβ accumulation, particularly in middle-aged APOE ɛ4 carriers, may thus signal AD before Aβ reaches traditional thresholds of abnormality.
In addition to age and APOE ɛ4, other factors including sex, lifestyle factors, cerebrovascular disease, and other genetic factors have been implicated as risk factors for AD [15 –18]. Understanding how these complex genetic, lifestyle, and health-related factors modify the association between AD biomarkers and cognitive outcome will also be critical to understanding and recognizing the earliest stages of AD. We therefore developed the Healthy Brain Project (HBP), an Australian cohort of middle-aged (40–70 years) community-dwelling adults. We aimed to measure changes in cognition, lifestyle, mood, and medical health in relation to genetic risk (collected from posted saliva samples), to facilitate the identification of the earliest stages of AD. The HBP was designed to recruit, assess, and monitor participants predominantly online using a secure website (healthybrainproject.org.au). Using this platform, we were able to rapidly recruit participants in a cost-effective manner, while maximizing population generalizability and racial diversity, and minimizing participant burden. The use of online platforms to perform large studies evaluating risk for neurodegenerative disease is becoming more common as a consequence of rapid technological advances, improvements in the understanding of the strengths and limitations of these technologies as well as increased familiarity and use of online systems by the general public. For example, in the United States of America (USA), both the Brain Health Registry (BHR; brainhealthregistry.org) and the TRC-PAD initiative utilize online platforms to identify large numbers of at-risk individuals (e.g., 50,000) for enrolment into AD clinical trials [19, 20]. In Europe, several initiatives such as the Dutch Brain Health Registry (www.hersenonderzoek.nl), Join Dementia Research (joindementiaresearch.nihr.ac.uk) and the European Prevention of Alzheimer’s Disease (ep-ad.org) have also successfully identified many individuals at risk of AD via online platforms [21, 22]. Recruitment for these studies has been demonstrated to be rapid and cost-effective and reported to be more feasible than studies requiring in-clinic assessment. Furthermore, use of online platforms facilitates the inclusion of individuals from more diverse backgrounds who may not typically have access to medical research studies due to factors such as proximity to research sites, time to attend research visits, or restrictions due to physical impairments [23].
Despite the growing popularity of online studies of early AD, the design characteristics necessary for the successful use of online platforms for the recruitment, assessment, and continued engagement of participants in research studies or clinical trial-ready cohorts are yet to be elucidated. For example, the length of assessments, nature of information gathered, and usability of the website have been shown to influence adherence in online psychological experiments [24]. Adherence and completion of online assessments are influenced by physical factors such vision, hearing and motor skills, as well as cognitive abilities and demographic factors including education levels and familiarity with online platforms [24, 25].
The aims of this report were to describe the baseline characteristics of the first wave of recruited participants in the HBP and to describe usability and adherence to the HBP platform by examining rates of attempts and completion of the different questionnaires and cognitive tests.
METHODS AND MATERIALS
Study inclusion criteria
The HBP is open to adults aged 40 to 70 years who live in Australia, with a first-or second-degree family history of dementia. Participants are only permitted enrolment into the HBP platform if they confirm that they are currently residing in Australia (irrespective of citizenship); they are fluent in English; they have a first-or second-degree family history of dementia; that they do not have a diagnosis of Alzheimer’s disease, Parkinson’s disease, dementia with Lewy bodies, or other known diagnosis of dementia; that they do not have a history of major traumatic brain injury or other neurological disease or insult; that they do not have a diagnosis of a major psychiatric condition (e.g., schizophrenia, uncontrolled current major depressive disorder, or other psychiatric disorder); and that they do not use any Pharmaceutical Benefit Scheme approved medication for the treatment of AD (e.g., donepezil, galantamine, rivastigmine, or other approved medications). Participants receive no compensation for completing the study.
HBP platform and procedure
The HBP consists of a public website (healthybrainproject.org.au), which can be used on desktop computers, laptop computers, tablets, and mobile devices which run Chrome, Safari, Internet Explorer, or Firefox web browsers. The HBP platform was developed by PearlArc Systems Private Limited (Bengaluru, India) and SRC Innovations (Melbourne, Australia) using C# in InVision Studio. All online data is encrypted and stored securely on servers based at the Florey Institute of Neuroscience and Mental Health (“Florey”). The primary investigators of the HBP (YYL, RFB, NY) have access to all stored data, and are administrators of the database server. Identifying information for each participant is stored separately from online study data and is held in a password-protected folder located on a secure server at the Florey. The HBP was approved by the human research ethics committee of Melbourne Health at the Royal Melbourne Hospital.
The landing page of the HBP website has a “Join Now” button that directs participants to the plain language statement and consent form. Participants can view the consent form through a web browser, download a portable document format (PDF) of the form, or request a copy to be emailed to them. Participants then indicate their willingness to join the study by clicking on a box and entering their full name (in lieu of a signature). After providing consent, participants are then directed to an enrolment page where information including first and last name, email address, password, handedness, date of birth, sex, and mailing address is collected. Participants are required to confirm that they reside in Australia (physical habitation in Australia is required, regardless of citizenship), and that they are fluent in English to allow compliance with the study protocol. Upon enrolment, an automated email is sent to welcome the participant to the HBP. This email reiterates the aims of the study and the tasks that the participant is required to complete.
