
Abstract
Background:
Accessible measurements for the early detection of mild cognitive impairment (MCI) due to Alzheimer’s disease (AD) are urgently needed to address the increasing prevalence of AD.
Objective:
To determine the benefits of a composite MemTrax Memory Test and AD-related blood biomarker assessment for the early detection of MCI-AD in non-specialty clinics.
Methods:
The MemTrax Memory Test and Montreal Cognitive Assessment were administered to 99 healthy seniors with normal cognitive function and 101 patients with MCI-AD; clinical manifestation and peripheral blood samples were collected. We evaluated correlations between the MemTrax Memory Test and blood biomarkers using Spearman’s rank correlation analyses and then built discrimination models using various machine learning approaches that combined the MemTrax Memory Test and blood biomarker results. The models’ performances were assessed according to the areas under the receiver operating characteristic curve.
Results:
The MemTrax Memory Test and Montreal Cognitive Assessment areas under the curve for differentiating patients with MCI-AD from the healthy controls were similar. The MemTrax Memory Test strongly correlated with phosphorylated tau 181 and amyloid-β42/40. The area under the curve for the best composite MemTrax Memory Test and blood biomarker model was 0.975 (95% confidence interval: 0.950–0.999).
Conclusion:
Combining MemTrax Memory Test and blood biomarker results is a promising new technique for the early detection of MCI-AD.
INTRODUCTION
As the aging population rapidly increases, the prevalence of Alzheimer’s disease (AD) has concomitantly increased, becoming a major public health challenge [1]. Currently, AD is an irreversible and incurable disease. Early detection of mild cognitive impairment (MCI), the symptomatic preclinical phase of AD, is an important clinical focus, as it can improve patients’ health and slow its progression [2]. However, the early detection of MCI remains a challenge, particularly in non-specialty clinics where patients with MCI are frequently not recognized by general practitioners, such as in primary care settings. Moreover, cognitive impairment assessment tools appropriate for primary care facilities are lacking, contributing to these missed diagnoses [3].
Accuracy and efficiency are imperative for cognitive evaluations. Most available memory and cognition assessment utensils, such as the Montreal Cognitive Assessment (MoCA) and the Mini-Mental State Examination (MMSE), require professional clinicians or specially trained psychologists to evaluate the results [4, 5]. However, routine cognitive screening in non-specialty clinics or primary care settings must be short, easy to use, friendly to seniors, not influenced by education, culture, or language, and have sufficient specificity and sensitivity [6].
Digital biomarkers, which are simple assessments that require less time than traditional cognitive assessments, are becoming increasingly applicable outside memory clinics. For example, the MemTrax Memory Test (hereafter called MemTrax) is an online cognitive test ideal for routine use in non-specialty clinics [7]. Specifically, MemTrax outperforms MoCA for use outside of specialized memory clinics owing to its simple self-testing methods and good diagnostic performance. Consequently, older individuals with suspected cognitive abnormalities identified by MemTrax could be admitted to memory clinics for further evaluation, which is crucial for early diagnosis and treatment. Given that MemTrax is minimally influenced by language or culture, it presents a practical solution for the early identification of MCI [8].
MemTrax has been validated in several studies and developed into a simple online form [9]. MemTrax uses simple picture recognition memory to evaluate episodic memory, attention, and processing speed. Therefore, it is a feasible tool for evaluating episodic memory and other cognitive domains. Additionally, visual stimuli minimize language and cultural influences, and the test’s simplicity also ensures that people with different cognitive levels, from normal to mild or moderately impaired, can understand and follow instructions.
In clinical practice, differentiating MCI-AD from other causes of MCI is critical. Currently, blood biomarkers can detect AD pathology and identify AD in the preclinical stages of the disease. Furthermore, they are accessible and easy to implement for discriminating AD from non-AD. Plasma amyloid-β (Aβ) and phosphorylated tau (P-tau) levels reflect the two principal pathological features of AD, namely brain amyloidosis and tau pathology [10, 11].