Participants can then sign into their participant portal, where they are presented with a series of modules to complete. Each module is comprised of a series of questionnaires or cognitive tests, with each questionnaire taking 2–3 minutes to complete, and each cognitive test taking 10–15 minutes to complete. The total time to complete all questionnaires is approximately 85 minutes, and for all cognitive tests is 25 minutes. Table 1 summarizes the modules of the HBP, including the aim of each module and details of each questionnaire and cognitive test. Participants can complete modules and questionnaires/tests on separate days, and in any order. Up to two reminder emails are sent to participants if any module remains incomplete after 2 weeks and 1 month, respectively. Upon successful completion of all questionnaires and cognitive tests, an automated email is sent to the participant to thank them for their time and effort, and to inform them that a saliva sampling kit will be mailed to them shortly. Reminder emails are also sent to participants who fail to return their saliva samples.
Healthy Brain Project online modules, questionnaires and cognitive tests
The HBP platform also includes an administrator portal, which allows the research team to moderate registrations (e.g., withdraw participants from the study, delete duplicate accounts), track participants’ progress, create new modules, add new questionnaires or cognitive tests, create and export datasets for analyses, and moderate forum discussions.
Online modules and questionnaires
There are 5 main modules on the HBP website, each consisting of a set of well-validated questionnaires (see Table 1 for details). The overarching aim for the inclusion of each module is also summarized in Table 1. The vernacular term used to describe each questionnaire to participants was altered to make it more informative and accessible. The questionnaires were otherwise presented in their published and validated forms, except for small modifications to three questionnaires. For the GCS, which measures menopausal symptoms, participants must first indicate whether their biological sex is male or female. Only female participants are presented with the questionnaire. Similarly, for the PCL-5, participants must first indicate whether they have experienced a traumatic event in the past month. Only participants who respond “Yes” to the question “In the past month, have you experienced a very stressful life event (e.g., divorce, car accident, assault, threats to your safety or the safety of your family)?” are directed to complete the PCL-5. For the CFI, which was originally designed for older adults, some items were modified to include ecologically valid questions about subjective experiences of memory and thinking at work, and other relevant aspects of an individuals’ life (see the Supplementary Material).
In June 2018, a module was introduced to the HBP platform aimed at gauging participant’s motivation for medical research, barriers to participating in medical research, suggestions to increase participant engagement, and level of interest in participating in future biomarker studies. We also surveyed participants on the type of environment (e.g., at home, at work) in which they typically completed the modules and questionnaires. As this module was introduced very recently, only 596 participants had completed it at the time of analysis.
Online computerized cognitive assessments
To measure cognitive function in an unsupervised, online platform, we selected the Cogstate Brief Battery (Cogstate Ltd., Melbourne, Australia), and the Cambridge Neuropsychological Test Automated Battery (CANTAB) Paired Associate Learning (PAL) task (Cambridge Cognition, Cambridge, United Kingdom). Both batteries were provided at no charge through academic agreements, have been validated for unsupervised assessment, have demonstrated sensitivity to the construct of primary interest (memory), and have demonstrated sensitivity to AD-related cognitive change. Together, these tasks cover a wide range of cognitive domains, including processing speed, attention, learning and working memory. While participants can complete the questionnaires on any device, participants are required to complete all cognitive tests on a desktop or laptop. The Cogstate Brief Battery must be completed using Internet Explorer or Safari, and the CANTAB PAL must be completed using Google Chrome or Safari.
The Cogstate Brief Battery consists of four tasks: Detection (DET), Identification (IDN), One Card Learning (OCL), and One-Back (OBK) [40, 42]. DET is a simple reaction time test shown to measure psychomotor function. IDN is a choice reaction time test shown to measure visual attention. The primary outcome measure for DET and IDN was reaction time in milliseconds (speed), normalized using a log10 transformation. OCL is a continuous visual recognition learning task that assesses visual learning within a pattern separation model. OBK is a task of working memory and attention. The primary outcome measure for OCL and OBK was the proportion of correct answers (accuracy), normalized using an arcsine square-root transformation.
The CANTAB PAL task is a test of episodic memory [41, 43]. Between 6–8 boxes are displayed and opened in a randomized order to reveal two or more patterns. Each pattern is then shown in the middle of the screen and the participant must select the box where the pattern was originally located (using a mouse or trackpad). If an error is made, all pattern locations are revealed in sequence again. After four failed attempts within one stage, the task terminates. Participants complete 2, 4, 6, and 8 pattern trials. The main outcome measures are PAL total errors adjusted (total number of errors adjusted for the stage at which participants reached, with higher error scores denoting poorer performance), and PAL first attempt memory score (frequency with which participants chose the correct box on their first attempt, with lower scores denoting poorer performance) [41, 44].
Saliva sampling
Genotek Oragene (OG-500) 2 ml saliva kits (including instructions on saliva collection) are mailed out to participants who have completed at least 4 out of 5 modules. All saliva tubes are coded (deidentified) by the research team before being sent to the participant. Saliva is collected by the participant and returned via pre-paid registered post to the research team at the Florey. Upon return, saliva samples are temporarily stored at the Florey, after which they are posted in batches of 1,000 samples to GenoFIND Services laboratory (Salt Lake City, UT, USA), where they are processed to extract targeted SNPs including for APOE (rs429358, rs7412).
Recruitment
We have conducted a series of media appeals for volunteers, including through several news outlets (print, television, radio), organizations (e.g., Dementia Australia, NHMRC National Institute for Dementia Research) which have promoted the HBP to their networks, university newsletters, traditional word of mouth, and social media (e.g., Twitter, Facebook). Recruitment drives have also occurred through invited public lectures hosted by the Florey and other community-based organizations (e.g., we partnered with a large local football organization in August 2017 which resulted in nearly 2,000 enrolled participants). We have also published articles for The Conversation pertaining to dementia and brain health and have encouraged enrolment in the HBP in such articles [45 –47].
Participant engagement
An important component of the HBP is the involvement and engagement of participants. Participants who have successfully enrolled in the study have access to an online forum. This forum is closely monitored by the primary investigators of the study (YYL, RFB, NY), and their research team. The forum serves as a platform for participants to engage directly with the research team by asking questions pertaining to brain health or other aspects of their participation. It also allows participants to interact with each other by sharing their own strategies for maintaining brain health (moderated by the research team). Participation in the forum is optional. We also send biannual newsletters to participants, which summarize new features of the HBP, educational resources on brain health, AD and/or other dementias, and research activities of the research team. In addition, we host a Facebook page (∼530 followers), a Twitter feed (∼270 followers), and a YouTube channel (∼204 views per video).
Google analytics
Google Analytics is a free web analytics service offered by Google that tracks and reports website traffic. It provides information on the source of site users (e.g., organic web search, direct website entry, referral from other sites or social media), duration of site usage sessions, frequency of site visits per user, devices used to access the website (desktop, mobile, or tablet), usage metrics by time of day, pages within the site that are most frequently visited, and user geographical location. This platform is increasingly being used to analyze online medical research traffic patterns, and participant recruitment [48]. For the HBP, Google Analytics was employed from 1 January 2018. The tracking was placed on the main page, although subsidiary connections were automatically connected to the sub-components of the HBP website. In this report, we present Google Analytics data collected from 1 January 2018 to 15 August 2018, and only report metrics from the main page.
Data analysis
Recruitment into the HBP is ongoing. The current report includes data that have been collected up to the first formal DataFreeze on 15 August 2018.
For this report, we have defined “attempters” as participants who have completed at least one questionnaire or test (from any module). We have defined completion at the level of the modules. As such, “completers” are participants who have completed at least one questionnaire or test from each of the five main online modules described in Table 1. For example, an individual who completes all questionnaires in “Basics”, “Health History”, “How You Feel”, and “How You Live”, but not any cognitive tests in “How You Think” would be considered a “non-completer”. Conversely, an individual who completes 50% of questionnaires from each of the five modules would be considered a “completer”.
All analyses were conducted in the statistical program R (v 3.3.3). InteractiVenn was used to create a Venn diagram of the number of participants who completed each online module [49]. A series of chi-squares and analyses of variances (ANOVAs) were conducted to determine differences between “attempters” and “non-attempters”, and “completers” and “non-completers”. As the aim of this report is to provide a snapshot of the baseline characteristics of enrolled participants, and given the potentially large number of outcome variables, we have chosen to only report key variables from each module. These include basic demographics (age, sex, height, weight, ethnicity, years of education, occupational status, number of dependents, self and household income levels, geographical location), health history (current/past medical and psychiatric history, current medications, family history of dementia, history of smoking, excessive alcohol consumption and/or illicit drug use), personality (BFAS scores for neuroticism, openness, conscientiousness, agreeableness, and extraversion), subjective cognitive function (CFI total score), mood (DASS depression, anxiety and stress scores), and general physical health (RAND general health score). We also report measures of sleepiness (ESS total score), number of minutes spent sitting on a weekday and weekend, and the proportion of individuals who engaged in recreational walking, and vigorous recreational activities (e.g., aerobics, running, fast bicycling, or fast swimming) (IPAQ). For measures of cognitive function, we used raw scores for DET, IDN, OCL, OBK, and PAL. Future studies will provide more in-depth analyses of other outcome measures.
To determine the geographical location of participants, we used categories outlined in the Australian Statistical Geography Standard (ASGS) – Remoteness Structure [50]. These categories divide Australian postcodes into (a) major cities of Australia (RA1), (b) inner regional Australia (RA2), (c) outer regional Australia (RA3), (d) remote Australia (RA4), and (e) very remote Australia (RA5). Thus, we have classified the location of individuals in RA2-RA5 as “rural Australia”.
Medications were extracted from free-text entries by participants. Medication names that were incorrectly spelled were corrected with coding procedures, and then all duplicate medication names were removed from the total medication list to form a total of 622 unique medications. Each of these medications was subsequently classified using the World Health Organization Anatomical Therapeutic Chemical (ATC) code for drug classification (www.whocc.no/atc_ddd_index). This code classifies medications based on the organ or body system on which they have their primary effect, followed by sub-classifications based on specific pharmacological and chemical properties of the medication.
Despite our large sample size, the statistical significance for all comparisons was set at p < 0.05. Analyses were not adjusted for multiple comparisons as this is a novel area of research that reports one of the first outcomes of remote and unsupervised assessment of mood and cognitive function. Additionally, and where applicable, measures of effect sizes (Cohen’s d) were used to quantify the magnitude of difference between males and females. Effect sizes of <0.2 were classified as trivial, and not interpreted regardless of their statistical significance [51]. This reduces the likelihood of Type I error and contextualizes the meaningfulness of our findings.
RESULTS
Recruitment and geographical spread of participants
The HBP was launched on 1 February 2017. Figure 1 shows the cumulative enrolment of participants from 1 February 2017 to 15 August 2018, and our projected enrolment based on current recruitment rates. To date, 4,000 individuals have provided data on age, sex, and geographical location. Mean (SD) participant age is 55.2 (6.9) years, and 71.2% of participants are females. Most participants (2,514, 62.9%) were from Victoria, with the remainder from New South Wales (570, 14.2%), Queensland (337, 8.4%), Western Australia (239, 6.0%), South Australia (176, 4.4%), Tasmania (73, 1.8%), the Australian Capital Territory (71, 1.8%), and the Northern Territory (20, 0.5%). A quarter of participants (964) reported postcodes in rural Australia.