Overall, we aim to develop a simple but reliable screening method capable of early MCI-AD detection in clinical services outside of specialized memory clinics. Therefore, this study assessed the clinical application of MemTrax in the Guangzhou Healthy Aging and Dementia cohort for identifying individuals with MCI-AD and created a combined digital and blood biomarker screening tool.
MATERIALS AND METHODS
Study population
We consecutively recruited individuals from the Guangzhou Healthy Aging and Dementia cohort. Participants in this cohort included patients admitted to memory-clinics in the Department of Neurology at the First Affiliated Hospital of Sun Yat-Sen University and healthy older controls recruited from the community between June 2020 and November 2022. All participants had completed detailed cognitive function assessments including MMSE, MoCA, Clinical Dementia Rating (CDR), Functional Activities Questionnaire (FAQ), MemTrax, blood tests, and neuroimaging including MRI, PET-CT (AV45 and FDG), or both. Participants in this study were screened from the cohort.
This study was approved by the ethics committees of the First Affiliated Hospital of Sun Yat-Sen University. All participants or guardians provided informed consent.
Classification of HC and MCI-AD
Vascular, traumatic, neurodegenerative, or other diseases related to cognitive dysfunction were excluded and classified into MCI-AD and healthy control (HC) groups based on the following criteria. The inclusion criteria of HC were no cognitive impairment in the neurocognitive test and a CDR score of 0. The diagnosis of MCI was based on a modified version of the criteria from Petersen et al., included the following elements: 1) Self and/or informant report cognitive decline and objective cognitive impairment in one or more domains in neuropsychological tests (scored at least 1.5 standard deviations below the aged and education matched norm). 2) Global CDR score = 0.5 or 0. 3) Daily activities and social functions are mainly preserved, or at least that impairment is minimal (A total FAQ score≤5). 4) No depression or other psychiatric conditions. 5) No dementia [12, 13]. MCI-AD was diagnosed based on a DSM-5 diagnosis for mild neurocognitive disorder based on the Diagnostic and Statistical Manual of Mental Disorders guidelines. Participants with visual or motor impairments that could hinder their completion of MemTrax or patients unable to comprehend the specific test instructions were excluded. Patients with a history of mental or neurological diseases that could lead to cognitive impairment were also excluded.
Study procedure
Demographic and personal information, including sex, age, years of education, living arrangements, smoking habits, regular alcohol consumption, family history of cognitive impairment, and medical history, were collected for each participant through a comprehensive paper questionnaire. Subsequently, the participants underwent neuropsychological tests, including MMSE, MoCA, CDR, FAQ, and MemTrax tests, in a relatively quiet room by well-trained interviewers and experts. First, a study team member collected the test results on paper, including the MemTrax percentage of correct responses (MTx-% C), the mean response time (MTx-RT), and the testing date and time. Then, two study team members verified the completed questionnaires and other neuropsychological tests results separately.
MemTrax test
A comprehensive examination of the principles and structure of MemTrax has been previously published [9]. Concisely, MemTrax consists of a 50-picture series comprising 25 novel pictures and 25 repeated pictures; one picture from each of the five categories is repeated twice. Each picture is presented for three seconds or until a behavioral response is elicited. The participants are instructed to respond swiftly by touching the screen only when presented with a repeated picture. Following the completion of the test, the program automatically calculates and presents the MTx-% C, MTx-RT, and the date and time of testing. The MemTrax composite score (MTx-Cp) was calculated by dividing MTx-% C by MTx-RT.
MoCA
Trained researchers administered the Beijing version of the Chinese form of MoCA following standard test guidance. Notably, the Beijing version has been established as a reliable cognitive screening tool for the Chinese elderly population regardless of education level. MoCA scores range from 0 to 30, with higher scores representing a better cognitive function. The test evaluates eight cognitive domains, which include attention, executive function, memory, language, visuospatial, abstract thinking, computation, and orientation. Each test requires 5–10 min of administration, depending on the participant’s cognitive capacity.