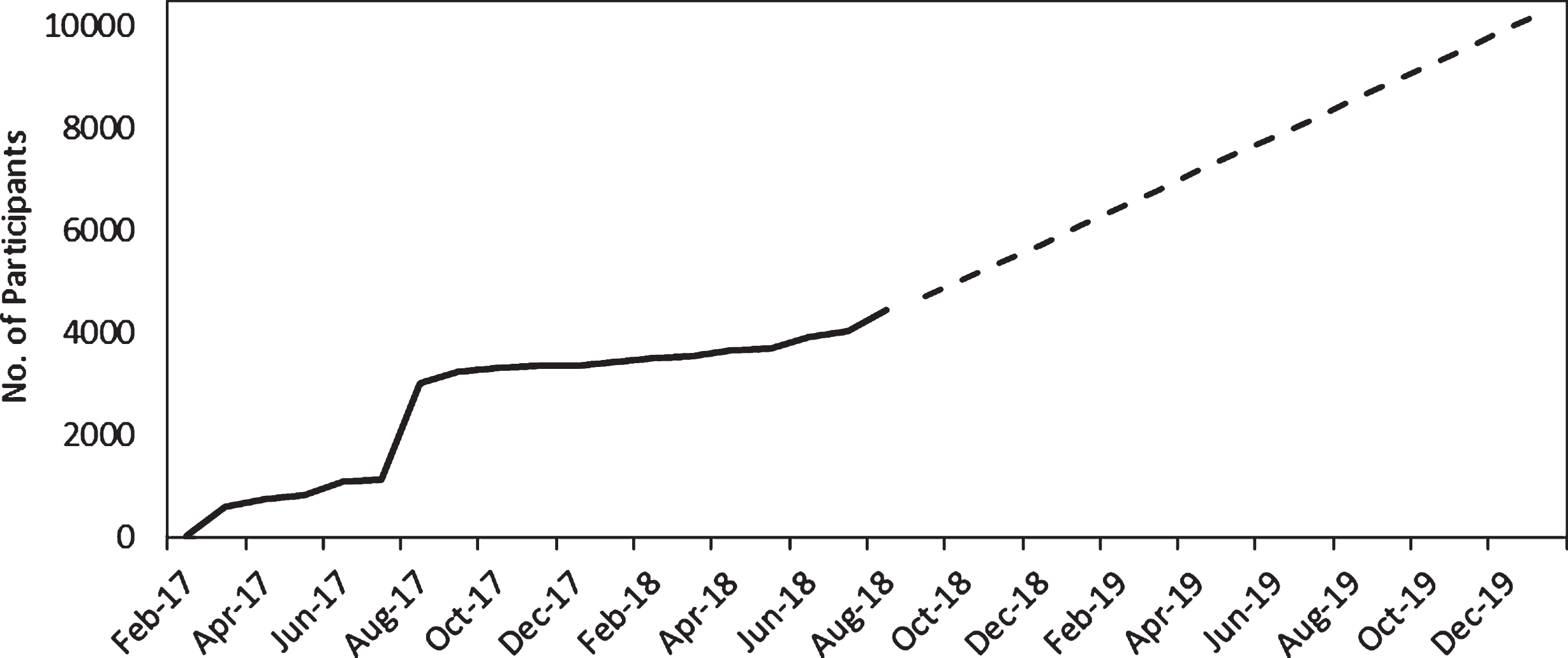
Current rate of recruitment (solid line) and projected enrolment (dotted line).
Most participants heard about the HBP through our media drives (57%), although others were also referred through social media (13%), word of mouth from friends and family (11%), the Florey (11%), and other (8%) sources (e.g., Dementia Australia, internet search).
Completion rates and environment
Of the 4,000 participants who enrolled on the Healthy Brain Project website, 2,703 participants ( 68%) completed at least one questionnaire or cognitive test (i.e., attempters). Participants who enrolled on the HBP website and provided data on age and sex but did not attempt any questionnaires or cognitive tests were younger (attempters = 55.53 years versus non-attempters = 54.65 years, (df)F = (1,3998) 14.15, p < 0.001), but the magnitude of this age difference was very small (Cohen’s d = 0.13 [0.06–0.19]). We also observed a significant difference in the proportion of females between attempters and non-attempters, with females making up 74% of attempters, and only 66% of non-attempters, χ 2 = 26.16, p < 0.001.
Figure 2 illustrates the number of individuals who had provided sufficient data to be considered a “completer” of each online module. Approximately 36% (n = 1,450) of the total sample were “completers”. Questionnaire data was available on 55% (n = 2,182) of the total sample, and cognitive data was available on approximately 42% (n = 1,675). At the time of analysis, saliva kits had been mailed to 1,816 participants (i.e., participants who completed all online questionnaires), and 89% had been returned (n = 1,618).
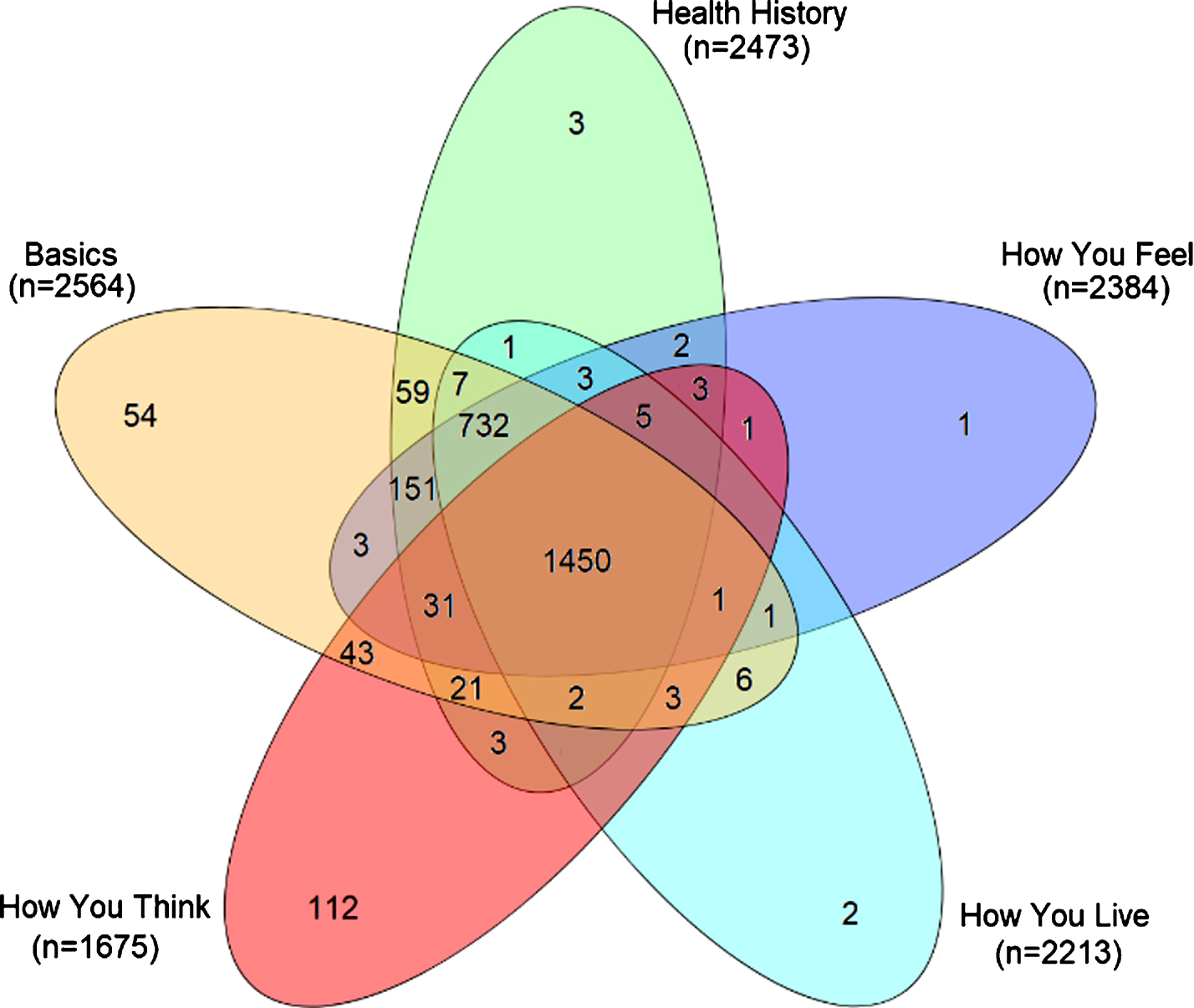
Number of individuals who completed each online module (blank segments indicate 0 participants).
Table 2 summarizes the number of participants who completed each online module, and each questionnaire or test within each module. “Completers” took approximately 26.32 days (SD 49.33) from the date of enrolment to complete the online modules. Most participants completed all questionnaires and tests within each module, with the highest completion rates observed for “The Basics” (99.5%), followed by “Health History” (99.2%), “How You Feel” (97.1%), “How You Live” (94.3%), and “How You Think” (82.3%).
Number of participants who completed each module, and number of days between enrolment and module completion
*Note: Motivation & Engagement module was only introduced in June 2018.
We also surveyed the environment in which participants typically completed testing on the HBP website (Fig. 3). Most completed questionnaires and cognitive tests at home, with 67% of participants indicating that they complete testing at home alone all the time or often, 47.7% of participants indicating that they complete testing at home, where others are present but are quiet (Fig. 3). Most participants (>80%) did not complete testing in environments that may be considered distracting (e.g., at work when other people are around and are noisy; public spaces).

Types of environment where participants completed testing on the Healthy Brain Project website.
Google analytics
Between 1 January 2018 to 15 August 2018, we received 8,008 new users visiting the website (i.e., new IP addresses that had not been previously logged by Google Analytics), and 3,364 unique returning visits (i.e., returning users that had their IP address logged by a previous visit), resulting in a total of 155,356 pageviews. The most common mode of access to the HBP website was by directly typing in the URL (42.8% [n = 3427] of new users; 50.6% [n = 1702] of returning users). Other common ways of accessing the website were to go through Google’s search engine (2,482 new users (31%), 875 returning users (26%)), and referrals from the Conversation website (1,842 new users (23%), 807 returning users (24%)). During Google Analytics active period, new users largely came from major metropolitan regions (i.e., Melbourne, Sydney, Brisbane, Perth, Adelaide, Darwin, 2,487 (92%)), with a minority from rural population centers (203 (7.5%)). Both new and returning users spent, on average, ∼9.5 minutes on the website each time they logged in.
The most common time to log into the website was in the morning prior to 12 pm, and the most common days were Sunday and Tuesday, which is partly due to the timing of major press releases. Windows operating systems were the commonest for new users (1,197, 44.5%), however, iOS was also common (872, 32%). New users typically accessed the website via their desktop computers (1516, 56.4%), followed by mobile access (728, 27.0%), and tablet devices (446, 16.6%).
Demographic, personality, mood, lifestyle, and cognitive characteristics
Table 1a and 1b summarize the demographic, personality, mood, lifestyle, and cognitive characteristics of the overall sample of 2,703 participants who had attempted questionnaires or cognitive tests (actual sample size varies by questionnaire and test). Overall, the typical HBP participant was a Caucasian female adult in their 50 s, with an average of 12 years of education, an annual personal income of ∼AUD$67,000, and who resided in an Australian capital city.