Plasma biomarkers
Blood samples were collected systematically from each participant at the study onset. Following collection, the samples were centrifuged for 10 min at 4000 rpm (4°C). Subsequently, the EDTA plasma Aβ40, Aβ42, and P-tau181 concentrations were determined utilizing an ultra-sensitive Simoa technology (Quanterix Corporation, Billerica, MA, US) via an automated Simoa HD-X platform (GBIO, Hangzhou, China) following the manufacturer’s protocol. The Neurology 4-Plex E Assay Kit (Cat No:103670) and P-tau181 Advantage V2 Assay Kit (Cat No: 103714) were acquired from Quanterix and utilized accordingly. The plasma samples were diluted 1 : 4 for measuring. The calibrators and quality controls were measured in duplicate to ensure accuracy and consistency. Importantly, kits from the same lot number were used in all sample measurements. The operators were unaware of the participants’ information.
Predictive modeling
Predictive modeling was performed using five common machine learning models: logistic regression, Naïve Bayes, K-nearest neighbors, support vector machine, and random forest. The models were trained and evaluated using a five-fold cross-validation algorithm. Specifically, the data were randomly divided into five equal segments: four for training and one for testing. This process was repeated five times utilizing a different segment as the test set. The area under the receiver operating characteristic curve (AUC) was utilized to assess the performance of the different models. The model building and evaluation processes were repeated multiple times to reduce bias and ensure replicability. The hyperparameter settings were selected based on previous research that indicated their robustness to various data. Further parameter tuning was not employed to avoid overfitting and increase the clinical utility of the models beyond the specific data used in this study. The mean Decrease Gini for each predictor was calculated to reflect the importance of each variable for the classification.
Statistical analyses
R version 4.1.3 (R Core Team, Vienna, Austria) was used for statistic analysis; all figures were generated with R software. Baseline demographic and clinical data and biomarker levels were analyzed using chi-square tests, unpaired student t-tests and Mann– Whitney U tests. Delong test was used to compare whether there is a significant difference in AUC between two models. Correlations between MemTrax and blood biomarker levels were calculated utilizing Spearman’s rank correlation analyses. p-values <0.05 were considered statistically significant.
RESULTS
Participant characteristics
We recruited 200 participants; 101 had MCI-AD, and 99 were HCs. Table 1 details the demographic and clinical manifestation of both groups; sex, age, living state, tobacco use, and alcohol addiction did not differ between them. The mean years of education were 12 and 9 in the HC and MCI-AD groups, respectively. Hypertension (p = 0.748), diabetes mellitus (p = 0.838), and hypercholesterolemia (p = 0.612) did not differ between the two groups. However, the MCI-AD group had significantly more patients with a family history of cognitive impairment than the HC group (p = 0.014). Additionally, the MCI-AD group had significantly lower MoCA scores than the HC group. Finally, the P-tau181 (p = 0.005) concentrations were significantly higher in the MCI-AD group compared with HC group. However, the Aβ42/40 ratio was significantly lower in the MCI-AD group when comparing to HC group (p = 0.000).
Demographic features and clinical manifestation of the participantsa
HC, cognitive normal healthy control subjects; MCI-AD, subjects with mild cognitive impairment due to Alzheimer’s disease; Aβ, amyloid-beta; P-tau181, phosphorylated tau 181.aValues are number (percentage) or mean±standard deviation, median (interquartile range [IQR]); bold values are statistically significant (p < 0.05);b Student’s t test;cMann-Whitney U testdChi-square test.
Differentiating HC and MCI-AD
As shown in Table 1, MTx-% C was significantly lower in the MCI-AD group compared with that in the HC group (p < 0.0001). Correspondingly, MTx-RT was markedly longer (p < 0.001) and MTx-Cp was significantly lower (p < 0.0001) in the MCI-AD group than those in the HC group.
Next, we performed logistic regression analyses to evaluate the diagnostic accuracies of MemTrax and MoCA. The AUCs for differentiating MCI-AD and HC individuals were calculated and compared between MemTrax (MTx-% C) and MoCA. The AUCs for differentiating MCI-AD and HC individuals were 0.770 (95% confidence interval [CI]: 0.711–0.830) for MoCA and 0.752 (95% CI: 0.692–0.812) for MTx-% C. There was no significant difference between the two AUCs (p = 0.662). However, the MTx-RT (AUC: 0.605, 95% CI: 0.537–0.673) and MTx-CP (AUC: 0.700, 95% CI: 0.636–0.764) AUCs were significantly lower than the AUC for MoCA.
Table 2 lists the model’s accuracy and the MoCA and MemTrax cutoff values. The best cutoff value for discerning HCs from individuals with MCI-AD based on MTx-% C was 79%, resulting in an MCI-AD diagnostic accuracy of 75%. Similarly, when MTx-Cp was used to classify the HC and MCI-AD groups, the best cutoff value was 55.9%, resulting in an MCI-AD diagnostic accuracy of 70%.
Logistic regression results of MoCA, MemTrax test scores, and blood biomarkers
MoCA, Montreal Cognitive Assessment; MTx-% C, MemTrax percent correct; MTx-RT, MemTrax mean response time; MTx-Cp, MemTrax composite score; Aβ, beta-amyloid; P-tau181, phosphorylated tau 181.
Correlation of MoCA and MemTrax
We further explore the relationship between MoCA and MemTrax performance to prove the consistency of the two tests and calculated the Spearman correlation between them. Figure 1 showed that MoCA was strongly correlated with MemTrax performance. The higher the MoCA score, the better the corresponding MTx-% C (r = 0.4335, p < 0.0001) and MTx-Cp (r = 0.3429, p < 0.0001). On the contrary, MoCA was negatively correlated with MTx-RT(r=-0.2504, p = 0.0004).
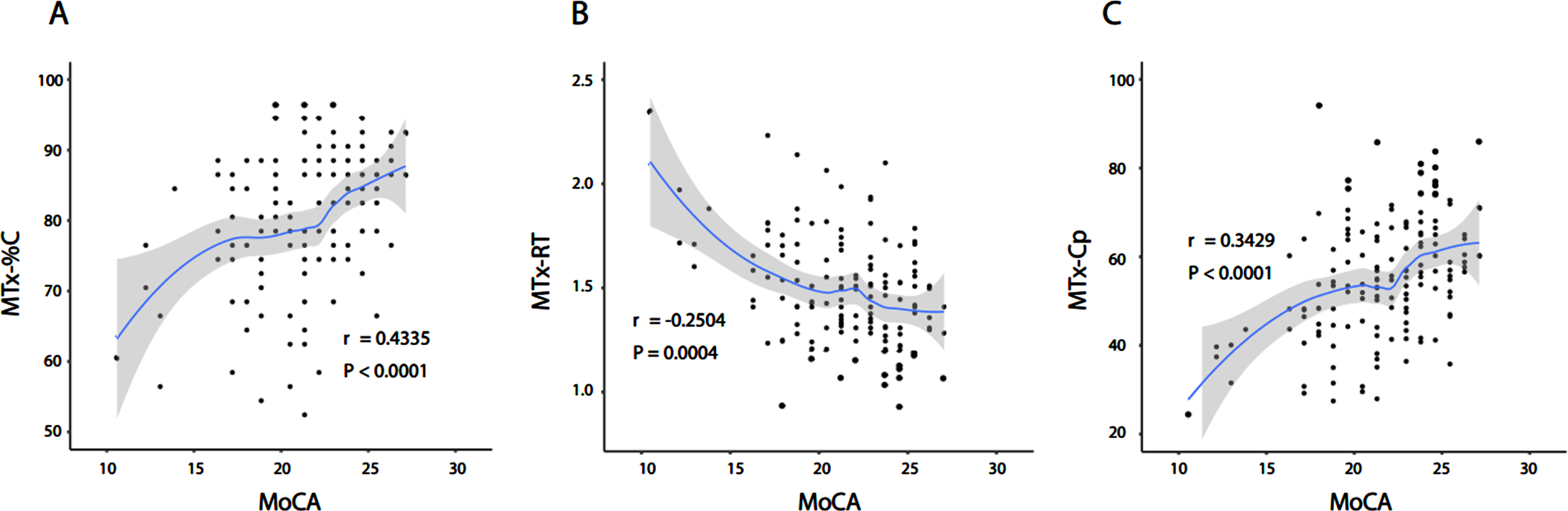
Strong relationship between MoCA and MTx-% C (A), MTx-RT (B), and MTx-Cp (C).