Of the 2,703 participants who had attempted questionnaires or cognitive tests, 1,450 participants submitted sufficient information across all 5 online modules to be classified as a “completer”, while 1,250 participants were classified as a “non-completer”. Table 3a and 3b summarizes the demographic, personality, mood and lifestyle characteristics of the overall sample, and differences between completers and non-completers. Compared to non-completers, completers were more likely to be female, Caucasian, and retired. Completers were also significantly older, exhibited higher levels of conscientious personality traits, and had lower depressive and anxiety symptoms. Completers reported higher levels of physical general health (RAND-GH) and were also more likely to engage in vigorous recreational activities.
Self-report demographic characteristics (categorical variables)
Note: *5 participants indicated that they would prefer not to disclose sex status; #Employed = full-time, part-time or casual employment.
Self-report demographic and personality characteristics (continuous variables)
Completers and non-completers did not differ in their geographical location, number of years of education, number of dependents, amount of time spent sitting on weekdays or weekends, or any measure of cognitive function (all d’s<0.2).
Medical conditions (self and family history)
Figure 4a-c illustrate participants’ current and past medical and psychiatric history, and current medications. A large proportion of participants ( 50%) reported no significant current or past medical history (Fig. 4a). The most common reported current medical conditions were arthritis (16%), hypercholesterolemia (16%), and hypertension (15%). Similarly, most participants ( 85%) reported no significant current or past psychiatric history (Fig. 4b). The most common reported current psychiatric conditions were anxiety disorders (7%) and depressive disorders (4%). Approximately half of the sample reported a first-degree family history of dementia (Table 1a), particularly in mothers (64%). Approximately 60% (n = 1475) reported a first-degree family history of cardiovascular disease, particularly in fathers (49%), and approximately 50% reported a first-degree family history of cancer, of which 34% were in fathers and 40% in mothers.
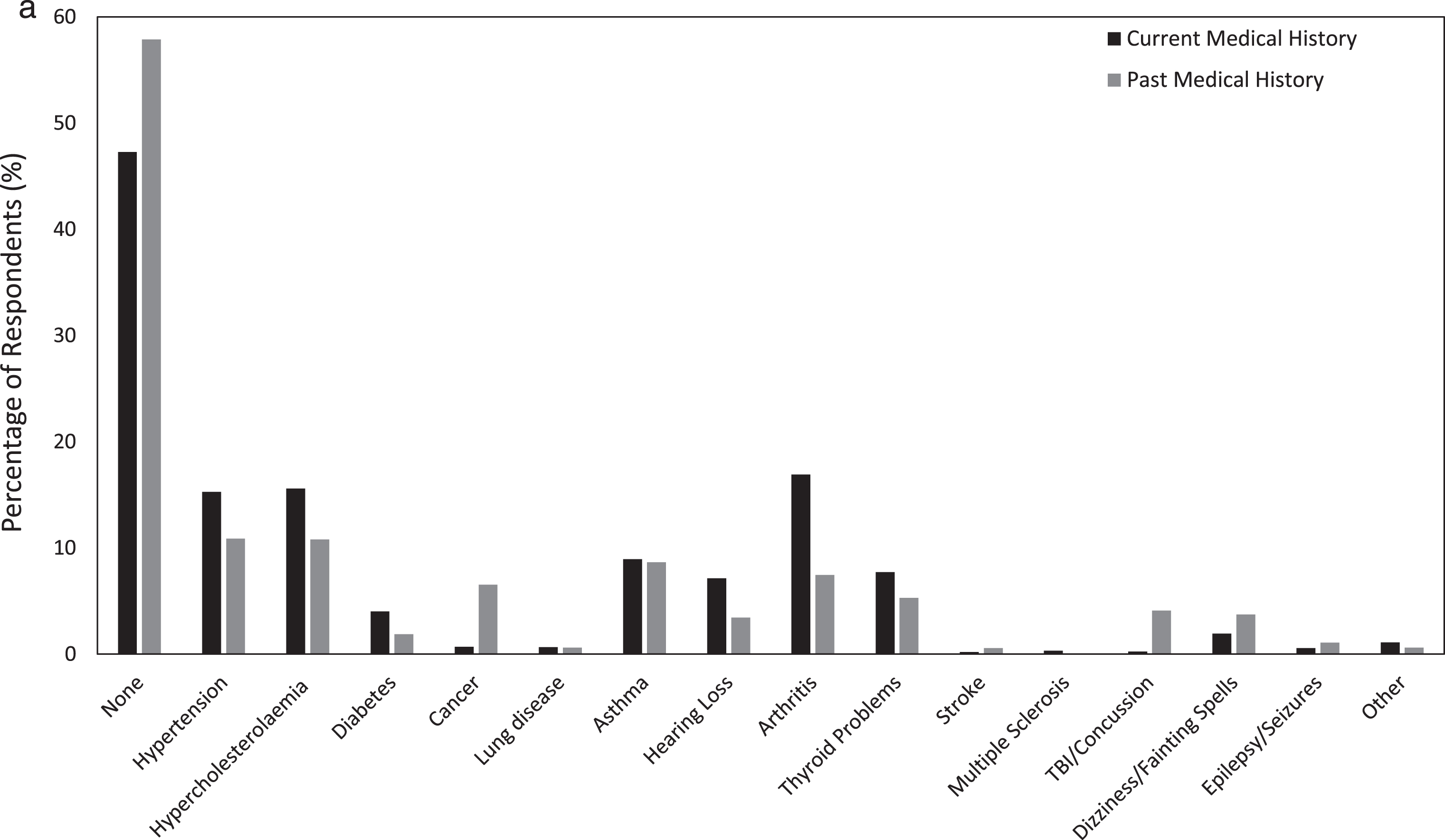
Self-report current and past medical history of participants.