Correlation of plasma biomarkers and MemTrax performance
The P-tau181 and Aβ42/40 plasma biomarkers differed between the MCI-AD and HC groups (Table 1). The P-tau181 and Aβ42/40 AUCs for differentiating individuals with MCI-AD and HCs were 0.703 (95% CI: 0.607–0.798) and 0.691 (95% CI: 0.613–0.794), respectively (Table 2). Furthermore, a high P-tau181 level was associated with worse MTx-% C performance (r = –0.3683, p = 0.0030), a long MTx-RT (r = 0.4990, p < 0.0001), and a low MTx-Cp (r = –0.5057, p < 0.0001) in MCI-AD. Additionally, a high Aβ42/40 level was associated with a high MTx-Cp (r = 0.3016, p = 0.0163) and a long MTx-RT (r = –0.2896, p = 0.0213) in MCI-AD. On the contrary, Aβ42/40 level was not related to MTx-% C. No association was found between MemTrax performance and plasma biomarkers in HC (Fig. 2). Also, MoCA was not significantly correlated with blood biomarkers in neither MCI-AD nor HC group (Fig. 2D, H).

Machine learning analysis
Five machine-learning approaches were evaluated to differentiate between the MCI-AD and HC groups (Table 3). When MTx-% C was the only variable, all five algorithms had similar effects (all p > 0.05); the AUCs were: logistic regression: 0.732, 95% CI: 0.670–0.794, naïve Bayes: 0.752, 95% CI: 0.692–0.812, and each of the other three algorithms: 0.780, 95% CI: 0.722–0.838. When P-tau181 and MTx-% C were used, the AUC values of all models remained similar to those obtained using only MTx-% C (all p > 0.05), except for the random forest model. The random forest model with the MTx-% C and P-tau181 variables had an AUC of 0.933 (95% CI: 0.892–0.974; Fig. 3A). Finally, when Aβ42/40 was added to the random forest model, the AUC reached 0.975 (95% CI: 0.950–0.999; Fig. 3A). The MemTrax and MoCA AUCs did not differ when blood biomarkers were added (p > 0.05). Thus, the random forest model was the best-performing classifier for discerning individuals with MCI-AD and HC among the five machine-learning approaches. Furthermore, combining blood biomarkers with MemTrax enhanced the classification performance compared to MemTrax or plasma biomarkers independently. Finally, MemTrax had the same verification efficiency as MoCA using the combination models.