Self-report current and past psychiatric history of participants.

Classification of common medications reported.
The class of current medications reported most commonly were the psychoanaleptics (26%) including non-selective monoamine reuptake inhibitors, selective serotonin reuptake inhibitors, and other anti-depressants. Other commonly reported medication classes were agents that act on the renin-angiotensin system (25%), such as angiotensin II agonists or angiotensin converting enzyme inhibitors, and lipid modifying agents (21%), which were largely HMG CoA reductase inhibitors (statins). The most common drug classification where multiple drugs from the same class were used by an individual were drugs used in diabetes (32% of those taking drugs from this classification took two or more of these types of drugs), antivirals for systemic use (30%), and psycholeptics (23%).
Motivation and engagement
In June 2018, we introduced a questionnaire to gauge participant’s motivation and engagement in medical research. A total of 596 participants (81.2% female) completed this questionnaire at the time of writing this manuscript. Of these, 90% (n = 537; 445 female, 90 male, 2 prefer not to disclose sex) considered themselves to be generally motivated to participate in medical research studies, and 97% (n = 572; 465 female, 105 male, 2 prefer not to disclose sex) would like to be contacted about future studies (59% research in general, 41% research in AD). A higher proportion of females than males reported being motivated to participate in medical research in general (92% versus 81%, χ 2 = 10.269, p = 0.001). However, equal proportion of females and males indicated that they would like to be contacted about future studies (98% versus 97%, χ 2 = 0.183, p = 0.67). When asked what would help participants remain engaged in the Healthy Brain Project each year, most (61%) indicated reminder emails, although a substantial portion (23%) would also like to receive reports on their own performance.
DISCUSSION
The identification of AD risk in middle-aged adults requires the assembly of a large cohort of people, as changes in cognition, behavior, mood, or brain volume due to accumulating Aβ are likely to be subtle. The aim of the HBP is to facilitate investigation of longitudinal change in cognition, lifestyle, mood and general health in middle-aged adults and consider these in relation to future risk of dementia, particularly AD. This is achieved through the use of an online platform to recruit, assess and prospectively monitor mood, cognition and behavior in a large number of middle-aged adults. The use of online platforms to recruit and survey participants for dementia research is increasing, and awareness related to the understanding of optimal design and implementation of such online platforms is also developing. Rapid changes in computer technology and demographic characteristics of older adults means that factors related to completion and general usability of the HBP platform will require ongoing active review, with dynamic adjustments made where limitations are found.
In this report, we present outcomes from the initial implementation phase of the HBP by describing the respondents, their patterns of adherence and their performance on the assessments contained therein. In the first 18 months of the HBP, 4,000 participants enrolled at a recruitment rate of ∼250 per month. The HBP platform was designed to allow participants to complete assessments in more than a single session, and in any order. While the aim of this approach was to reduce burden, it may also potentially increase risk of incomplete data if participants choose not to return to complete their assessments. At the time of analysis, 54% of enrolled participants had completed all assessments. This rate is equivalent to that reported in the BHR [20], where participants are requested to complete all assessments at enrolment. However, only 68% of participants completed at least one questionnaire, compared to 98% in the BHR, which may be due to the small number (2 maximum) of reminder emails we send to avoid excessive participant burden. As our participants have now indicated that they would like to receive more reminder emails, we intend to increase the frequency of reminder emails in the future, and we anticipate that this will improve our completion rates. Our results suggest that willingness to engage with research portals aimed at understanding early AD may be related more strongly to personal motivating factors, rather than time and effort requirements. In support of this, the HBP participants showed high levels of motivation not only for participation in the current study, but also to be contacted about future studies.
Participants mostly completed assessments in their homes, where they rated their environment as quiet. However, 15% did report completing assessments in noisy environments such as at home, work, during their commute, or in public (Fig. 3). Future studies should determine the relationship between environment and test performance. Participants who enrolled and completed assessments (completers) were ∼2 years older and more likely to be female than those who did not complete assessments (non-completers). The lower age limit of the HBP was set to recruit individuals for study prior to biomarker levels becoming abnormal; however, the older age of completers does suggest that older adults are more likely to participate in online studies of dementia research. There was also an over-representation of the number of females (74%) to males enrolled in the HBP. This over-representation persisted despite efforts to target male participants. For example, in August 2017, when we partnered with a large football sporting organization to promote recruitment, 65% of the participants recruited in this process were female. Females were also more likely to be completers (75%) and this bias is consistent with that observed in the BHR (74% female) [20], and even in early AD research studies that require in-person assessment, such as in the Australian Imaging, Biomarkers and Lifestyle (AIBL) study (60% female) [52]. This is also consistent with studies that have shown that males are less likely to seek help from health professionals than females [53, 54]. It is possible that this restrained pattern of help-seeking behavior in men may also extend to participation in medical research studies. Reviews of this sex bias in research participation suggest that females are more likely to participate due to encouragement by friends or family, general altruism, and fewer time constraints (e.g., due to part-time work, flexibility with work hours) [55 –57]. Thus, the sex difference identified here and other related studies suggest strongly that utilization of a remote and computer-based interface does not influence the differing levels of willingness of males and females to participate.