AUC values of different machine learning approaches to classify MCI-AD and HC
MTx-% C, MemTrax percent correct; MTx-RT, MemTrax mean response time; MTx-Cp, MemTrax composite score; MoCA, Montreal Cognitive Assessment; Aβ, amyloid-beta; P-tau181, phosphorylated tau 181.
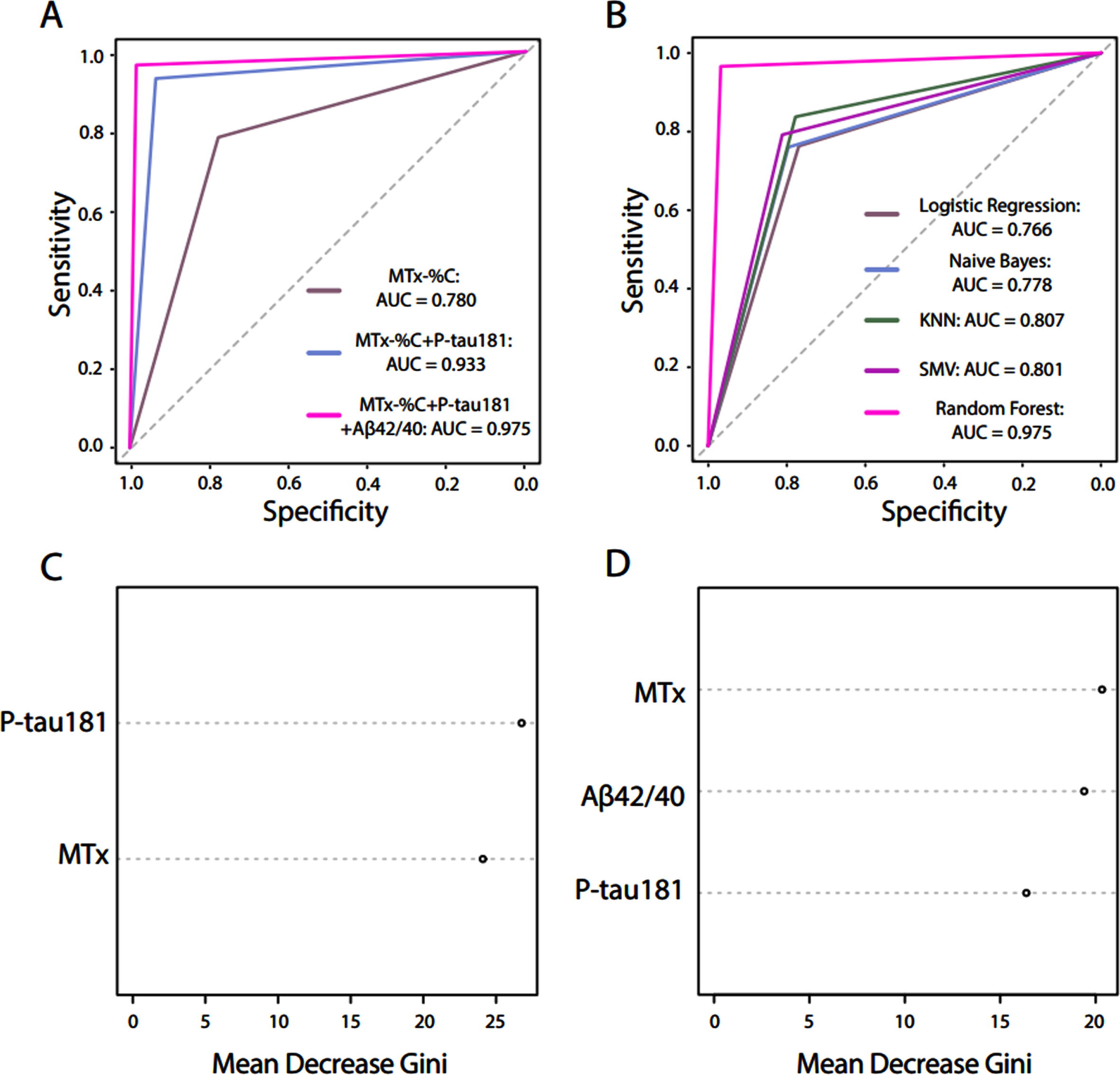
We further calculated the Mean Decrease Gini for each predictor variable in the random forest model, which reflects the importance of each variable for the classification. Figure 3C and 3D shows the Mean Decrease Gini of each predictor variable in each random forest model in Fig. 3A. The Mean Decrease Gini values indicate that MTx-% C is an essential variable for discriminating MCI-AD from HC using the final random forest model (Fig. 3).
DISCUSSION
This study validated a digital cognitive assessment using MemTrax in patients from the Guangzhou Healthy Aging and Dementia cohort; the AUCs were 0.752 for MTx-% C, 0.605 for MTx-RT, and 0.700 for MTx-CP. Thus, MTx-% C was the best index for differentiating individuals with MCI-AD from HCs. Additionally, MTx-% C scores≥79% had an accuracy of 75%.
As a screening tool for early detection of MCI, MemTrax has its pros and cons. Firstly, MemTrax is less time-consuming (1.5–2.5 min) than traditional cognitive tests, such as the MoCA (5–10 min), which makes it suitable for large-scale screening. In addition, MemTrax test is less affected by language and education levels because MemTrax test is based on recognition of pictures. However, it should be noticed that MemTrax test does not accurately reflect the function of different cognitive domains although its outcomes have been reported to be correlated with multiple cognitive domains [7]. In contrast, MoCA is able to evaluate multiple cognitive domains, which is more suitable for clinical practice.
P-tau181 and Aβ42/40 are two primary biomarkers for diagnosing AD [14–16]. Plasma P-tau181 and Aβ42/40 correlate with pathological cerebrospinal fluid Aβ42/40 concentrations and Aβ-positron emission tomography scans at different stages of AD [17]. We found that the P-tau181 and Aβ42/40 AUCs for differentiating individuals with MCI-AD from HCs were 0.703 and 0.691, respectively, similar to a previous study [18]. In addition, we found that the MemTrax score had a good correlation with P-tau181 and Aβ42/40.
A previous study reported better predictions of longitudinal changes in Mini-Mental State Examination results and the progression from MCI to AD dementia after integrating plasma neurofilament light chain, P-tau, and Aβ42/40 variables into a predictive model [19]. Furthermore, combining plasma P-tau217, APOE genotype, memory, and executive function has been shown to produce higher accuracy [20]. Studies have already demonstrated that MemTrax can differentiate patients with MCI from HCs [8]. Subsequently, we found that MemTrax results combined with AD-related blood biomarkers could also distinguish patients with MCI-AD from HCs. Notably, MemTrax with P-tau181 and Aβ42/40 resulted in a significant AUC increase, from 0.780 to 0.975 (Fig. 3A). Therefore, we could identify MCI-AD at an early stage using a simple self-assessment (i.e., MemTrax) combined with AD-related blood biomarkers. This result is valuable because early identification can lead to early interventions that potentially delay disease progression to AD, reducing the burden on families and society.
One limitation of our study was the age difference between the two groups, which was relatively large; however, it was statistically insignificant (p = 0.058). Furthermore, owing to the study’s cross-sectional nature, we could not track disease progression over time, which is critical for early intervention. However, a longitudinal study (the Guangzhou Healthy Aging and Dementia study) was conducted based on the results of this study for prediction of the progression from MCI to AD. Most importantly, our study is a case-control study based on retrospective data, which may introduce selection bias and confounding factors. Therefore, our discriminant rule should be interpreted as the Phase I development of a new diagnostic tool for MCI-AD rather than a definitive diagnostic criterion. Further studies are needed to validate and optimize our discriminant rule in prospective cohorts with different settings and populations.
In conclusion, we assessed the clinical application of the MemTrax in the Guangzhou Healthy Aging and Dementia cohort for identifying individuals with MCI-AD and created a combined digital and blood biomarker screening tool, which is promising to enhance the early detection of MCI-AD.
Footnotes
ACKNOWLEDGMENTS
The computer code for developing MemTrax in China was provided by MemTrax, LLC, CEO, Curtis Ashford, Dr. Ashford’s son. We would like to thank all the colleagues, friends, and the patients to participate in this study.
FUNDING
This study was supported by grants from the National Key R&D Program of China (2022YFA1104900), the National Natural Science Foundation of China (No. 81873751, No. 82271266, No. 82071255, No. 82201468, No. 31900475, No. 32270701), Guangdong Basic and Applied Basic Research Foundation (No. 2021B1515120062), the Guangdong Provincial Key Laboratory of Diagnosis and Treatment of Major Neurological Diseases (2020B1212060017), Guangdong Provincial Clinical Research Center for Neurological Diseases (2020B1111170002), Southern China International Joint Research Center for Early Intervention and Functional Rehabilitation of Neurological Diseases (2015B050501003 and 2020A0505020004), Guangdong Provincial Engineering Center for Major Neurological Disease Treatment, Guangdong Provincial Translational Medicine Innovation Platform for Diagnosis and Treatment of Major Neurological Disease, Guangzhou Clinical Research and Translational Center for Major Neurological Diseases (201604020010), Young Talent Recruitment Project of Guangdong (2019QN01Y139) and The Fundamental Research Funds for the Central Universities, Sun Yat-sen University (22ykqb07).
CONFLICT OF INTEREST
The authors report no relevant financial or other conflicts of interest in relation to this study. Dr. Ashford serves as an unpaid advisor to MemTrax, LLC, which provides the MemTrax test for a fee. Dr. Ashford is an Editorial Board Member of this journal but was not involved in the peer-review process nor had access to any information regarding itspeer-review.
DATA AVAILABILITY
The data supporting the findings of this study are available on request from the corresponding author.