HBP completers and non-completers were not different in the proportions who reported a first-degree family history of dementia, or any current medical or psychiatric history. However, non-completers did report higher levels of depressive and anxiety symptoms, and lower scores of general physical health. While the magnitude of these differences was small (e.g., d = 0.2), it does raise the possibility that non-completers exhibit poorer levels of physical and mental health, although these symptoms may not yet meet clinical diagnostic thresholds. Whether rates of completion may be increased through strategies aimed at alleviating anxiety and depressive symptoms (e.g., through the provision of health education, offering pathways to clinical management, or providing summary reports of their performance) remains to be determined.
In the HBP, participants can work through each of the modules in any order. In this context, we observed that HBP participants were much more likely to complete the questionnaires than they were the cognitive tests. Participants who completed the cognitive tests were also older, more likely to be female, and exhibited higher levels of depressive and anxiety symptoms. The lower rate of completion of cognitive tests may also be because the cognitive tests were more demanding than the questionnaires, and their instructions were lengthier and more complex than those of the questionnaires. Finally, online cognitive tests require specific software specifications. For example, a browser switch is required for the completion of some tasks (i.e., Internet Explorer for Cogstate; Google Chrome for CANTAB). While instructions for this are provided to participants on their portal, these additional steps may have resulted in a decrease in completion rates of cognitive tests. We are currently undergoing a technological update with both Cogstate and CANTAB to avoid the need for these additional steps, and we anticipate that this will lead to higher adherence and completion rates. In addition, a future aim is to introduce mobile cognitive testing apps to further allow experiential sampling of a participant normal daily activities.
While online portals may increase the access of individuals to research participation, the extent to which such approaches provide data reflective of the population remains unclear. For example, an initial concern during the design of the HBP was whether adults aged over 60 years would be able to readily access a computer to complete the online assessments. In this analysis, ∼30% of the sample were aged between 60 and 70 years. Thus, despite the online nature of assessment, the study appears to be accessible to older middle-aged adults. This proportion is consistent with that from the 2016 Australian census which indicated that 50% of 65–69-year-old adults residing in Australia completed the census form using the online portal [58]. The current data also suggest that the socioeconomic background of participants did not influence completion as the average level of education (12 years) and personal income ($67,000) reported is comparable to the average education and income of Australians [58]. The HBP sample was predominantly Caucasian (76%), and this is consistent with the characteristics of the general Australian population [58]. However, the proportion of participants who classified themselves as Indigenous Australians (1.5%) or Asian (1.5%) was lower than the proportion of these groups in the general population (2.8% Indigenous Australians, 3.9% Asians) [58]. Of the HBP participants, 25% of completers were from regional or rural centers, compared to 32% of the general Australian population [58]. It is well understood that individuals in regional or rural centers often have limited access to medical research studies, and the significant proportion of participants from these areas in the HBP is a major strength of the study.
We have demonstrated that the HBP platform can feasibly recruit, monitor, and assess a very large group of individuals at risk of AD in a relatively short period of time. The online study design has also resulted in a sample that is diverse in race and geography and is comparable to the Australian population in many key aspects. Despite this, an important limitation of the HBP sample is that it is not an epidemiological sample as we have focused on recruiting participants with a first-or second-degree family history of dementia. The relatively lower proportion of males, younger middle-aged adults, and Indigenous Australians, Asians, and other ethnic groups will also be a focus of future recruitment drives. Another limitation of the HBP sample is that the process of assessing participants via an online platform assumes that participants will provide accurate and truthful reports of their health. While we require participants to confirm that they have a first-or second-degree family history of dementia, and that they do not have a neurological condition, the veracity of this information cannot be accurately determined online. Inaccuracies in participant self-report across various health conditions have been well-reported [59, 60] and is a limitation that all online-based cohorts and registries need to balance against the benefits of participant convenience and generalizability of the sample.
An increasing number of biomarker studies now suggest that the accumulation of AD proteinopathies begins many decades prior to clinical symptoms becoming evident [13 , 61]. In addition, cardiovascular disease is more strongly associated with later life dementia and brain atrophy when vascular risk factors are measured in midlife [62 –65]. As such, several studies and clinical trials are beginning to turn their focus toward understanding the genesis of AD in middle-aged adults [8 , 66], with the aim of designing preventative strategies to attenuate Aβ and tau accumulation before they reach clinically significant thresholds of abnormality. The HBP joins a global effort to understand and identify the earliest clinical symptoms of AD through the use of well-validated cognitive tasks and genetic analysis to understand AD risk. The HBP is a unique Australian resource, which will assist in the development and implementation of techniques for the early detection of AD, the elucidation of the role of genetics, midlife vascular factors and lifestyle factors to later-life cognitive decline and AD risk, as well as the facilitation of pre-screening and enrolment into future AD clinical trials. Consideration of the limitations and areas for refinement of online platforms for the study of aging or dementia described in this report will also provide current and future studies with guidelines for the optimal design and implementation of such platforms.
Footnotes
ACKNOWLEDGMENTS
Funding for the Healthy Brain Project was provided by the National Health and Medical Research Council (GNT1111603, GNT1105576, GNT1104273, GNT1147465) and the Alzheimer’s Association (USA) (AARG-17-501424). We would like to thank our study partners (PearlArc, SRC Innovations, Cogstate Ltd, Cambridge Cognition) for their support of the Healthy Brain Project. The Florey Institute of Neuroscience and Mental Health acknowledges support from the Victorian Government, in particular funding from the Operational Infrastructure Support Grant. We thank Paul Maruff for his comments and contributions to an earlier draft of this manuscript. We thank the media team of the Florey Institute of Neuroscience and Mental Health (particularly Amanda Place, Jane Standish and Dr Tom Keeble), the team at KAYO Consulting, Eddie McGuire and the Collingwood Football Club for assisting us with the recruitment of participants. We also thank all those who participated in the study for their commitment and dedication to helping advance research into the early detection and causation of Alzheimer’s disease.